
Abstract
Gabapentin was approved in the United States in 1993 for the treatment of seizure disorder, but since that time, it has increasingly been prescribed for a number of other conditions. It is a γ-aminobutyric acid (GABA) analog that is structurally related to GABA, but it does not bind to the GABA receptors or affect GABA binding, uptake, or degradation.1,2 Although gabapentin does not interact with the GABA neurotransmitter system itself, it does exert a neuronal inhibitory effect by blocking voltage-dependent calcium channels, resulting in central nervous system effects. 1 The pharmacokinetics of gabapentin include peak plasma concentrations 3 hours after oral ingestion, but these concentrations can be variable because of a dose-limited, interindividual absorption process. 2 Its elimination is renal, and its half-life ranges between 5 to 7 hours in patients with normal renal function. Historically, gabapentin has been used with little concern because of the limited number of reported adverse effects and drug interactions. Because of its central nervous system effects, gabapentin has been evaluated in the treatment of substance abuse and withdrawal and alcohol withdrawal and dependence. 3 Prudent evaluation regarding the long-term safety and efficacy when using gabapentin for an off-label indication is important. It was initially marketed as an agent that had no significant risk for dependence or abuse—hence its lack of classification as a scheduled medication. However, those with a history of substance abuse may misuse any medication, particularly those that affect the dopaminergic reward system. 4 A survey in the United Kingdom was performed to determine the prevalence of misuse of GABA analogues (the broader class to which gabapentin belongs). 5 This online survey was distributed to residents between 16 and 59 years old. The researchers received 1500 completed surveys reporting an overall 1.1% rate of gabapentin misuse in the general population. Only 13.1% of those using these medications were doing so as legitimately prescribed. Clearly, misuse of gabapentin is a much more common problem than was previously appreciated.
To identify potential abuse issues regarding gabapentin a PubMed literature search for articles published in English from 1993 through October 2015 was performed using the search terms gabapentin, addiction, dependence, and withdrawal. Additional references were identified from a review of literature citations. This article summarizes all identified case reports and studies regarding patients who abused, became dependent on, and/or experienced withdrawal from gabapentin.
Abuse and Dependence
There have been 8 case reports published that address the abuse and dependence of gabapentin. All these cases occurred in patients with a previous history of drug abuse or dependence. Four of the patients who abused alcohol were in an age range from 33 to 67 years4,6,7 (Table 1); 3 of the patients were started on gabapentin for the treatment of pain; the fourth patient was taking the medication to reduce his cravings for alcohol. Half of the patients reported that they had been sober for more than 2.5 years.6,7 The dosages of abuse were between 3600 and 7200 mg of gabapentin per day, with 3 of the patients reporting that they self-titrated to these amounts. Two of the patients reported symptoms of delirium, sedation, confusion, and fatigue while taking the medication.4,7
Gabapentin Abuse and Dependence Cases.
