
Abstract
Introduction
Heart failure (HF) is a major public health problem. 1 In the United States, approximately 5.1 million individuals have HF, with an estimated cost of $30.7 billion in 2012. 1 It is predicted that the prevalence of HF will increase to more than 8 million individuals in 2030. 1 Among Medicare beneficiaries, HF is the most frequent principal diagnosis on hospital discharge and accounts for the most common diagnosis for readmission. 2 The 30-day all-cause readmission rates among Medicare patients from 2004 to 2006 have remained around 23%. 3 A similar trend is found within the Veterans Affairs (VA) Health Care System, with 30-day all-cause readmission rates unchanged at 22.5% in 2002 and 2006. 4 A prospective analysis of the Organized Program to Initiate Life-Saving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) registry, which is a hospital-based quality improvement program and Internet-based registry for patients with HF, revealed that 36.2% of patients with HF experience death or rehospitalization within 60 to 90 days following HF hospitalization. 5
Management of patients with HF through specialized clinics has been associated with a reduction in hospital readmission, along with improved medication adherence and titration efficacy to evidence-based HF therapies.6,7 In older patients, providing home visits or increasing frequency of follow-up post-HF admission decreases readmission rates. 8 Most recently, Hernandez et al 9 showed that hospitals with a higher rate of follow-up within 7 to 14 days of HF hospitalization discharge experienced a decreased risk of 30-day rehospitalization, suggesting that a quality improvement intervention that provides early follow-up for patients with HF would enhance quality of care and lower the cost of hospitalization. However, there is still little evidence of the impact of HF posthospitalization management on all-cause mortality. In an effort to reduce HF readmission rates in our institution, we developed a fixed-duration, comprehensive, multidisciplinary HF postdischarge management clinic program of approximately 3 months in duration. Our clinic program has focused visits with specified goals and standardized documentation to identify HF etiology and precipitating factors, optimize titration of evidence-based HF medications, enhance patient education for sodium and fluid restriction, and improve medication adherence. The objective of this study was to evaluate the effect of the new HF posthospitalization management clinic on the rate of 90-day HF readmission and all-cause mortality in patients who were recently discharged from a HF hospitalization and received care in the clinic as compared with historical controls.
Methods
Study Design
We conducted a retrospective cohort study using data from the electronic health records at the Veterans Affairs Greater Los Angeles Healthcare System (VAGLAHS).
Patient Population
Patients with a primary diagnosis of HF during index hospitalization who were discharged alive from VAGLAHS were the target population for inclusion. Electronic medical records were used to identify patients with a principal discharge diagnosis of HF of ICD-9 code 428. Patients excluded were those who died during the index hospitalization, those whose emergency department visit did not result in admission, and those without a documented principal diagnosis of HF during the index admission.
Intervention Group
The HF postdischarge management (HF-PDM) clinic was established in July 2010 at VAGLAHS. Patients who had a principal discharge diagnosis of HF of ICD-9 code 428 and actually received care in the HF-PDM clinic between July 2010 and August 2012 were included in the intervention group. No other changes were made in our clinic referral process during the study period.
Patients are enrolled into this multidisciplinary clinic by referral from discharge physicians and case managers, with the goal of being seen within 1 to 2 weeks after their HF hospitalization discharge. Discharge physicians and case managers were initially slow to make referrals because of lack of awareness of our clinic. However, referral rates gradually improved. The clinic program is fixed in duration, over approximately 10 to 12 weeks. Within an average of 6 clinic visits, patients are seen by a physician assistant/nurse practitioner, a clinical pharmacist specialist, and a nurse case manager, with care overseen by an attending cardiologist who specializes in the management of patients with HF and was present at each clinic for immediate consultation. Tables 1 and 2 summarize the purpose, goals, and structure of the clinic. The initial consultation, conducted by the physician assistant, focuses on determination of HF etiology and precipitating factors of the HF admission. In subsequent visits, the patient’s progress and medication regimen are assessed by the clinical pharmacist using patient interview, physical assessment, and review of laboratory tests; therapeutic adjustments are made, with close monitoring and follow-up consultations scheduled. The pharmacist also prevents or resolves any drug-drug interactions, adjusts HF medications based on renal function, and educates patients on medication adverse effects. The nurse case manager educates patients on lifestyle modifications, including dietary counseling for sodium and fluid restriction, and medication adherence. The final assessment with the physician assistant and nurse case manager ensures that patients receive follow-up with the appropriate outpatient clinic and referral for other diagnostic or therapeutic procedures, such as repeat echocardiogram or consultation for an implantable cardioverter-defibrillator or implantation of cardiac resynchronization device, if suitable. All clinic visits were documented in the electronic medical record using standardized clinic note documentation templates.
