
Abstract
Introduction
Acute postoperative pain after total knee arthroplasty (TKA) surgery is a common clinical problem. Wylde et al 1 found that 58% of patients reported moderate to severe pain on postoperative day 1. Severe pain following TKA hinders mobilization, resulting in likelihood of developing immobility-related complications such as venous thromboembolism. Appropriate postsurgical pain control helps promote healing, faster patient mobility, and decreased length of hospitalizations. 2 Other potential benefits of optimal postsurgical pain control include improving patient satisfaction and reducing opioid medication use and its associated adverse effects.1,3
There are several methods of pain control, including various regional techniques. These include single-injection and continuous peripheral nerve block or continuous intra-articular infiltration analgesia provided by infusion pumps, usually pain balls containing local anesthetics.4-6 Pain balls are elastomeric pumps that provide continuous pain relief by delivering a regulated flow of ropivacaine or other local anesthesia to a targeted surgical site or nerve via a catheter. Pain balls using the ON-Q Pain Relief System can provide pain relief for up to 5 days. 7 An adductor canal block (ACB) is an alternative technique that involves single or continuous injection of local anesthetic at the adductor canal. This leads to disruption of predominantly sensory as opposed to motor nerves. ACBs have been shown to better preserve quadriceps muscle strength and early functional recovery compared with femoral nerve blocks but without significant changes in postoperative pain and opioid use. Ropivacaine and bupivacaine are common local anesthetics used in pain ball devices or ACBs.8-10
In comparison to its related compound, ropivacaine, bupivacaine hydrochloride (HCl) is more toxic toward the central nervous system and cardiovascular system. 11 Bupivacaine liposome (EXPAREL; bupivacaine liposome injectable suspension; Pacira Pharmaceuticals, Inc, Parsippany, NJ) is an extended-release delivery system composed of a phospholipid bilayer encapsulating bupivacaine. This liposomal bilayer functions as a drug carrier and allows a slow and controlled release of the medication. The lipid formulation also provides a better safety profile when compared with its nonlipid counterpart, with fewer systemic cardiac side effects and central nervous system reactions characterized by dizziness, somnolence, and syncope as well as an overall lower incidence of adverse events. Common adverse events (incidence = 2%-10%) include pruritis, pyrexia, hypotension, and headache. 12 Bupivacaine liposome is currently Food and Drug Administration (FDA) approved as a single-dose administration of 266 mg in soft-tissue procedures, such as bunionectomy and hemorrhoidectomy. It yielded significant reduction in pain intensity in patients undergoing hemorrhoidectomy and bunionectomy, assessed by area under the curve of the numerical rating scale, compared with placebo for up to 24 hours.12,13 Bupivacaine liposome has seen increased use for postoperative pain control in TKA at our institution, but efficacy outcomes have not been compared with those of pain ball devices. There are also few studies analyzing the cost of using bupivacaine liposome. 14 The objectives of this study were to evaluate the impact of ACB with liposome bupivacaine versus 0.1% ropivacaine pain ball (RPB) on postoperative pain control, pain medication use, and associated costs.
Methods
This institutional review board–approved study was a single-centered, retrospective review comparing a cohort of patients who received an ACB using bupivacaine liposome or RPB as postoperative analgesia following TKA, from February 2013 to June 2014. Patients in each cohort were manually matched in a 1:1 ratio by age and sex into either the bupivacaine liposome group or 0.1% RPB group. Medical data of patient demographics and patient-recorded pain scores were retrieved from our institution’s electronic medical record. Our financial billing system was used for all direct, indirect, and medication costs.
The study included all patients 18 years or older who had received at least a dose of bupivacaine liposome or pain ball infusion of 0.1% ropivacaine after TKA surgery. Patients were excluded if they received both interventions or had a recorded hypersensitivity reaction to ropivacaine or bupivacaine. Because there was no method of retrieving history of chronic pain or opioid use, these patients were not excluded from the study population. The primary endpoint was mean pain score over a 72-hour period or on patient discharge, whichever was earlier. Mean pain score was measured by the patient-reported 11-point Visual Analogue Scale (VAS). A score of 0 indicated no pain and a score of 10 indicated worst imaginable pain. Pain scores taken postsurgery were listed as time 0 hours, with subsequent pain scores recorded as the number of hours after the first pain score rating. Pain scores were averaged at fixed intervals as well as overall throughout the 72-hour period. Secondary endpoints included mean opioid consumption, mean nonopioid pain medication use, and total cost per patient case.
Pain balls delivered 0.1% ropivacaine using the ON-Q Pain Relief System. In the past, our institution used 0.2% ropivacaine in the pain balls; however, because of increased weakness and rates of falls from patients, the hospital anesthesia protocol switched to 0.1% ropivacaine. Because our institution predominantly used RPBs prior to the addition of bupivacaine liposome on our orthopedic surgery protocol, patients who received the 0.1% RPB were selected from the time period February 2013 to October 2013. The patients who received bupivacaine liposome were selected from the time period November 2013 to June 2014. The placement of the catheter for the ropivacaine continuous infusion was done in the adductor canal space via the Seldinger technique. A 20-gauge B Braun Stimplex catheter was placed through an 18-gauge needle. The bupivacaine liposome dose was administered between two surgeons or surgeon and anesthesiologist, with each physician injecting 15 mL of bupivacaine liposome in the adductor canal, for a total volume of 30 mL or a dose of 266 mg. Procedures were performed by 12 different surgeons throughout the study period.
