
Abstract
Introduction
Heparin-induced thrombocytopenia (HIT) is a potentially life-threatening immune-mediated reaction to heparin therapy that can lead to thrombosis, limb loss, or death. It is associated with a prothrombotic state in which immunoglobulin G antibodies form against heparin and platelet factor 4 (PF4) complexes. 1 This complex promotes platelet aggregation and activation (thrombocytopenia) as well as thrombin generation through platelet activation and tissue factor release by endothelial cells. 1 Early recognition of this phenomenon through clinical probability scoring with calculation of the 4T score, 2 supporting laboratory analysis,3,4 and avoidance of heparin with alternative anticoagulation is paramount. 1
Bivalirudin is a parenteral direct thrombin inhibitor (DTI) that has been approved by the Food and Drug Administration (FDA) for percutaneous transluminal coronary angioplasty and percutaneous coronary intervention (PCI) in patients with or without HIT and has been used off-label for the treatment of HIT.5-9 Unlike other DTIs, bivalirudin does not rely on hepatic metabolism and is extensively degraded by plasma proteolytic cleavage, with only a minor (approximately 20%) component of renal clearance. Its short half-life of approximately 25 minutes, in patients with normal renal function, provides rapid elimination from the body in the absence of an antidote. 10 Despite the lack of FDA approval in the treatment of HIT, several studies have demonstrated effective anticoagulation and evaluated dosing schemes in various clinical scenarios.5-9
One complicating aspect shared among all DTIs is the prolongation of the prothrombin time (PT) and resultant elevation in the international normalized ratio (INR). This elevation can lead to confusion when transitioning patients from bivalirudin to warfarin therapy because INR values are rendered inaccurate for monitoring warfarin effect. Each intravenous DTI displays varying degrees of INR elevation. Argatroban is associated with the highest level of PT prolongation, followed by bivalirudin and lepirudin, respectively. 11 There is little literature regarding the transition from bivalirudin to long-term anticoagulation with warfarin, leading to an inconsistent and potentially high-risk approach to transitioning patients. With the regular use of bivalirudin at our institution, we created a clear and simplistic approach to bridging bivalirudin to warfarin and implemented a transition protocol in September 2013 (Figure 1). This protocol was approved by our institution’s Antithrombotic Task Force and was incorporated into our HIT treatment guideline and electronic health record.
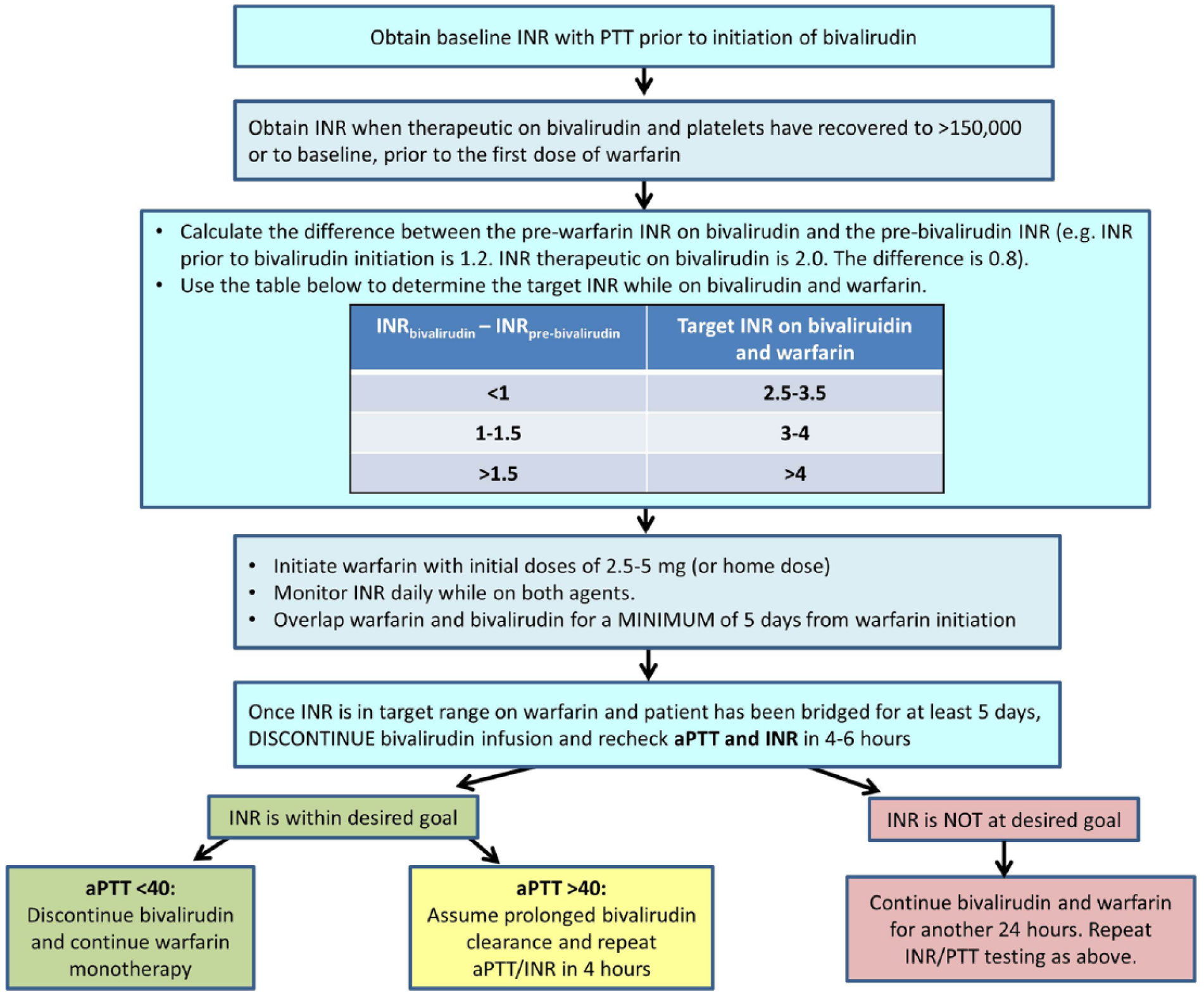
Bivalirudin transition protocol.