Design of Multidisciplinary HF Posthospitalization Clinic Program.
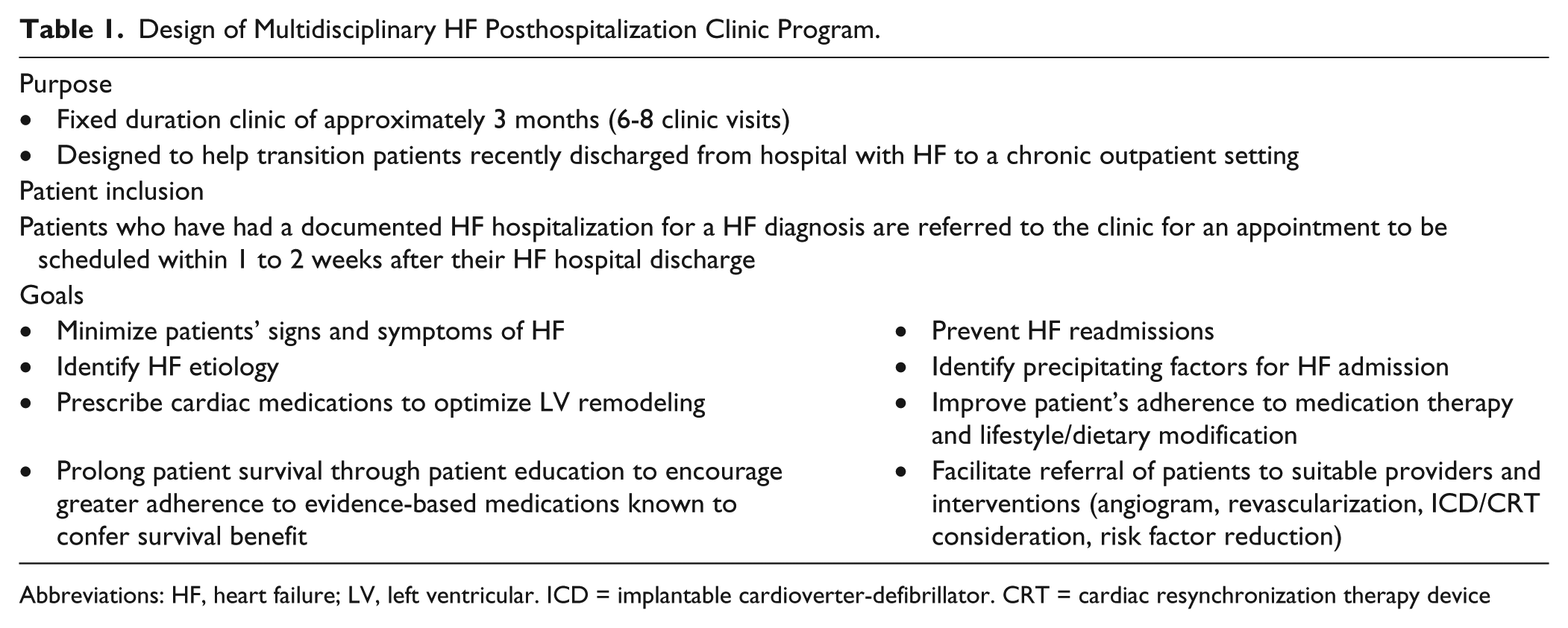
Abbreviations: HF, heart failure; LV, left ventricular. ICD = implantable cardioverter-defibrillator. CRT = cardiac resynchronization therapy device
Overview of HF-Post-Discharge Management Program Schedule. a
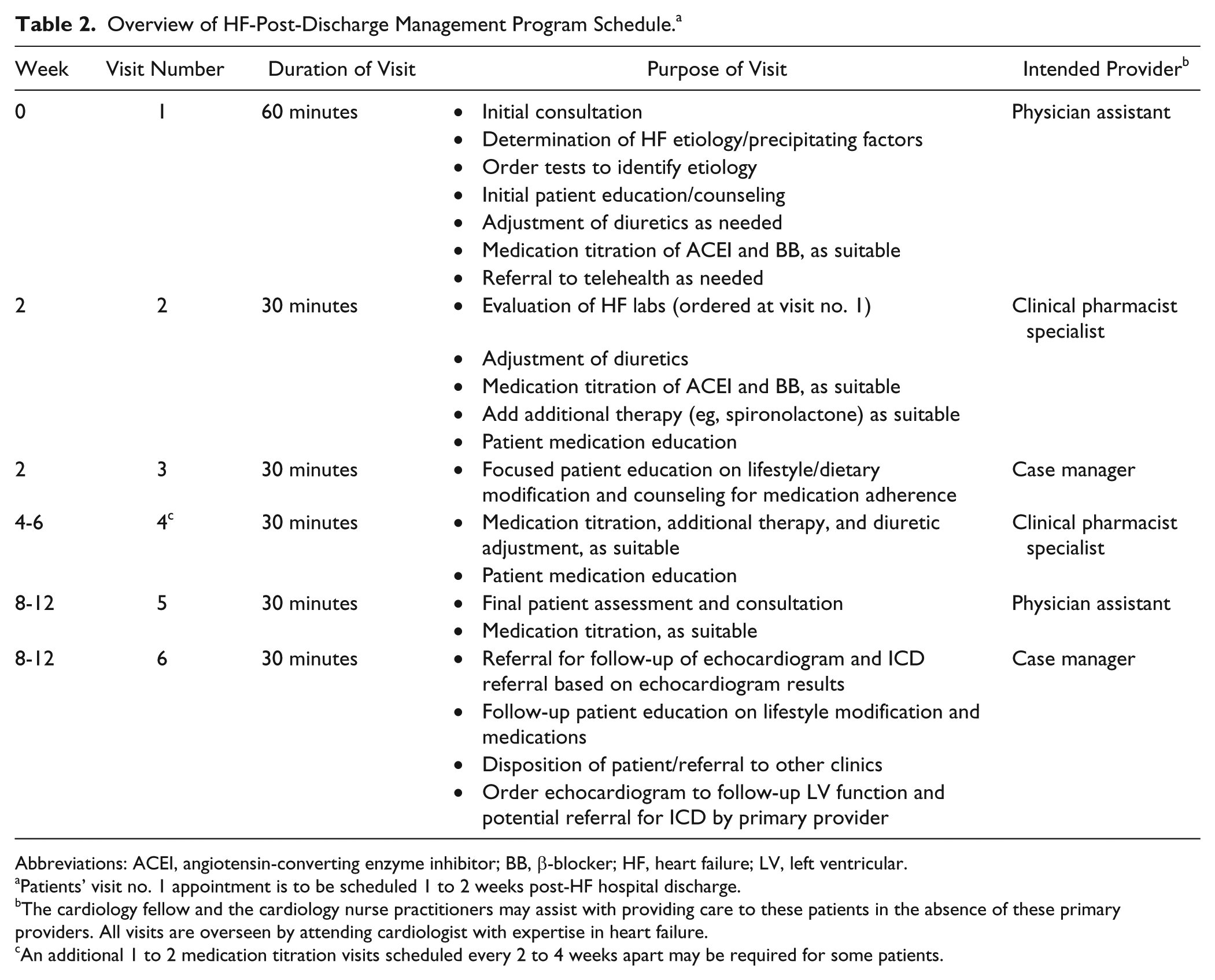
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; BB, β-blocker; HF, heart failure; LV, left ventricular.
Patients’ visit no. 1 appointment is to be scheduled 1 to 2 weeks post-HF hospital discharge.
The cardiology fellow and the cardiology nurse practitioners may assist with providing care to these patients in the absence of these primary providers. All visits are overseen by attending cardiologist with expertise in heart failure.
An additional 1 to 2 medication titration visits scheduled every 2 to 4 weeks apart may be required for some patients.
Control Group
Patients with a primary diagnosis of HF during index hospitalization who were discharged alive from VAGLAHS between January 2009 and December 2009 were included as historical controls. To avoid patient duplication, patients with a HF admission in 2009 but who received care in the HF-PDM clinic were excluded from historical controls and included in the clinic group.
