
Abstract
Introduction
Depression is a well-known complication of different types of cancers. 1 Not only does depression reduce quality of life in patients with cancer, but it is also known to be associated with worse prognosis and lesser chances of survival. 2 Breast cancer is the leading malignancy among women, accounting for 1 in 4 cancers in females 3 and the third cancer with the highest association with depression, only behind oropharyngeal and pancreatic cancers. It has been estimated that 1.5% to 46% of patients affected by breast cancer develop depression, mainly during the first year following diagnosis. 4 More than half of depressive episodes among breast cancer patients are mild, making underdiagnoses and lack of appropriate interventions more likely. 5 Cancer-related pain is another common finding in those affected by this malignancy. 6 Not only does poor management of pain result in decreased quality of life, but it is also known to be associated with higher rates of depression in breast cancer patients. 7 Hence, concurrent and efficient management of both pain and depression may result in better quality of life and prognosis. Nonsteroidal anti-inflammatory drugs (NSAIDs) are a major group of analgesic agents widely used for pain management in patients with breast cancer. These drugs are used as first-line analgesics in cancer patients with bone metastasis, and they are also administrated routinely for pain relief in breast cancer patients with arthralgia resulting from the use of aromatase inhibitors.8,9
Among the different types of analgesics, celecoxib, an NSAID that acts via the selective inhibition of cyclo-oxygenase (COX)-2, has shown beneficial effects in several psychological disorders, including schizophrenia, 10 autistic disorder, 11 and depression. 12 Antidepressive effects of celecoxib have been attributed to its inhibitory effect on proinflammatory cytokines. 13 Several studies have shown increase in levels of proinflammatory cytokines, including interleukin (IL)-6 and tumor necrosis factor (TNF)-α in patients with major depressive disorder (MDD), thus indicating the probable role of uncontrolled inflammatory responses in the etiopathogenesis of depression. 14
Interestingly, celecoxib seems to have some potential beneficial effects in breast cancer. One remarkable feature of celecoxib is its antitumor effects. Celecoxib may halt malignant transformation of cells in patients with extensive actinic damage, thus preventing the development of squamous cell carcinomas and basal cell carcinomas. 15 This agent also proved to be effective in preventing the development of colorectal adenomatous polyps.16,17 Most important, the administration of celecoxib in animal models of breast cancer has resulted in significant reduction in all tumor parameters. 18 Celecoxib has also shown promising results in reducing the resistance of tumor cells to anticancer drugs as well as breast cancer recurrence.19,20 Furthermore, celecoxib has also been shown to be effective in improving bone marrow density in breast cancer patients. 21 It is also notable that breast cancer patients who receive hormonal therapy, including aromatase inhibitors; fulvestrant, an estrogen receptor antagonist; and luteinizing hormone-releasing hormone agonists are at high risk of bone loss and osteoporosis.21-23
Diclofenac, another NSAID, is a nonselective inhibitor of both COX-1 and COX-2 and is routinely used for pain management in different conditions, including breast cancer. 24 The use of diclofenac has been reported to be associated with an increased risk of developing gastrointestinal (GI), cardiorenal, and hepatic adverse events compared with celecoxib, which appears to have similar pain relief benefits. 25 There is inconsistency in the current literature regarding the analgesic efficacies of diclofenac and celecoxib compared with each other; for example, whereas one study reported superior analgesic effect for diclofenac compared with celecoxib, 26 another study did not observe this finding. 25 Moreover, the use of celecoxib as an alternative to diclofenac in the management of pain has been shown to be more cost-effective, mainly because of the lower risk of developing GI complications, most notably bleeding. 27
To the best of our knowledge, the current study is the first report comparing the antidepressant effects and safety of a selective COX-2 inhibitor, celecoxib, and a nonselective inhibitor of COX-1 and COX-2, diclofenac, in breast cancer patients with mild to moderate depression who suffered from pain and needed analgesics. We hypothesized that celecoxib may be a safe and appropriate alternative to diclofenac because of its superior antidepressive effects, lower incidence of adverse effects, and comparable analgesic effects.
