
Abstract
Introduction
The American Cancer Society estimates 76 380 new cases of melanoma to be diagnosed in 2016 with about 10 130 predicted deaths. 1 It is estimated that 2% to 5% of patients with melanoma present with distant metastatic disease. The 5-year survival rates range from 20% to 70%, and 10% in stage III and stage IV melanoma, respectively. 2 The wide range of survival rates in stage III is a result of the extent of the disease, with 5-year survival rates for local, regional, and distant melanoma being 98%, 63%, and 17%, respectively. 1 Current guidelines recommend immunotherapy, either as monotherapy (pembrolizumab, nivolumab) or combination therapy (nivolumab and ipilimumab), targeted therapy if BRAF (B-Raf Proto-Oncogene, Serine/Threonine Kinase) mutation–positive, or clinical trials for the treatment of metastatic or unresectable disease. 2
Approximately one-half of the metastatic melanoma cases present with activating mutations in the BRAF. The prognosis for these patients is similar to those without BRAF mutation. 3 More than 90% of BRAF mutations are at codon 600, with a mutation at nucleotide 1799; 90% of these mutations are BRAFV600E, whereas 5% to 6% are BRAFV600K. 4
The discovery of targeted therapy for patients with a BRAF mutation has changed the landscape of melanoma treatment. Vemurafenib was the first BRAF inhibitor to be approved by the US Food and Drug Administration (FDA) in 2011 for the treatment of unresectable or metastatic melanoma with BRAFV600E mutation. 5 It is associated with a median progression-free survival (PFS) of 5 to 7 months, with a median overall survival (OS) of 16 months—7 months longer than that for the previous standard of care, dacarbazine. Dabrafenib, another BRAF inhibitor, was approved by the FDA two years later for the same indication. 6 Tumor resistance to BRAF inhibition has limited sustained benefit from these agents because reactivation of the BRAF pathway occurs in about 80% of the tumors after a median of 6 to 7 months.7-9
MAPK/extracellular signal regulated kinase (MEK) inhibitors were developed to overcome BRAF resistance by targeting downstream inhibition of the mitogen-activated protein kinase (MAPK) pathway. Trametinib was the first MEK inhibitor approved in May 2013 as a single agent or in combination with dabrafenib for the treatment of patients with unresectable or metastatic melanoma with BRAFV600E or V600K mutation. Cobimetinib (Cotellic), a second MEK inhibitor, developed by Genentech was approved by the FDA in November 2015 for the same indication as trametinib but in combination with vemurafenib, instead of dabrafenib. Cobimetinib underwent an expedited 6-month review through the FDA’s priority review program and received orphan drug designation. 10
Data Sources
A PubMed search was conducted from January 2000 to June 2016 using the search terms melanoma, MEK inhibitor, and cobimetinib. A second search was conducted to identify melanoma guidelines using the terms melanoma and National Comprehensive Cancer Network. Governmental sources were searched using the term cobimetinib, and all ongoing trials using cobimetinib in melanoma were included. All data from studies and review articles were included if they provided relevant data to the practicing clinician.
Pharmacology