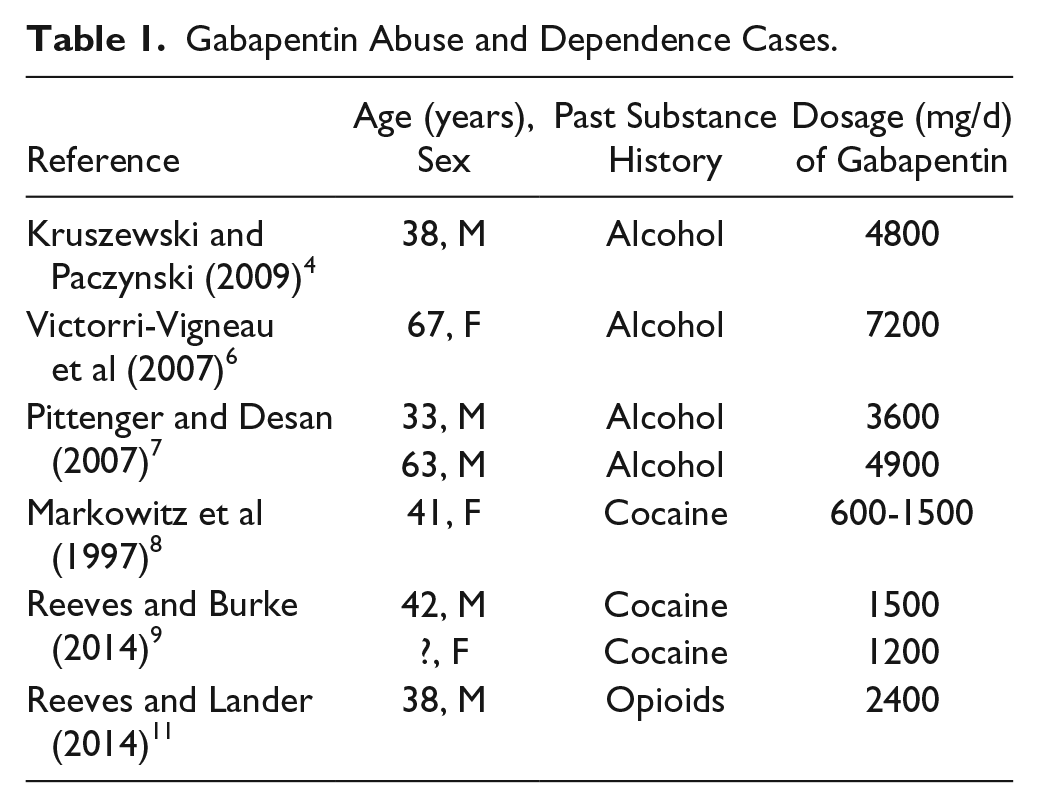
Separate studies reported a total of 8 cases of gabapentin misuse in patients who had a history of cocaine abuse.8-10 The first had posttraumatic stress disorder; the cocaine abuse ended simultaneously with the initiation of gabapentin to treat cocaine withdrawal. 8 Two of the patients abused gabapentin and quetiapine. They reported sedation and euphoric effects or similar but weaker effects compared with a cocaine high when the combination was used. 9 The remaining 5 patients were inmates in a Florida state correctional institution who attested to the diversion of gabapentin. 10 This correctional institution had discovered that several inmates frequently requested early refills of their gabapentin, and a following recall of all prescription bottles revealed that less than 20% was in the possession of the intended patient.
Gabapentin abuse has also been reported in patients taking opioids for the potentiation of desired opioid effects. One reported case described a 38-year-old man who abused illicit opioids. 11 Buprenorphine/naloxone was part of his rehabilitation treatment; however, he appeared intoxicated during a visit with his probation officer. The patient stated that he added gabapentin to his opioid regimen to maintain a “high.” This medication combination provided him with a desirable relaxed, euphoric effect.
Two studies have been conducted to further evaluate the presence of opioid and gabapentin cross-abuse. The National Health Service of the United Kingdom conducted an optional survey in substance misuse clinics. It focused on gabapentin abuse among methadone users. 12 Patients who attended the clinic for 3 months or greater were eligible, and 129 surveys were returned. In all, 22% of the patients reported abusing either gabapentin or pregabalin and took methadone concurrently; 76% of the patients admitted to taking 1 of these 2 medications to become intoxicated and 38% to potentiate the effects of the methadone. Similarly, a quality-improvement project in the United States queried 162 patients who received treatment in an inpatient opioid detoxification program. 13 It was found that 22% of the patients were prescribed gabapentin, and 40% of them took higher-than-prescribed doses. An additional 13% of patients took diverted gabapentin. Overall, 22% of the patients in the detoxification program misused gabapentin.
These cases and surveys demonstrate a potential for gabapentin misuse, especially in patients who have or are currently using or abusing other substances.