Patients and Methods
Trial Design and Setting
This single-center, 6-week, randomized, double-blind, controlled, parallel-group trial was conducted in the outpatient clinics of Imam Hospital (Tehran University of Medical Sciences, Tehran, Iran) between June 2014 and January 2015. The institutional review board (IRB) of Tehran University of Medical Sciences approved the trial protocol (Grant No. 24350). The trial was conducted according to the Declaration of Helsinki and its subsequent revisions. Written informed consent was obtained from all participants prior to study entry. The participants were free to withdraw from the study at any time without compromising their relationship with their health care provider. The trial was registered at the Iranian registry of clinical trials (www.irct.ir; registration number: IRCT201405271556N58).
Participants
Eligible patients were women aged 18 to 70 years with a diagnosis of breast cancer for more than 100 days, major depression according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), a score ≤18 in the 17-item Hamilton Depression Rating Scale (HDRS) to have mild to moderate depression, 28 mild to moderate pain, and need for analgesic. Exclusion criteria were as follows: receiving any antidepressant medication during the previous month, receiving electroconvulsive therapy (ECT) during the past 2 months, history of any other mental disorder on the DSM-IV axis I, alcohol or substance (with the exception of nicotine) dependence, being under concomitant medications that increase GI bleeding risk, using opioid analgesics, history of cardiovascular or thyroid disease, and pregnant and nursing women.
Interventions
Eligible patients randomly received either 200 mg celecoxib (celebrex, Pfizer, 200 mg capsule) twice daily or 50 mg diclofenac twice daily (50-mg capsules) in the same manner for 6 weeks. All participants were receiving standard breast cancer treatment. Participants were not allowed to use any other psychotropic medication or undergo behavioral intervention therapy during the trial course. Medication adherence was measured using weekly capsule counts justified against participant reports of medication intake to calculate the proportion of dispensed medication doses that were actually ingested.
Outcomes
Participants were evaluated using HDRS at baseline and at weeks 3 and 6. HDRS is a validated 17-item rating scale that has been widely applied in psychiatric studies to measure the severity of depressive symptoms and also has been used to evaluate treatment efficacy and severity of depressive symptoms in several clinical trials in Iran.29-32 The Visual Analogue Scale (VAS) was used to measure pain intensity (0 to 100, from “no pain” to “worst possible pain”). The primary outcome measure was to evaluate the efficacy of celecoxib in improving depressive symptoms compared with diclofenac during the trial course using a general, linear repeated-measures model. The secondary outcome measures of this trial were comparison of changes in HDRS score from baseline to each time point, response to treatment (defined as ≥ 50% reduction in the HDRS score), remission (defined as HRDS score ≤ 7), and severity of pain intensity between the treatment groups and evaluation of the antidepressant effects of each drug separately. Adverse events were systematically evaluated at each time point using a checklist. Furthermore, patients were first asked an open-ended question about any adverse event that was not mentioned on the checklist. Patients were also asked to immediately inform the research team of any unexpected symptom during the trial course.
Sample Size
Assuming a difference of 3 on the HDRS score, standard deviation (SD) of 3 (based on our pilot study), a 2-sided significance level of 5%, and a power of 90%, a total sample size of 46 (23 in each arm) was needed. Assuming a 20% attrition rate, a final sample size of 56 was calculated.
Randomization, Allocation, Concealment, and Blinding
A computerized random number generator (blocks of 4, allocation ratio 1:1) was applied for generation of randomization codes. An independent group that was not involved elsewhere in the study was responsible for generation of randomization codes. Sequentially numbered and sealed packages were used to conceal allocation. Separate people were responsible for random allocation and rating of patients. The participants, the physician who referred the patients, the physician who prescribed the medications, the rater, and the statistician were all blinded to the allocated treatment. Celecoxib and diclofenac capsules were completely identical in their size, shape, color, texture, and odor.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS version 20, IBM Company, USA) was used for statistical analysis. All analyses were performed based on the intention-to-treat principles with at least 1 postbaseline measurement. Categorical variables were reported as frequency (percentage), and continuous variables were reported as mean ± SD. Baseline continuous variables were compared using the independent t test. The mean difference (MD) between the celecoxib and diclofenac groups was reported as MD (95% CI). A 2-factor repeated-measures analysis of variance (ANOVA) was used to evaluate Time × Treatment interaction. Results of Greenhouse-Geisser adjustment were reported if Mauchly’s test of sphericity was significant. To compare score changes from baseline to each time interval between the 2 study groups, the independent t test and Cohen’s d effect size were used. VAS scores were compared between the groups using the independent t test at baseline and at study conclusion. The paired t test was used to compare HDRS scores at baseline with each time point in each group. Categorical variables were compared using the χ2 test or Fisher’s exact test.