For adjunctive pain relief, our institution’s multimodal approach includes options of oral pregabalin 50 mg preoperatively and then twice daily, extended release oxycodone 10 or 20 mg oral preoperatively and then every 12 hours, and methylprednisolone 125 mg preoperatively. Barring contraindications, all patients received intravenous (IV) acetaminophen 1000 mg, which was given intraoperatively every 8 hours for 3 days. Patients also had the option to receive ketorolac 30 mg every 6 hours for the first 48 hours, with the first dose given intraoperatively based on patient tolerability and renal function. Oral oxycodone 5 mg could be given every 3 hours for mild pain rated 1 to 4, and oral oxycodone 10 mg orally every 3 hours was given for moderate pain rated 5 to 7. These options are available as order sets to the physicians.
To accurately compare total and mean opioid use between the two groups, IV and oral opioid narcotics were converted to IV equivalent of morphine expressed in milligrams. Conversion was done via a Microsoft Excel opioid dose equivalent spreadsheet provided by Cadence Pharmaceuticals using the following formula: 0.33 (mg oral hydrocodone) + 0.33 (mg oral morphine) + 1.33 (mg oral hydromorphone) + 0.50 (mg oral oxycodone) + 0.05 (mg oral codeine) + 100 (mg IV fentanyl) + 6.67 (mg IV hydromorphone) + 0.12 (mg meperidine) + 1 (mg oral methadone). Fentanyl patches were converted to its equivalent daily IV fentanyl dose in milligrams and then converted to IV morphine. 15 This formula is used in practice at our institution. The mean and total dosages of other pain medications were also calculated via sum and average function in Microsoft Excel.