Genetic changes from germline alterations in the MAPK pathway lead to a loss of cell cycle control and homeostasis. The complete inhibition of the MAPK pathway is crucial to prevention of metastatic melanoma progression. The MAPK pathway involves a signaling cascade of guanosine triphosphatase (GTPase) RAS and downstream activation of rapidly accelerated fibrosarcoma (RAF), extracellular signal-regulated kinase (MAP/ERK, including MEK1 and MEK2), and MAPK (ERK2 and ERK1) kinases. BRAF V600E, and V600K mutations lead to continuous activation of the BRAF pathway, which includes MEK1 and MEK2. This pathway transcribes for cyclin-dependent kinase inhibitor 2A (CDKN2A) locus, which encodes for tumor suppressors p16INK4A and p14ARF. Cell cycle control is maintained by p16INK4A, which inactivates retinoblastoma-associated protein (RB), and P14ARF, which degrades tumor antigen p53. The G1-S cell-cycle transition is constantly stimulated by inactivating mutations in CDKN2A, leading to a loss of these two regulators of cellular homeostasis (Figure 1). 11
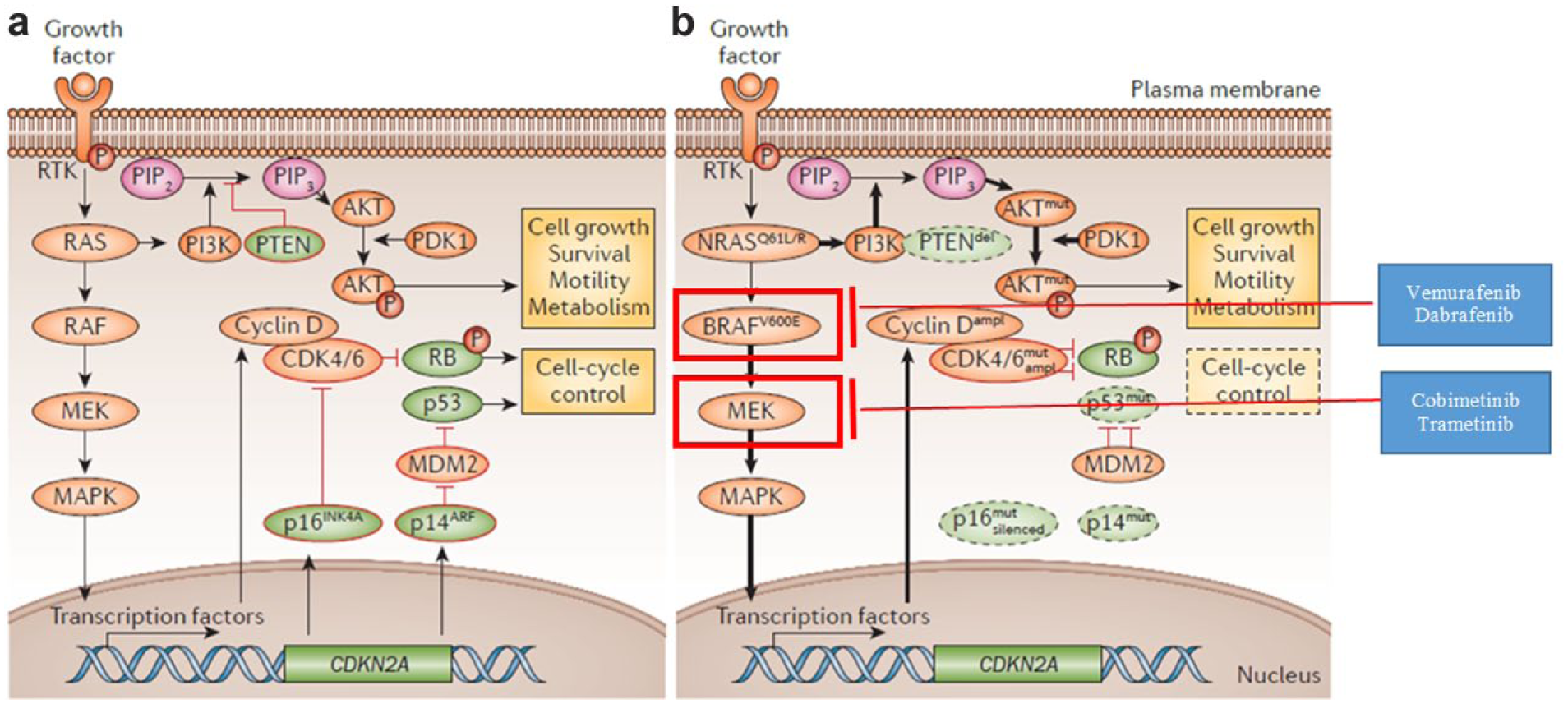
Signaling pathways in melanoma 11 : A. Under normal conditions, mitogen-activated protein kinase (MAPK) and phosphatidylinositol 3-kinase (PI3K)-AKT signaling allow balanced homeostasis, including cell-cycle regulation, survival, motility, and metabolism. B. In melanoma, the depicted genetic alterations are frequently observed, and lead to continuous pathway activation and loss of cell cycle control. Vemurafenib and dabrafenib inhibit BRAF V600E and V600K mutations to suppress the continuous activation of the MAPK pathway. Cobimetinib and trametinib inhibit MEK1 and MEK2 downstream of BRAF in the MAPK pathway. This dual inhibition leads to a longer duration of MAPK pathway inhibition.a
BRAF inhibitor therapy is limited by intrinsic and acquired resistance from the reactivation of the MAPK pathway through MEK. Cobimetinib is a reversible inhibitor of MEK1 and MEK2. It inhibited tumor cell growth in mice implanted with tumor cell lines expressing BRAF V600E. Coadministration of vemurafenib and cobimetinib resulted in increased apoptosis in vitro and reduced tumor growth in mouse implantation models of tumor cell lines harboring BRAF V600E mutations. 12
Pharmacokinetics
Following a 60-mg, once-daily oral dosing in cancer patients, average maximum concentration (Cmax), steady-state area under the curve (AUC0-24h), and time to maximum plasma concentration (Tmax) were 273 ng/mL, 4340 ng h/mL and 2.4 hours, respectively. Population pharmacokinetics showed that age, sex, and race did not have a clinically important effect on cobimetinib’s systemic exposure. Cobimetinib is 95% protein bound, independent of drug concentration. It is primarily metabolized by CYP3A4 oxidation and UGT2B7 glucuronidation and is a substrate of P-glycoprotein. 12 When coadministered with vemurafenib, the exposure of either drug is not altered because vemurafenib is metabolized by CYP3A and cobimetinib is neither an inducer nor an inhibitor of CYP3A. 13
In the dose expansion stages of the phase I study, fluorodeoxyglucose was measured by positron emission tomography (PET) scan as a pharmacodynamics marker. PET scans were performed at baseline, steady state (cycle 1, days 10-14), and trough (cycle 1, days 26-28). The 60-mg dose at steady state and trough had metabolic response rates of 47% and 31%, respectively. 14
