
Abstract
Introduction
Postoperative anemia is a common complication in patients undergoing major orthopedic surgery, including elective total hip arthroplasty (THA) and total knee arthroplasty (TKA). Postoperative anemia is associated with postoperative infections, poor physical function and recovery, and increased length of hospital stay and mortality. 1 The prevalence of anemia at baseline in adults 65 years or older is 11% for men and 10.2% for women, potentially leading to a higher rate of underlying anemia prior to elective surgery because of a greater incidence of THA and TKA in the elderly population.2,3 In patients undergoing elective THA or TKA, the prevalence of preoperative anemia is approximately 24.9% ± 9%, with estimations of subsequent postoperative anemia at 51% ± 10%. 1 The pervasiveness of perioperative anemia in this patient population increases the risk for postoperative complications.
Anemia in elective orthopedic surgery is multifactorial. A major contributing factor related to surgery itself is intraoperative blood loss, which may be as significant as1 to 2 L during the procedure. 4 The acute blood loss during surgery and subsequent decline in oxygen delivery to vital tissues is often unable to be corrected by the red blood cell (RBC) maturation process, which typically takes 1 to 2 weeks.5,6 Anemia may also arise as a result of a postoperative inflammatory response. This leads to decreased erythropoietin (EPO) production or response inhibition, even with normal levels of circulating EPO. The inflammatory response has the potential to modify iron metabolism and decrease the body’s ability to utilize iron stores.7-9 Each pathway to the development of postoperative anemia must be considered when evaluating potential treatment strategies. Additionally, certain risk factors or patient demographics have been identified as predictors for postoperative anemia in the overall surgery population. These include female sex, smaller body surface area, and African American racial identity.10,11 Regardless, all patients should be screened for anemia preoperatively and throughout the surgical setting.
Correction of postoperative anemia has historically been focused on blood transfusions. Orthopedic surgery alone accounts for 10% of all packed RBC transfusions nationwide. 12 A recent observational study at a large hospital network found transfusion rates of 19.3% and 38.5% in patients undergoing TKA and THA, respectively, with considerable variation among surgeons. 13 With blood transfusions come numerous complications, culminating in a high incidence of morbidity and mortality.12,14 From 2008 to 2012, 198 transfusion-related mortalities were reported to the US Food and Drug Administration. 12 Blood transfusions pose an increased burden on the health care system and are associated with a number of complications and poor outcomes, which are listed in Table 1.12,14,15 In addition to various complications, there is also considerable monetary cost associated with transfusions. An evaluation of allogenic blood transfusions in patients undergoing elective THA found that transfusions increased total cost for patients by $1731 ± $49 compared with patients who did not receive transfusions (P < 0.001). 15
Various approaches have been studied to reduce the use of blood transfusions to prevent transfusion-related adverse events, increase patient safety, and reduce cost. The American Association of Blood Banks (AABB) published clinical practice guidelines in 2012 evaluating transfusion thresholds in hospitalized patients. 16 For postoperative surgical patients who are otherwise stable, including those with a preexisting cardiovascular condition, the AABB recommends a traditional transfusion threshold of 8 g/dL or less or as needed when symptoms (chest pain, orthostatic hypotension, tachycardia unresponsive to fluid resuscitation, or heart failure) arise. Overall, this strategy is associated with 39% fewer transfusions, with improved morbidity and mortality and no difference in efficacy. 16 Beyond a transfusion threshold, additional strategies can aid in correcting anemia and further mitigate the need for transfusion, such as the use of intravenous (IV) or oral iron therapy or erythropoiesis-stimulating agents (ESAs).
To date, there is no standard of care in perioperative management of anemia in patients undergoing elective THA or TKA. In this article, we discuss various approaches to minimize blood transfusions in patients undergoing elective orthopedic surgery, focusing on the role of IV and oral iron and ESA pharmacotherapy, as well as important treatment considerations for the use of these agents.
Methods
An English-language literature review was performed through a PubMed and MEDLINE database search from 1964 through March 2016 using the following terms alone or in various combinations: orthopedic, surgery, elective, anemia, blood transfusion, iron, erythropoiesis-stimulating agents, and erythropoietin. Additionally, references of relevant articles were reviewed for additional studies.
Results
A total of 8 prospective and retrospective studies and 1 meta-analysis evaluating strategies to limit blood transfusions in elective orthopedic surgeries in adult patients were included in the review.