The cost analysis compared mean direct, indirect, medication, and total costs per patient case. Direct cost included all patient-specific costs associated with the surgery, including the medications used and the services provided. Indirect costs include non–patient-specific costs such as administrative and general facility costs. Cost of bupivacaine liposome versus RPB was also compared.
Student’s t tests were utilized to compare mean outcome variables between the two treatment groups. Total and mean IV morphine equivalents of opioid analgesics and nonopioid pain medications were also compared. Fisher’s exact test was used to compare nominal variables such as comorbidities. Statistical significance was determined at a P value of less than 0.05 between groups.
Results
There were a total of 357 patients who received TKA during the time period of February 2013 to June 2014. A total of 341 met inclusion criteria, with 16 patients excluded because they received both interventions. Of the 341 patients, 117 patients received bupivacaine liposome. To match both cohorts by age and sex evenly in a 1:1 ratio, 113 patients were excluded from the RPB group, and 6 were excluded from the bupivacaine liposome group (Figure 1). This yielded a total of 222 patients, with 111 patients in each cohort. Characteristics of excluded patients were similar to those of included patients (Supplementary Table 1 [available at http://aop.sagepub.com/content/by/supplemental-data]). For included patients, there were no significant differences in baseline demographics or mean preoperative pain scores (2.66 vs 2.81, P = 0.70). All patient demographic results are found in Table 1.
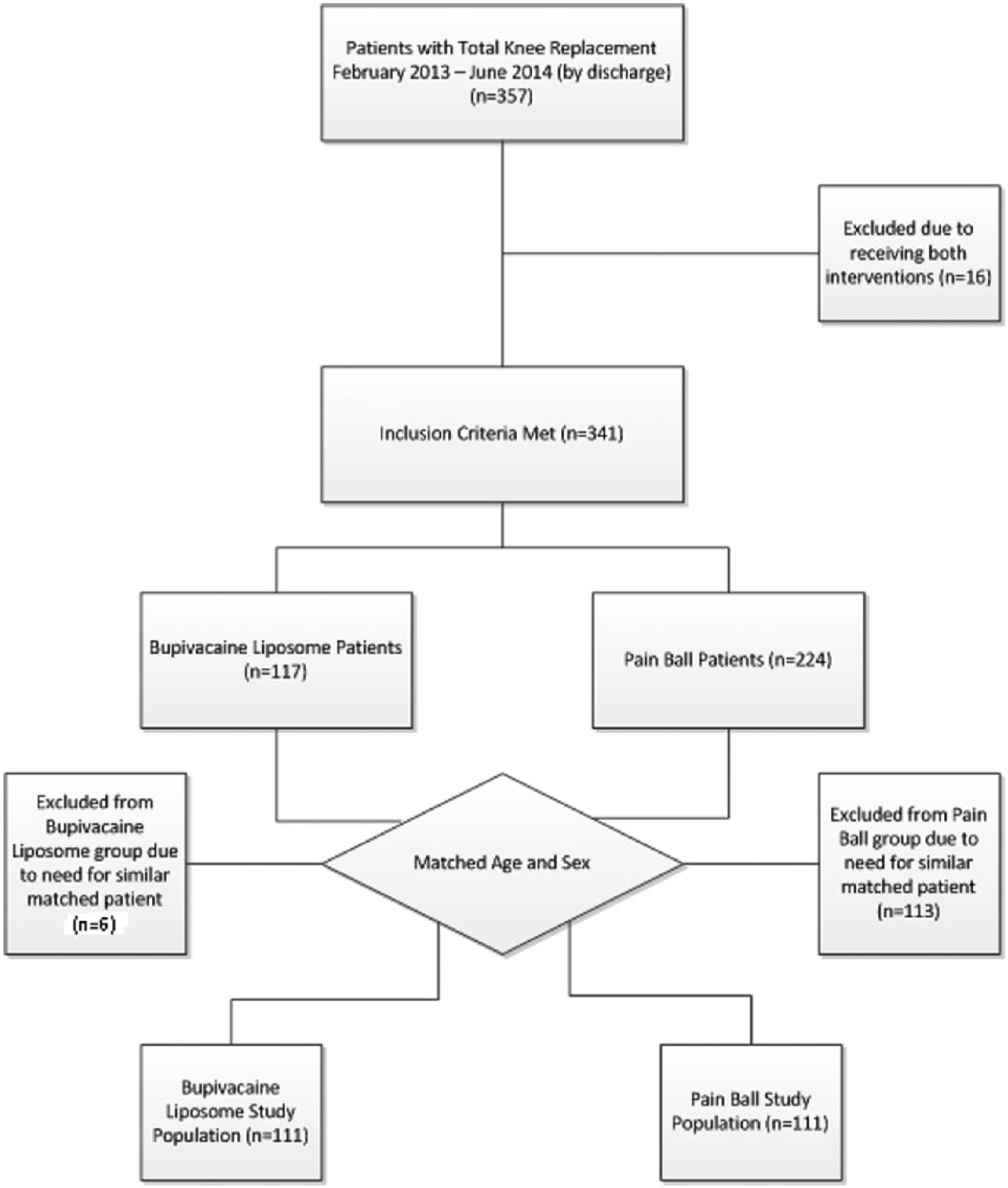
The figure shows the breakdown of patients included and excluded from the study.
Baseline Demographics of Bupivacaine Liposome and RPB Group.
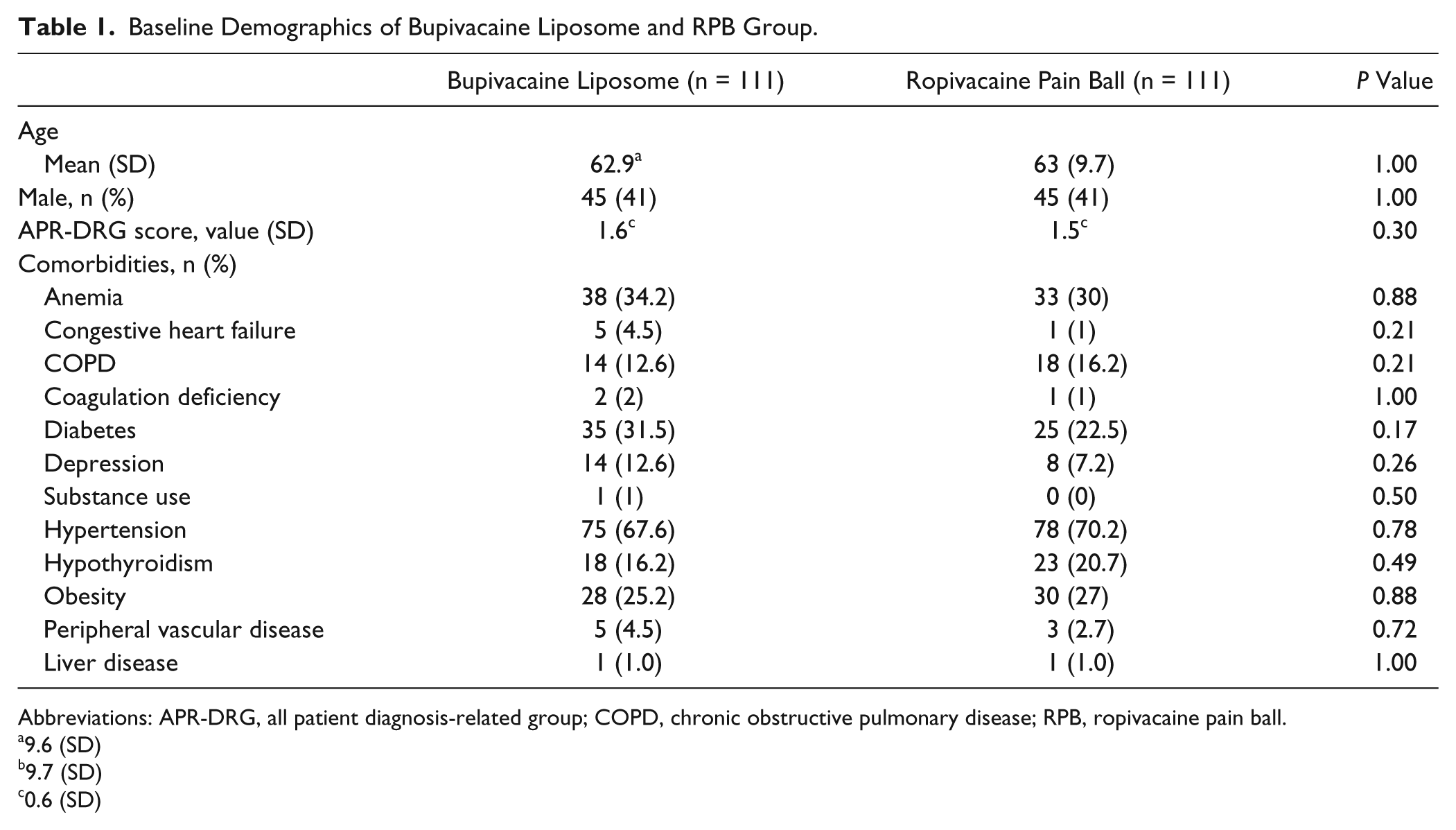
Abbreviations: APR-DRG, all patient diagnosis-related group; COPD, chronic obstructive pulmonary disease; RPB, ropivacaine pain ball.