The primary aim of this study was to assess the transition from bivalirudin to warfarin as measured by successful attainment of target INR values before and after the implementation of the institution-wide transition protocol.
Methods
This retrospective analysis was reviewed by our institution’s investigational review board and determined that no consent was required. Patients receiving bivalirudin therapy were identified from our electronic health record between January 2012 and June 2015. Patients treated before the implementation of our protocol were assigned to the preprotocol group, whereas patients treated with bivalirudin after September 2013 were assigned to the postprotocol group. Bivalirudin was dosed in both groups according to a hospital-wide, pharmacist-driven dosing protocol, whereas warfarin dosing was left to the treating provider in both study groups. The following entry criteria were used to identify study patients: bivalirudin therapy for an indication other than procedural use (suspected or confirmed HIT, history of HIT, suspected or confirmed antithrombin deficiency, bridging postcardiac surgery per local practice) and transitioned to warfarin. Indications for bivalirudin were determined by reviewing provider documentation in the medical record and serological testing results. A diagnosis of HIT was confirmed through documented history of HIT and intermediate or high probability of HIT (4T score of ≥4), with either a positive antiheparin/PF4 antibody assay (optical density ≥1.0), a positive serotonin release assay, or a strong clinical suspicion for HIT despite negative laboratory testing. Patients were required to have a planned transition from intravenous bivalirudin to oral warfarin, also defined as warfarin prescribed at discharge. Patients receiving >1 dose of warfarin at the time of bivalirudin initiation, along with those who received intraprocedural bivalirudin for the indication of PCI, coronary artery bypass grafting, or vascular intervention during admission were excluded.
Provider documentation, lab values, and medication administration records were used to determine study end points. Data collected from patient records consisted of a baseline INR value prior to bivalirudin initiation when available, prewarfarin INR while receiving bivalirudin, last recorded INR while on both bivalirudin and warfarin, first INR drawn a minimum of 2 hours after discontinuation of bivalirudin, any subsequent INR draw within 24 hours of bivalirudin cessation, and all recorded times for bivalirudin initiation, warfarin initiation, and INR draws after bivalirudin discontinuation. Target INR goals on discontinuation of bivalirudin were predetermined by the prescribing provider and recorded from each medical record. The implemented protocol recommends the attainment of both an INR and an activated partial thromboplastin time (aPTT) at the time of bivalirudin discontinuation to rule out any sustained effects of bivalirudin as a result of prolonged clearance. For the purpose of this study, the primary outcome of successful transition was defined as patients achieving a therapeutic INR measurement after the discontinuation of bivalirudin. The INR used for determination of successful transition was the first INR obtained with a concomitant aPTT value <45 s because the effect of bivalirudin on the INR should be minimal. If the INR value was not obtained with an aPTT, the first follow-up INR obtained at least 4 hours after bivalirudin discontinuation was used. In the event that there was only one follow-up INR or aPTT measurement obtained after the discontinuation of bivalirudin, this value was used regardless of the aPTT result. Secondary outcomes of this study included hospital length of stay, time of total bridge therapy from bivalirudin to warfarin, and total length of bivalirudin therapy. Safety outcomes were assessed in patients hospitalized for >24 hours after bivalirudin discontinuation and included INR values outside the therapeutic goal range, any documented bleeding event within 72 hours of bivalirudin discontinuation, arterial or venous thrombosis within 72 hours of bivalirudin discontinuation, or the withholding of warfarin or use of anticoagulant reversal agents or packed red blood cell transfusions within 48 hours after the discontinuation of bivalirudin. The shorter time period for withheld warfarin doses or anticoagulant reversal agents was selected to demonstrate events surrounding the transition from bivalirudin rather than nonprotocolized warfarin dosing. Thrombosis was defined as any documented event originating from arterial or venous sources, including venous thromboembolism (VTE; pulmonary embolism/deep vein thrombosis), myocardial infarction, and stroke. Defined agents for the use of anticoagulant reversal included vitamin K, prothrombin complex concentrate, fresh frozen plasma, and recombinant factor VIIa.
Because of the small population, data for the total cohort of this study were presumed to not be normally distributed; therefore, continuous variables are presented as median values with interquartile ranges. A χ2 test or Fisher’s exact test was used when comparing dichotomous variables in the treatment groups. Continuous variables were analyzed using the Wilcoxon rank sum test. Levene’s test for homogeneity was used to test the variability between the 2 groups for the outcome of “off bivalirudin INR.” P values ≤0.05 were considered to indicate a statistically significant difference. All statistics were analyzed using SAS statistical add-in (version 5.1) for Microsoft Excel 2010.