Prehospitalization Setting
Emphasis should be placed on prevention, prompt identification, and correction of anemia in patients undergoing elective orthopedic surgery. Several strategies have been evaluated to achieve this in the preoperative setting. Initially, patients should be instructed to discontinue antiplatelet, anticoagulant, and NSAID (nonsteroidal anti-inflammatory drug) medications prior to surgery. Patients with planned elective surgeries should be screened for underlying anemia as soon as possible.12,17 Iron replacement and ESAs have been studied preoperatively as a way of preemptively correcting anemia.
Preoperative iron-deficiency anemia (IDA) has been shown to increase transfusion requirements in the cardiac surgery population and remains a concern in various types of surgical populations. 18 Correcting IDA preoperatively through the use of oral or IV iron may be of benefit, especially in the elective orthopedic surgery population where there is ample time to correct preoperative anemia. 19 Oral iron is typically preferred over IV iron; however, IV iron is indicated for patients who cannot tolerate oral iron; those who are experiencing persistent iron losses; patients receiving EPO; those with iron malabsorption issues, including short bowel syndrome; and patients with a short timeline before surgery.
Oral iron is best suited for planned TKA or THA surgeries when preoperative anemia is identified ahead of time, noting that oral iron takes 3 to 6 months to fully replete stores. 4 One study assessed oral iron (formulation and doses not specified) given for a mean of 24.5 weeks preoperatively in orthopedic patients with hemoglobin concentrations less than 12 g/dL. Of the 26 patients identified, 24 (92%) were female; the average age was 67 years; and all were undergoing primary THA. Patients responding with improved hemoglobin concentrations greater than 12 g/dL demonstrated lower transfusion rates than those who did not respond (9% of responders [n = 1 of 11] compared with 33% of nonresponders [n = 5 of 15]; P < 0.05). 20 Additional labs such as ferritin and transferrin saturation were not reported, making it difficult to identify underlying iron deficiency. Challenges to administering oral iron preoperatively include proper identification of IDA several months in advance of planned surgeries and patient adherence to oral iron repletion (Figure 1).
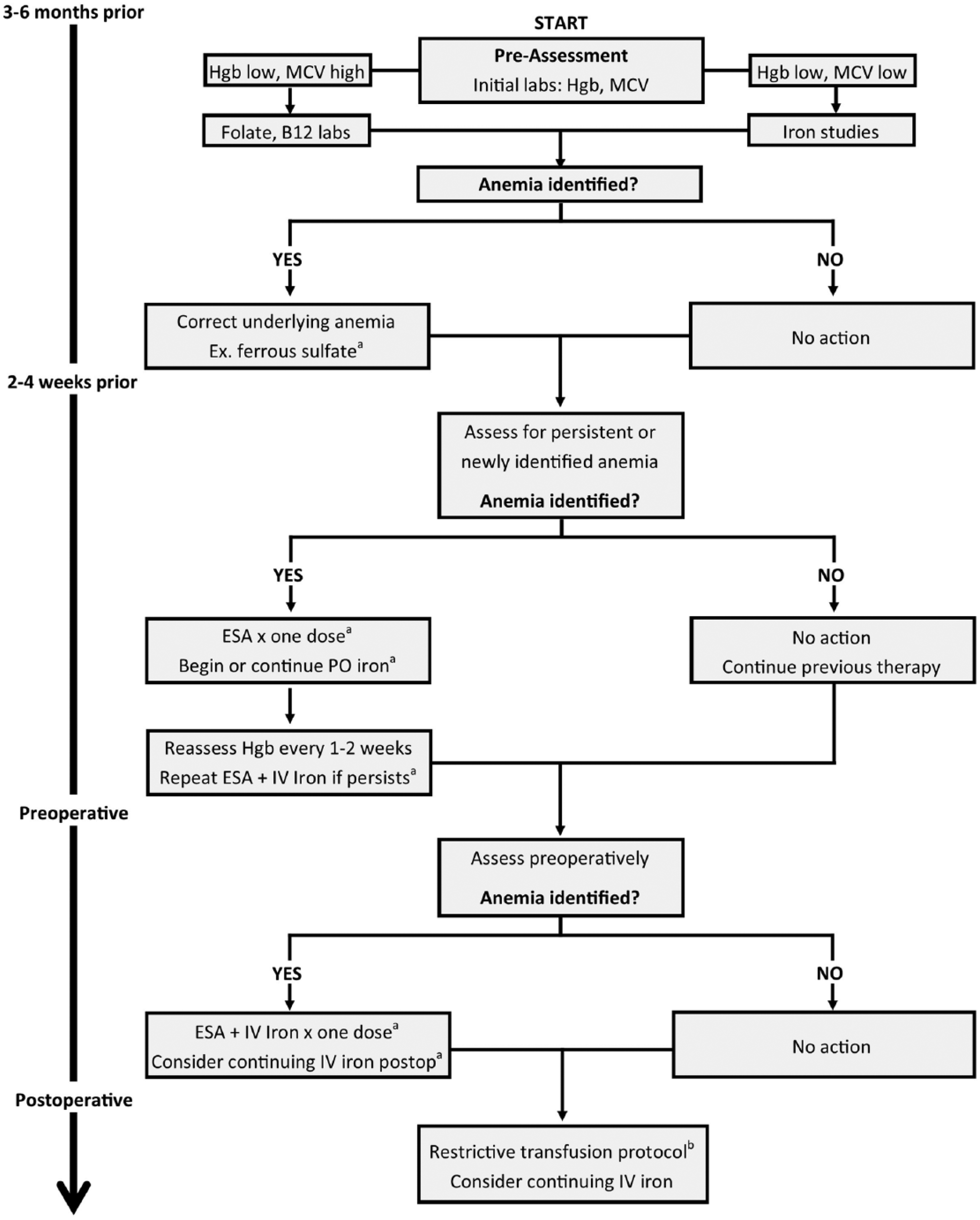
Proposed algorithm for identification and correction of perioperative anemia in elective orthopedic surgery patients.
IV iron may be indicated in patients for whom quick repletion of stores is desired, such as patients found to have IDA in the perioperative setting. 21 However, the convenience of administering higher doses over a shorter period of time may be offset by concern for hypersensitivity reactions, which although rare, may be life-threatening. 22 Although IV iron provides more timely repletion than oral iron, no studies evaluating IV iron alone within the preoperative setting were identified.