9.6 (SD)
9.7 (SD)
0.6 (SD)
Mean pain scores between the bupivacaine liposome group and RPB group over the 72-hour period were 3.24 and 3.84, respectively (P < 0.001). Significantly lower mean pain scores were found in the bupivacaine liposome group during the first 36-hour interval postsurgery compared with the RPB group (overall 3.1 vs 4.0, respectively, P < 0.001), as shown in Figure 2. Pain scores from hours 37 to 72 were comparable (3.4 vs 3.6, respectively, P > 0.05).
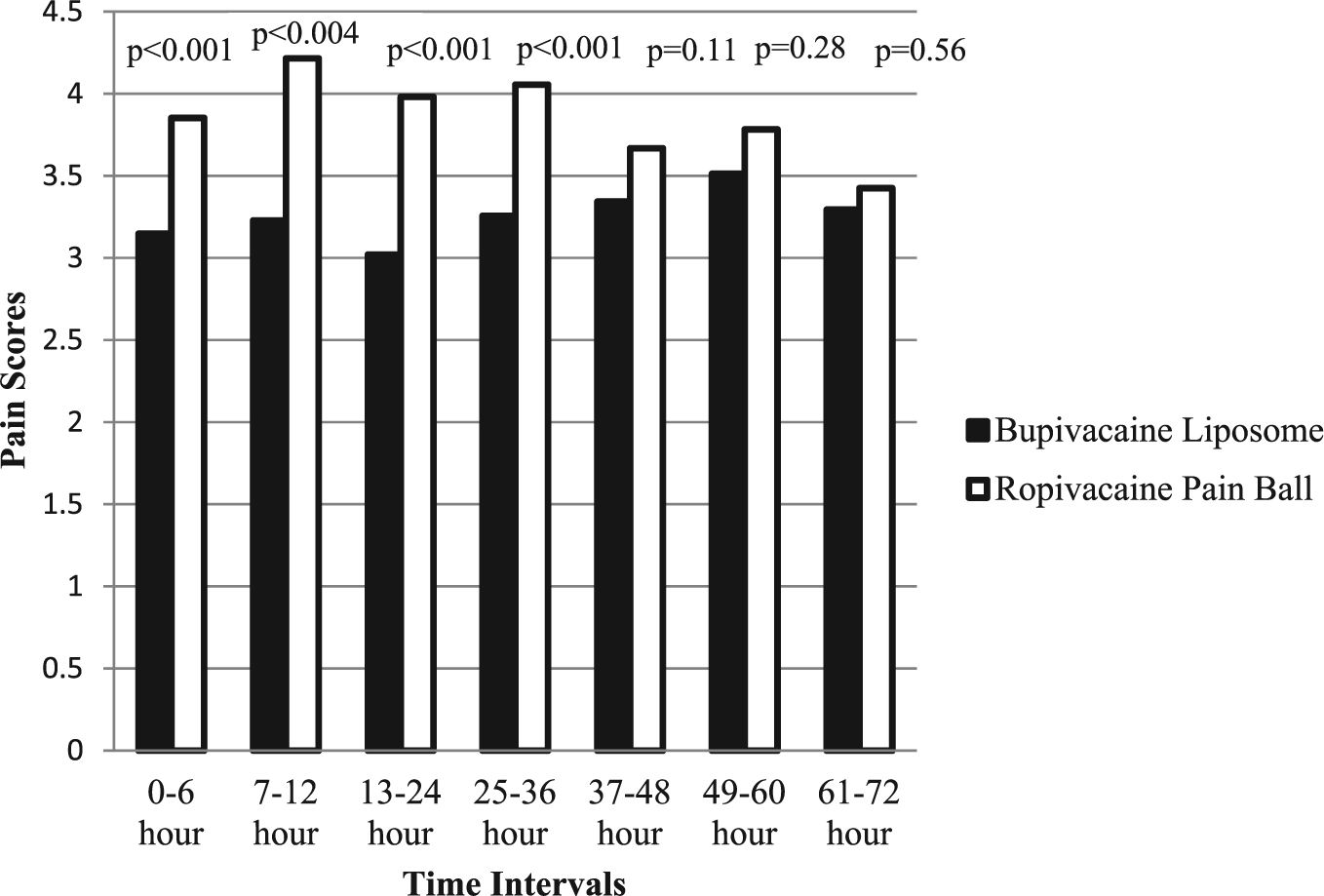
This graph shows the mean pain score over the 72-hour period divided into 6-hour intervals. The difference in pain scores from the bupivacaine liposome group to the ropivacaine pain ball was statistically significant for the 6-hour intervals in the first 36 hours (overall 3.1 vs 4.0, respectively, P < 0.001). By the 72-hour interval, the pain scores were comparable.