Study End Points
The primary clinical outcome was 90-day HF readmission rates following discharge from the index HF hospitalization. Readmission was defined as a documented clinical diagnosis of HF decompensation made by the attending physician at the time of discharge after hospital admission. Electronic medical records were used to confirm the clinical diagnosis of HF during the rehospitalization. The time to first readmission was calculated as the number of days between the index discharge date and the readmission date for up to 90 days. We chose 90-day readmission rather than a shorter time frame for readmission for our primary outcome because our clinic program intervention lasted approximately 10 to 12 weeks. Secondary clinical outcomes included 90-day all-cause mortality and a composite of HF readmission and all-cause mortality within 90 days.
Statistical Analysis
Patient characteristics were compared between groups using χ2 or Fisher’s exact test for categorical and the t test for continuous variables. The primary outcome of 90-day HF readmission was compared using the χ2 test, and hazard ratios (HRs) with 95% CIs were calculated. Secondary clinical outcomes were compared similarly.
A multivariate Cox-proportional hazard model was constructed to assess for avoidance of HF readmission, survival, and a composite of event-free survival. The time to first readmission, death, and a composite of first readmission or death were compared using the log-rank test. Based on differences in baseline characteristics from the univariate analysis and known clinically relevant patient characteristics,4-6 adjustments in the Cox model were made for age, ejection fraction, hospital length of stay, baseline sodium, admission functional class, HF etiology, chronic kidney disease history, precipitating factors, discharge use of evidence-based β-blocker, evidence-based angiotensin-converting enzyme inhibitor, and hydralazine. Analyses were conducted using STATA 11.2 (StataCorp, College Station, TX). P values <0.05 were considered statistically significant. The institutional review board of VAGLAHS and Western University of Health Sciences approved the study.
Results
A total of 277 patients were included in the study—133 control patients and 144 clinic patients; 162 patients were identified to have an ICD-9 428 principal diagnosis from January through December 2009 for the historical control group, and 147 patients who received care in the HF-PDM clinic from July 2010 through August 2012 were identified for the clinic group. Among them, 29 control group patients were excluded: 1 patient died during index HF hospitalization, 2 patients were seen in the HF-PDM clinic after subsequent hospitalizations and were included in the clinic group, 18 cases were not admissions, and 8 patients did not have a principal discharge diagnosis of HF. Three clinic group patients were excluded because they were not hospitalized for HF but enrolled in the HF-PDM clinic per referring provider request. The median time from discharge to the first HF-PDM clinic visit was 19 calendar days (interquartile range = 13-26 days). All clinic patients had an initial consultation with the physician assistant, and 68% of patients had at least 1 visit with the clinical pharmacist for medication titration. The mean number of clinic visits was 3.8 visits per patient.
Patients were primarily male and elderly, with a mean age of 69 years in the control group and 72 years in the clinic group. The 2 groups were well balanced with respect to most characteristics, with a few exceptions (Table 3). More clinic patients had a nonischemic HF etiology (P < 0.001) and precipitating factors of dietary noncompliance (P < 0.001), arrhythmia (P = 0.003), and infection (P = 0.003), whereas control patients had a higher rate of unknown or undocumented HF etiology (P < 0.001) and precipitating factors (P < 0.001). Fewer control patients were discharged on hydralazine compared with the clinic group (11% vs 22%, respectively; P = 0.01). There was no difference in the time to the first primary care or cardiology clinic visit between groups (median: control, 15 days; clinic, 14 days; P = 0.21).
Baseline Characteristics.