Results
Participants and Baseline Characteristics
A total of 94 patients were screened for eligibility; 56 patients were randomly assigned to receive either celecoxib (n = 28) or diclofenac (n =28); 52 patients (26 in each arm) had at least 1 postbaseline measurement, and 52 participants completed the trial (Figure 1). Baseline characteristics of the patients were not significantly different between groups (Table 1). All patients were compliant to their treatment. Only 1 patient did not use celecoxib for 2 days because she was on a trip.
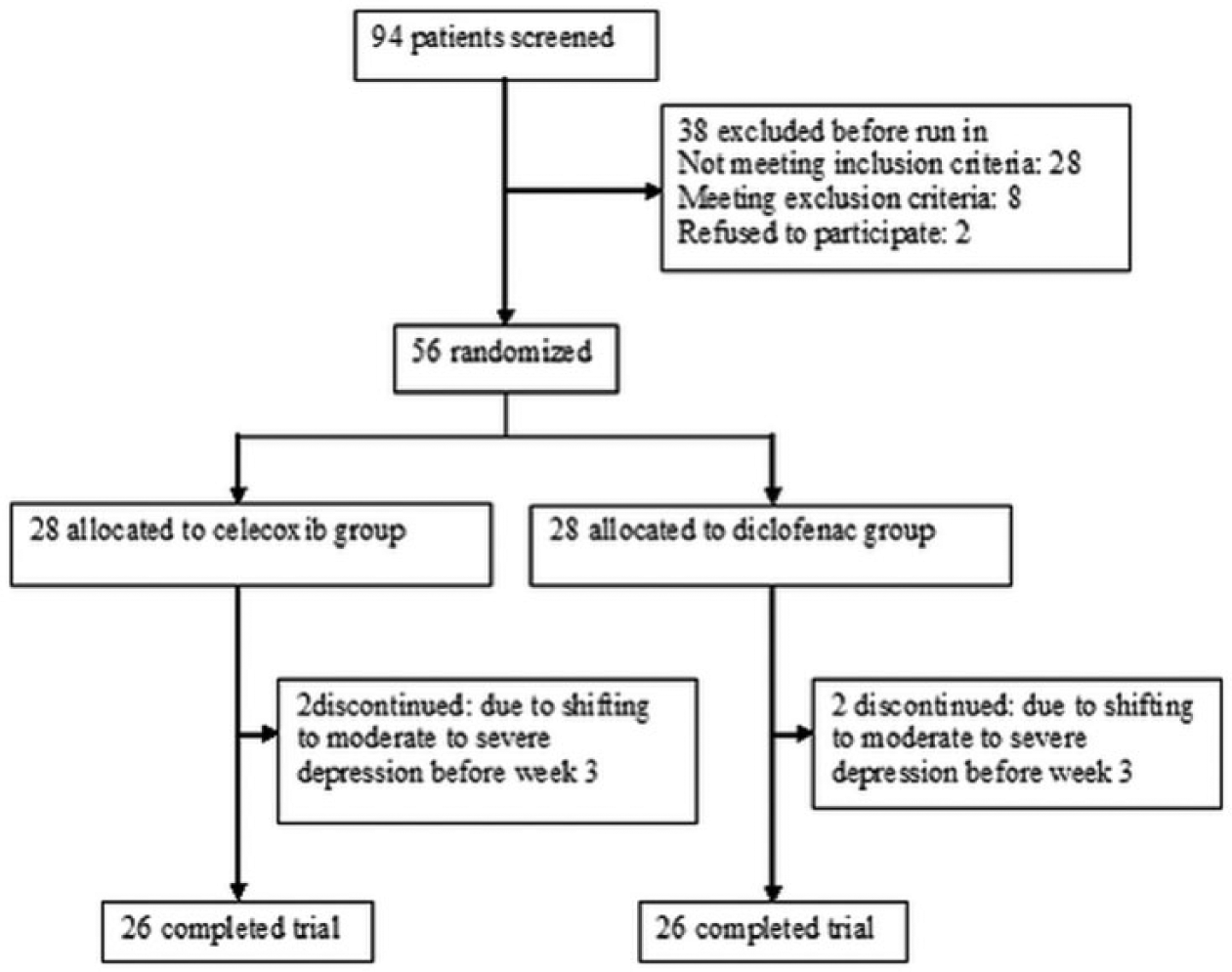
Flow diagram of the study.