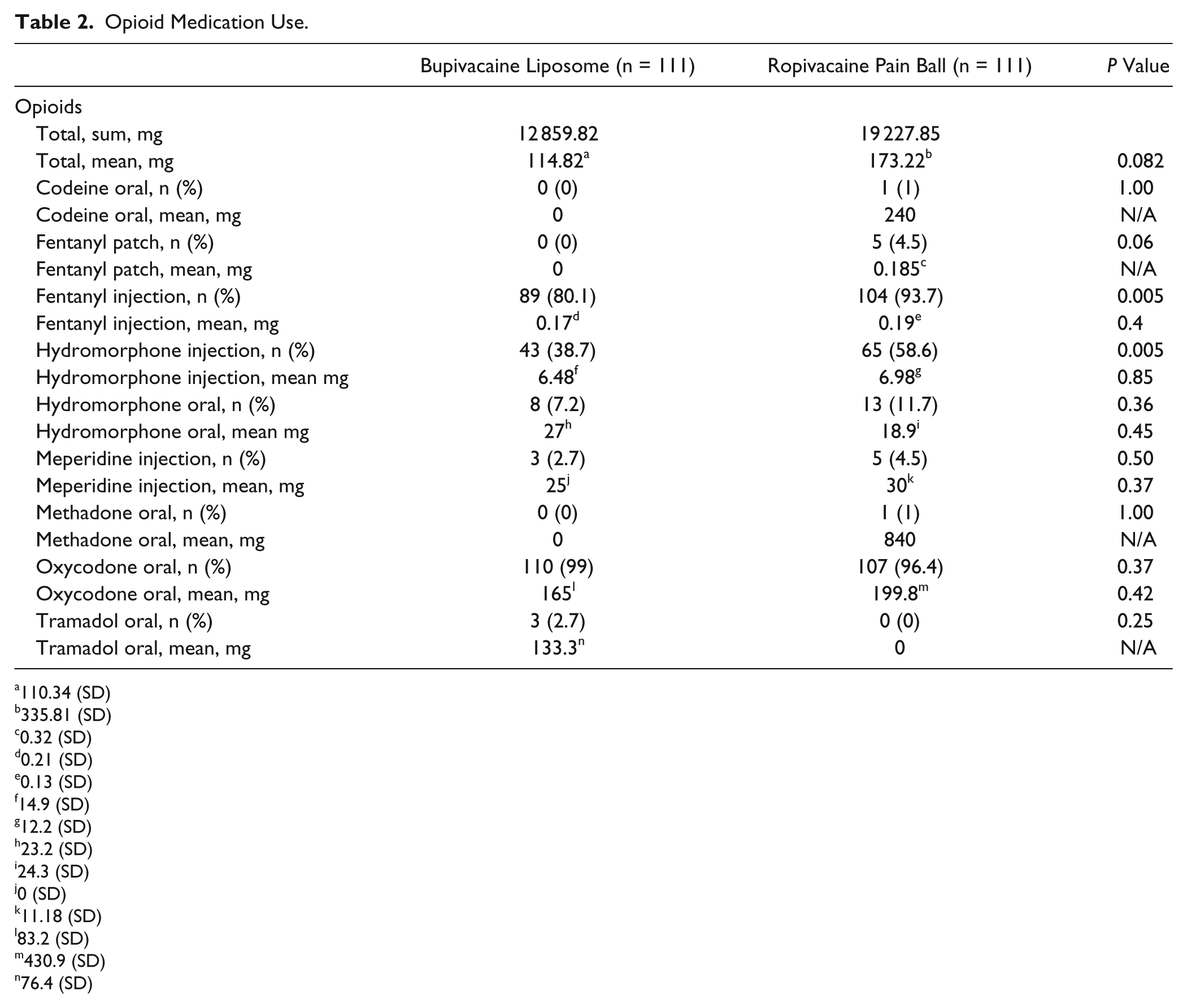
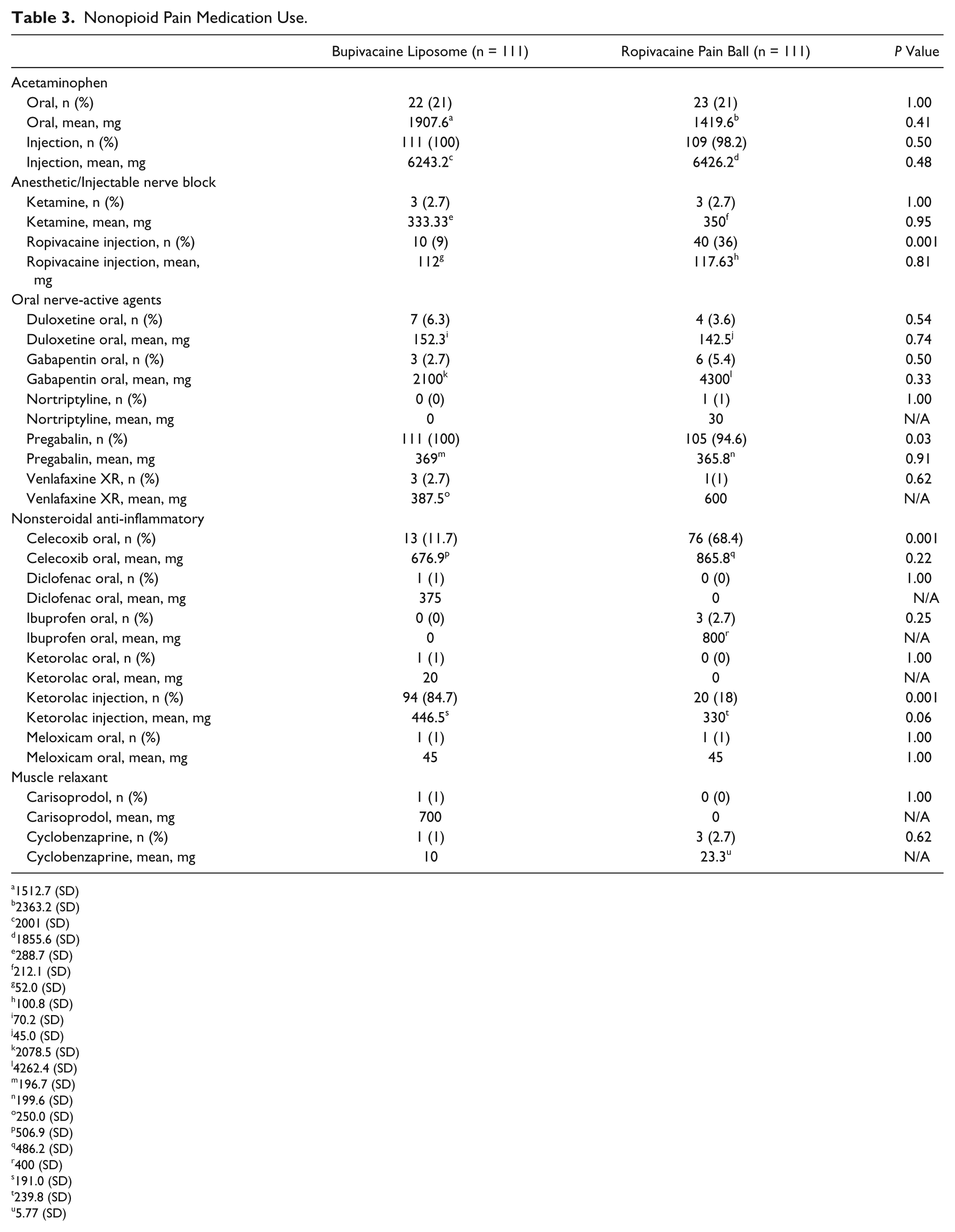
The mean length of stay was comparable between the two groups (3.1 days in the bupivacaine liposome group vs 3.2 days in the RPB group, P = 0.96). Patients in the bupivacaine liposome group used numerically lower amounts of opioids, although this was not statistically significant (115 ± 110 vs 173 ± 336 mg, P = 0.08); a detailed breakdown is given in Table 2. The large standard deviation of the mean opioid use per patient was caused by a few outliers who received much more opioids than the average. One patient in the bupivacaine liposome group received 1000 mg IV morphine equivalents because of heavy use of oral morphine and oral oxycodone. In the RPB group, there was an outlier who received 2628 mg of IV morphine equivalents of opioids because of heavy use of oral oxycodone and oral methadone. Another patient in the ropivacaine liposome group received 1094 mg of IV morphine equivalents, with 900 mg morphine equivalents of IV fentanyl. As shown in Table 3, mean nonopioid pain medication use was comparable for most medications between the 2 groups, except for statistically significant differences in the number of patients who received pregabalin, celecoxib, and ketorolac.
Opioid Medication Use.
110.34 (SD)
335.81 (SD)
0.32 (SD)
0.21 (SD)
0.13 (SD)
14.9 (SD)
12.2 (SD)
23.2 (SD)
24.3 (SD)
0 (SD)
11.18 (SD)
83.2 (SD)
430.9 (SD)
76.4 (SD)
Nonopioid Pain Medication Use.