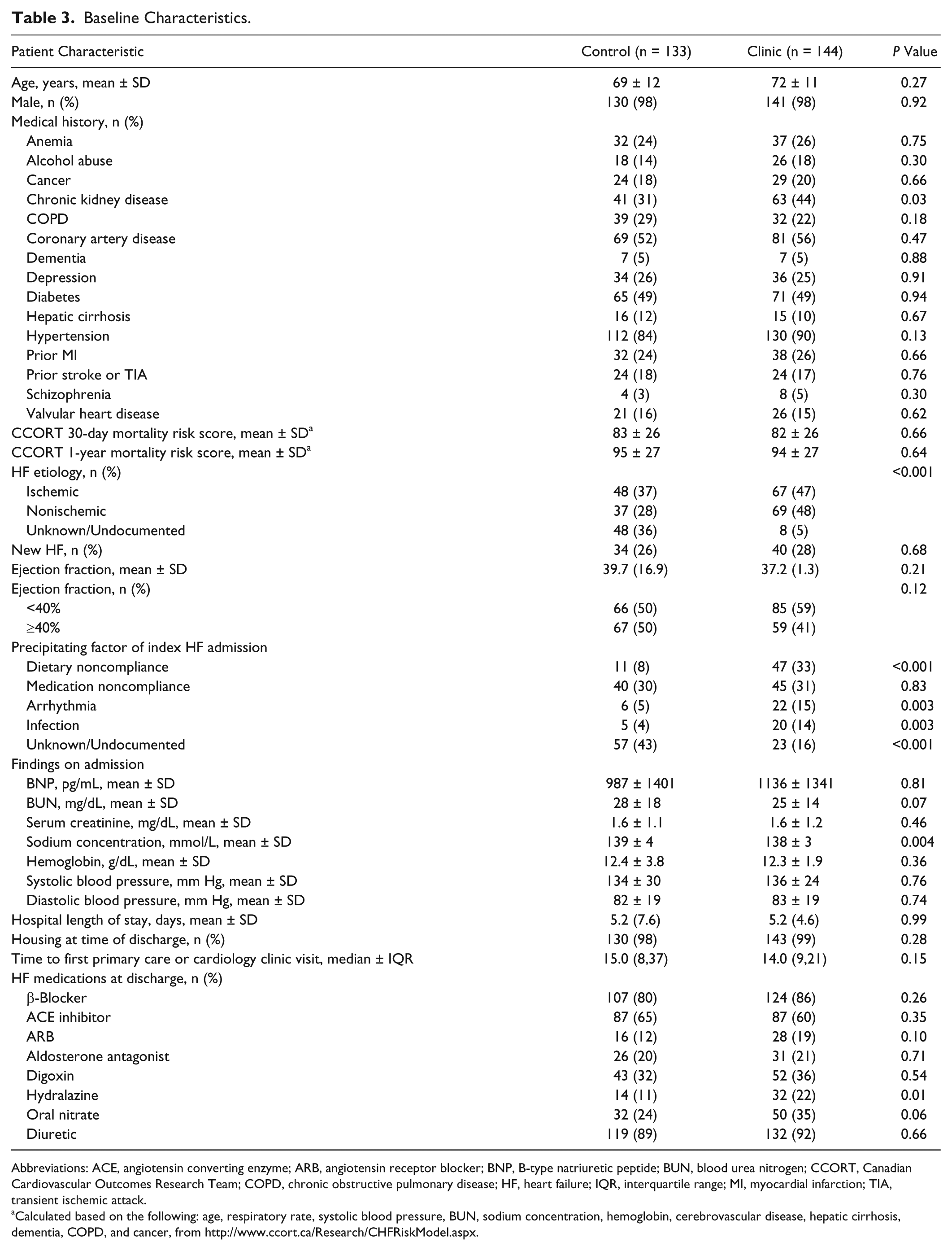
Abbreviations: ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; BNP, B-type natriuretic peptide; BUN, blood urea nitrogen; CCORT, Canadian Cardiovascular Outcomes Research Team; COPD, chronic obstructive pulmonary disease; HF, heart failure; IQR, interquartile range; MI, myocardial infarction; TIA, transient ischemic attack.
Calculated based on the following: age, respiratory rate, systolic blood pressure, BUN, sodium concentration, hemoglobin, cerebrovascular disease, hepatic cirrhosis, dementia, COPD, and cancer, from http://www.ccort.ca/Research/CHFRiskModel.aspx.
Among the 277 patients, 31 patients in the control group (23.3%) and 11 patients in the clinic group (7.6%) were readmitted for HF within 90 days of index hospitalization discharge (unadjusted HR = 0.30; 95% CI = 0.15-0.59; P < 0.001; Table 4; Figure 1A). There was no difference in all-cause mortality within 90 days between the control (5.3%) and clinic (1.4%) groups (unadjusted HR = 0.26; 95% CI = 0.05-1.25; P = 0.064). When combined, 38 control patients (28.6%) and 13 clinic patients (9.0%) experienced either HF readmission or all-cause mortality within 90 days of discharge (unadjusted HR = 0.28; 95% CI = 0.15-0.52; P < 0.001; Figure 1B).
