
Abstract
Introduction
Amiodarone, a Vaughan-Williams class III antiarrhythmic drug, exhibits negative chronotropic and dromotropic effects. In the acute care setting, these properties make it an ideal agent for the treatment of ventricular and supraventricular tachyarrhythmias. In nonemergency situations, the dosing of amiodarone can be divided into 2 phases: a loading dose of 150 mg given over 10 minutes, following by the initiation of a maintenance phase infusion. One of the major limitations to the use of amiodarone is the adverse effect profile, with hypotension as the primary dose-limiting effect of the intravenous formulation. Amiodarone has been shown in both controlled and open-label studies to have an incidence of hypotension of approximately 15.6%.1,2 In a patient population that is already hemodynamically unstable, further fluctuations in blood pressures could correlate with negative outcomes. In addition, several publications allude to excipients in the amiodarone formulation as contributors to the hypotensive effect.3-5 However, these studies only evaluated short-term infusions, and fail to evaluate the mean arterial pressure (MAP) throughout the standard 24-hour maintenance phase infusion. Two excipients, benzyl alcohol and polysorbate 80, have been shown to exert negative hemodynamic effects in both animal and human studies. A study performed on dogs evaluated the cardiovascular and hemodynamic effects of the combination form of amiodarone (amiodarone plus polysorbate) and amiodarone alone. The study demonstrated that the combination formulation caused a 60% drop in mean blood pressure. The authors concluded that the observed decrease in MAP was related to the vasodilatory and negative inotropic effects of polysorbate 80. 6 Two studies have compared the Cordarone (Wyeth Pharmaceuticals Inc) formulation containing polysorbate 80/benzyl alcohol with the Amio-Aqueous (Academic Pharmaceuticals Inc) formula, which is free of the 2 excipients. The Amio-Aqueous formula infusion resulted in an increase of peripheral vascular resistance, compensating for an initial decrease in myocardial contractility. Inversely, the Cordarone formulation containing the aforementioned excipients resulted in vasodilation and hypotension.7,8 Neither of these studies evaluated the hypotensive effect beyond the first 6 hours of the infusion.
Because of limited information on the hemodynamic effect of amiodarone during the maintenance phase infusion, we sought to evaluate the change in MAP when utilizing an intravenous amiodarone formulation containing polysorbate 80 and benzyl alcohol compared with a formulation that does not contain these agents.
Methods
Until March 31, 2014, the study institution utilized the intravenous formulation of amiodarone containing benzyl alcohol and polysorbate 80 (Bioniche Pharma USA) as part of the hospital formulary (control group). Beginning in April of 2014, the study institution began utilizing a different formulation (Nexterone®, Baxter Healthcare Corporation USA) for the maintenance infusions (cyclodextrin group). All bolus doses contained the benzyl alcohol/polysorbate 80 formulation for the duration of this study.
Patients admitted to the study institution between January 1, 2012 and October 31, 2014 were screened for inclusion in the study. To maintain a simple study design, increase the homogeneity of the study population, and optimize the generalizability of the study results, the study population consisted of patients who were 18 years or older and were being treated with intravenous amiodarone for atrial fibrillation. Patients had to receive a 150-mg amiodarone bolus dose prior to the initiation of the maintenance phase infusion. Patients were excluded if they were diagnosed with sepsis and/or septic shock prior to initiation, if they were receiving vasopressors at the start of the study period, or if there was inadequate documentation of blood pressure readings in the electronic medical record throughout the first 24-hours of the maintenance phase infusion.
This was an institutional review board–approved, retrospective cohort analysis conducted at a large, tertiary care, academic medical center. The primary outcome was defined as the relative change in MAP as measured during 4 different 6-hour time blocks post-infusion initiation, utilizing the last measured blood pressure prior to receiving amiodarone and comparing it with the lowest measured blood pressure during each period. All data were gathered from the electronic medical record. Secondary endpoints included time to lowest recorded systolic blood pressure, number of patients who required fluid boluses for the treatment of hypotension, the initiation of vasopressors, as well as the total intravenous amiodarone dose received during the study period.
The design of the trial, the approval of the statistical analyses, the review and interpretation of the data, the writing of the manuscript, and the decision to publish the manuscript involved all investigators listed. All authors had full access to the data and vouch for the accuracy and completeness of the data and the analyses.