Results
A total of 262 patients received bivalirudin for nonprocedural systemic anticoagulation between January 2012 and June 2015. A total of 39 patients were included in the preprotocol (n = 19) and postprotocol (n = 20) groups (Figure 2). Baseline characteristics of the 2 groups are shown in Table 1. The groups were well matched in age, weight, body mass index, baseline creatinine clearance, and indication for bivalirudin therapy. More patients in the preprotocol group had an indication for anticoagulation for VTE compared with the postprotocol group (57.9% vs 30.0%, P = 0.079); however, fewer patients in the preprotocol group had mechanical heart valves (5.3% vs 30.0%, P = 0.092). Overall, 22 of the total number of 39 patients (56.4%) had confirmed cases of HIT as the indication for bivalirudin therapy, followed by 7 patients with a history of HIT, 9 patients with suspected/clinical HIT, and 1 patient in the postprotocol group with an antithrombin III (ATIII) deficiency.
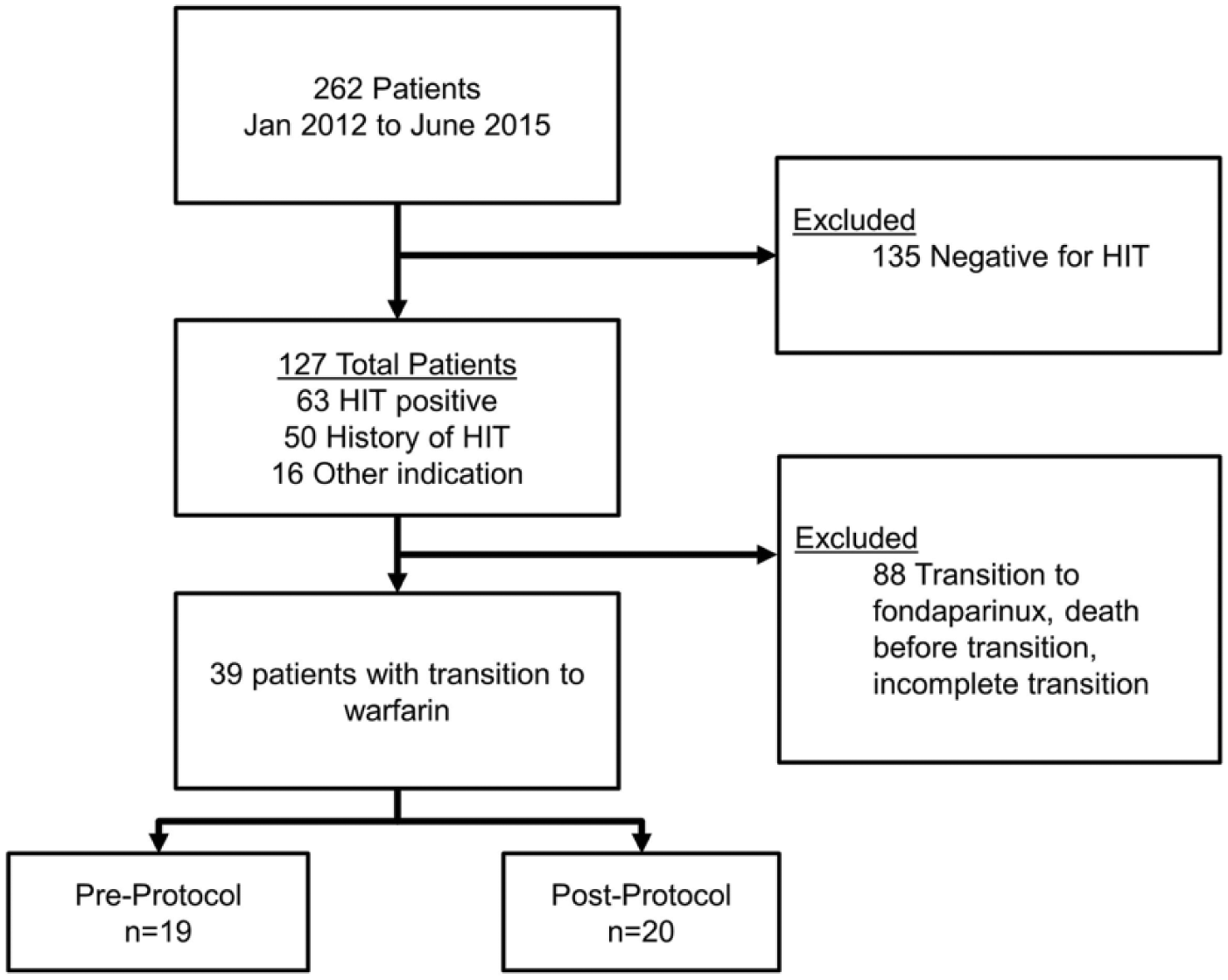
Patient selection.