Cobimetinib is mainly eliminated via the fecal route (76%) and partially eliminated through the renal route (17.8%). The half-life is 44 hours (range: 23-70 hours), and mean apparent clearance is 13.8 L/h. The extended half-life could potentially lead to a slower recovery of normal tissues, necessitating the 21 days on/7 days off dosing schedule. Potent CYP3A inhibitors (eg, amiodarone, itraconazole, diltiazem) can increase cobimetinib’s AUC and Cmax by 6.7-fold and 2.3-fold, respectively, whereas potent CYP3A inducers (ie, carbamazepine, efavirenz, phenytoin) can decrease cobimetinib’s exposure by 83%. Therefore, coadministration with strong CYP3A inducers should be avoided, and if cobimetinib is coadministered with strong CYP3A inhibitors, patients should be closely monitored for signs and symptoms of toxicity. 12
Efficacy
BRIM-7 was a phase Ib dose-escalation trial conducted in 129 patients with unresectable, locally advanced, or metastatic melanoma with BRAFV600 mutation and no evidence of hepatic or renal impairment. A total of 66 patients had recently progressed on vemurafenib, whereas 63 patients never received a BRAF inhibitor. All patients received vemurafenib 720 or 960 mg twice a day continuously in combination with cobimetinib 60, 80, or 100 mg once a day for 14 days on/14 days off, 21 days on/7 days off, or continuously. Vemurafenib 960 mg twice a day and cobimetinib 60 mg daily, 21 days on/7 days off, was deemed to be the safest regimen in this study. The median PFS was 2.8 months and 13.7 months in patients who had recently progressed on vemurafenib and never received a BRAF inhibitor therapy, respectively. Median OS was 8.3 months, and estimated 1-year OS was 32% in patients who had recently progressed on vemurafenib. Patients who had never received BRAF inhibitors had an estimated 1-year OS of 83%. 13
The FDA approval of cobimetinib was based on the coBRIM trial—a multicenter, randomized, phase III study to evaluate the safety and efficacy of cobimetinib in unresectable, locally advanced stage IIIC or IV melanoma with a BRAFV600 mutation. Patients of at least 18 years of age were randomized to receive vemurafenib 960 mg orally twice daily continuously in combination with placebo or cobimetinib 60 mg orally once daily (21 days on/7 days off). Patients with hepatic impairment, history of acute coronary syndrome within 6 months, evidence of class II or greater congestive heart failure, active central nervous system lesions, or evidence of retinal pathology were excluded from the study. The median age of enrolled patients was 55 years. Of the entire study population, 58% were male, 93% were Caucasians, and 60% had M1c disease. Furthermore, 10% of the total population received prior adjuvant therapy (immunotherapy: eg, ipilimumab). Samples were obtained on 81% of patients, and of these, 86% and 14% were identified as having BRAFV600E and BRAFV600K mutations, respectively. The majority of the response rates were seen by week 8, with the objective response rate being 68% in the combination group and 45% in the vemurafenib monotherapy group (complete response 10% and 4% in the combination group and monotherapy group, respectively). The median duration of response was not reached in the combination group and was 7.9 months in the control group. Median PFS was 9.9 months and 6.2 months in the combination and vemurafenib monotherapy groups, respectively (P < 0.001). Similar results were seen for all subgroup analyses (disease stage, age less than or greater than 65 years, sex, geographic region, Eastern Cooperative Oncology Group (ECOG) performance status, lactate dehydrogenase level, prior adjuvant therapy, and BRAF mutation status). Whereas the median OS was not reached in either study arm, the rate of OS at 9 months for the combination group was 81% compared with 73% in the control group (Table 1). 15
Efficacy of Cobimetinib With Vemurafenib.