Statistical Analysis
The initial sample size was chosen to be sufficiently large to conduct a mixed analysis between 2 independent groups utilizing a 3:1 ratio of controls (polysorbate 80/benzyl alcohol formulation) to cases (cyclodextrin formulation). The primary endpoint was analyzed with the use of a mixed analysis of variance in order to determine the change between subjects across the 4 time points. Bonferroni tests and between-group t-tests were employed in a post hoc fashion to explain the significant main effect of MAP across time. In addition, baseline variables were added as covariates to the mixed analysis of variance model to account for any potential confounding. Categorical variables were analyzed using a chi-square or Fisher’s exact test as appropriate. Normally distributed continuous variables were analyzed using an independent-samples t-test. Non-normally distributed continuous variables were analyzed using a Mann-Whitney U test. Normality of continuous variables was assessed using skewness and kurtosis statistics. Any skewness or kurtosis above an absolute value of 2 assumed a non-normal distribution. Normally distributed variables were expressed as means and standard deviations while non-normal variables were expressed using medians and interquartile ranges. Analyses were performed with the use of SPSS software, version 22 (IBM Corporation, Armonk, NY). All reported P values were 2-sided. A P value of less than 0.05 was considered statistically significant.
Results
A total of 160 patients were included in the final analysis. Of these 160 patients, 120 received the formulation containing the polysorbate 80/benzyl alcohol excipients, and 40 received the formulation without these excipients. Baseline characteristics for the 2 groups are listed in Table 1. The mean age of the cyclodextrin and control groups was 68.7 ± 10.7 and 69.2 ± 11.0 years, respectively. The majority of patients were male, and approximately 98% were Caucasian. Of the evaluated comorbid disease states, only the presence of heart failure and hypertension differed between the 2 study groups. Approximately 20% of patients were current smokers. In addition, the baseline MAP before the initiation of the maintenance phase infusion was higher in the control group.
Baseline Patient Demographics.
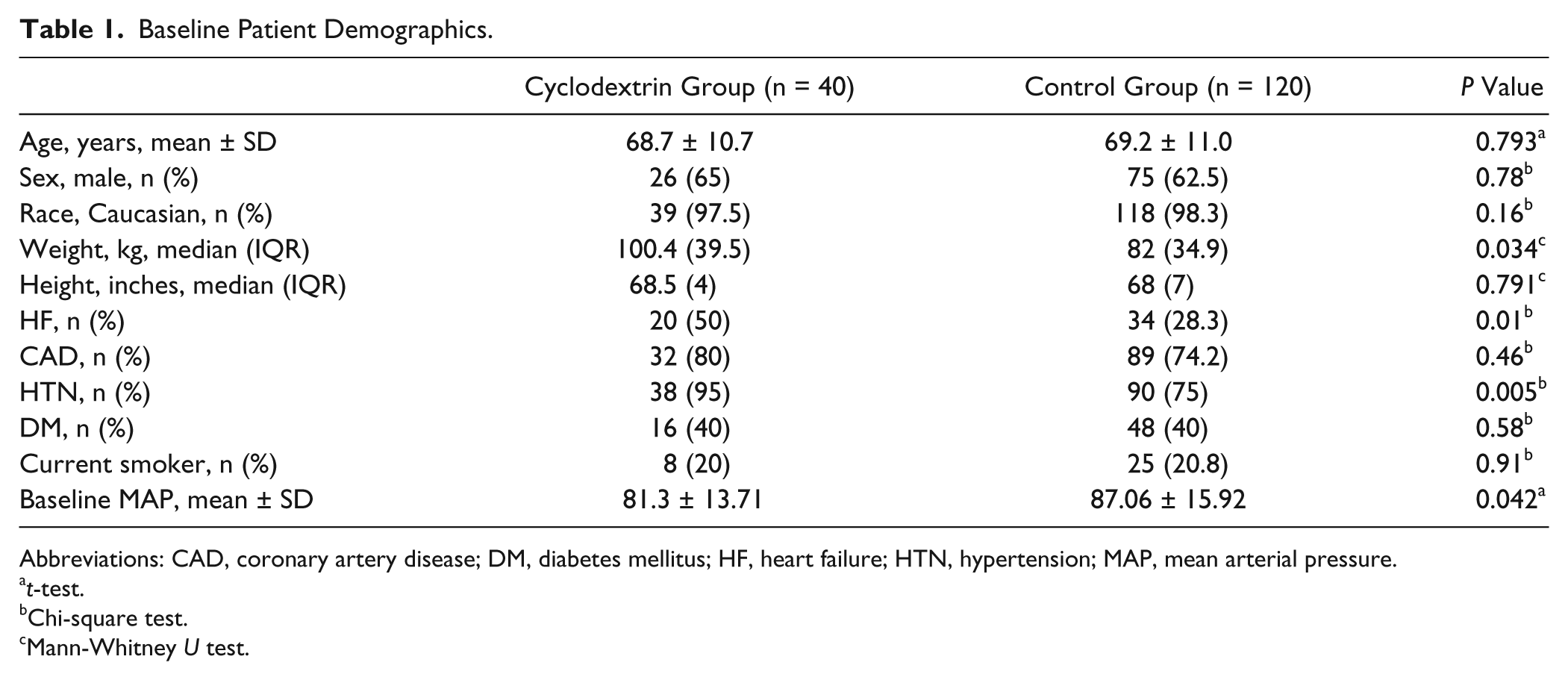
Abbreviations: CAD, coronary artery disease; DM, diabetes mellitus; HF, heart failure; HTN, hypertension; MAP, mean arterial pressure.
t-test.
Chi-square test.
Mann-Whitney U test.
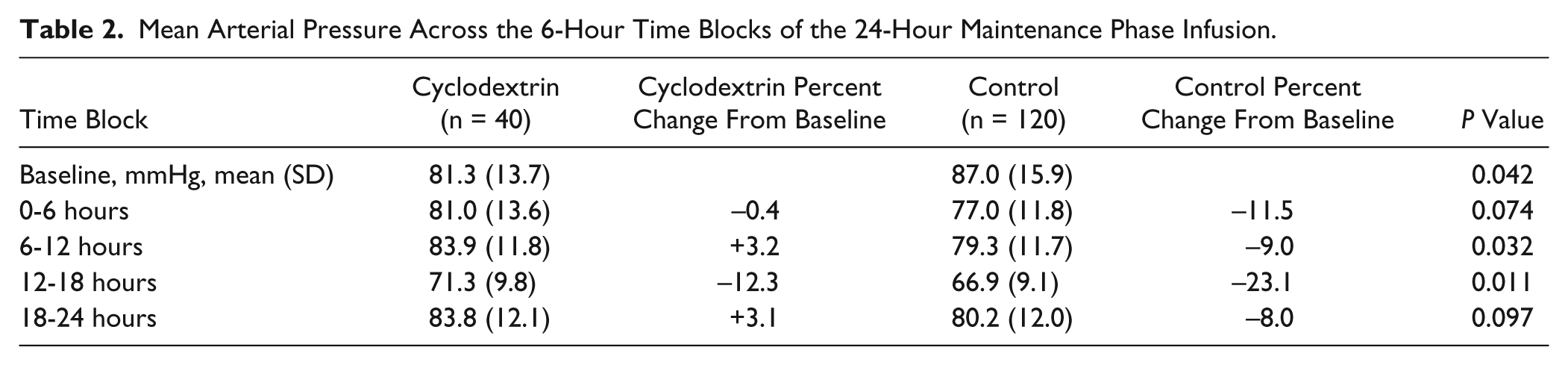
Based on the results of a mixed analysis of variance conducted to compare MAP between the 2 different amiodarone formulations across 4 time blocks (0-6 hours, 6-12 hours, 12-18 hours, and 18-24 hours), there was a significant interaction (P < 0.001) between formulation of amiodarone and time (Figure 1). In addition, when we added gender, age, ethnicity, HF (heart failure), CAD (coronary artery disease), HTN (hypertension), DM (diabetes mellitus), smoking status, fluid bolus, vasopressor, weight, and baseline MAP differences to the model as covariates, the formulation of amiodarone received remained the only statistically significant interaction (P < 0.001). A post hoc analysis revealed that there was a significant change in MAP in the 0- to 6-hour observation (P < 0.001) and the 12- to 18-hour observation periods (P < 0.001). Also, at the baseline, 12-hour, and 18-hour time points, there was a statistical difference when the 2 groups were compared (Table 2).
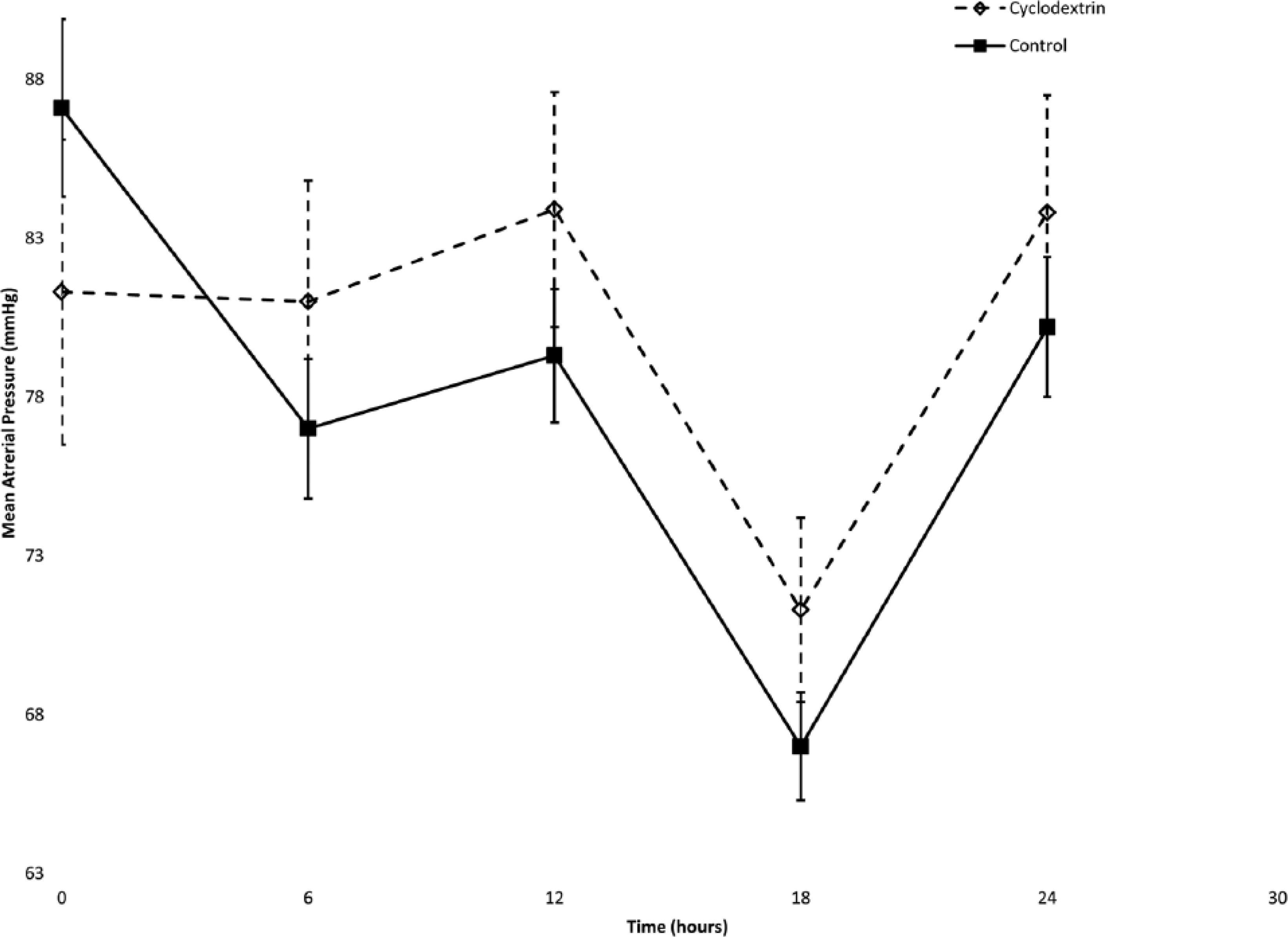
The average lowest mean arterial pressure during each time block compared for both amiodarone formulations.
Mean Arterial Pressure Across the 6-Hour Time Blocks of the 24-Hour Maintenance Phase Infusion.