Use of an ESA, in tandem with oral or IV iron, may help increase circulating erythrocytes and improve perioperative outcomes.23,24 A recent meta-analysis highlighted results from 26 trials encompassing 3560 orthopedic patients receiving an ESA, with or without iron. Of the trials included, 96% (n = 25) combined ESA and iron therapy, whereas 35% (n = 9) combined ESA, iron, and preoperative autologous blood donation. All patients included in this analysis underwent elective TKA or THA. The ESA dosing, schedule, and duration varied among the clinical trials, and 20 trials included in the analysis involved participant weight and ESA dosing. Globally, doses ranged from 225 IU/kg/wk to 2100 IU/kg/wk, with the most consistent dosing regimen of epoetin alfa at 600 IU/kg/wk. Most frequently, patients were initiated on therapy from 7 to 35 days prior to procedure, with the most common starting date cited at 21 days preoperatively (13 trials). Administration continued anywhere from 0 to 7 days prior to procedure, although continuation of ESA dosing postoperatively was rarely seen. 23
Five trials used an ESA with IV iron, 2 included a combination of IV and oral, and the remaining used oral iron supplementation. Commonly, oral iron was initiated at the time of epoetin alfa; however, 1 trial did initiate oral iron 2 weeks prior to epoetin alfa. Regardless of dose and duration, use of oral iron in conjunction with epoetin alfa led to mixed results with respect to transfusion requirements. The combination of oral iron and epoetin alfa never resulted in more transfusions; however, when study protocols allowed for an iron-alone arm, these patients often required more blood transfusions than those in the combination arm. Administration of IV iron, as compared with oral iron, did not alter these findings.
Though the details included in the analysis were not fully described in the article, the authors noted that use of ESAs led to higher hemoglobin concentrations at discharge. This finding did not reach statistical significance and was not adjusted for iron administration, baseline hemoglobin values, or postoperative differences in hemoglobin. As a safety end point for the meta-analysis, thromboembolic events were reviewed. The authors found no difference in thromboembolic risk when using an ESA; however, minimal data were provided about use of venous thromboembolism prophylaxis. The findings from this meta-analysis suggest that ESA use may provide modest benefits in reducing transfusion rates in the short-term preoperative setting, without an increase in adverse events. Interestingly, these results are further supported by a recent prospective study demonstrating a 10% absolute reduction in transfusions (24 [13%] vs 5 [3%]; P = 0.0003) after implementation of a protocol utilizing ESA + IV iron in anemic preoperative and perioperative patients. 24 Allotment of 3 to 4 weeks preoperatively is necessary to allow the full effects of ESA administration to be seen. If used, ESAs should be given with iron to maximize the benefit (Figure 1).