1512.7 (SD)
2363.2 (SD)
2001 (SD)
1855.6 (SD)
288.7 (SD)
212.1 (SD)
52.0 (SD)
100.8 (SD)
70.2 (SD)
45.0 (SD)
2078.5 (SD)
4262.4 (SD)
196.7 (SD)
199.6 (SD)
250.0 (SD)
506.9 (SD)
486.2 (SD)
400 (SD)
191.0 (SD)
239.8 (SD)
5.77 (SD)
Cost of bupivacaine liposome and RPB groups were comparable ($797.70 vs 813.80, respectively, P = 0.63) as also indirect cost ($6768.40 vs $7108.70, respectively, P = 0.12). Significantly lower mean direct cost ($14 151.10 vs $15 465.50, P = 0.04) and total cost ($20 919.53 vs $22 574.17, P = 0.03) of care was found in the liposome bupivacaine group compared with the RPB group, as shown in Figure 3.
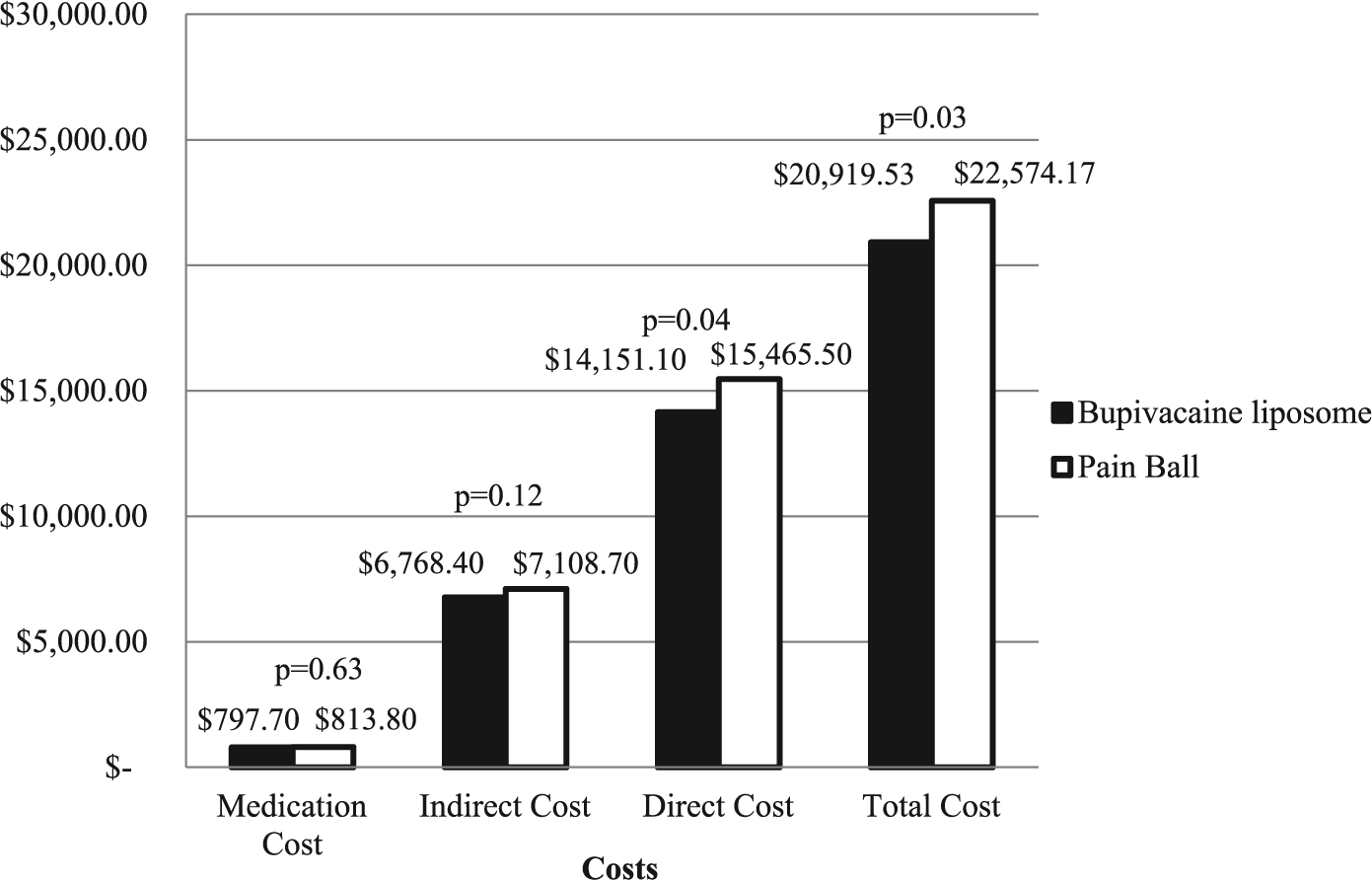
This figure shows the total cost breakdown for medication (bupivacaine liposome or cost of ropivacaine pain ball), indirect costs, direct costs, and total costs. Although medication and indirect costs were similar, the direct and total costs per patient case is significant.