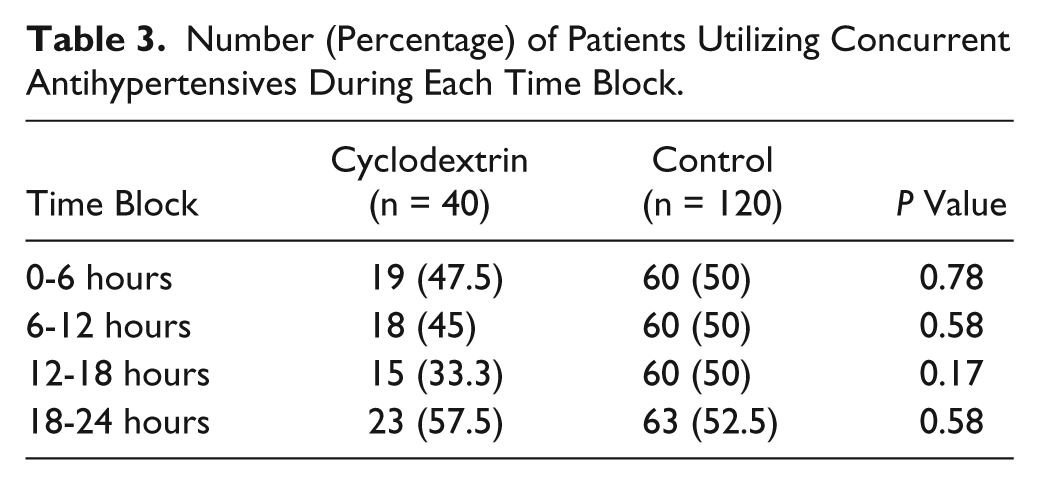
Antihypertensives could have an effect on the change in MAP when used concurrently with intravenous amiodarone. When evaluating the concurrent antihypertensive use across both groups during each 6-hour time block, there was no statistical difference found in the number of patients who used these agents during each time block (Table 3).
Number (Percentage) of Patients Utilizing Concurrent Antihypertensives During Each Time Block.
The secondary outcomes are summarized in Table 4. In both groups, the lowest recorded systolic blood pressure occurred during the 6- to 12-hour time block (9.3 hours postinfusion for the cyclodextrin group; 8.92 hours for the control group; P = 0.783). Patients in the control formulation group required a significantly higher number of fluid boluses for the treatment of hypotension (P < 0.001). Though it did not reach statistical significance, more control formulation group patients were initiated on vasopressors (P = 0.33). There was no difference found in the total amiodarone dose received by either group.
Secondary Objectives.
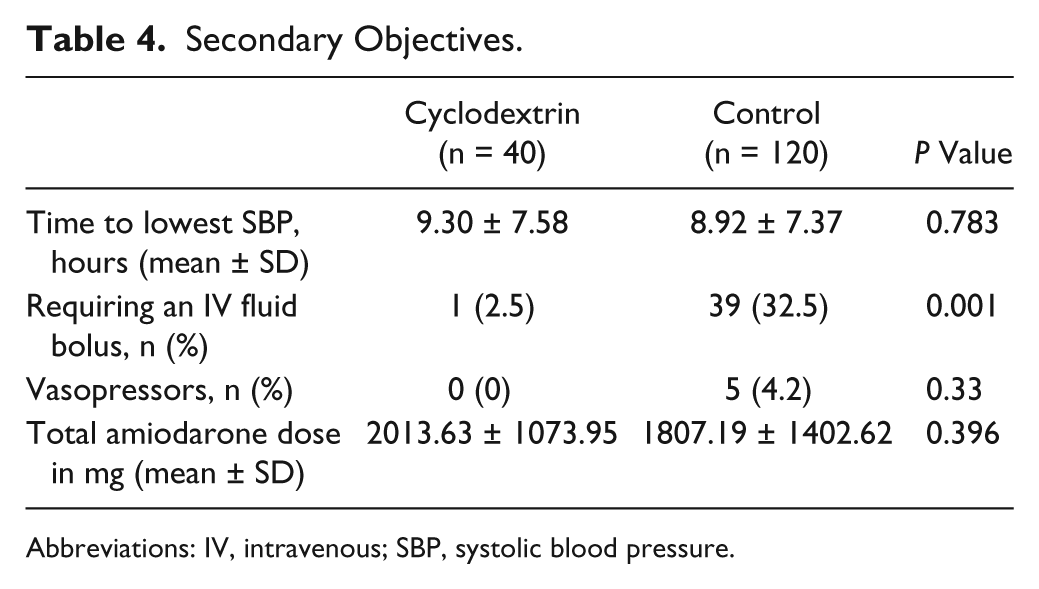
Abbreviations: IV, intravenous; SBP, systolic blood pressure.