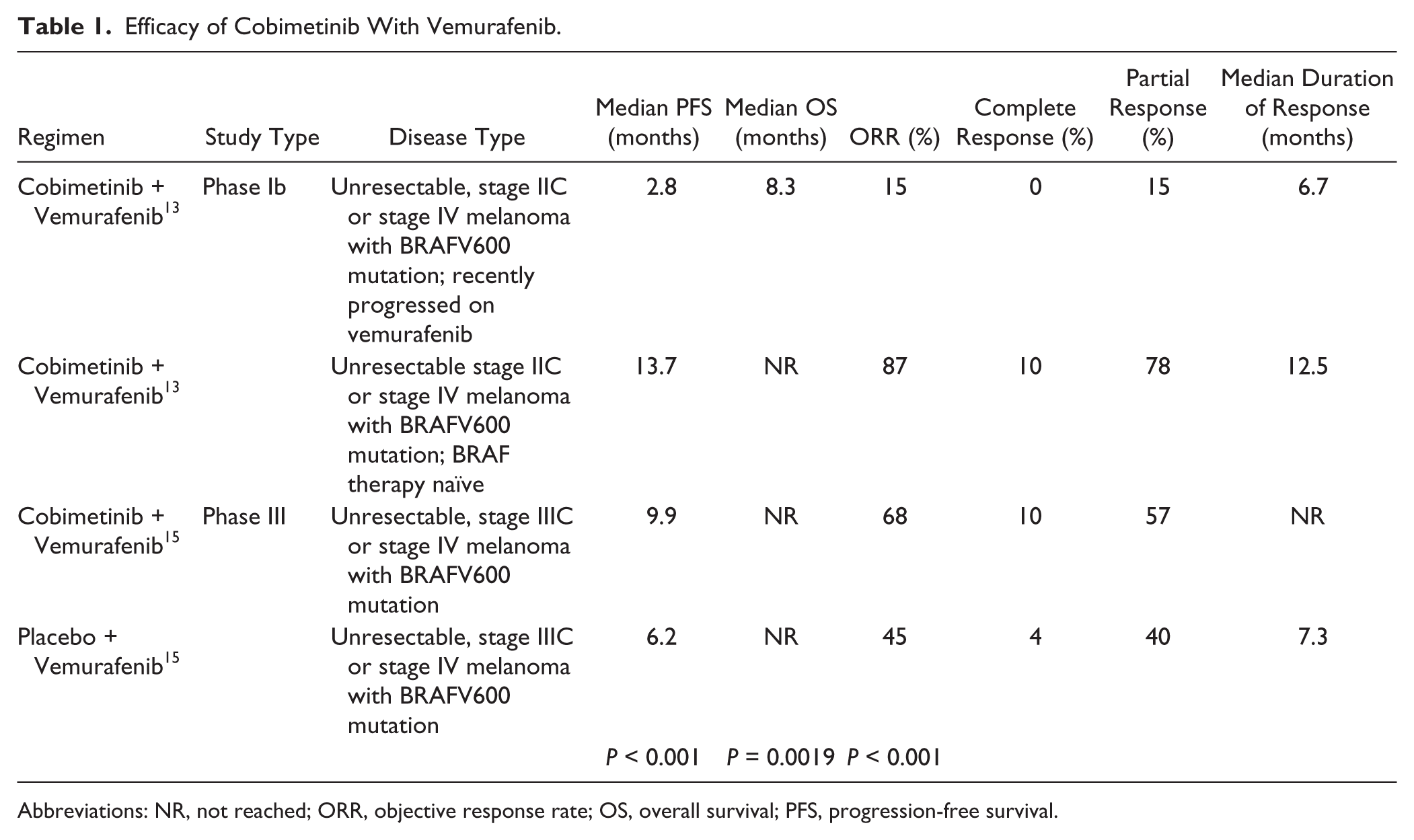
Abbreviations: NR, not reached; ORR, objective response rate; OS, overall survival; PFS, progression-free survival.