Baseline Characteristics of the Participants.
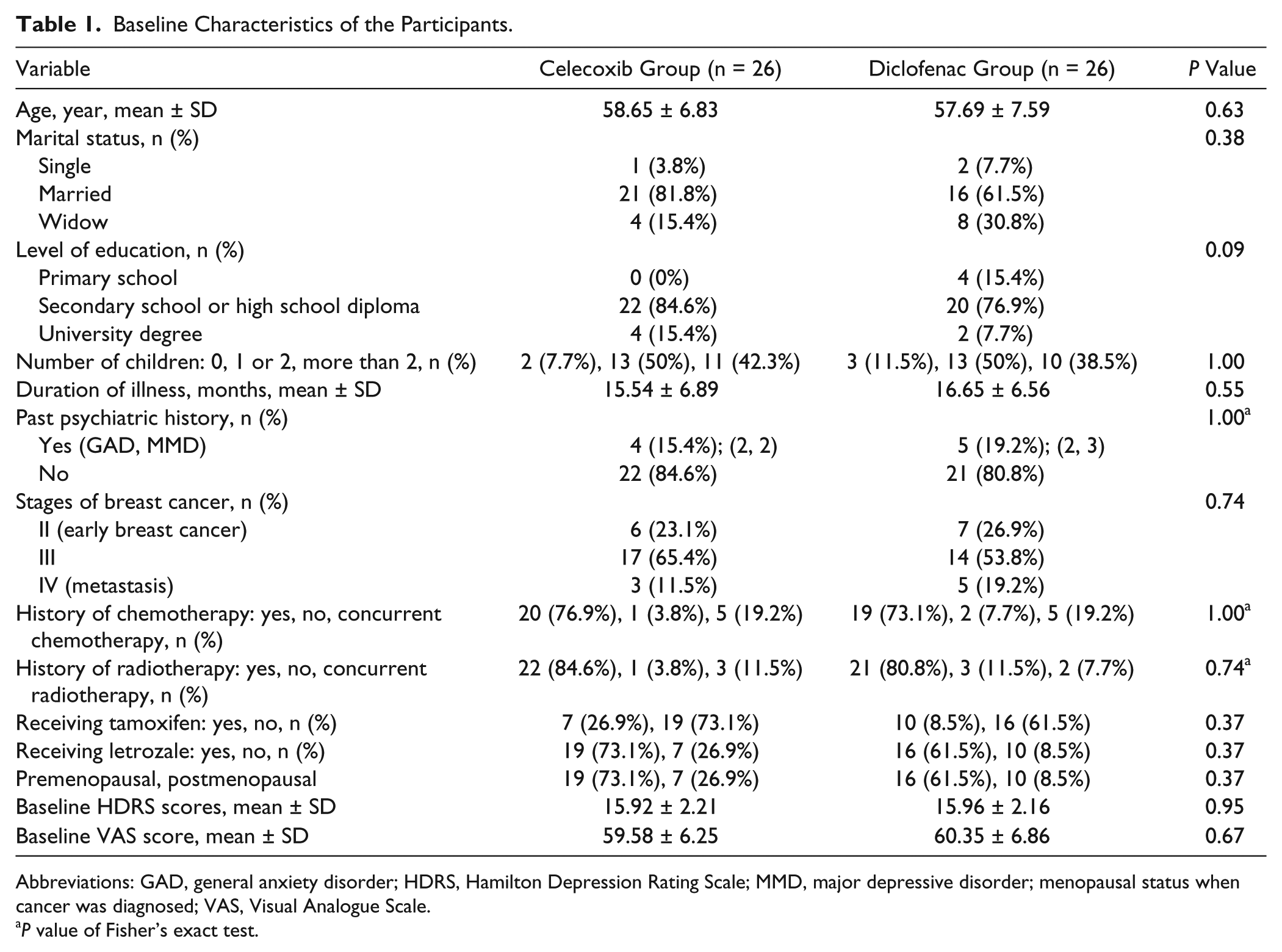
Abbreviations: GAD, general anxiety disorder; HDRS, Hamilton Depression Rating Scale; MMD, major depressive disorder; menopausal status when cancer was diagnosed; VAS, Visual Analogue Scale.
P value of Fisher’s exact test.