Baseline Demographic and Clinical Characteristics. a
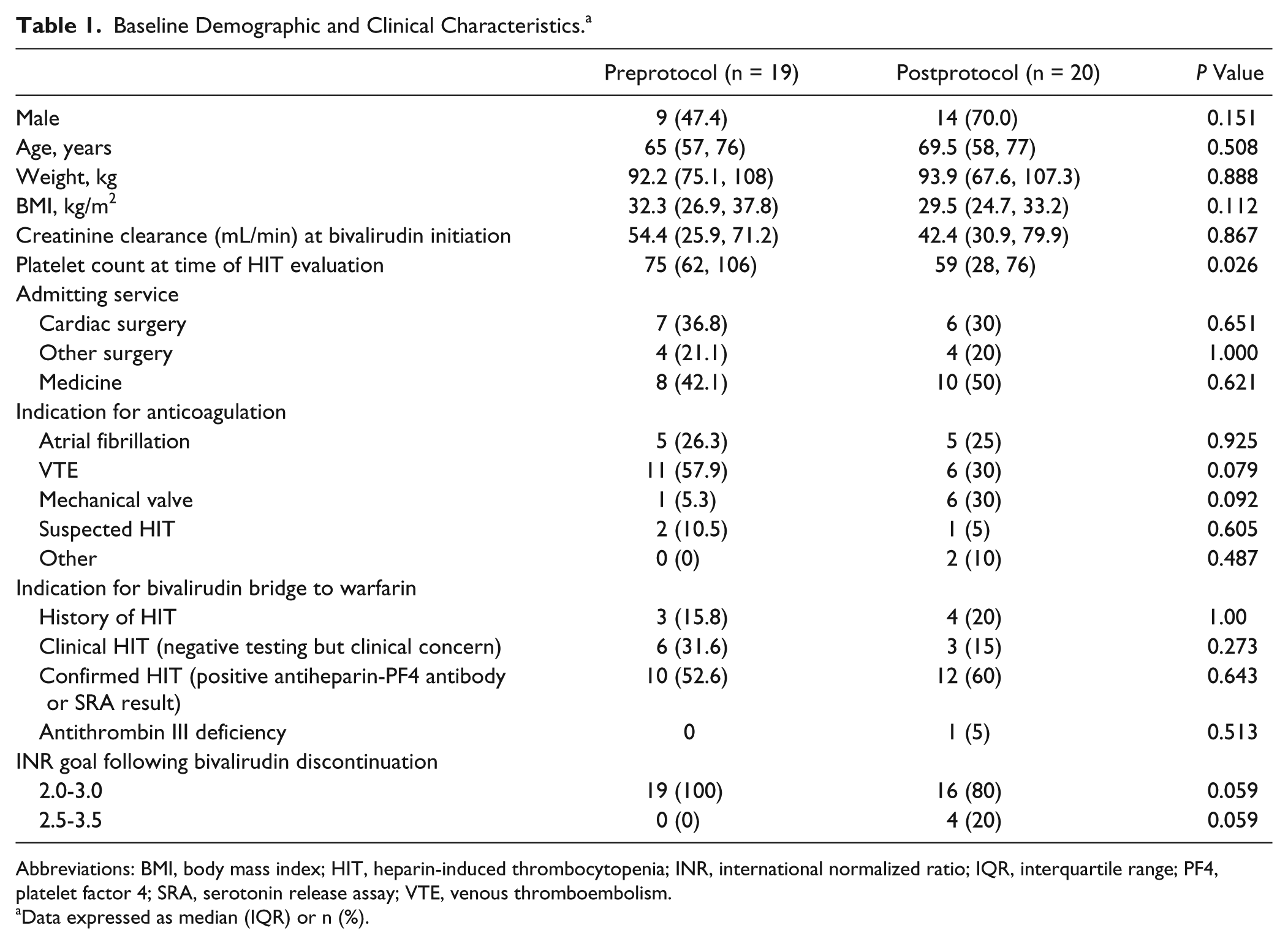
Abbreviations: BMI, body mass index; HIT, heparin-induced thrombocytopenia; INR, international normalized ratio; IQR, interquartile range; PF4, platelet factor 4; SRA, serotonin release assay; VTE, venous thromboembolism.
Data expressed as median (IQR) or n (%).
The percentage of patients achieving a successful transition was significantly higher in the postprotocol group compared with the preprotocol group (80.0% vs 42.1%, P = 0.015; Table 2). Of those patients who did not achieve a successful transition, a larger number in the preprotocol group had supratherapeutic INRs on bivalirudin discontinuation compared with the postprotocol group (47.4% vs 15.0%, P = 0.041). In all, 13 (68.4%) patients in the preprotocol group and 12 (60%) patients in the postprotocol group were hospitalized for more than 24 hours after bivalirudin discontinuation and were assessed for safety outcomes. Bleeding events within 72 hours after the discontinuation of bivalirudin occurred at a similar frequency between the 2 groups (3/13 [23.1%] vs 2/12 [16.7%], P = 0.689). Bleeding events in the preprotocol group included epistaxis (n = 1), vaginal bleeding (n = 1), and bleeding at the site of PEG tube (n = 1), which occurred after discontinuation of bivalirudin therapy. Bleeding events in the postprotocol group included 2 events of hematochezia. Withheld warfarin doses or the use of anticoagulant reversal agents within 48 hours of the discontinuation of bivalirudin were numerically lower in the postprotocol group compared with the preprotocol group; however, this difference was nonsignificant (2/12 [16.7%] vs 6/13 [46.2%], P = 0.202; Table 2). Six patients in the preprotocol group required withholding of warfarin doses, with 1 patient requiring administration of packed red blood cells; 2 patients in the postprotocol group had doses of warfarin withheld, with 1 patient receiving packed red blood cells. No events of thrombosis were observed within 72 hours after discontinuation of bivalirudin in either group. In addition to the increased percentage of patients achieving INR values within the therapeutic range, patients in the postprotocol group had less variability in their postbivalirudin INR values (Figure 3) compared with those in the preprotocol group.
Study Outcomes. a
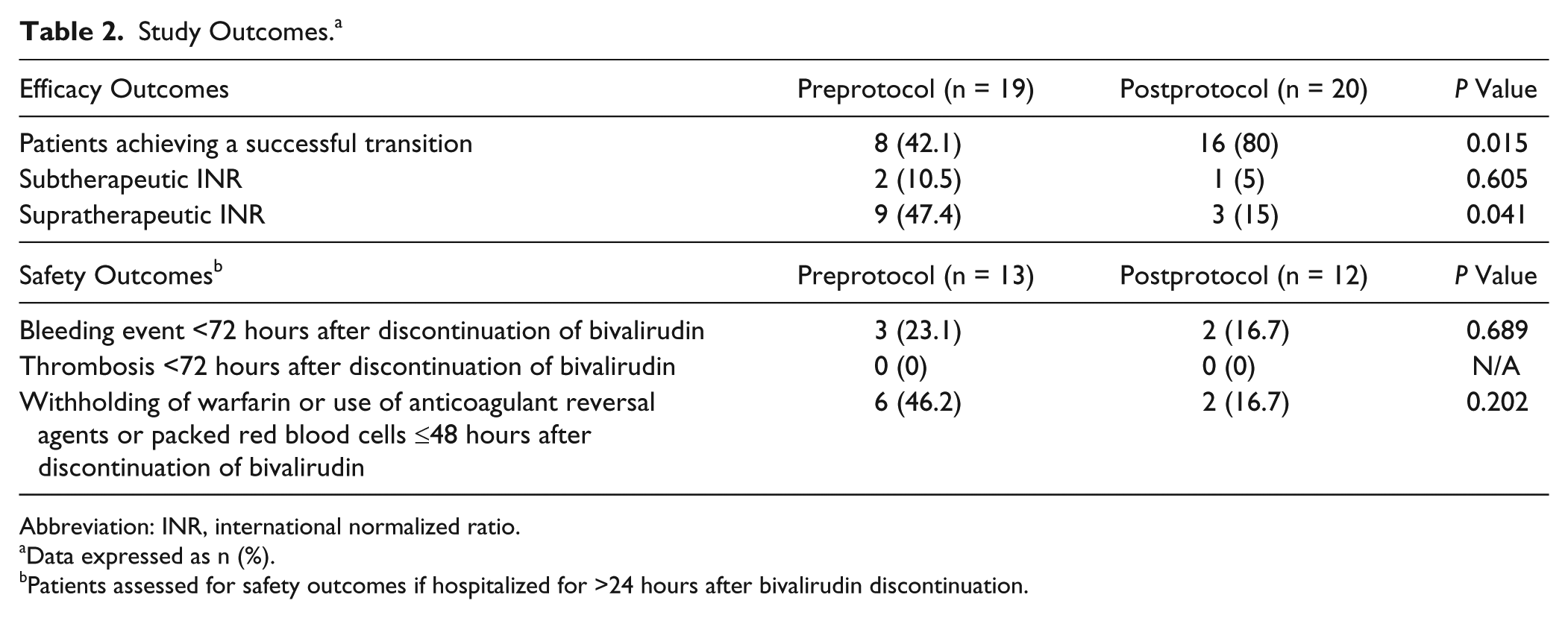
Abbreviation: INR, international normalized ratio.
Data expressed as n (%).
Patients assessed for safety outcomes if hospitalized for >24 hours after bivalirudin discontinuation.