Intraoperative Setting
Although outside the scope of this review, numerous interventions have been studied in the intraoperative setting to reduce the need for blood transfusions in orthopedic surgery. These consist of nonpharmacological and pharmacological strategies. Nonpharmacological modalities include normovolemic hemodilution, hypotensive anesthesia, tourniquets, bipolar sealants, and Cell Saver. Of these, the use of regional and hypotensive anesthesia has the most promising results. 12 Pharmacological strategies include fibrin sealants, desmopressin, thrombin, epinephrine or norepinephrine lavage, ε-aminocaproic acid, and tranexamic acid (TXA). To date, TXA, administered locally or systemically (IV), has the most robust data to support intraoperative use; however, any strategy used should be in tandem with preoperative assessment to augment transfusion reduction.12,25 Local and systemic (IV) administration of TXA are both effective techniques, without an increased rate of complications.
Perioperative Setting
IV iron repletion alone has been evaluated in orthopedic surgery in the perioperative setting, including the immediate preoperative and postoperative periods, for the past decade. The iron formulation primarily utilized is iron sucrose; however, ferric carboxymaltose has also been used. No standard dose exists in this setting; however, total doses of 200 to 600 mg of iron sucrose (100-200 mg every 48 hours for 2-3 doses beginning on the day of admission) perioperatively have been reported in studies focusing on IV iron.26-31 Studies typically did not report baseline iron labs; however, 1 trial specified that patients had near-normal iron levels (46.3-53.2 µg/dL), with no significant difference between groups as well as normal ferritin and transferrin levels. 26 No difference has been shown in blood transfusion rates (percentage of patients receiving a transfusion) in studies that compared patients receiving IV iron alone administered throughout the preoperative and postoperative periods with patients not receiving iron.26-28 Conversely, a retrospective study focusing only on postoperative IV iron administration found that its use significantly reduced the percentage of patients receiving a transfusion (11.5% vs 26.4%, P = 0.001). 29 These findings are further complicated by subanalyses of 2 of the aforementioned trials showing that patients with preoperative hemoglobin concentrations greater than 12 g/dL required fewer transfusions compared with those in control groups.26,27 This indicates that the ability of IV iron monotherapy to maintain hemoglobin concentrations above transfusion thresholds may be limited in the short-term setting when patients have lower baseline hemoglobin.
In addition to IV iron, postoperative oral iron has been evaluated. One study assessed patients with normal iron stores who were treated with oral iron therapy (ferrous sulfate 325 mg 4 times daily) or placebo, starting postoperative day 2 for the duration of their hospitalization. 32 No difference in transfusion rates or hemoglobin concentrations was noted between groups, likely because of the length of time it takes to see effects with oral therapy. Additionally, neither group experienced a hastened recovery of hemoglobin concentrations, and both had similar increases in reticulocyte fractions. This study did not assess other outcomes associated with postoperative anemia. IV iron may be preferred in the acute perioperative setting because it may allow rapid administration and use of iron despite the presence of inflammatory processes, which mitigate the body’s ability to utilize iron stores.
Discussion
A focus on limiting blood transfusions secondary to postoperative anemia in elective orthopedic surgery patients is essential to improve patient outcomes. Measures can be taken to reduce blood transfusions after elective orthopedic surgery, including preoperative screening and treatment of underlying anemia and use of iron or ESAs to improve perioperative anemia.
