
Abstract

Polymyxin B (PMB) is a lipopeptide antibiotic increasingly used as a last-line antibiotic against extensively drug-resistant Gram-negative bacteria. 1 To date, there is minimal information available regarding PMB stability in different types of infusion solutions (ISs). He et al 2 found that 500 000 PMB units in 500 mL of 0.9% sodium chloride were stable for at least 1 day when stored at 4°C or 25°C. Unfortunately, this limits its clinical use in critically ill patients who are at risk of developing fluid overload states. We aimed to determine PMB stability in various reduced volumes of IS.
Each PMB vial (500 000 PMB units, approximately 50 mg, XGen Pharmaceuticals, USA) was reconstituted according to manufacturer’s instructions and injected into sterile polypropylene syringes (Becton-Dickinson) containing 25 mL (PMB: 2 mg/L), 50 mL (PMB: 1 mg/L), or 100 mL (PMB: 0.5 mg/L) of 0.9% sodium chloride, 5% dextrose, 0.45% sodium chloride/5% dextrose, and 0.225% sodium chloride/5% dextrose, respectively. The solutions were stored at 4°C, 25°C, and 30°C, respectively. The type of IS, storage temperatures, and duration of stability evaluated were based on the common use of these IS in intensive care units, regular room temperatures in the Asia-Pacific region, and its potential for use in the outpatient setting.
Samples were withdrawn at regular intervals over 24 hours (stored at 25°C and 30°C) and over 168 hours (stored at 4°C) and analyzed via a validated liquid chromatography tandem mass spectrometry (MS) method according to Food and Drug Administration guidance for analytical procedures and methods validation for drugs. In brief, the major constituents of PMB (PMB1, PMB2, PMB3, and PMB1-Ile) (TOKU-E, Bellingham, USA) were separated on a C18 column. Detection and quantification of the various PMB components were based on multiple reaction monitoring by MS. Calibration ranges of PMB2, PMB3, and PMB1-Ile were 0.01 to 0.5 mg/mL, whereas that of PMB1 was 0.1 to 5 mg/mL. Samples at baseline and at the end of the experiment were measured for pH using a pH meter (Fisher Scientific, Pittsburgh, PA), and osmolarity was measured using an osmometer (Wescor Inc, Logan, UT).
All samples retained more than 95% of their initial concentration at 24 hours stored at 25°C and 30°C in various ISs (Table 1). Samples stored at 4°C retained nearly 100% of their initial concentration after 168 hours. The variability of the PMB components was consistent with results published previously (data not shown). 3 The pH and osmolarity of PMB diluted in the 4 pharmaceutical ISs were fairly similar throughout the study period when compared with baseline conditions.