Outcomes
HDRS Score
Baseline HDRS scores were not significantly different between the celecoxib group and the diclofenac group: MD (95%CI) = 0.04 (−1.18 to 1.26); t(50) = 0.06; P = 0.95 (Table 1). Two-factor repeated-measures ANOVA demonstrated significant effect for Time × Treatment interaction on HDRS score during the course of study: F(1.76, 87.85) = 9.66; P < 0.001 (Figure 2). Improvements in HDRS score were not significantly different between the treatment groups at week 3. However, significantly greater reduction in HDRS score was observed in the celecoxib group than in the diclofenac group at week 6 (Table 2). There were significant improvements in the HDRS scores at weeks 3 and 6 in both the celecoxib and the diclofenac groups (Table 3). However, at study conclusion, no patient in the diclofenac group and only 1 patient in the celecoxib group achieved response to treatment (P = 1.00). No one achieved remission (HDRS ≤ 7) in both groups.
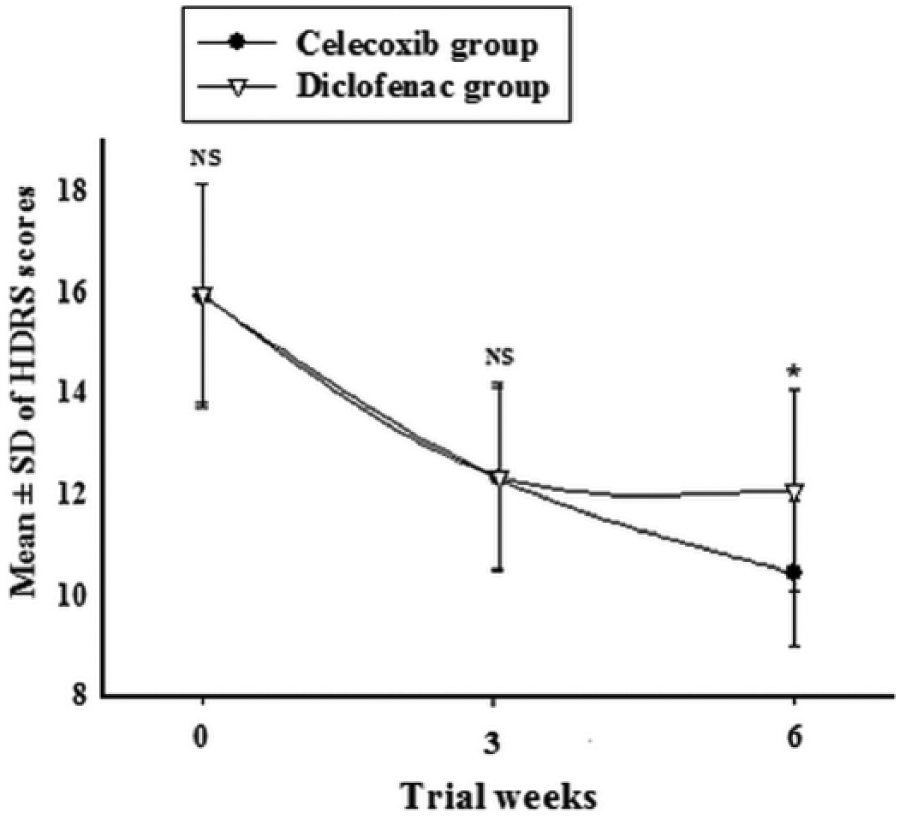
Repeated measure for comparison of the effects of 2 treatments on the Hamilton Depression Rating Scale (HDRS). Values represent mean ± SDs. P values show the result of the independent t test for comparison of scores between the 2 groups at each time interval. *P < 0.05.
Comparison of Score Changes Between the 2 Groups Using the Independent t Test.