Discussion
The effects of hypotension on cardiac patients could have detrimental effects, including increased morbidity and mortality. Historically, significant hypotension associated with amiodarone was related to the higher administration rates utilized during a bolus infusion. However, our study revealed that hypotension can persist throughout the duration of the 24-hour maintenance phase infusion, and that the formulation, specifically the excipients in the formulation, may play a significant role in perpetuating this hypotension. Unlike previous animal and human studies, we evaluated the effects of intravenous amiodarone throughout the entire duration of the maintenance phase infusion. Previous trials evaluated short-term infusions, with the longest study in humans evaluating up to 15 minutes into the maintenance phase infusion; thus, little data were available regarding whether the effects of the excipients persisted. 9 Another study evaluating this hypotensive effect in dogs only evaluated the first 6 hours of the infusion. 10 Our study was able to show that the hemodynamic effects of intravenous amiodarone could extend beyond the first 6 hours of the maintenance phase infusion and may be attributable in part to the excipients used in the formulation.
The trend in MAP was similar between the 2 groups throughout the duration of the study, as shown in Figure 1. In the 6- to 12-hour time block, as well as the 18- to 24-hour time block, there was an increase in MAP as compared with baseline in the cyclodextrin-containing group. Over every time block, the polysorbate 80/benzyl alcohol formulation not only significantly lowered the MAP from baseline but was also found to be consistently lower than the cyclodextrin group. The significant drop seen during the 12- to 18-hour time block may be attributed to the accumulation of drug, but further investigation into this is warranted.
Patients with chronic comorbidities could require various antihypertensive medications of differing potencies. The control group was found to have a higher MAP at baseline, while the cyclodextrin group was found to have a higher incidence of hypertension. Both these differences could confound the findings of this study; relative decreases in the MAP of the control group may be more pronounced secondary to the higher baseline pressure, and it may have been more difficult to lower the blood pressure in the cyclodextrin group. Because of the statistically significant differences seen in the baseline incidence of heart failure and hypertension in the study population, the effect of concurrent antihypertensive regimens with different mechanisms of action on MAP throughout the maintenance phase infusion should be considered. Regimens included angiotensin-converting enzyme inhibitors, angiotensin-receptor blockers, β-blockers, calcium channel blockers, nitrates, and diuretics. These nonstandardized regimens could account for the discontinuation rates seen in the cyclodextrin group between the 6- to 12-hour and 12- to 18-hour time blocks. Although the number of patients in this study who discontinued antihypertensives was small, this would warrant further evaluation in larger studies.
One patient between the first (0-6 hours) and second (6-12 hours) observation periods, and 3 patients between the second and third (12-18 hours) observation periods in the cyclodextrin group had their antihypertensive medications withheld, as seen in Table 4. No patients in the control group required discontinuation. The reasons for discontinuation were not clear; however, this could have been to attenuate a decrease in MAP. Although no statistical differences were found in the number of antihypertensives used by each group during each of the time blocks, future larger studies could evaluate these findings.
The results of our study are consistent with current published literature that evaluated the hemodynamic effects of the excipients, polysorbate 80 and benzyl alcohol.3-5 Several other limitations exist in our study, including a limited patient population at a single institution, small sample size, as well as the potential for bias due to a lack of nursing documentation in the electronic medical record. Although the number of patients who utilized concurrent antihypertensive agents during each time block was similar between groups, the effect of various longer acting agents over the study period cannot be ruled out.
Conclusion
There was a significant difference in MAP between the formulations of amiodarone across the 24-hour maintenance phase infusion. There was a significant difference between formulations in regards to the average MAP during each time block, and the number of patients receiving the cyclodextrin formulation was associated with fewer treatments for hypotension.
Footnotes
Acknowledgements
The authors would like to acknowledge Shane Baker for his contribution to data collection.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Rowe is a member of the speakers bureau for The Medicines Company. All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.