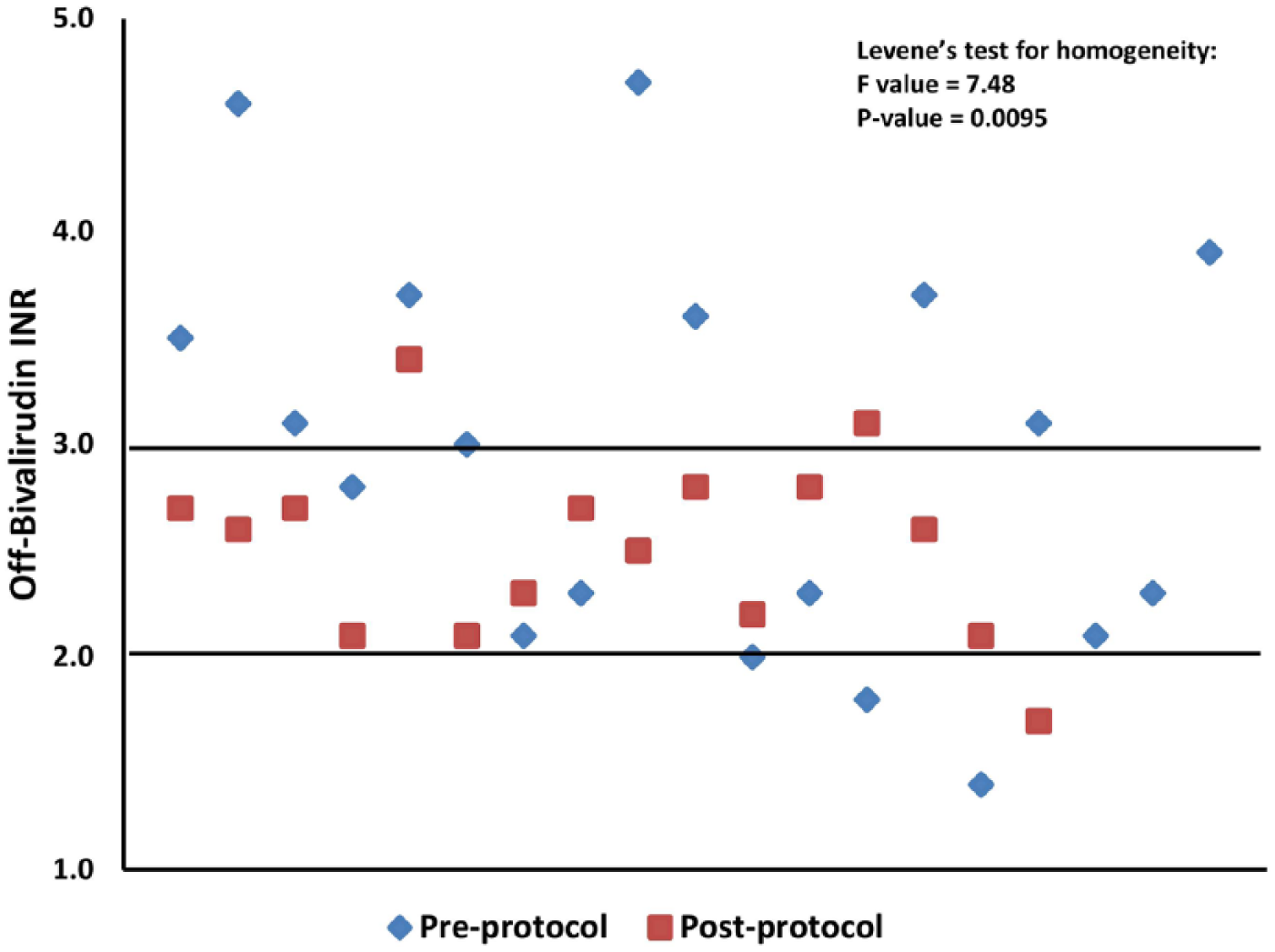
Scatter plot of first INR value of each patient recorded after the discontinuation of bivalirudin. Horizontal lines within the graph represent the typical INR goal range of 2 to 3 once bivalirudin was discontinued. Patients with a target INR goal of 2.5 to 3.5 on discontinuation of bivalirudin were excluded from this figure (n = 4).
The median length of stay was 25.9 (16.9, 40.6) days in the preprotocol group compared with 16.1 (10.9, 22.4) days in the postprotocol group (P = 0.067; Table 3). Median time durations of bridge therapy from warfarin initiation to bivalirudin discontinuation in the preprotocol and postprotocol groups were 4.7 (3.1, 8.4) days and 4.5 (2.8, 5.2) days, respectively (P = 0.318). Total median lengths of bivalirudin therapy in the preprotocol and postprotocol groups were 13.7 (7.8, 15.5) days and 8 (6, 12.2) days (P = 0.054), whereas time to warfarin initiation was 5.3 (3.1, 10.1) and 3.7 (2.6, 6.2) days in the preprotocol and postprotocol groups, respectively (P = 0.164).
Treatment Summary. a
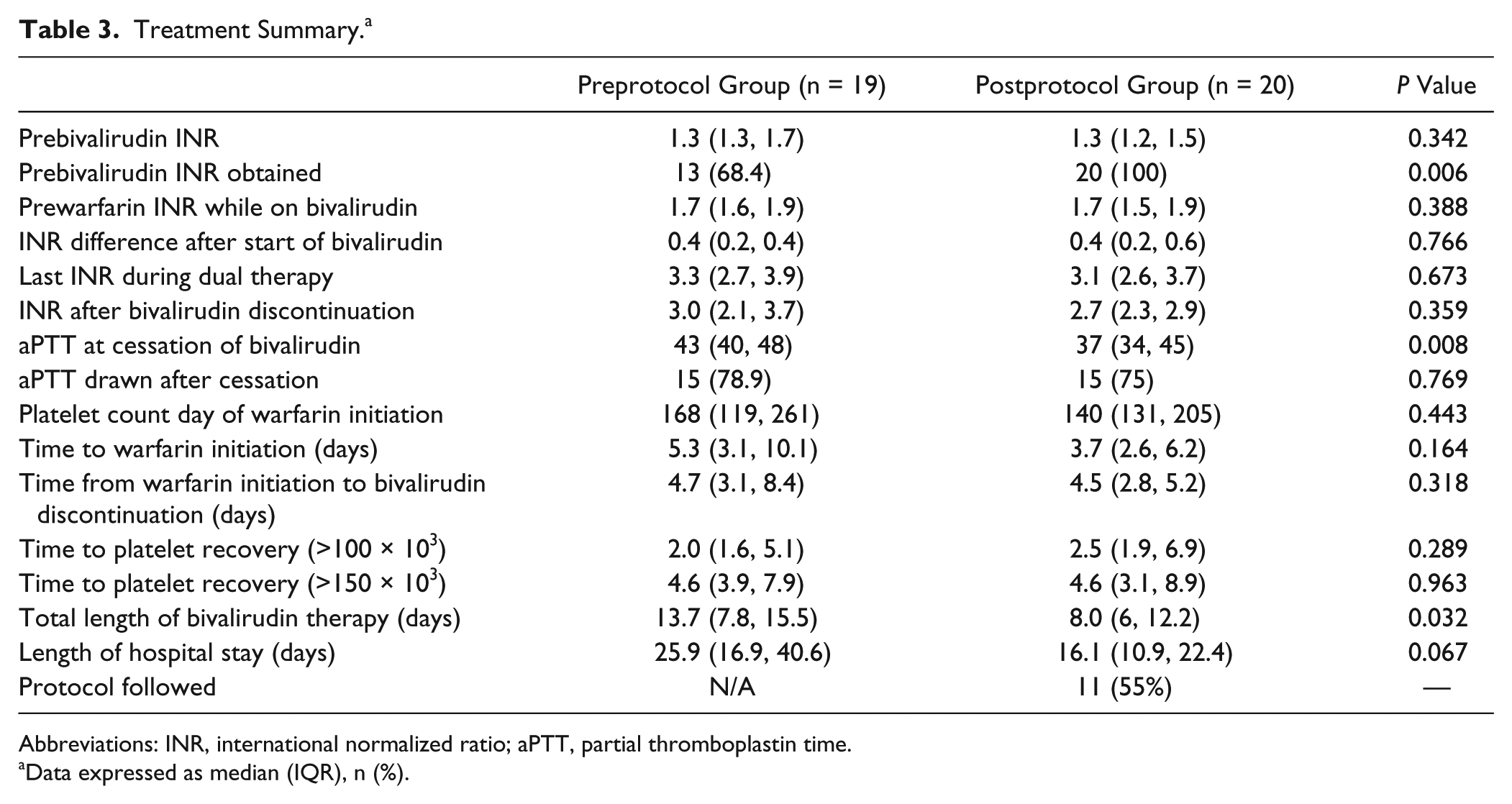
Abbreviations: INR, international normalized ratio; aPTT, partial thromboplastin time.
Data expressed as median (IQR), n (%).
Adherence to the protocol when assessed for achievement of target INR was met in 17/20 (85%) patients. The protocol was correctly implemented in its entirety in 11/20 (55%) patients in the postprotocol group (Table 3). The majority of the transitions not meeting 100% adherence were a result of bivalirudin overlap therapy of less than 5 days (6/20, 30%). Of these 6 patients, 2 patients received 4 days of overlap therapy and were being bridged to warfarin for atrial fibrillation; 2 patients tested negative for HIT and were not undergoing treatment for active thrombosis; 1 patient was bridged for HIT without thrombosis; and 1 patient was found to be sensitive to warfarin, with INR rising to 4.8 by day 3 of combination therapy with bivalirudin and warfarin. The remaining 3 patients where the protocol was not entirely followed either did not meet the target INR while on both bivalirudin and warfarin (n = 2) or exceeded the INR target (n = 1) prior to the cessation of bivalirudin.
Discussion