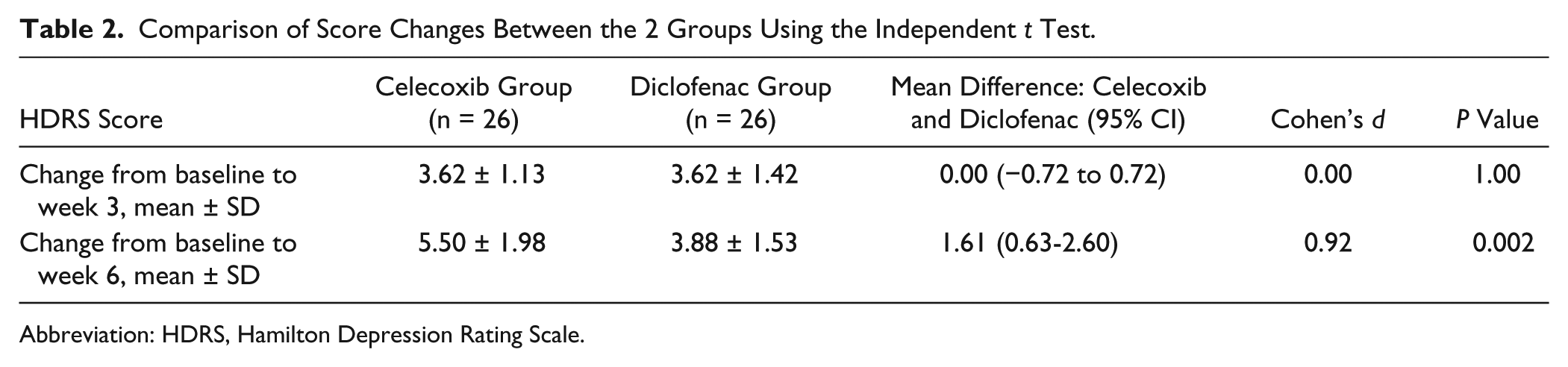
Abbreviation: HDRS, Hamilton Depression Rating Scale.
Comparison of HDRS Score at Each Time Point With Baseline HDRS Score in Each Group Using the Paired t Test.

Abbreviation: HDRS, Hamilton Depression Rating Scale.
VAS Score
There was no significant difference between the mean VAS scores for celecoxib and diclofenac groups at baseline and at the study end point (59.58 ± 6.25 vs 60.35 ± 6.86, P = 0.67, and 45.88 ± 5.74 vs 44.50 ± 5.41, P = 0.37, respectively; Figure 3).
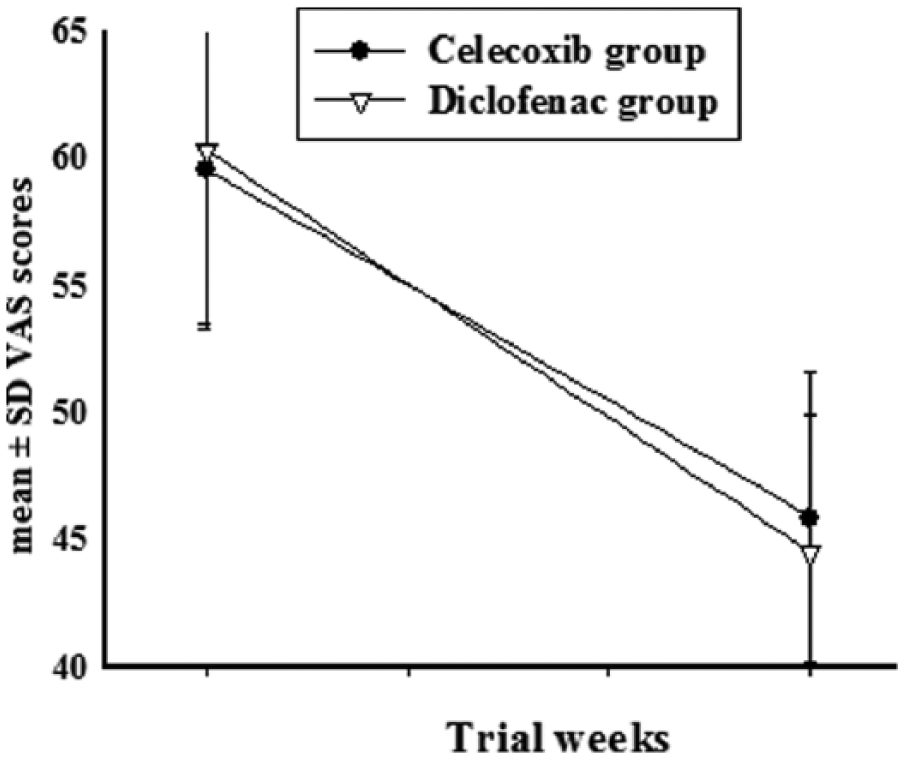
Visual Analogue Scale (VAS) scores in celecoxib and diclofenac groups at baseline and at the study end point.
