
Abstract
Introduction
Atrial fibrillation (AF) is a common arrhythmia and increases in prevalence with advancing age. In the United States, more than 2.5 million people suffer from AF. 1 AF is associated with increased risk of morbidity and mortality. Catheter ablation (CA) and antiarrhythmic drugs (AADs) are effective interventions to reduce the frequency of or eliminate episodes of AF. 1 Compared with AADs, CA is more effective in maintaining sinus rhythm and has emerged as first-line treatment to control cardiac rhythm. 2 However, inflammation caused by CA promotes a proarrhythmic milieu, so recurrence of atrial tachyarrhythmias is very common within the first few months postablation. 3 Because “AF begets AF,” early recurrence of atrial tachyarrhythmias (ERAT) may lead to late recurrence of AF (LRAF). ERAT has been demonstrated as an independent risk factor for LRAF. 4 Therefore, short-term use of AADs following AF ablation is a common strategy used by cardiologists for the purposes of not only reducing ERAT, but also preventing LRAF.
Xu et al 5 had done a meta-analysis to evaluate the efficacy of such treatment and showed that short-term use of AADs could reduce the incidence of ERAT but could not prevent LRAF. Nevertheless, there were several limitations in their study. First, an included study enrolled patients undergoing atrioventricular junction ablation rather than AF ablation. Second, the number of enrolled patients was small (814 patients). Third, they did not perform subgroup analyses and sensitivity analyses, which are necessary to arrive at more reliable conclusions. In addition, they did not consider all clinically meaningful end points such as cardioversions and arrhythmia-related hospitalizations. Therefore, we performed a meta-analysis that tried to improve on the disadvantages mentioned above to comprehensively evaluate the efficacy of short-term use of AADs postablation in preventing ERAT and LRAF.
Methods
Search Strategy and Eligibility Criteria
PubMed, Embase, Cochrane Library, and ClinicalTrials.gov (until May 1, 2016) were searched for randomized controlled trials (RCTs) that compared short-term use of AADs after AF ablation against controls; there were no language restrictions. The following Mesh or terms were used: (Anti-arrhythmia agents OR anti-arrhythmia drugs OR antiarrhythmi* OR procainamide OR disopyramide OR mexiletine OR flecainide or propafenone OR bisoprolol OR esmolol OR amiodarone OR dofetilide OR sotalol OR ibutilide OR azimilide OR moricizine OR cibenzoline) AND (atrial fibrillation OR atrial fibrillat* OR auricular fibrillat* OR atrium fibrillat* OR AF) and (catheter ablation OR ablat* OR radiofrequency OR cryoablation OR PVI OR pulmonary vein isolation). We also checked the reference lists of all key articles for any additional eligible articles. Studies were included if they met the following criteria: (1) enrolled patients undergoing CA for AF; (2) compared AAD use within the first 3 months after CA with placebo or no treatment; (3) type of study was RCT; (4) reported end points of interest. In our study, the primary end points were early recurrence of tachyarrhythmias and late recurrence of AF (recurrence within the first 3 months postablation was defined as early recurrence; otherwise defined as late recurrence). Second end points were cardioversions and arrhythmia-related hospitalizations within the first 3 months after CA for AF. We excluded duplicate reports and post hoc analyses. We excluded abstracts from meeting proceedings, unless full texts were published in a peer-reviewed journal. The selection of eligible articles was performed by 2 investigators independently. Disparities between investigators were resolved by discussion between them.
Data Extraction and Quality Assessment
Two authors independently extracted data from eligible studies. The following data were extracted from each RCT: the year of publication, sample size, patient characteristics, ablation procedure, AAD use, outcome measure, and end points of interest. The methodological quality was evaluated by using the Cochrane Collaboration’s tool, which includes 7 domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. 6 Definitions and judgment criteria for each domain are available in Cochrane Handbook. 6 The judgment criteria for other bias in Cochrane Handbook are ambiguous. In our meta-analysis, studies were judged as having a high risk of other bias if at least 1 of the following problems was present: (1) the results were probably influenced by funders, such as industry-initial trials, and (2) the study was not strictly carried out according to prespecified protocol. Studies without these 2 problems were judged as having a low risk of other bias. Studies with insufficient information to assess these 2 problems were judged as having an unclear risk of other bias. Assessment of risk of bias was performed for primary end points. We judged trials with 2 or more high-risk domains as having a high risk of bias and trials with 1 high-risk domain as having a moderate risk of bias. Quality assessment was also independently carried out by 2 authors. All disagreements between the 2 authors were resolved by discussion.
Statistical Analysis
We pooled data across trials according to the intention-to-treat principle and calculated relative risks (RRs) with 95% CIs to compare the differences for dichotomous outcomes. Fixed-effects models were preferred, and random-effects models were selected only when significant heterogeneity was identified. The χ2-based Q test and I2 statistic were used to test heterogeneity among studies. When P <0.05 and/or I2 >50%, significant heterogeneity was presumed.
Stratified analyses were conducted to evaluate the impact of selected patient characteristics on primary end points. Analyses were stratified according to the mean age of patients >60 years, the mean AF duration >60 months, and the mean left-atrial diameter (LAD) >40 mm. The Q test based on the random-effects model was used to detect difference between subgroups. Sensitivity analyses were performed by removing each study and switching the analysis model.
When fewer studies are included in a meta-analysis, the power of funnel plots to detect publication bias is low, so according to Cochrane Handbook, tests for funnel plot asymmetry are not recommended when fewer than 10 studies are analyzed. 6 The meta-analysis was conducted using Revman 5.3 software.
Results
Characteristics of Studies and Quality Assessment
The study selection process is presented in Figure 1. Briefly, 3423 references were identified after searching databases. After scanning the titles and abstracts, 3231 citations were excluded; 192 full-text articles were assessed for eligibility. Finally, 6 studies were included in our meta-analysis involving 2764 patients. Five studies enrolled patients with paroxysmal, persistent, and/or long-standing AF,7-11 and the remaining one only enrolled patients with paroxysmal AF.12,13 The mean age of patients ranged from 50 to 63 years, and most patients were male. In all studies, the mean duration of AF was more than 12 months, and in 4 of them, the mean AF duration was more than 50 months.8,10-13 The average LAD was more than 40 mm in 4 studies8,10-13; in the remaining two, it was 38 and 39 mm, respectively.7,9 Three studies reported the proportion of additional ablation ranging from 32% to 100%.7-9 In all studies, investigators combined standard electrocardiograms (ECGs), Holtor monitoring, and ambulatory ECGs to detect AF recurrence. Regarding the baseline characteristics, no significant difference was found between the 2 groups in each study. All studies reported the incidence of ERAT and LRAF, except the study by Lodziński et al, 11 which just reported the incidence of ERAT. The characteristics of studies are summarized in Table 1.7-13
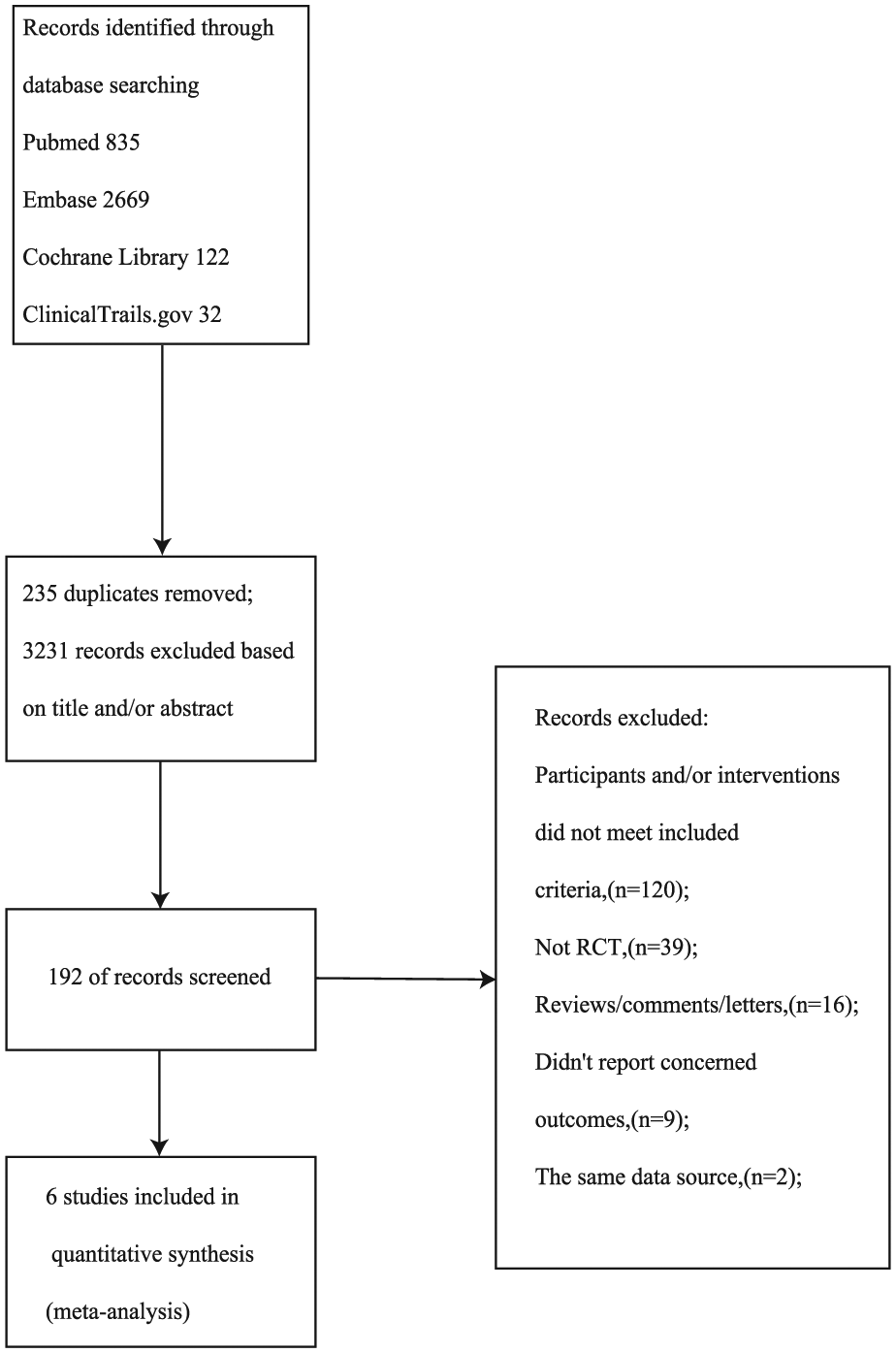
Flow diagram of the selection process of eligible articles.
Characteristics of Eligible Studies.
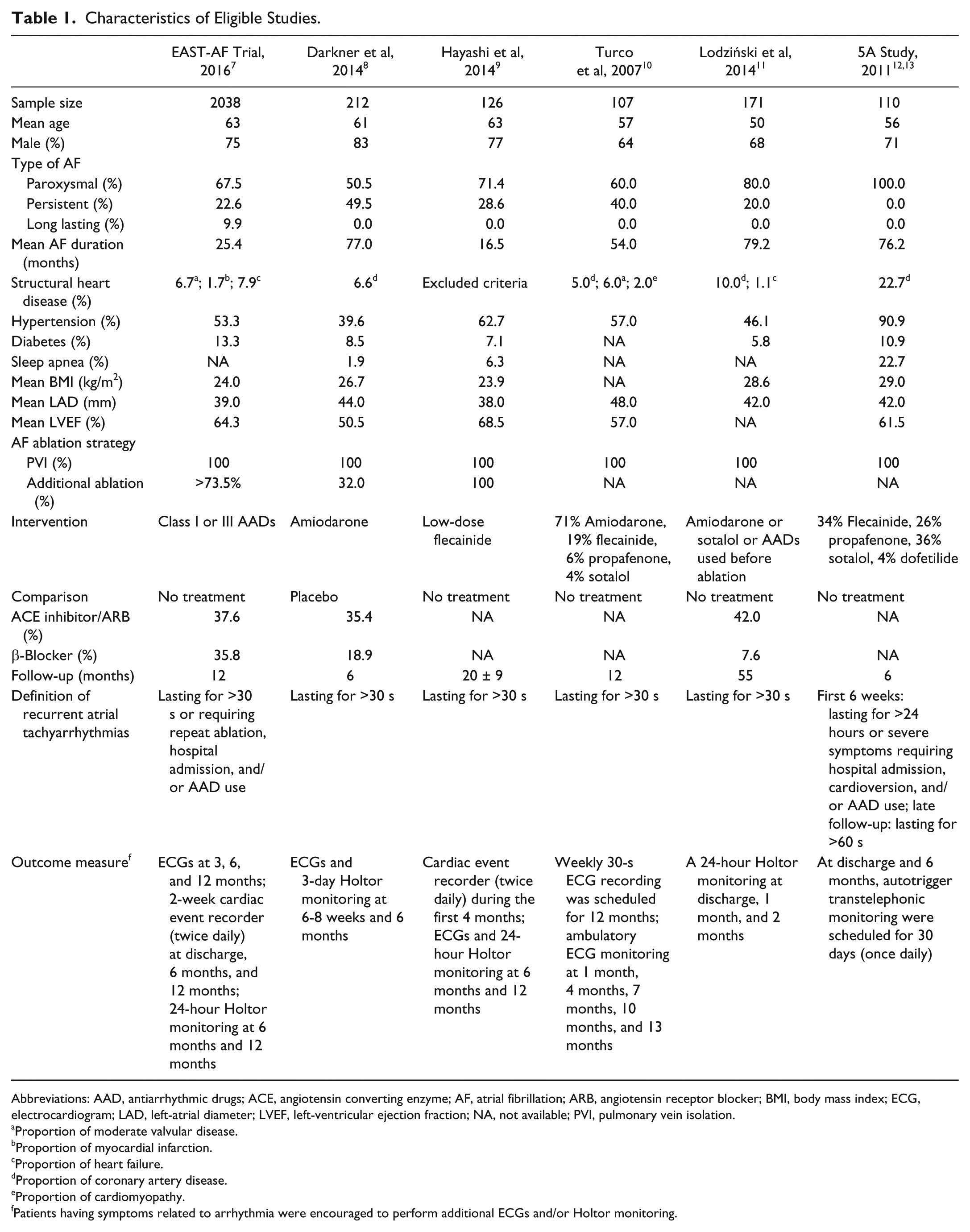
Abbreviations: AAD, antiarrhythmic drugs; ACE, angiotensin converting enzyme; AF, atrial fibrillation; ARB, angiotensin receptor blocker; BMI, body mass index; ECG, electrocardiogram; LAD, left-atrial diameter; LVEF, left-ventricular ejection fraction; NA, not available; PVI, pulmonary vein isolation.
Proportion of moderate valvular disease.
Proportion of myocardial infarction.
Proportion of heart failure.
Proportion of coronary artery disease.
Proportion of cardiomyopathy.
Patients having symptoms related to arrhythmia were encouraged to perform additional ECGs and/or Holtor monitoring.
A risk bias assessment was performed for the primary end points in each trial. Two studies10,12 reported appropriate methods to generate the random sequence. Allocation concealment was reported in only 1 study. 12 Blinding was applied and reported in only 1 study. 8 Incomplete outcome data and selective reporting were not observed, except in the study by Lodziński et al, 11 in which selective reporting was a high risk. The risk of other bias was low in 2 studies7,8 and was unclear in the other studies. Overall, the study by Darkner et al 8 had a low risk of bias; the study by Lodziński et al 11 had a high risk of bias; and the remaining studies had a moderate risk of bias.7,9,10,12,13 The results are summarized in Figure 2.
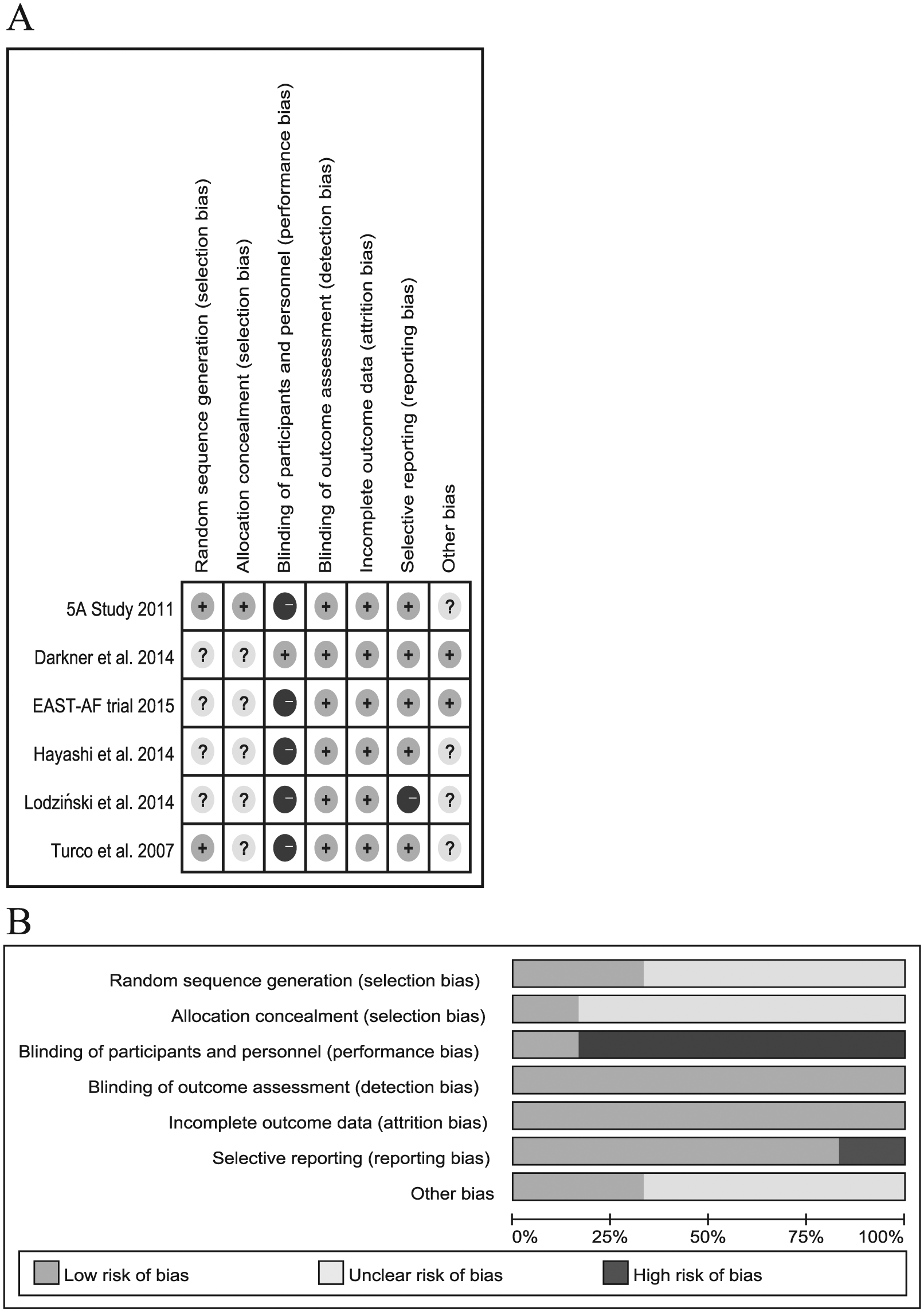
Risk of bias assessment for the included trials: A. Summary of the risk of bias for each individual trial. B. Overall risk of bias.
Efficacy of Short-term AAD Use
The frequency of ERAT was 39.5% (556 of 1407) in the AAD group, and it was 47.2% (640 of 1357) in the control group. The pooled risk ratio of the AAD group to the control group was 0.78 (95% CI = 0.62-0.98). Significant heterogeneity was detected in this analysis (P for heterogeneity = 0.02; I2 = 0.62; Figure 3). Because of the high risk of bias, we excluded the study by Lodziński et al, 11 and the pooled RR was 0.71 (95% CI = 0.56-0.91; P for heterogeneity = 0.06; I2 = 56%). We conducted stratified analyses to evaluate the impact of selected patient characteristics on the results. The results are shown in Table 2.
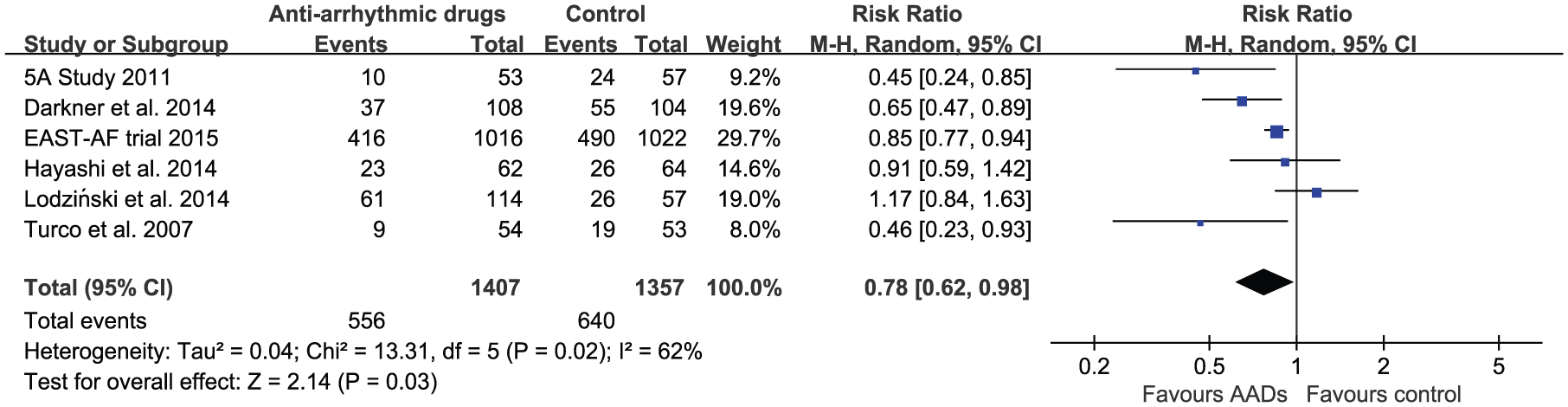
Forrest plot showing the efficacy of short-term use of AADs following catheter ablation for atrial fibrillation in reducing ERAT.
Subgroup Analyses on the Basis of ERAT.
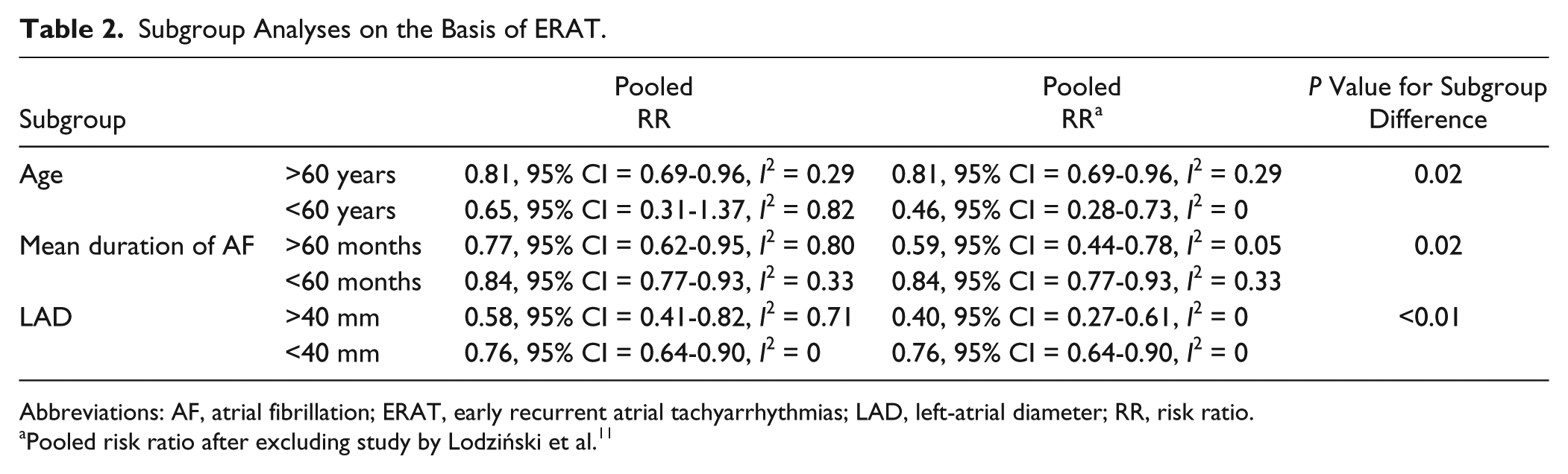
Abbreviations: AF, atrial fibrillation; ERAT, early recurrent atrial tachyarrhythmias; LAD, left-atrial diameter; RR, risk ratio.
Pooled risk ratio after excluding study by Lodziński et al. 11
Five studies reported the incidence of LRAF.7-10,12,13 The incidence of LRAF in the treatment group and the control group was 32.5% (420 of 1293) and 34.6% (450 of 1300), respectively. The pooled RR was 0.94 (95% CI = 0.85-1.05), and no significant heterogeneity was detected in this analysis (P for heterogeneity = 0.86; I2 = 0; Figure 4). In subgroup analyses, the results remained consistent in all subgroups.
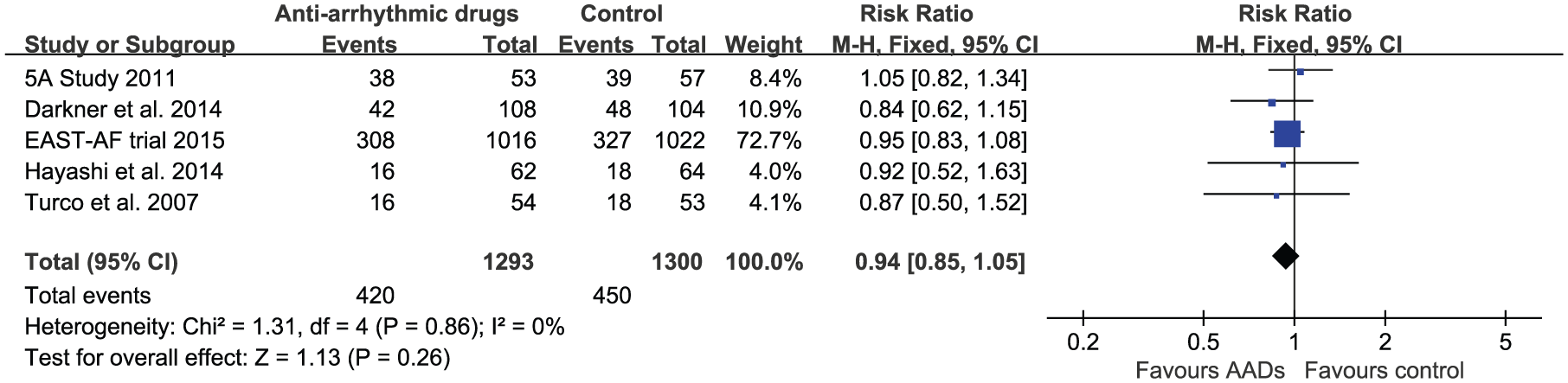
Forrest plot showing the efficacy of short-term AAD use following catheter ablation for atrial fibrillation in preventing LRAF.
Three studies reported the rate of cardioversions within the first 3 months after CA (Table 3). The pooled result showed no statistical difference between the 2 groups (RR = 0.78; 95% CI = 0.60-1.01; P for heterogeneity = 0.38; I2 = 0). Although Darkner et al 8 did not report the rate of cardioversions, the authors showed that short-term use of AADs could reduce the frequency of cardioversions (RR = 0.36; 95% CI = 0.20-0.62). 8 Only 2 studies reported the incidence of arrhythmia-related hospitalizations. In the study by Darkner et al, 8 short-term AAD use significantly reduced arrhythmia-related hospitalization rates (RR = 0.44; 95% CI = 0.31-0.61). However, in the study by Hayashi et al, 9 no difference was detected between the 2 groups (0/62 vs 1/64, P = 0.33).
Incidence of Cardioversions Within the First 3 Months Following Catheter Ablation.

Abbreviation: AAD, antiarrhythmic drug.
Sensitivity Analyses
In sensitivity analyses, switching the analysis model or removing each individualized trial did not have any relevant influence on the results.
Discussion
The main results of this meta-analysis are as follows: (1) short-term use of AADs after CA could reduce the incidence of ERAT; (2) short-term use of AADs post-CA was ineffective in preventing LRAF; and (3) it remained controversial whether short-term use of AADs could reduce the frequency of cardioversions and arrhythmia-related hospitalizations within the first 3 months postablation.
ERAT, defined as the recurrence of atrial tachyarrhythmias within the first 3 months after AF ablation, is very common. In our study, the incidence of ERAT in the AAD group and the control group was 39.5% and 47.2%, respectively. The results are in accordance with previous studies, which reported that the incidence of ERAT ranged from 15.9% to 65%. 14 There may be several causes of ERAT: (1) acute inflammation caused by CA, (2) early resumption of electrical activity in ablation lines, (3) transient imbalance of the autonomic nervous system, and (4) a lack of delayed lesion formation. 15 ERAT may resolve spontaneously, and patients may have long-term freedom from AF recurrence. Therefore, reablation is not recommended during this period. 2 However, ERAT could cause symptoms related to arrhythmias and even increase arrhythmia-related hospitalizations and cardioversions. Treatment with AADs as an alternative to maintain sinus rhythm is a common strategy used by cardiologists. In our study, although significant heterogeneity was detected across studies, most studies demonstrated that short-term AAD use could reduce the incidence of ERAT (Figure 3). Stratified by age, duration of AF, and LAD, there was no significant heterogeneity in each subgroup, and the pooled results of each subgroup showed that short-term AAD use could prevent ERAT (Table 2). Thus, we concluded that short-term AAD use was effective in preventing ERAT. In subgroup analyses, short-term use of AADs seemed to be more effective in reducing ERAT in patients who were younger, had a longer duration of AF, and had larger left atria. It may be attributed to the fact that ERAT is more frequent in patients with longer duration of AF and/or larger left atria.
Although CA is superior to AADs in maintaining sinus rhythm, the incidence of LRAF is still unsatisfactory. A prior meta-analysis reported that the rate of LRAF with a single procedure was nearly 50%. 16 Pooled incidence of LRAF in our meta-analysis was 33.6%. Advanced technology, short-term follow-up, and more skilled operators contributed to the lower rate of LRAF in our study. Many studies had shown that ERAT was a risk factor for LRAF.4,17-19 How ERAT affects long-term outcomes is not fully established. Nowadays, the concept that “AF begets AF” is widely accepted. The major mechanisms are electrical and structural remodeling induced by AF. In animal studies, there was mounting evidence that early rhythm control resulted in reversal of atrial remodeling. 20 Recently, Walters et al 21 showed similar results in humans. Reversal of atrial remodeling is an independent predictor of long-term success of AF CA.22,23 Tao et al 24 observed that patients with ERAT had increased LAD at the time of reablation. Therefore, we hypothesized that ERAT might interrupt reversal of atrial remodeling after AF ablation and then promote LRAF. So it seemed to be reasonable that reducing ERAT might improve long-term outcomes. Unfortunately, our study demonstrated that short-term use of AADs could prevent ERAT, but the incidence of LRAF did not decrease as expected. The results were consistent in subgroup analyses. The underlying mechanism is not fully understood. One potential explanation is that long-term AF leads to irreversible atrial remodeling. In the included studies, the mean duration of AF ranged from 16 to 80 months, and left atrial dilation, a marker of remodeling, was obvious. Thus, the atrium was too degenerated to expect the reverse remodeling within 3 months. In practice, AF ablations are usually performed in patients with short-term AF, so we expect further studies to confirm the results in patients with short duration of AF. Another possible reason is that the clinical significance of some ERAT equals that of LRAF. Recently, the clinical significance of ERAT was investigated by Nalliah et al. 25 In their study, 73% of patients with recurrence of AF at the third month after CA suffered from LRAF, but the rate was only 25% in those with recurrence of AF within the first 2 months. ERAT may be caused by early resumption of ablation lesions, which is also a cause of LRAF. Andrade et al 19 reported that nearly 50% of patients with ERAT had early reconnection and benefited from early reablation. Transient suppression of this kind of ERAT could not improve long-term outcomes. Overall, according to our study, short-term use of AADs following AF CA was unnecessary with regard to the prevention of LRAF.
Whether long-term AAD use after CA could improve long-term outcomes is also debatable. Rordorf et al 26 summarized the observational studies and showed that compared with CA alone, combining CA and long-term use of AADs increased long-term success rates by 15%. Recently, Zhang et al 27 compared the long-term use of AADs with reablation in patients suffering from LRAF and showed the superiority of reablation over AAD use in maintaining sinus rhythm.
Regarding arrhythmia-related hospitalizations and cardioversions within the first 3 months after ablation, our results were controversial. In contrast to the study by Darkner et al, 8 pooled results of 3 studies showed that short-term use of AADs might reduce the frequency of cardioversions, but there was no statistical significance. It is hard to explain the discrepancy. In the study by Darkner et al, the investigators showed that short-term use of AADs reduced the frequency of cardioversions and arrhythmia-related hospitalizations in patients with persistent AF but did not in patients with paroxysmal AF. 8 Most patients included in our study suffered from paroxysmal AF. We hypothesized that patient characteristics (AF type) contributed to the discrepancy, and it needs further investigation. The avoidance of unnecessary physician visits, cardioversions, and hospitalizations after ablation is a very meaningful end point, especially for patients. We expect further studies evaluating the efficacy of such treatment strategies in improving quality of life and reducing cardioversions and arrhythmia-related hospitalizations.
Because of the lack of a unified standard, methods to detect recurrence of AF must be emphasized. As is well known, AF can be paroxysmal and asymptomatic, especially in patients undergoing AF ablation. 28 Thus, it is probable that some AF episodes may be missed by intermittent rhythm monitoring. In our study, most investigators discretely monitored recurrence of AF/AT by combining standard ECGs, Holtor monitoring, and ambulatory ECGs. The effect of such a strategy on verification of LRAF needs to be fully evaluated. Recently, a RCT reported that 7 days of Holtor monitoring at discharge, 3 months, and 12 months after CA recorded only half the episodes of AF verified by implanted cardiac monitors. 29
Limitations
The current meta-analysis presents several limitations. (1) Because of unavailability of raw data, analyses were not stratified by AF type and ablation procedure. However, AF type does not seem to be an important confounder for pooled estimates. In the EAST-AF trial, results remained consistent when patients were stratified according to AF type. 7 (2) In our study, stratified analyses were performed based on study-level data. A statistical association between 2 study-level variables is not equal to association at the individual level. Moreover, the number of studies in each subgroup was small, so the power to detect statistically significant findings was limited. Overall, the results need to be confirmed by patient-level data. (3) Most included studies were nonblinded, and all studies required patients to perform additional ECGs and/or Holtor monitoring if they had symptoms related to arrhythmia. Patients in the control group might have performed more ECGs and/or Holtor monitoring and had more chances to record recurrent AF. (4) The end points were recurrent AF. However, AF recurrence is not failure per se; a reduction in the AF frequency and the duration of episodes also implies treatment success. 2 Thus, AF burden is a more proper end point to assess the efficacy of treatment. (5) Because of the absence of a standard antiarrhythmic treatment postablation, use of AADs varied among studies. (6) Our results are heavily influenced by the results of the EAST-AF trial, which accounted for three-fourths of patients. 7
Conclusions
This meta-analysis of currently available studies demonstrated that short-term use of AADs following AF ablation reduced the incidence of early recurrent atrial tachyarrhythmias but did not prevent LRAF. The necessity of such a treatment strategy needs further evaluation.
Footnotes
Authors’ Note
Buyun Xu and Fang Peng contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.