Withdrawal
There have been several case reports in the literature describing the potential effects of withdrawal from gabapentin14-25 (Table 2). The onset of withdrawal symptoms in each of these patients began between 12 hours and 7 days after cessation of use, with the majority of cases occurring between 24 and 48 hours. More than half of the reported withdrawal symptoms consisted of some form of agitation. Confusion and disorientation were the next most frequent symptoms, occurring in 45% of the cases. Other common symptoms included diaphoresis (36%), nonspecified gastrointestinal symptoms (23%), tremor, tachycardia, hypertension (each at 18%), and insomnia (14%). Whereas the above symptoms represent the majority of cases, individual cases have also presented as akathisia, catatonia, and seizures.22-24 In addition, one new born baby experienced withdrawal secondary to her mother’s use of gabapentin during the pregnancy. 25
Gabapentin Withdrawal Cases.
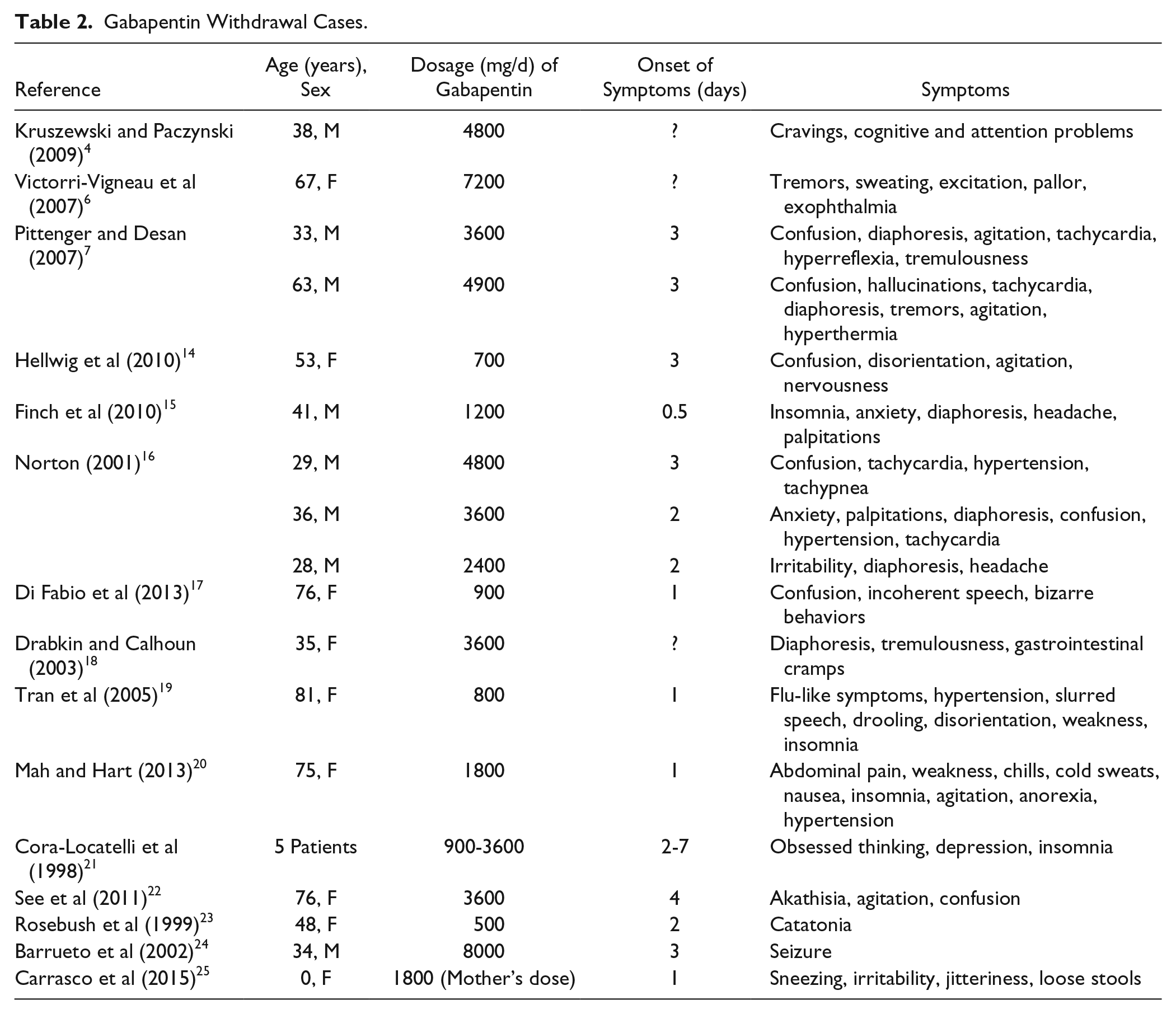
The treatment of these withdrawal states varied among the cases. In those patients for whom gabapentin was reinitiated (n = 18), all symptoms resolved.4,7,14-16,19-22,24,25 This included those patients who failed other therapies; 6 patients were administered a benzodiazepine and 2 others a benzodiazepine plus haloperidol.7,14,20,22-25 Out of 8 of these patients, 7 did not experience control of their withdrawal symptoms from this treatment regimen. Benztropine was tried in one patient who presented with catatonia, but it proved to be ineffective. 23 One patient who received haloperidol for her unusual behaviors did experience relief of her symptoms. 7 In the patient who experienced a seizure, phenobarbital and phenytoin were effective in controlling further seizures. 24 Also, 3 of the patients were not treated with any medications, and over time, their symptoms dissipated.6,18,21
There is a potential for a variety of withdrawal symptoms after gabapentin is discontinued, whether abruptly or after a taper. Reinstitution of gabapentin was effective in alleviation of withdrawal symptoms.
Discussion
These case reports have raised some concern regarding the abuse and withdrawal potential of gabapentin. On average, the patients were taking more than 3000 mg/d (600-8000 mg/d). A history of alcohol or substance abuse appears to be an important part of a patient’s past medical history when evaluating for the risk of addiction and abuse.