Limited availability of FDA-approved drugs for the treatment of HIT has led to the use of alternative therapies. The only available FDA-approved agent for HIT in the United States, argatroban, has been associated with complex dosing regimens and therapeutic monitoring, leaving bivalirudin as a favorable option. 6 Although transitions to oral anticoagulation from argatroban have been studied and recommendations exist, the varying degrees of INR elevation between argatroban and bivalirudin have left a gap in knowledge for the transition of patients to vitamin K antagonists from bivalirudin. Data from our study show that the implementation of a standardized bivalirudin-warfarin transition protocol led to a significant increase in percentage of patients successfully achieving a therapeutic INR (42.1% preprotocol vs 80% postprotocol, P = 0.015) on bivalirudin discontinuation. Implementation of our standardized transition protocol was associated with a reduced number of patients requiring interruption of warfarin doses or use of reversal agents following the cessation of bivalirudin therapy.
Published data to guide the transition from bivalirudin to warfarin are extremely limited. Available data with argatroban studies have offered some direction on this issue; however, the use of argatroban transition guidelines in relation to bivalirudin are not ideal because they may lead to an overestimation of goal INR values and increased bleeding risk. Argatroban labeling recommends doses up to 2 µg/kg/min be discontinued when the INR is greater than 4. The package insert recommends that an INR be repeated 4 to 6 hours after discontinuation of argatroban, restarting argatroban if the INR is below the desired therapeutic range and repeating until the desired therapeutic range of warfarin alone is achieved.12,13 Alternative guidance with argatroban has shown the use of an international sensitivity index (ISI)-based calculation for the prediction of INR values on warfarin monotherapy using a mathematical equation with the INR on combination therapy (argatroban and warfarin). 14 This calculation is likely burdensome to the average clinician because it requires one to identify the ISI value of the thromboplastin reagent used in that specific institution’s coagulation laboratory.
Clinical studies evaluating argatroban to warfarin transition have highlighted the difficulty of managing this situation.15,16 One study prospectively identified 304 patients from a previous trial treated with argatroban for HIT, 165 of whom were transitioned from argatroban to warfarin therapy without a standardized approach. 16 Argatroban and warfarin therapy overlapped for a median of 4 days, during which time 86 (54%) of 159 patients with available data had an INR greater than 5 (median maximum INR = 5.3; maximum value = 16). Posttransition INR values were available in 108 patients and showed that 43 (40%) patients had a therapeutic INR, 34 (31%) had subtherapeutic INR values, and 31 (29%) had supratherapeutic INR values on the completion of the transition. 16 Rates of therapeutic INR values achieved after the discontinuation of argatroban were well below the rates observed in our study, further confirming the significance of a standardized transition protocol. Compared with this argatroban study, results from these data were consistent in terms of length of transition times along with nonsignificant rates of bleeding.
The implemented bivalirudin transition protocol in this study took a simplistic approach to calculating goal INR levels, factoring in the lesser degree of INR elevation attributed to bivalirudin along with individual responses to therapy. Previous studies have documented an INR increase ranging from 0.4 to 0.8 in patients treated with bivalirudin,6,11,17 and our results reflect a similar median increase of 0.4. The approach to our protocol reflects the dose-dependent, linear effects that bivalirudin demonstrates on INR values. 11 Unlike in the case of argatroban, the linearity of the INR prolongation and resulting initial change in INR (INRbivalirudin − INRprebivalirudin) caused by bivalirudin seem to be less variable between thromboplastin reagents and patients. 11 Therefore, this approach can be implemented as a useful tool to determine target INR values during the transition to warfarin. Hohlfelder et al 17 recently conducted a retrospective analysis of bivalirudin prolongation of the INR in a population largely consisting of patients with ventricular assist devices. 17 The authors concluded that the INR on discontinuation of bivalirudin was influenced by changes in renal function, higher change in INR on starting or discontinuing bivalirudin, and higher bivalirudin infusion rates prior to discharge. From their findings, they have developed a predictive mathematical model that allows one to potentially predict the “warfarin only” INR. This study also showed a 60% achievement of INR values within the therapeutic range on discontinuation of bivalirudin. Our simplistic approach to the bivalirudin-warfarin transition was associated with a higher percentage of patients (80%) achieving a therapeutic INR on cessation of bivalirudin therapy in a more diverse patient population, offering an advantage over mathematical prediction models.
The value of a standardized approach when transitioning from bivalirudin to warfarin is substantial. Our results suggest that the implemented protocol represents a safe and effective method to this transition. Interestingly, patients in the postprotocol group were observed to have a decreased length of hospital stay and total length of bivalirudin therapy, despite no difference in length of bivalirudin bridging therapy. This is likely attributed to the longer length of overall bivalirudin therapy in the preprotocol group compared with the postprotocol group as well as a shorter time to starting warfarin in the postprotocol group (approximately 1.5 days), though this was not statistically significant. An additional factor that may have contributed to a longer time to warfarin initiation, but was not assessed, is the varying degree of stability in patients, with some possibly requiring more procedures than others. Overall, implementation of a standardized transition protocol at our institution may be an effective strategy, with a promising potential to reduce therapeutic costs, improve patient safety, and achieve a therapeutic INR after the discontinuation of bivalirudin.
Several limitations existed within the study. The findings of this study represent that of a single facility along with a small patient population, which is to be expected given that our population consisted of patients with HIT. Additionally, creatinine clearance was assessed at the initiation of bivalirudin therapy but not at discontinuation. Unknown changes in renal function during this time could have affected the therapeutic effects of bivalirudin, resulting in elevated aPTT levels and supratherapeutic INR readings. Adherence to the transition protocol is also an influential factor to acknowledge because the protocol was observed to be correctly implemented in 11/20 (55%) of postprotocol patients. The protocol was not followed in a majority of patients simply because the bridge did not meet the minimum 5-day requirement. Although an adequate length of bridge therapy is necessary for active thrombosis, the paramount feature of the protocol is the creation of target INR ranges while on both agents. When evaluating the cessation of therapy in concordance with INR goals created by the protocol, adherence was increased to 17/20 (85%) of the postprotocol patients. Another limitation to address within the study relies on the fact that clinical discretion may have been used by practitioners alongside this protocol in the transition from bivalirudin to warfarin. Bivalirudin dosing at our institution requires a mandatory consult to pharmacy for initial dosing, subsequent titrations, and follow-up laboratory testing. Warfarin dosing, implementation of the transition protocol, and ordering of follow-up laboratory testing is left to the discretion of the treating clinician. This may have contributed to variability in cessation of warfarin therapy, over- or underdosing of warfarin, lack of follow-up PTT results, or decisions to omit warfarin doses for various reasons.
Conclusion
This study, which assessed the transition of bivalirudin to warfarin after implementation of a transition protocol in a real-world patient population, was associated with a significant improvement in the achievement of therapeutic INR values after the discontinuation of bivalirudin. Historically, documented guidance in the transition from bivalirudin to warfarin has been limited, if not nonexistent. Replication of this clinical study in a larger patient population should be done to corroborate the safety and efficacy of this standardized approach to transitioning patients from bivalirudin to warfarin. This task may prove difficult given the small population of patients with an indication for bivalirudin requiring a transition to warfarin therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.