Safety
Common adverse events (AEs) in the phase Ib study in patients who had progressed on vemurafenib and patients who had never had BRAF inhibitor therapy were nonacneiform rash (33% and 87%), diarrhea (47% and 83%), fatigue (27% and 70%), photosensitivity (15% and 67%), and liver enzyme abnormalities (33% and 67%), respectively. BRAF inhibitor–naïve patients had a higher incidence of typical MEK inhibitor toxicities, including eye disorders (retinal detachment [2%], chorioretinopathy [5%], retinopathy [3%], and macular edema [2%]), diarrhea, increase in creatine phosphokinase (CPK), and acneiform rash, all of which are also seen with trametinib administration.13,16,17 The exact mechanism of these MEK inhibitor AEs remains to be investigated; however, there is some evidence to suggest that the tight junctions between epithelial cells are regulated by the MAPK pathway. MEK inhibition could impede fluid transport and result in a buildup of fluid behind the fovea, leading to some of the retinal toxicities. 18
The adverse event profile of cobimetinib in the phase III trial was similar to that in the phase Ib trial. In the phase III trial, the combination of cobimetinib and vemurafenib was associated with higher frequency of central serous retinopathy, gastrointestinal events (nausea, vomiting, or diarrhea), photosensitivity, elevated aminotransferase levels, and increased CPK level, compared with vemurafenib monotherapy. The incidence of grade 3 AEs was similar in both arms (49%); however, the incidence of grade 4 AEs was higher in the vemurafenib plus cobimetinib arm (13%) compared with the vemurafenib monotherapy arm (9%). Elevated CPK level is a known class effect of MEK inhibitors, although the majority of the elevations were grade 1 to 2 (66%). Rates of QT-interval prolongation and decreased ejection fraction were low and similar in both groups. 15 AEs in the phase Ib and III trial were assessed using the Common Terminology Criteria for Adverse Events (CTCAE) version 4. 19
The incidence of serous retinopathy was 26% in the combination arm compared with 3% in the vemurafenib monotherapy arm. The median time to onset was 1 month, and the majority of patients were asymptomatic. The majority of patients were managed with close observation without modification of therapy. There were a total of 6 and 3 deaths attributed to AEs in the combination and control groups, respectively. The rate of discontinuation of therapy as a result of AEs was similar in both groups. 15 Overall, combination therapy seems as safe as monotherapy, with a similar incidence of deaths and rates of discontinuation for AEs, although combination therapy was associated with a slightly higher incidence of grade 4 AEs.
Dosage and Administration
Cobimetinib is administered as 60 mg orally once daily for the first 21 days followed by 7 days off of each 28-day cycle until disease progression or unacceptable toxicity. It can be taken with or without food. If concurrent short-term use (14 days of less) of moderate CYP3A inhibitors is unavoidable, cobimetinib dose should be reduced to 20 mg for the duration of concurrent therapy. Although dose adjustment is not needed for CrCl ≥30 mL/min, information on its use in patients with CrCl <30 mL/min is not available, and use should be avoided in this population. Dose adjustment is not recommended in patients with mild hepatic impairment (total bilirubin ≤ upper limit of normal [ULN], AST > ULN, or total bilirubin >ULN but ≤1.5 times ULN and any AST). However, cobimetinib is associated with elevation in transaminases; hence, hepatic enzymes should be monitored at baseline and routinely. Cobimetinib should be held for the following: grade 3 hemorrhage, asymptomatic absolute decrease in left ventricular ejection fraction (LVEF) from baseline of greater than 10%, symptomatic LVEF decrease from baseline, grade 2 (intolerable) or grade 3 to 4 dermatological reactions, serous retinopathy, first occurrence of grade 4 hepatotoxicity, grade 4 CPK or any CPK elevation and myalgia, and grade 2 (intolerable) or grade 3 to 4 photosensitivity. Cobimetinib should be permanently discontinued if patients develop retinal vein occlusion, recurrent grade 4 liver enzyme abnormalities, or any recurrent grade 4 AEs. 12