Adverse Events
Frequencies of adverse events were not significantly different between groups (Table 4). No cardiovascular adverse event occurred in the celecoxib group, which was confirmed by physical examination and normal ECG. No serious adverse events or deaths were observed. GI discomfort was the most common complication in the diclofenac group, affecting 5 (19.2%) patients. The most common adverse events in the celecoxib group were GI discomfort and diarrhea, both observed in 2 (7.7%) patients. No treatment discontinuation was observed as a result of drug adverse events.
Frequency of Adverse Events in the 2 Study Groups.
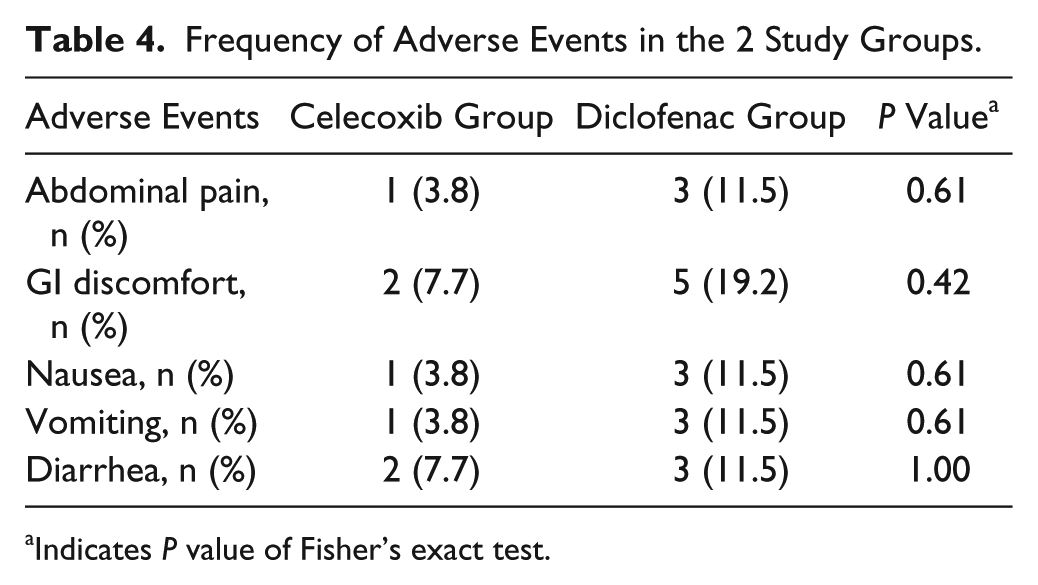
Indicates P value of Fisher’s exact test.
Discussion
The findings of the current study showed greater antidepressant effects for celecoxib versus diclofenac during the course of the trial. However, no one experienced remission (HDRS ≤ 7) in either the celecoxib or the diclofenac groups. The analgesic efficacy of these drugs was comparable. The use of both celecoxib and diclofenac appeared to be safe and well tolerated, and no serious adverse event was reported in any of the patients in either of the groups. Because baseline characteristics of patients in the 2 study groups did not differ significantly, it cannot explain the greater beneficial effect of celecoxib on depressive symptoms compared with diclofenac.
In agreement with our findings, several previous studies have shown significant improvement in depressive symptoms among patients receiving celecoxib. In one study, Müller et al 33 compared the efficacy of celecoxib in comparison with placebo as an add-on to reboxetine, a norepinephrine reuptake inhibitor, in reducing depressive symptoms in patients with major depression. They reported a significantly greater improvement in depressive symptoms in the celecoxib group and concluded that the antidepressive effect of an anti-inflammatory agent indicates the probable role of proinflammatory pathways in the etiopathogenesis of depression. The results of a recent meta-analysis on the efficacy of celecoxib as an adjuvant therapy in the management of MDD, which included 4 studies and 150 cases (75 in the treatment arm and 75 in the placebo arm), demonstrated significantly greater improvement in the celecoxib arm. 34 In another study, Fields et al 35 investigated the prevalence of depressive symptoms in 2312 elderly patients who received either placebo, celecoxib, or naproxen, which is an NSAID and nonselective inhibitor of both COX-1 and COX-2. They found no statistically significant difference in depressive symptoms between these groups. Although their findings are in contrast with the results of the present study, this inconsistency may be explained via several factors. First, whereas we assessed depressive symptoms at 3-week intervals, Fields et al performed their investigations at yearly intervals with variation in the follow-up period of different patients. It is possible that Fields et al missed the early responses, and their long-term results could be affected by the relapse of cancer. Moreover, it is also likely that patients with more severe depressive symptoms fail to attend follow-up visits. Second, Fields et al used the 30-item version of the Geriatric Depression Scale (GDS) for assessment of depressive symptoms. Even though the GDS has been validated against HDRS for use in the elderly, it is generally regarded as a screening method, and the clinical diagnosis of depression, especially in its minor forms, could not be based on GDS alone. 36 Third, Fields et al used a population study of elderly individuals with a family history of Alzheimer-like dementia. The association between depression and dementia is well described in the literature and may have affected the outcome of treatment in this group of elderly individuals. 37