Unadjusted and Adjusted a Rates of Clinical Outcomes.
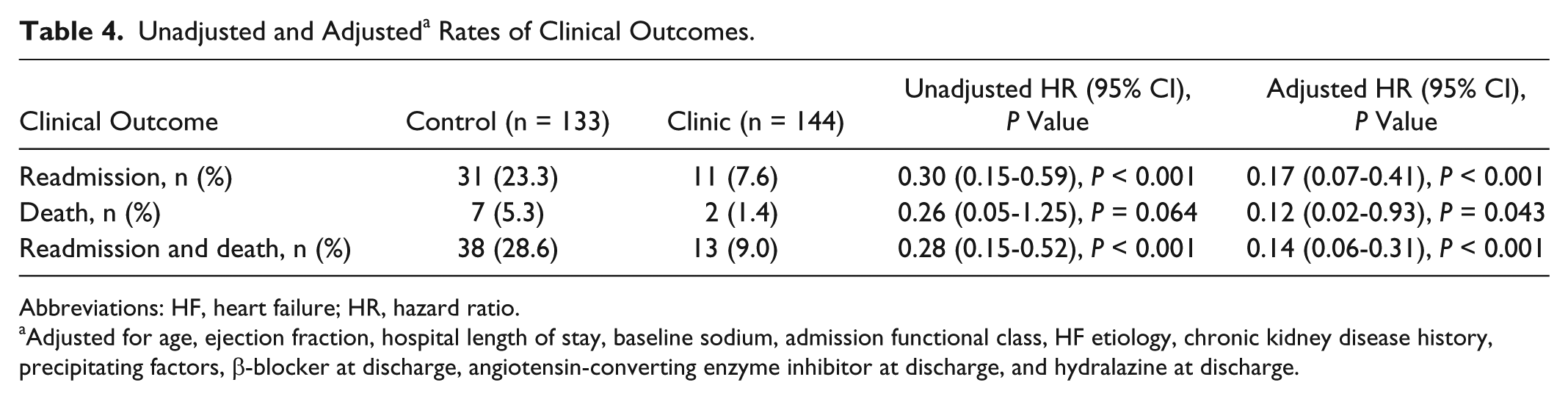
Abbreviations: HF, heart failure; HR, hazard ratio.
Adjusted for age, ejection fraction, hospital length of stay, baseline sodium, admission functional class, HF etiology, chronic kidney disease history, precipitating factors, β-blocker at discharge, angiotensin-converting enzyme inhibitor at discharge, and hydralazine at discharge.
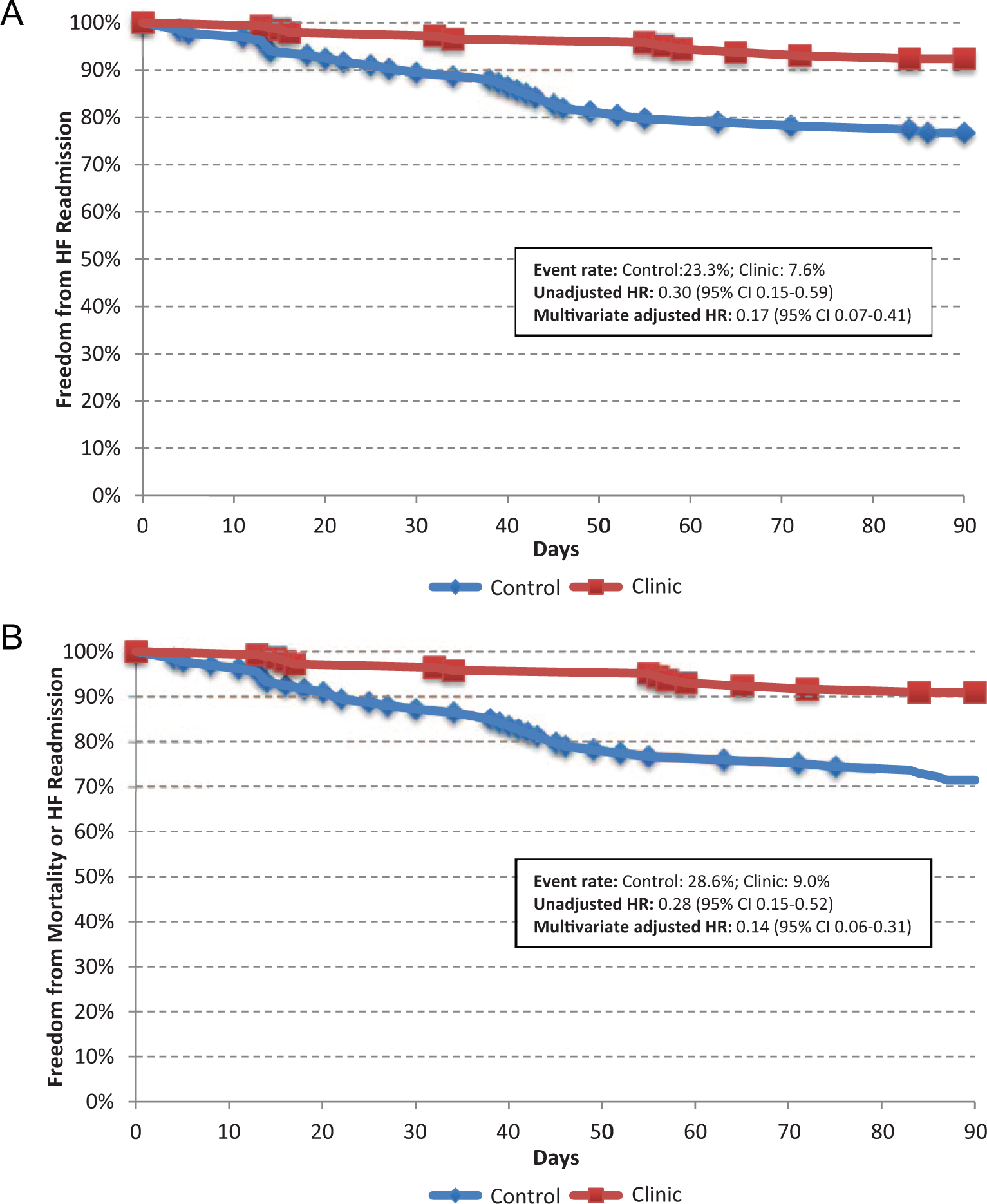
A. Kaplan-Meier estimates of the primary outcome of heart failure readmission at 90 days. B. Kaplan-Meier estimates of the composite outcome of heart failure readmission or all-cause mortality at 90 days.
After adjusting for potential confounders, the clinic group maintained a significantly lower risk of HF readmission compared with the control group (HR = 0.17; 95% CI = 0.07-0.41; P < 0.001). After adjustment, the risk of all-cause mortality was significantly lower in the clinic group compared with the control group (HR = 0.12; 95% CI = 0.02-0.95; P = 0.043). The combined outcome of 90-day HF readmission or all-cause mortality continued to be significantly lower in the clinic group compared with the control group after adjustment for potential confounders (HR = 0.14; 95% CI = 0.06-0.31; P < 0.001; Table 4).
Discussion
We found that a multidisciplinary HF-PDM clinic was associated with a significant reduction in the rate of 90-day HF readmission, such that for every 7 patients enrolled in our HF-PDM clinic program, 1 patient avoided a HF readmission. We also found a significant reduction in 90-day mortality and combined 90-day HF readmission or all-cause mortality, so that for every 6 patients enrolled in our HF clinic program, 1 patient avoided either HF readmission or death.