Discussion
Patients undergoing TKA often experience intense postoperative pain that interferes with their functional recovery. Continuous ACBs have been shown to be superior to continuous femoral nerve blocks in promoting greater early postoperative ambulation with reported median distances of 37 m (0-90 m) versus 6 m (0-51 m) for continuous ACB and continuous femoral nerve blocks, respectively (P < 0.001). 9 This retrospective study was completed to determine the efficacy of bupivacaine liposome given as a single injection for ACB compared with continuous ACB provided by pain balls containing ropivacaine. Because bupivacaine liposome has a duration of approximately 24 hours, it can provide continuous pain relief similar to that of a pain ball.8,9
The results demonstrated that although initial pain scores within the first 36 hours were significantly better in the bupivacaine liposome group, these differences were comparable after the 36-hour mark. There were also no statistically significant differences found in the use of opioid medications, although statistical significance was found in the use of certain NSAIDs, such as celecoxib and ketorolac, and local injection of ropivacaine, reflecting protocol changes over time.
These mean pain score results are consistent with findings from previous studies, where no statistically significant difference in pain scores between bupivacaine liposome and its comparators were found when used in TKA. Bagsby et al 16 compared bupivacaine liposome with peri-articular ropivacaine injection in a multimodal pain protocol for TKA and found higher self-reported pain scores in the bupivacaine liposome group compared with the traditional ropivacaine injection group after the initial 24 hours (4.9 vs 4.4, respectively, P = 0.04). The two TKA studies comparing liposomal bupivacaine with bupivacaine HCl found no significant differences in numerical rating scores. 17 Furthermore, in November of 2014, the FDA notified Pacira Pharmaceuticals for overstatement of the medication’s efficacy. Despite initial pharmacokinetics data suggesting bupivacaine liposome’s bimodal kinetics (allowing for 96 hours of pain relief), the original pivotal trials that led to bupivacaine liposome’s approval only found statistically significant pain scores within the first 24 hours. Between 24 and 72 hours after study drug administration, there were minimal differences in mean pain intensity between bupivacaine liposome and placebo. The package labeling has, thus, been changed to reflect the fact that pain control lasts only for 24 hours.18,19
There have been few studies that examined the economic impact of using bupivacaine liposome. A series of open-labeled, economic clinical trials comparing a bupivacaine liposome–based multimodal analgesia regimen with IV opioid–based patient-controlled analgesia found a reduction in mean hospitalization costs ($8271 vs $10 726, P < 0.109). In our study, we found that using bupivacaine liposome provided a statistically significant reduction in direct and total costs per patient case of $1314.40 and $1654.64, respectively. At our institution, the acquisition cost of bupivacaine liposome is about $75 less per patient case than 0.1% RPB prepared by an outside company. In this case, the use of bupivacaine liposome was a more cost-effective alternative to the RPB as the major postsurgical analgesia method while also demonstrating statistically better pain control. In terms of formulary management, bupivacaine liposome is restricted to surgery as postoperative anesthesia to prevent misuse in nonsurgical settings. As postsurgical pain control moves more toward a multimodal approach, cost-effectiveness analyses may follow. The results of this study provide positive economic outcome results, with comparable efficacy of bupivacaine liposome and RPB. 14
There are several limitations to this study. Because of the retrospective nature of the study, there are some confounders that could not be controlled. One such confounder is any surgical or injection technique that may differ slightly from surgeon to surgeon because the procedures were carried out by 12 different surgeons. Furthermore, pain ball pump failures, although they occur rarely at our institution, were not taken into consideration, which may affect pain scores. In addition, the short-term safety of the two interventions was not assessed, but differences in cost may imply tolerability. Second, patient-reported pain scores documented in the electronic medical record varied depending on the time of the pain assessments. This led to different proportion of patients with available pain scores at each timed assessment interval and was not consistent. As addressed earlier in the Methods section, the standard-dose bupivacaine liposome was compared with 0.1% ropivacaine, which is not the standard 0.2% RPB. At our institution, pain scores have not drastically increased since switching to the 0.1% RPB, and fall rates have decreased. Thus, the 0.1% ropivacaine was chosen in our hospital’s standard surgical protocol. Additionally, because of the lack of baseline information for chronic opioid users and prior pain medication history, these patients may skew the pain medication use results. It was highly likely that these outliers, who led to the large standard deviation in mean opioid use, were patients already on chronic opioids. Finally, an endpoint that we were not able to collect because of time constraints was the lack of physical therapy (PT) results, which would be evaluated in a future study. Patients may have received PT for different lengths of time or multiple times per day at different intensities, which would have an impact on patient-reported pain scores.
From this retrospective cohort study, bupivacaine liposome only displayed clinically and statistically significantly better pain control within the first 36 hours postsurgery. Although the overall mean pain score over the 72 hours was statistically significantly lower, clinically they were comparable. Use of liposome bupivacaine led to a significantly lower mean direct cost and total cost per patient case. In the current health care environment, there is an increasing expectation to provide high-quality care at a lower cost. The use of ACB with liposomal bupivacaine may help meet those demands. Further studies need to be conducted to support these findings. As addressed earlier, future evaluations would consider safety and PT endpoints, such as adverse event outcomes, time to ambulation, and walking distance. Use of different metrics of pain control may also be warranted to provide more information on the efficacy of bupivacaine liposome in TKA.
Footnotes
Acknowledgements
The opioid dose calculator was provided by Cadence Pharmaceuticals, Inc, now Mallinckrodt Pharmaceuticals.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.