Several hypotheses have been proposed for the mechanism of action of COX-2 inhibitors in reducing depressive symptoms. 16 The most likely explanation involves the anti-inflammatory effects of COX-2 inhibitors on the central nervous system. 33 Upregulation of COX-2 is known to result in increased production of PGE2, which in turn stimulates expression of IL-6. Animal studies have shown that inhibition of COX-2 could result in reduction of proinflammatory cytokines. In one study, El-Ghazaly et al 38 evaluated serum levels of IL-6, TNF-α, and PGE2 in a rat model of the inflammatory state. Rats showed decrease in levels of mentioned inflammatory markers after 7 days of treatment with either celecoxib or diclofenac. No significant differences in reduction were observed between the 2 groups. This may be in line with the findings of the present study in which patients treated with either celecoxib or diclofenac showed a significant reduction in depressive symptoms by week 3, although those who received celecoxib showed greater reduction by week 6. In another study, Abbasi et al 39 measured serum levels of IL-6 in patients with MDD who received either celecoxib or placebo as an adjuvant therapy to sertraline. They reported significant association between decrease in serum levels of IL-6 and improvement of depressive symptoms in those who received celecoxib. This further supports the influence of COX-2 inhibitors on the underlying inflammatory processes responsible for the etiopathogenesis of depression.
We administrated celecoxib with a fixed daily dosage of 400 mg over a period of 6 weeks. In accordance with previous observations,12,14,39,40 this practice was well tolerated and safe, with no serious adverse events. Compared with nonselective inhibitors of both COX-1 and COX-2, such as diclofenac, selective COX-2 inhibitors are believed to cause fewer GI adverse events. 41 Even though there have been several reports on the increased incidence of cardiovascular events among users of COX-2 inhibitors,42,43 we did not observe such adverse events, which may be a result of the short duration of the current study, low dosage of celecoxib administered, and the relatively small number of patients investigated. Interestingly, the results of a recent meta-analysis indicated that compared with placebo, celecoxib increases the risk of both serious vascular events and nonfatal acute myocardial infarction. However, no significant differences were found in this regard between celecoxib and naproxen, a nonselective inhibitor of COX-1 and COX-2. 44 The authors suggested that because of the clinical insignificance of these potential adverse effects, the benefits of celecoxib still outweigh the risk of cardiovascular events.
Even though the present study has several advantages, such as the double-blind, controlled design, its limitations should be addressed to prevent overgeneralization of its findings. First, the sample size was relatively small. This made it impossible to perform subgroup analyses and assessment of the probable role of different clinical features such as the tumor stage, therapies used, and their complications. Second, depression is known to be a chronic disorder with a very high probability of relapse. 45 Hence, the true long-term effects of the agents administered here are not clear because of the short follow-up duration of this study. This may also apply to the side effects that may be observed with greater frequencies in the long term. Third, because we did not investigate the molecular basis of depression and the probable mechanisms responsible for the antidepressive effects of the agents used here, it is not possible to investigate the probable causative relationships. It would be beneficial to evaluate the serum levels of proinflammatory cytokines at baseline and during the course of the study.
Conclusion
In conclusion, celecoxib seems to possess superior antidepressive effects compared with diclofenac in breast cancer patients with mild to moderate depression. Further studies with larger sample sizes, longer duration of follow-up, and assessment of the molecular basis of the responsible mechanism are warranted to further explore the benefits of this practice.
Footnotes
Acknowledgements
This study was Dr Pantea Arya’s postgraduate thesis toward the Iranian Board of Psychiatry. The current study complies with contemporary laws and regulations in Iran.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Tehran University of Medical Sciences to Prof Shahin Akhondzadeh (Grant No: 24350). The funding organization had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript and the decision to submit the paper for publication.