Postoperative anemia is easily explained by acute blood loss and the inflammatory state induced by surgery itself, leading to altered erythropoiesis and iron metabolism, and reduced availability of iron when the body attempts to compensate. In patients undergoing elective THA or TKA, the goal of limiting blood transfusions begins in the preoperative period, where screening and assessment are crucial. The Network for Advancement of Transfusion Alternatives (NATA) recommends that screening and correction of preoperative anemia take place 28 days or more prior to surgery. 3 As erythropoiesis and iron play an important role, strategies to overcome perioperative anemia include the use of iron and ESAs. If patients are found to be iron deficient, oral iron replacement is adequate in treating this underlying deficiency, provided there is adequate time prior to surgery. IV iron should be reserved for patients in whom oral therapy is not indicated. If patients have deficiencies in folate or vitamin B12, these should also be treated prior to surgery. For patients who do not respond to iron and those without nutritional deficiencies, ESA therapy may be implemented to correct the anemia. Regardless of the plan for preoperative autologous blood donation, the combination of IV iron and epoetin alfa has demonstrated the most favorable results when used in patients with preoperative anemia and should be considered in patients not responding to ESA therapy alone.
Agents used and dosing strategies varied throughout the literature; however, appropriate dosing for each of the agents used should be applied and may be institution specific. Table 2 outlines evidence-supported agents, dosing utilized, and estimated time to peak effect. Institution formulary and infusion protocols typically dictate which iron formulation is used and how it is given. Regarding ESA dosing, the literature and clinical trials suggest a preoperative hemoglobin level of 10 to 13 g/dL as a trigger for ESA therapy, but expected blood loss should also play a role in the decision to use an ESA. 23 To date, clinical trials have only used epoetin alfa; however, darbepoetin alfa may offer the advantage of a pre-filled syringe alternative. Darbepoetin alfa also has a 3-fold longer half-life than epoetin alfa and may be dosed less frequently. 33 Nevertheless, clinical benefits of darbepoetin alfa in the setting of elective orthopedic surgery remain to be evaluated.
Summary of Iron and ESA Dosing and Expected Time to Peak Effect for the Correction of Perioperative Anemia.
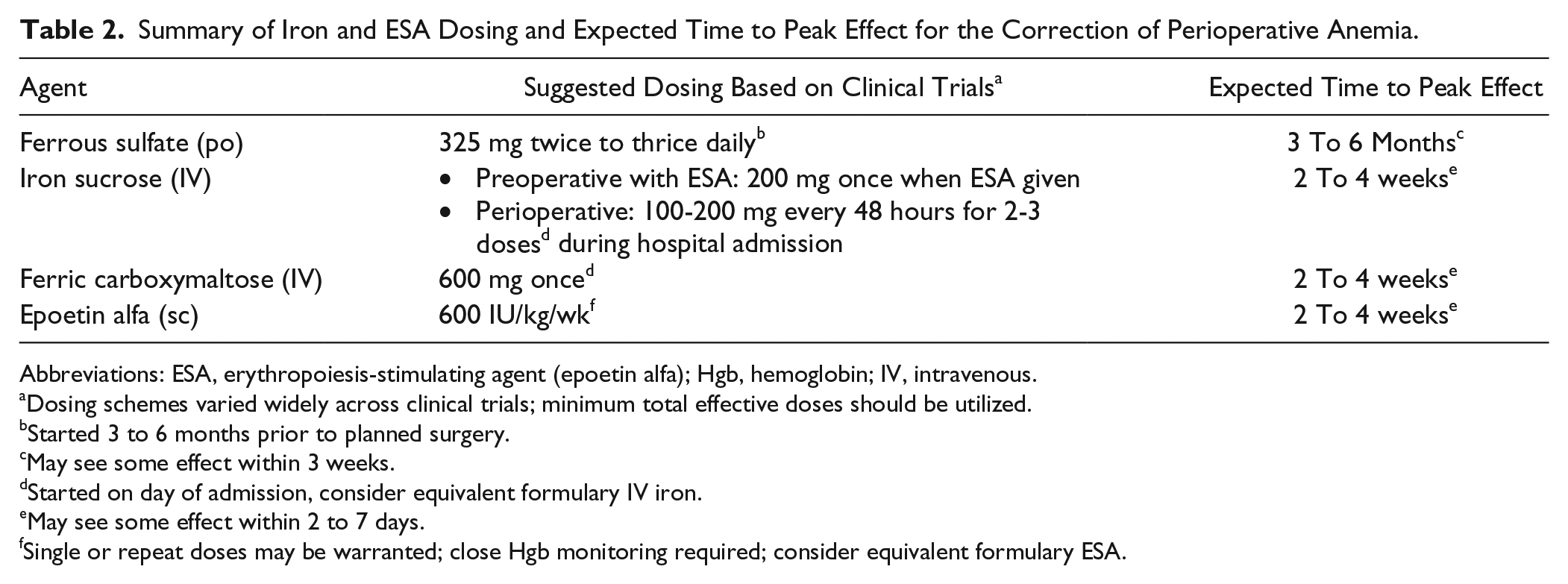
Abbreviations: ESA, erythropoiesis-stimulating agent (epoetin alfa); Hgb, hemoglobin; IV, intravenous.