Place in Therapy
The current guideline supports the use of immunotherapy, targeted therapy if BRAF mutated, or clinical trials for unresectable and metastatic melanoma (category 1). 2 First-line therapy should be patient specific and depends on several factors, including BRAF mutation status, aggression of disease, and presence or absence of cancer-related symptoms. In BRAF-positive symptomatic and aggressive disease, targeted therapy with BRAF and MEK inhibitors is preferred because it has been associated with high and quick response rates, days to weeks after starting the drug. Though caution should be exercised when making cross-trial comparisons, immunotherapy is associated with longer PFS compared with targeted therapy (11.5 months with nivolumab and ipilimumab vs 9.9 months with vemurafenib and cobimetinib).15,20 Response rates with targeted therapies are achieved earlier (8 weeks with vemurafenib and cobimetinib vs 3 months with nivolumab monotherapy or nivolumab plus ipilimumab).15,20 For the remainder of the cases (asymptomatic, nonaggressive BRAF-positive disease and BRAF wild type), frontline therapy with immune checkpoint inhibitors (pembrolizumab or nivolumab monotherapy or a combination of nivolumab and ipilimumab) is recommended.2,21
Dabrafenib and trametinib were the first targeted therapy combination to be approved for unresectable or metastatic melanoma with BRAF-positive mutation. Inclusion criteria were similar in both targeted therapy combination trials, with the exception that patients with brain metastasis in the dabrafenib and trametinib study had to have stable disease for 12 weeks compared with 3 weeks in the novel combination trial. Baseline characteristics were fairly similar between the studies; however, there were more patients with unresectable stage IIIc disease in the dabrafenib/trametinib trial (33%) compared with the vemurafenib/cobimetinib trial (9%). Although formal comparison across studies cannot be made, the median PFS between both BRAF/MEK inhibition combinations was similar (11.4 months for dabrafenib/trametinib vs 12.3 months for vemurafenib/cobimetinib).15,17 A recently published trial indirectly comparing both targeted therapy combinations did not show a significant difference in terms of PFS or objective response rate. This trial used indirect treatment comparisons of the two randomized control trials to evaluate the relative treatment effect by adjusting results of the direct comparison to preserve the strength of the randomized trials. 22
Both combinations are associated with a similar incidence of new primary cutaneous malignancies, hemorrhage, cardiomyopathy, and dermatological reactions.15,17 Dabrafenib plus trametinib is also associated with a risk of venous thromboembolism (VTE), interstitial lung disease, serious febrile reactions, and hyperglycemia; hence, vemurafenib and cobimetinib might be a better alternative for patients with underlying pulmonary disease or diabetes, or those with multiple risk factors for VTE, although more studies are warranted to better define specific patient populations where cobimetinib plus vemurafenib is preferred over dabrafenib plus trametinib. Vemurafenib plus cobimetinib can cause hepatotoxicity and severe photosensitivity, so dabrafenib/tramatenib may be better suited for patients with baseline hepatic dysfunction and those with underlying ocular disorders (<1% incidence with dabrafenib/trametinib).
Frequency of administration is similar for both targeted therapy combinations; however, cobimetinib/vemurafenib is a more complex regimen (cobimetinib dosing of 21 days on/7 days off) and has a higher pill burden. Both combinations are currently considered first-line therapy for unresectable or metastatic melanoma with a BRAF V600E or V600K mutation. 2 Until head-to-head comparisons become available, the choice between the two different BRAF/MEK inhibitor combinations should be based on patient characteristics, convenience, and adverse event profile (Table 2).