Physicochemical Stability, pH, and Osmolarity of Total PMB (50 mg, PMB1, PMB2, PMB3, and PMB1-Ile) Reconstituted in Different Diluents (25 mL, PMB 2 mg/L) at Different Temperatures.
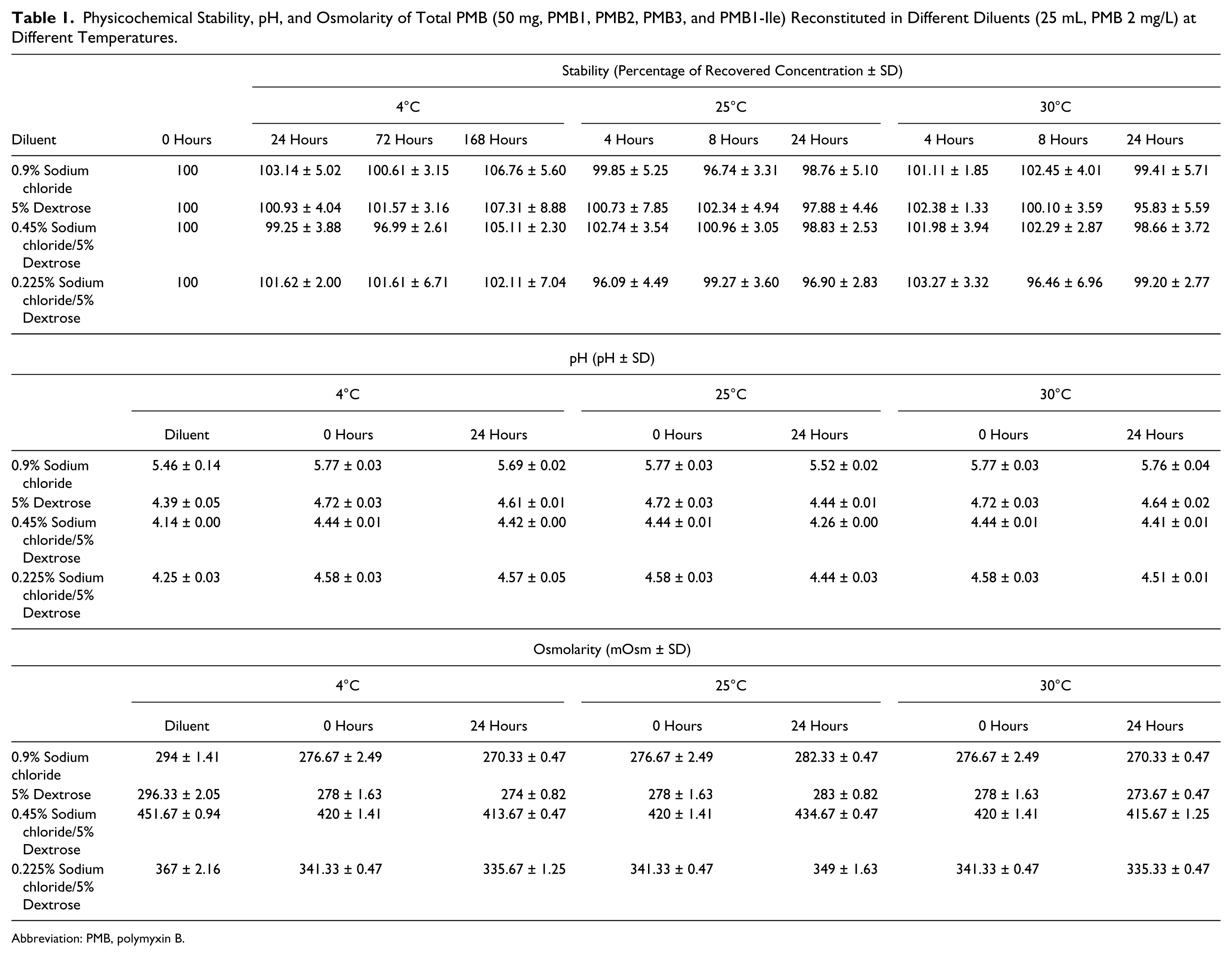
Abbreviation: PMB, polymyxin B.
To the best of our knowledge, this is the first study that examined PMB stability at high concentrations in various ISs. Previously, many clinicians substituted PMB with intravenous colistin (polymyxin E) as it can be diluted in 50 to 100 mL of IS for each usual dose of 1 to 2 million units thrice daily. However, this substitution may not be optimal because colistin (active drug) requires hydrolysis from colistimethate sodium and has been shown to result in insufficient serum levels at steady state. This may potentially compromise antimicrobial efficacy and, thus, patient outcomes. 4 Of note, a recent retrospective cohort study had also suggested a 2-fold increase in nephrotoxicity associated with colistin compared with PMB. 5
To summarize, PMB was stable for at least 1 day when stored at 4°C, 25°C, and 30°C in 0.9% sodium chloride, 5% dextrose, 0.45% sodium chloride/5% dextrose, and 0.225% sodium chloride/5% dextrose at a high concentration of 2 mg/mL. In view of the potential increased risk of adverse reactions such as thrombophlebitis at the infusion site, anaphylactoid reactions, and pain at the infusion site, we suggest that PMB be administered in small diluent volumes via central venous access.
Footnotes
Acknowledgements
We would like to thank Ms Evelyn Png from Singapore Eye Research Institute for her technical assistance with the osmometer measurements.
Authors’ Note
This study was presented in part at the Interscience Conference on Antimicrobial Agents and Chemotherapy/International Society of Chemotherapy (ICAAC/ICC) 2015; San Diego, CA; September 17-21, 2015. This study was approved by the institutional ethics review board prior to initiation (CIRB/2014/271/D).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Singapore General Hospital Research Grant (SRG/C1/01/2014); National Medical Research Council Centre Grant (NMRC/CG/016/2013); and Ministry of Health Communicable Diseases Public Health Research Grant (CDPHRG/12NOV015). The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication.