
Abstract
Introduction
Vitamin D is a fat-soluble vitamin that plays an important role in many physiological functions, including calcium metabolism and homeostasis, the immune system, and cellular proliferation and differentiation. 1 A small amount of vitamin D is obtained through dietary sources. The majority of bodily stores of vitamin D are obtained through synthesis in the skin in response to sunlight.1-3 Vitamin D deficiency remains a common problem in the United States, particularly in colder climates at high latitude, and deficiency of this important vitamin during pregnancy has been linked to maternal and infant health risks. 4
There are 2 major precursors to active vitamin D: ergocalciferol (D2) and cholecalciferol (D3). Both precursors must undergo 2 hydroxylation reactions, first in the liver, where they are converted to 25-dihydroxyvitamin D (25[OH]D), and second in the kidney, in which 25[OH]D is metabolized into the biologically active hormone called calcitriol or 1,25-dihydroxyvitamin D. Plasma levels of 25[OH]D are used to determine vitamin D status. 2 Although there are slight variations in definitions, the US Endocrine Society defines vitamin D deficiency as a 25[OH]D level ≤20 ng/mL. Vitamin D insufficiency is a level between 21 and 29 ng/mL, and a level ≥30 ng/mL is considered sufficient. 5
Common risk factors for vitamin D deficiency include the following: living in areas of high latitude, races with darker skin tones, and covering the skin with clothing.6-9 Obesity at baseline and multiparity are also risk factors contributing to vitamin D deficiency, specifically in pregnant women. 9
In its most severe form, vitamin D deficiency causes osteomalacia in adults and rickets in children. 10 Deficiency of vitamin D during pregnancy can lead to other adverse health outcomes. Women who are pregnant have a greater demand for vitamin D to provide calcium for fetal bone development.11,12 Studies have shown that low levels of vitamin D lead to higher rates of small-for-gestational-age and low-birth-weight infants.2,13,14 Fetal concentrations of vitamin D are dependent on maternal concentrations, so children born to mothers deficient in vitamin D are at risk of neonatal hypocalcemia and infantile rickets. 2 Complications for offspring of vitamin D–deficient mothers can last past the neonatal period. Studies suggest that these children are at an increased risk of developing asthma, type 1 diabetes, upper-respiratory infections, dental caries, and language impairment.15-17 Finally, many studies have shown that a deficiency of vitamin D during pregnancy can contribute to adverse maternal outcomes, including higher rates of preeclampsia, gestational diabetes, primary cesarean section, bacterial vaginosis, and postpartum depressive symptoms.12-14,18,19
Despite the known adverse outcomes of vitamin D deficiency in pregnancy, it remains a common problem. One study in Michigan found that as many as 92.5% of the women studied had a vitamin D level <30 ng/mL during pregnancy (n = 2839). 6 Although vitamin D deficiency in pregnancy is a common problem, there is a lack of consensus on the right amount of supplementation needed during pregnancy. In 2010, the Institute of Medicine stated that a daily intake of 400 to 600 international units (IU) per day was adequate during pregnancy. 20 It is known, however, that in healthy women taking 600 IU daily, the prevalence of vitamin D deficiency still remains high. 21 Most prenatal vitamins only contain 400 IU, so additional supplementation is typically needed. Guidelines from the US Endocrine Society recommend that, at a minimum, pregnant women take a prenatal vitamin containing 400 IU and an additional supplement containing at least 1000 IU. They recognize that 1500 to 2000 IU per day may be needed to maintain levels above 30 ng/mL. 5 Therefore, it is possible that an even higher dose is needed to treat women who are deficient. However, no recommendation of an appropriate dose for pregnant women who are deficient is given. An upper limit of 10 000 IU per day is suggested for pregnant women 19 to 50 years old (with a lower upper limit of 4000 IU in pregnant women <19 years). 5 One study in Canada found that doses of 4000 IU daily for adults was effective at achieving a serum 25[OH]D concentration >30 ng/mL in 88% of individuals, and no adverse effects from supplementation were seen (n = 61). 22 Additionally, a study in South Carolina in pregnant women (n = 161) found that doses of 2000 and 4000 IU daily both improved maternal/neonatal vitamin D status, with the 4000 IU dose achieving a higher vitamin D level. 23 Furthermore, the US Endocrine Society and the American Academy of Family Physicians do not make recommendations on the routine screening of vitamin D in pregnancy, whereas the American College of Obstetricians and Gynecologists suggests only testing pregnant women at elevated risk for vitamin D deficiency (eg, women with darker skin or limited sun exposure). 24
The Women’s Health Specialists (WHS) clinic is located in Minneapolis, MN, with approximately 22 000 patient visits per year. Patients at this clinic are at a high risk of vitamin D deficiency as a result of living in a high-latitude location. Additionally, many patients are of Somalian and other African descents, putting them at a further increased risk because of darker skin pigmentation. The Somalian women are mostly Muslim and are routinely covered throughout the year. In February of 2013, the WHS clinic initiated a new protocol for vitamin D supplementation and treatment of deficiency during pregnancy. The protocol was developed by the clinical pharmacist and medical director, based on the US Endocrine Society guidelines. The protocol was reviewed and approved by the provider team. Providers were educated at provider meetings, and the protocol was distributed electronically and available in hard copy form throughout the clinic. Prior to the implementation of this protocol, pregnant women were typically screened for vitamin D deficiency twice during their pregnancy (typically at initial intake visit and at approximately 28 weeks), and specific recommendations for vitamin D supplementation were decided by the individual provider. The new protocol calls for routine screening of vitamin D levels in all women at 2 specified time points throughout prenatal care: once at the initial prenatal visit and once at approximately 28 weeks’ gestation. Women with an initial vitamin D level ≥30 ng/mL are recommended to take 2000 IU vitamin D per day. Women falling below this are recommended to take 5000 IU daily throughout pregnancy. This dose was chosen because of the 2 studies that found that 4000 IU daily is enough to achieve sufficiency,22,23 and the 5000 IU dosage form is more conveniently available. Most local pharmacies readily carried 1000 IU, 2000 IU, and 5000 IU dosage forms, and taking one 5000 IU capsule was less pill burden than taking two 2000 IU tablets daily. This study aims to identify the prevalence of vitamin D deficiency in pregnant women and to analyze the impact of the implementation of a vitamin D deficiency screening and treatment protocol for pregnant women.
Methods
Study Setting and Data Source
This study was a retrospective chart review of women receiving prenatal care at the WHS clinic in Minneapolis, MN. Electronic medical records (EMRs) were utilized to create reports of all women who received prenatal care during the 2 time periods of April 1, 2011, through December 1, 2012 (preprotocol group) and July 1, 2013, through June 30, 2014 (postprotocol group), corresponding to before and after the treatment protocol was implemented. During these time periods, 722 women who received prenatal care were identified. EMRs were randomly reviewed by selecting every fourth EMR (returning to the beginning of the list and starting from the second after the list was exhausted) from each time period by 2 reviewers. Women were included in the study if they were followed for a documented pregnancy and had at least 2 documented vitamin D levels at any time during pregnancy. Exclusion criteria included a history of gastric bypass because this procedure affects intestinal absorption of vitamin D and causes high rates of vitamin D deficiency. 25 If women experienced multiple pregnancies during the study time frame, they were only included once. A convenience sample of 100 patients per time period was chosen. The final sample size of this study is 200, and the flow of selected charts is summarized in Figure 1. This study was approved through expedited review by the University of Minnesota Institutional Review Board.
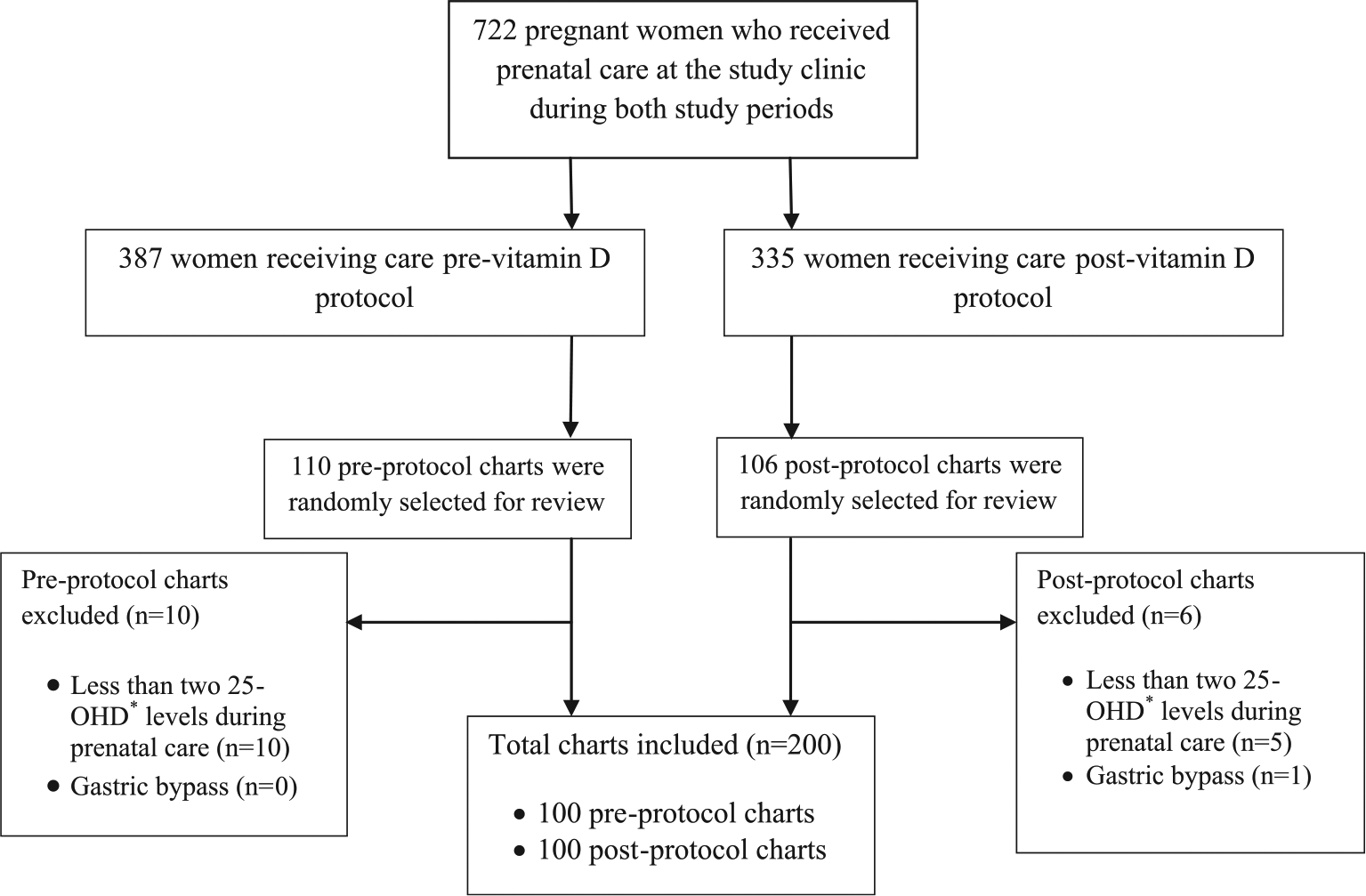
Flow of selected charts included in the study (*25-[OH]D stands for 25-dihydroxyvitamin D).
Measures
Vitamin D
Daily dose of vitamin D (<1000, 1000-2999, 3000-4999, or ≥5000 IU) was included. Reason for taking vitamin D was included and categorized as follows: patient reported, provider recommended without evidence of prescription, provider prescribed, or not applicable/missing. Vitamin D status (deficient, insufficient, or sufficient) was also included, and the classification was based on the US Endocrine Society guideline recommendations (≤20 ng/mL as deficiency, 21-29 ng/mL as insufficiency, and ≥30 ng/mL as sufficiency). 5 Finally, protocol adherence (followed, not followed, or unknown) of taking vitamin D was collected for the postprotocol group.
Covariates
Patient’s age (18-25, 26-30, 31-35, or 35-44 years), patient-reported race/ethnicity (African, American-other, Caucasian, or Others), and gestational age at the time of first vitamin D level checked (<10, 10-14, or ≥15 weeks) were included.
Analysis
The primary objective of the study was to evaluate the prevalence of vitamin D deficiency. Therefore, characteristics between study groups were examined. Cross-tabulations and Pearson’s χ2 tests were used to determine differences by study period. Secondary outcomes included evaluating the impact of protocol implementation. To complete this, achievement of vitamin D sufficiency was assessed by study period and initial status of vitamin D using Pearson’s χ2 tests. Additionally, the degree of protocol adherence among the postprotocol group was evaluated by reason for taking vitamin D and sufficiency status of vitamin D, using Pearson’s χ2 tests. All statistical analyses were conducted using Stata 13.1.
Results
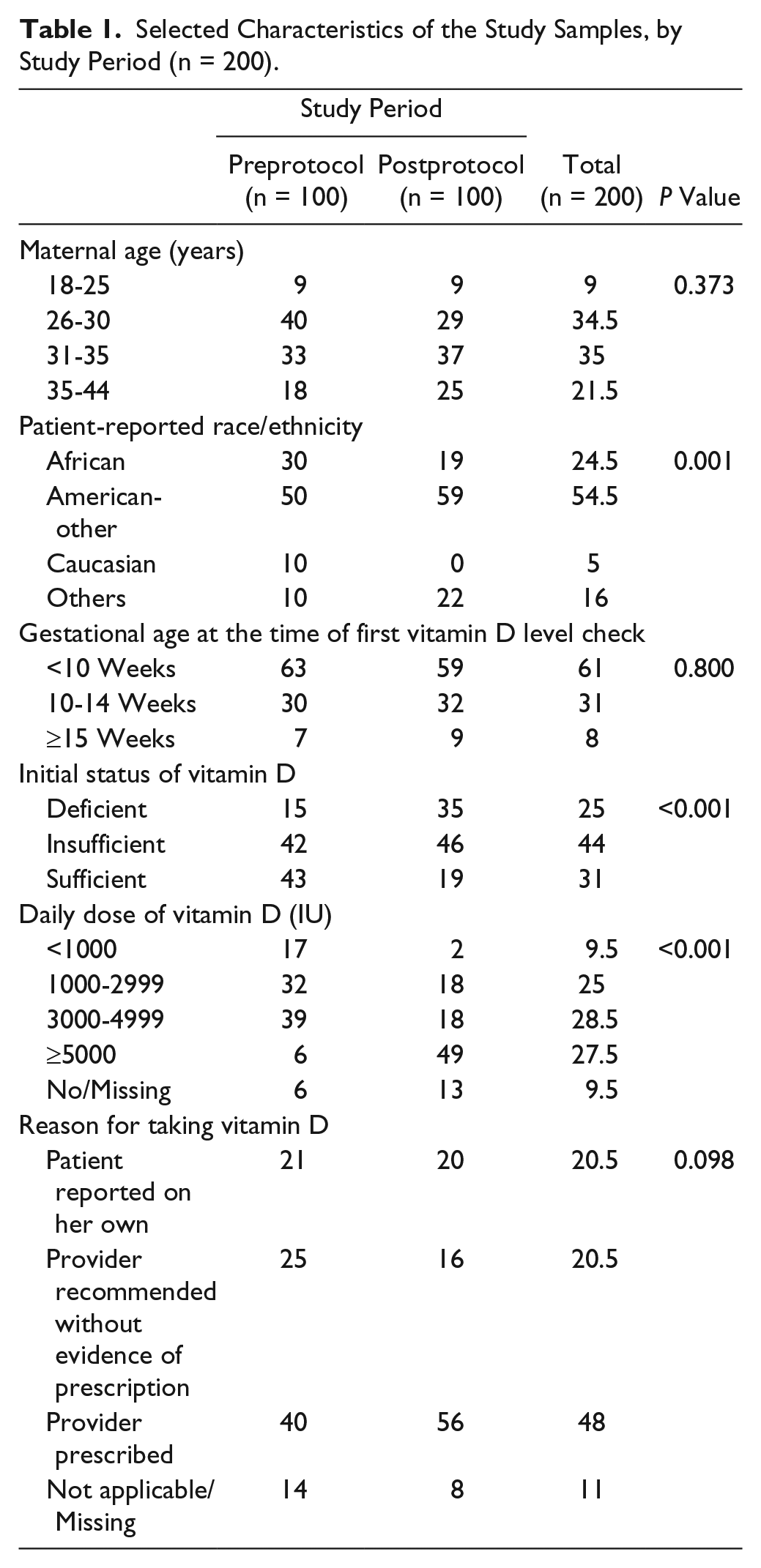
Patient characteristics were similar among study periods, except patient-reported race/ethnicity (P = 0.001), the daily dose of vitamin D (P < 0.001), and initial status of vitamin D (P < 0.001; Table 1). In the preprotocol group, 6% of women had doses of 5000 IU or higher of vitamin D daily, whereas 49.0% of women in the postprotocol group received 5000 IU or more of vitamin D daily. Across the protocol groups, 56.5% of women were 31 years old or older, and 61% of women had their first vitamin D level checked prior to 10 weeks’ gestation. Also, 48% of women reported taking vitamin D as their providers prescribed at clinic visits, though it was not possible to confirm adherence.
Selected Characteristics of the Study Samples, by Study Period (n = 200).
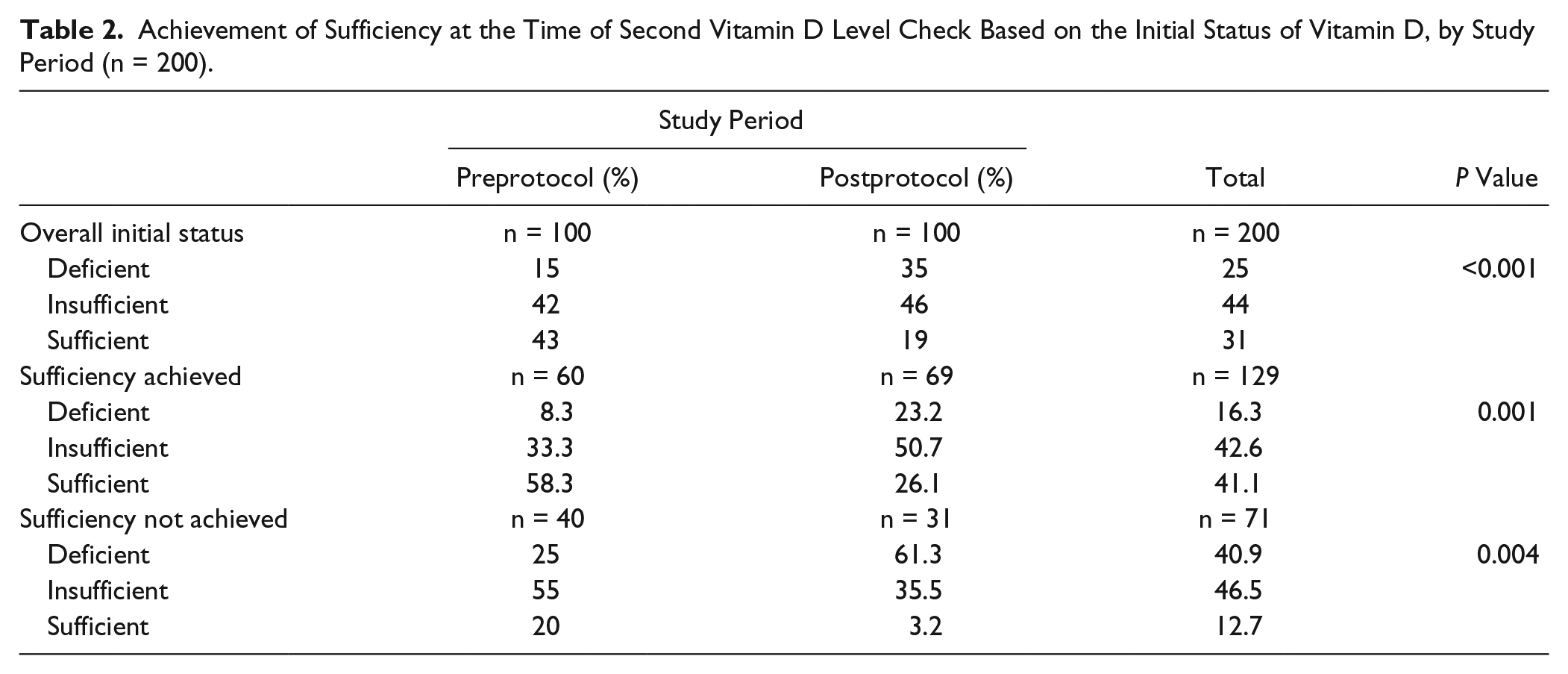
In both study period groups, initial vitamin D levels were either deficient or insufficient in more than half of the women at baseline (Table 2). The postprotocol group had a significantly lower percentage of women with a sufficient initial level than those of the preprotocol group (19% vs 43%, P < 0.001). Although not statistically significant, the postprotocol group had more women who achieved vitamin D sufficiency compared with the preprotocol group (69% vs 60%, P = 0.184), despite the fact that the postprotocol group had a higher percentage of women who were deficient at baseline (15% vs 35%, P < 0.001). Among women who achieved sufficiency at the time the second vitamin D level was checked, 58.3% had a sufficient initial level in the preprotocol group, and this was significantly different from those of the postprotocol group (26.1%; P = 0.001). Among women who did not achieve sufficiency in the postprotocol group, 61.3% had a deficient level of vitamin D during their initial check, and this was significantly different from those in the preprotocol group (25.0%; P = 0.004).
Achievement of Sufficiency at the Time of Second Vitamin D Level Check Based on the Initial Status of Vitamin D, by Study Period (n = 200).
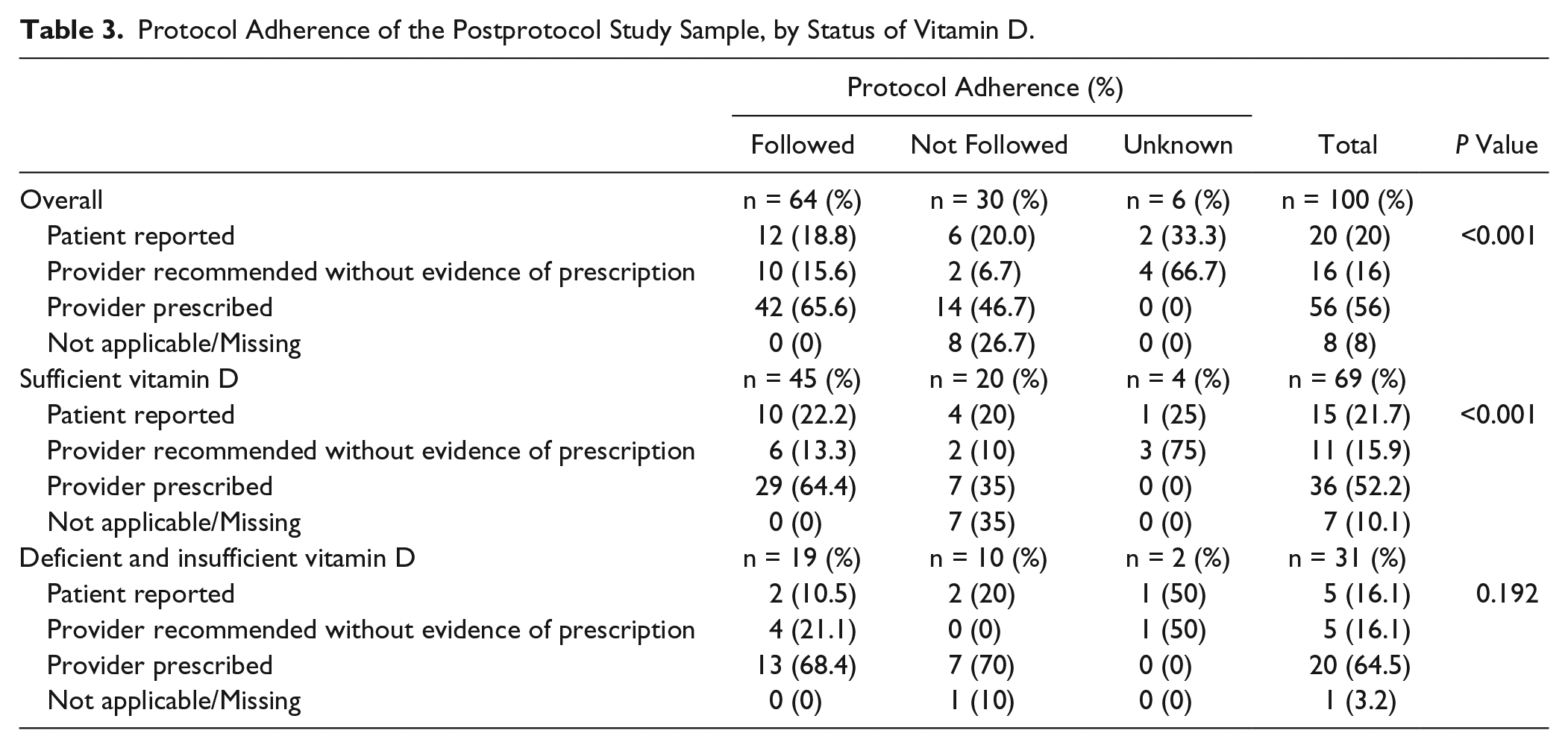
Overall, 64% of the postprotocol study samples adhered to the protocol, and 65.6% of these women were prescribed vitamin D (Table 3). Vitamin D supplement was more frequently prescribed when providers followed the protocol (P < 0.001). Among women who followed the protocol and achieved sufficiency, 64.4% took vitamin D because of the direct prescription by their providers, compared with those who did not follow protocol (P < 0.001).
Protocol Adherence of the Postprotocol Study Sample, by Status of Vitamin D.
Discussion
The results of this retrospective chart review confirmed that vitamin D deficiency is a prevalent problem in this population of pregnant women. This was expected because women at this clinic have known risk factors for low vitamin D levels, including living in a cold, high-latitude climate and dark skin pigmentation. One review reports a prevalence of vitamin D deficiency of 5% to 20% in light-skinned populations and 30% to 70% in dark-skinned or veiled populations. 3 However, one study in Sweden studied a light-skinned population living at a latitude of 57°N to 58°N and found an overall rate of deficiency of 65%, which increased to 85% during winter months. 26 The results of the Swedish study are more comparable with the rates seen at the WHS clinic, which is at a latitude of 45°N. Additionally, a study performed in Detroit, MI, found a prevalence of deficiency that was as high as 92.5%. 6 This study contained a patient population similar to that of the WHS clinic, including a mix of African, Asian, and Middle Eastern women and women who remain veiled.
The patient population in this review was diverse and included women from various ethnic backgrounds. The majority of women reported that their ethnic background was either “American” or “Other.” The “American” category may have included individuals from any ethnic background who prefer to describe their ethnic background as “American.” Alternatively, “American” is the default setting in the local EMR, and it is possible many patients were never asked to report their ethnicity in the registration process. Because of the limitation in the accuracy of the ethnicity data, subgroup analysis of lighter- and darker-skin-pigmented women was not possible in this study.
The results of this review showed that there was an increase in the number of women able to achieve sufficiency and that the amount of this increase was higher in the postprotocol group than in the preprotocol group. Despite a much larger percentage of women who were not initially sufficient in the postprotocol group, an overall greater percentage of women reached sufficiency in this group, though it was not statistically significant. Additionally, a higher percentage of women were initially deficient and required a greater increase in their vitamin D level to achieve sufficiency. The vitamin D protocol was created to give guidance to clinicians on the appropriate supplementation for women to either maintain or achieve sufficiency. There is currently a lack of data on the exact doses of vitamin D needed to achieve sufficient 25[OH]D levels. Guidelines from the US Endocrine Society state that pregnant and lactating women may need doses of 1500 to 2000 U/d to maintain levels ≥30 ng/mL, but the guideline do not address what dose should be used for pregnant women who are initially deficient in order to achieve levels ≥30 ng/mL. 5 In this review, the doses either prescribed, recommended, or patient reported followed the established protocol 64% of the time. Nonadherence to the protocol was often associated with patients whose initial levels were <30 ng/mL, for whom the clinician either prescribed or recommended 4000 IU daily, as opposed to the 5000 IU outlined in the protocol. Therefore, although this dose did not technically follow the protocol that was created, this was still clinically appropriate, considering the lack of conclusive data on the exact dose needed to achieve sufficient vitamin D levels.
Vitamin D supplementation use was well documented in both groups: 86% of women in the preprotocol group had documentation of supplement use, despite no protocol being in place at the time. The key difference between the preprotocol and postprotocol groups was the dosing of the vitamin D (6% of the preprotocol group vs 49% of the postprotocol group were on ≥5000 IU daily). This experience illustrates the need to supplement vitamin D in adequate doses in order to achieve sufficiency.
Overall, prescribing of supplements was the most common method used by clinicians in this study, although it was more common for those who were initially not sufficient than in those who were sufficient. Although the supplements are available over the counter, many of the providers choose to write a prescription, so that the dose is documented in the chart and there is a lower chance of a miscommunication with the patient regarding dosing. This is likely a result of providers having heightened concern about initial lab values that are abnormal. The act of prescribing a supplement did not necessarily lead to a higher percentage of women achieving sufficiency.
A significant limitation of this study was the lack of information about confounding variables, such as adherence to supplement use, diet, and sun exposure. 26 Vitamin D levels were not linked to the month evaluated in the data analysis, which limits ability to draw any conclusions related to season. The difference in the initial prevalence of vitamin D deficiency and insufficiency between the preprotocol group and the postprotocol group (combined deficiency/insufficiency 57% vs 81%) could have potentially been related to the difference in study time periods. The time period during which the report was created for the preprotocol group was slightly longer and included a greater number of summer months than the report for the postprotocol group. Because of the retrospective nature of the study design, only information that was documented in the patient’s medical chart was available. Therefore, adherence data were unavailable, and it was unknown if women missed doses or whether a prescribed supplement was filled and picked up. Further prospective studies documenting patient adherence with supplementation use and dose would help evaluate the proper dose needed to maintain or raise vitamin D levels. Finally, the preprotocol group had more cases excluded because they did not have 2 vitamin D levels drawn. Because this practice became more standardized after the implementation of the protocol, it is possible that women in the preprotocol groups were more likely to have screening completed by their provider because they had more risk factors.
Conclusion
In conclusion, this review demonstrated that there is a high prevalence of vitamin D deficiency during pregnancy at this women’s health clinic in Minneapolis, MN. Adequate vitamin D levels are an important component for the proper health of both a mother and her baby because insufficient levels may be linked to higher rates of birth complications. Implementation of a clinic-wide protocol for vitamin D supplementation during pregnancy resulted in a nonsignificant increase in the percentage of women who were able to achieve a status of vitamin D sufficiency. Ensuring adequate supplementation for women during pregnancy is vital to achieving sufficient vitamin D levels and positive maternal and fetal outcomes.
Footnotes
Authors’ Note
Drs Awker and Herbranson were students in the doctor of pharmacy (PharmD) program at the University of Minnesota College of Pharmacy during the time of this research. Dr. Rhee’s PhD degree is final in August 2016.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.