Adverse Events (All Grades) From Phase III Trials of Combination Therapies. a
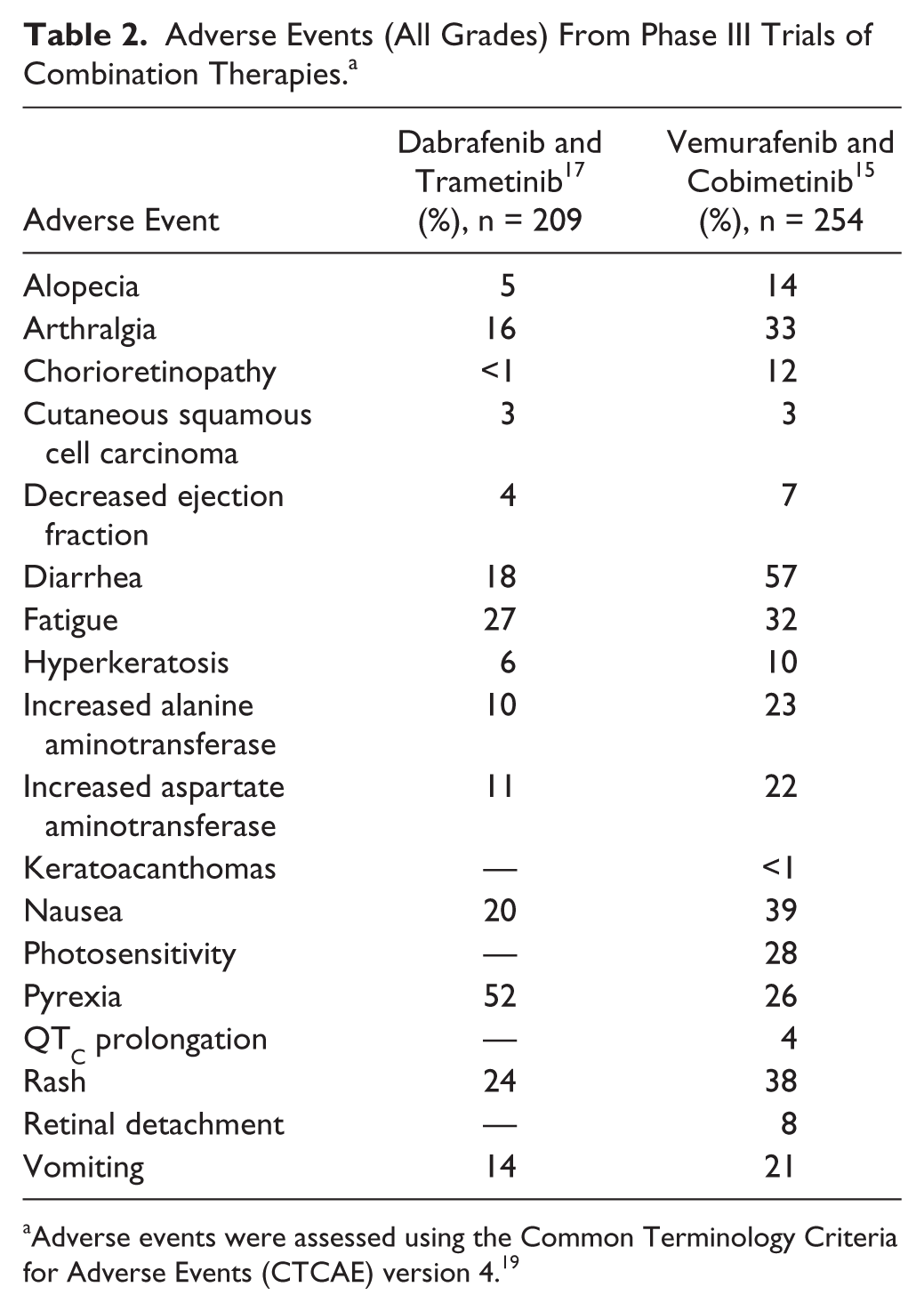
Adverse events were assessed using the Common Terminology Criteria for Adverse Events (CTCAE) version 4. 19
Financial Implications
The current average wholesale price (AWP) for a 21-day supply of cobimetinib is $7274.11 and for a 28-day supply of vemurafenib is $12 152.90. Hence, the total cost per cycle for this combination therapy would be $19 427. The AWP for 1 cycle of dabrafenib/trametinib would be $23 571.10. Even though the latter combination would result in higher costs to the health care system, the exact cost incurred by each patient would vary significantly depending on insurance coverage. 23
Future Directions
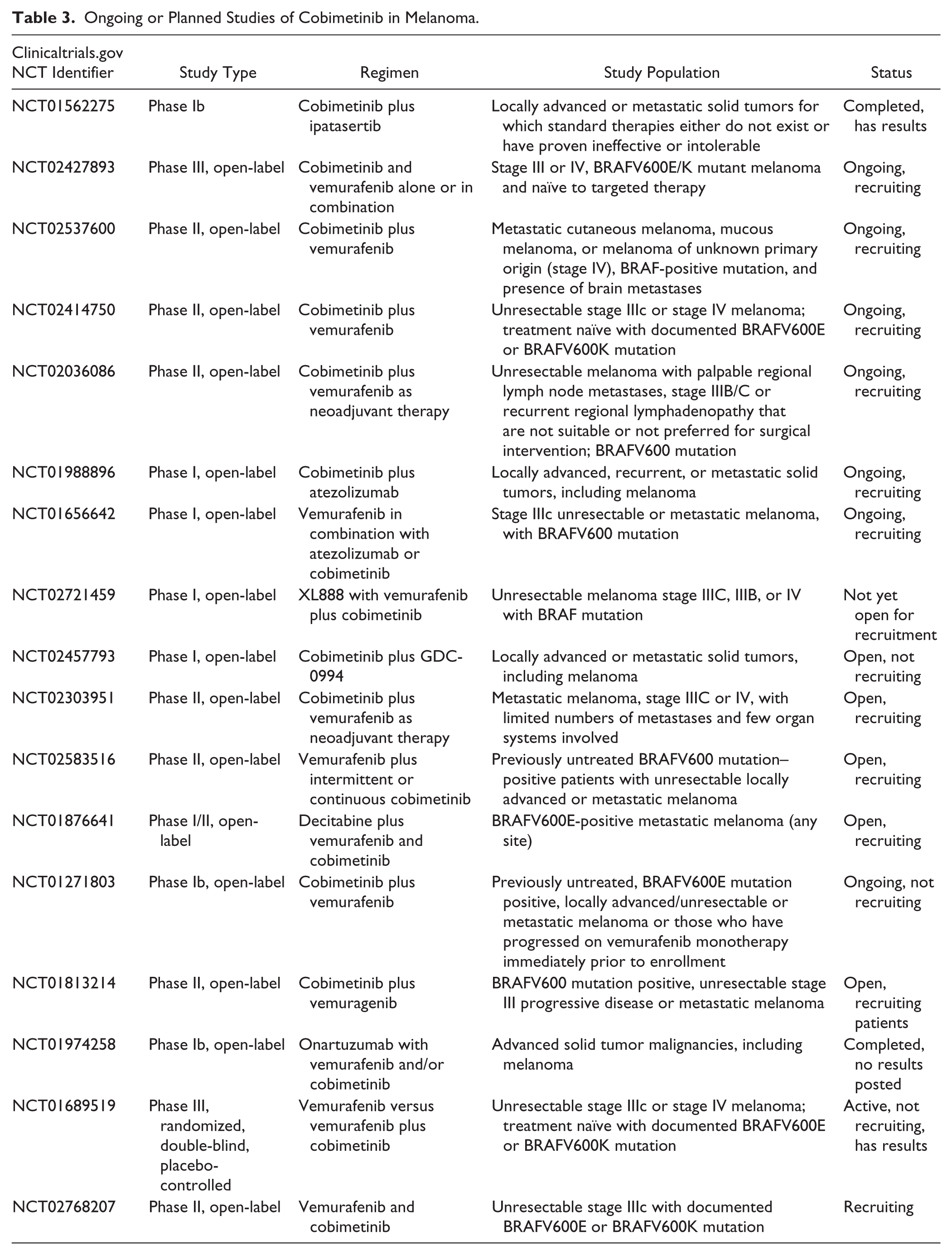
Despite improved response rates with the combination of MEK and BRAF inhibitors, resistance eventually occurs in 58% of the patients after 6 to 7 months.24,25 Several clinical trials are currently investigating the role of cobimetinib either as monotherapy or in combination with vemurafenib, as well as various targeted therapies in specific stages of melanoma (stage IIIB or C with palpable lymph nodes, unresectable stage IIIC, and stage IV with presence of brain metastases), or as neoadjuvant