Dosing schemes varied widely across clinical trials; minimum total effective doses should be utilized.
Started 3 to 6 months prior to planned surgery.
May see some effect within 3 weeks.
Started on day of admission, consider equivalent formulary IV iron.
May see some effect within 2 to 7 days.
Single or repeat doses may be warranted; close Hgb monitoring required; consider equivalent formulary ESA.
Although the agents discussed are being evaluated for short-term use, adverse events are important to consider. Oral iron commonly causes constipation, dark stools, stomach irritation, and nausea. Additionally, to maximize absorption, oral iron needs an acidic environment and should be taken on an empty stomach or with an acidifier such as vitamin C, which further increases some gastrointestinal adverse effects. Another consideration in postoperative patients and some preoperative patients is that many would also be receiving opioids for pain relief, which may compound constipation in patients receiving oral iron. IV iron is most notably associated with hypersensitivity reactions, including anaphylaxis; however, this is more common with older formulations or fast rates of administration. Other possible adverse events include hypotension, headache, nausea, and muscle cramps. 22 In orthopedic surgery studies, no differences were found between IV iron and comparators with regard to adverse events, and no severe adverse reactions to IV iron were noted.
ESAs are also associated with risks, most notably a boxed warning for cardiovascular events, including thromboembolic events. Aggressive venous thromboembolism prophylaxis following orthopedic surgeries should always be done, especially when using ESAs perioperatively. Other possible adverse effects include allergic reactions, hypertension, and gastrointestinal effects, including nausea and vomiting. With ESA use, weekly hemoglobin values should be monitored for rapid changes in concentrations and to assess the need for changes in dosing or frequency. If hemoglobin concentrations reach 13 mg/dL for men or 12 mg/dL for women, ESA therapy should be discontinued. 3 ESAs should be used with caution in chronic kidney disease and oncology patients. These patients are at higher risk of thromboembolic events and may have a lower threshold for ESA discontinuation (hemoglobin 10 to 11 mg/dL). 34 Iron deficiency, chronic inflammation, and underlying malignancy diminish response to ESAs. Iron studies should be completed prior to ESA use, and deficiencies should be corrected.
Finally, cost often accompanies agent selection, with oral iron as the least-expensive option, followed by IV iron, and then ESAs. A recent analysis demonstrated a reduction in blood transfusions with ESA therapy; however, use of ESAs in this analysis proved cost-prohibitive. ESA use was associated with an increased cost per patient of €785 (roughly US $860) and more than €7000 (roughly US $7650) per unit of blood transfusion avoided. Although the authors speculated that this could be partly a result of the strict transfusion protocol in place at their institution, careful cost considerations must be evaluated prior to ESA use. 35 IV iron, on the other hand, may be associated with neutral costs or modest cost savings, as demonstrated by one study. 29 This can likely be attributed to the fact that IV iron significantly reduced the percentage of patients transfused in this study.
Multiple facets should be evaluated when considering the use of oral or IV iron or an ESA to reduce blood transfusions in orthopedic surgery patients. The studies reviewed were limited by nonstandardized dosing, differences in timing of therapy initiation, and mixed reports of efficacy. Based on understanding of drug mechanisms and onset of action, pathophysiology of anemia, and available evidence, an assessment of findings and a proposed treatment algorithm is outlined in Figure 1, with dosing strategies outlined in Table 2. This algorithm is designed to serve only as a guide; clinical considerations, patient-specific factors, and individualized dosing should be evaluated. In addition to iron and ESAs, additional measures should be taken to reduce transfusions, including cessation of antiplatelet and anticoagulant medications prior to planned surgery and intraoperative strategies such as local or systemic TXA. Finally, strict transfusion protocols should be in place according to AABB guidelines (hemoglobin <8 g/dL or symptoms present) because they have been shown to reduce transfusion rates and potentially reduce mortality. With careful planning and strategic implementation of interventions such as iron supplementation and use of ESAs, blood transfusions can be minimized in patients undergoing elective orthopedic surgery, leading to reduced hospital cost and improved patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.