Gabapentin use has been reported among opioid abusers to enhance the effects of the opioids. Some cocaine users have used it—either alone or with quetiapine—as a substitute for cocaine or to avoid cocaine withdrawal symptoms.
The awareness of abuse and diversion of gabapentin is increasing. In the Florida state prison system, gabapentin use has been significantly restricted following an internal investigation. 9 In Scotland, it has been shown that the number of prescriptions increased significantly greater than the number of patients for whom the medication was prescribed (years 2002-2011). 26 The rate of patients enrolled in misuse of drug services who reported taking gabapentin was 5.2%. Postmortem toxicology examinations reported that gabapentin was detected in more than 3% of all cases, with 75% of them showing concurrent opioid use. 26 A cohort study reported a 165% increase in gabapentin use over a 1-year period, with 15% using gabapentin to obtain a high. 27 Users of gabapentin were also more likely to abuse oxycodone (18.3%), buprenorphine (18.4%), and benzodiazepines (21%) compared with nonusers. It was noted that gabapentin was obtained from physicians 52% of the time and drug dealers 36% of the time. 27
Although alcoholism or substance abuse may help predict abuse potential, it does not appear to be as strong of a factor when determining if a patient may withdraw from gabapentin. The onset of withdrawal symptoms correlate with the elimination half-life of the medication. 2 Of interest, benzodiazepines do not appear to control symptoms of gabapentin withdrawal in the majority of cases. Reinstitution of gabapentin was effective in alleviation of withdrawal symptoms.
Conclusion
There have been numerous documented cases of gabapentin abuse, dependence, and withdrawal. Despite its potential for abuse, gabapentin is currently not a controlled substance. Even though it could be considered as a treatment option for alcohol and substance abuse, it is important to monitor for drug-seeking and abuse behaviors, such as a need for early refills. Health care providers need to be aware of this risk in their patients and monitor for signs of abuse, dependence, and withdrawal.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.