Specialized HF clinics that do not specifically focus on the postdischarge period have significantly reduced hospital readmission rates, and some have also reduced mortality.6,8,10-12 The few studies that have focused on interventions in the immediate postdischarge period after HF admission have found reduced all-cause readmissions at 6 months to 2 years of follow-up.13-16 With no difference between groups in the time to first primary care or cardiology clinic visit following hospital discharge, we found a significant reduction with our program within 90 days postdischarge. The reduction in HF readmissions that our study was associated with was greater than those found in previous studies. The difference in magnitude may be a result of varying outcomes and design between studies, the extended duration of our intensive intervention, or the smaller sample size of our study. Our study evaluated more immediate outcomes, within 90 days of discharge, and focused on HF-related readmissions. Although our multidisciplinary approach shared similarities with these previous studies, our HF-PDM clinic was an intensive, team-based, 10- to 12-week, fixed-duration program, and patients were scheduled to receive care from all the providers, rather than see providers as needed or on consultation. Our findings highlight the benefit of receiving comprehensive care from a team of providers with expertise in HF management. In addition, interventions with more frequent initial visits scheduled every 1 to 2 weeks, similar to our program, have been found to be associated with reduced HF readmissions. 17
Apart from targeting prescription and titration of HF medications that are known to improve HF functional class and reduce mortality and HF readmissions, another focus of the clinic was to identify precipitating factors that led to the index hospitalization. Current HF guidelines recommend addressing these factors as a way of limiting recurrent admission in patients with HF.18,19 In our clinic group, precipitating factors were identified and documented significantly more often than for control patients because clinic practitioners were guided to do so on standardized clinic note documentation templates. Furthermore, because our clinic prioritized identification of the etiology of the HF, etiology was also identified significantly more often in our clinic compared with our control patients. By intensifying efforts to determine the etiology of the HF condition in our clinic program, clinicians facilitated timely ordering of diagnostic tests, such as coronary angiography, or referrals for arrhythmia consultation to further guide patient management, which may also have contributed to the reduction in 90-day HF readmission and all-cause mortality.
In addition to the need for follow-up, the timing of the clinic visit has also proven crucial. The importance of prompt outpatient follow-up stems from the fact that patients with HF are at high risk for mortality and hospital readmission shortly following discharge from HF hospitalization. An inverse relationship between follow-up within 7 to 14 days of HF hospitalization discharge and the rate of 30-day readmission has been demonstrated. 6 Hospitals with higher rates of early follow-up had a reduction in the risk of readmission compared with hospitals that had lower rates of early follow-up (20.9% vs 23.3%, P < 0.001). 6 The median time for first follow-up in the HF-PDM clinic was 19 days following discharge for the HF hospitalization. This present study supports the need for early outpatient follow-up after a HF discharge by demonstrating a reduction in the risk of HF readmission. Unlike previous studies, this study evaluated HF readmission rather than readmission for any cause or presentation to the emergency room without admission. By focusing on HF readmission, the impact of the clinic on rehospitalization for HF decompensation could be isolated. This study also had a long timeframe with which readmission was assessed. For clinic patients, the 90-day timeframe included the time from discharge until completion of clinic visits because the clinic lasts an average of 10 weeks.
Other studies have determined that HF clinics are associated with improved patient adherence and titration efficacy with evidence-based HF therapies.6,20 The reduction in HF readmission associated with this multidisciplinary clinic may be partly a result of these factors, and this is being investigated further in relation to our clinic.
The present study has limitations. Because this was an observational study, there is potential for selection bias and confounding. However, despite lack of randomization, our groups were well balanced. This is likely a result of capturing the target population of patients discharged after a hospitalization for HF in both groups. There was also a potential underestimation of readmission and mortality because events occurring outside the VA system may not be completely captured in our electronic medical record system. This underestimation, however, would affect both groups equally. Given the veteran population, the majority of patients in the study were male. It is possible that results may differ in a female population. In addition, our sample size was relatively small. Even though we had 95% power to detect the difference we found in 90-day HF readmission, our CIs are not precise because of the current sample size. Finally, because of slow clinic referrals and patients who failed to show up for their appointments in the beginning, the span of time taken to collect an equivalent number of patients in the clinic group was longer. We collected data on the clinic group over 2 years to match the number of patients included in the control group, which was examined over a span of 1 year. In conclusion, the multidisciplinary HF-PDM clinic was associated with a significant reduction in 90-day HF readmission. For every 7 patients enrolled in our HF posthospitalization management clinic program, 1 patient avoided a HF readmission. Whereas our results support previous studies, this multidisciplinary, fixed-duration clinic with comprehensive patient care is unlike the design of previously studied clinics. As such, the results suggest that patients with HF will significantly benefit from receiving care from a specialized, multidisciplinary clinic shortly following their HF hospitalization. The specific impact of the pharmacist on HF readmission and mortality in team-based HF patient care would benefit from further study.
Footnotes
Acknowledgements
We would like to acknowledge Reginald Villacorta, MS, who was a paid statistical consultant for the study. We would also like to acknowledge the following clinic providers: Jeffrey Garcia, PA-C, Maria Greco, RN, as well as the cardiology clinic nurse practitioners, cardiology fellows, clinic nurses, and clinic clerks.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.