therapy (Table 3). Combination therapy of cobimetinib with several new agents is currently under investigation, including ipatasertib, an Akt inhibitor (ClinicalTrials.gov identifier NCT01562275); atezolizumab, a PD-1 inhibitor (ClinicalTrials.gov identifier NCT01988896); and GDC-0094, an ERK inhibitor (ClinicalTrials.gov identifier NCT02457793). Triple therapy combination of vemurafenib and cobimetinib with a Heat Shock Protein 90 (HSP90) therapy is currently recruiting patients (ClinicalTrials.gov identifier NCT02721459). Either cobimetinib monotherapy or its combination with vemurafenib is also being investigated as frontline therapy in treatment-naïve patients with stage III or IV melanoma with BRAFV600E/K mutation (ClinicalTrials.gov identifiers NCT02583516, NCT02427893, NCT02414750, and NCT01689519). In addition, the role of cobimetinib plus vemurafenib after progression on vemurafenib is also under investigation (ClinicalTrials.gov identifier NCT01271803).
Ongoing or Planned Studies of Cobimetinib in Melanoma.
There are currently no phase III trials comparing dabrafenib/trametinib with cobimetinib/vemurafenib. Until such studies are conducted, both combination therapies remain the preferred frontline therapy for the treatment of patients with unresectable or metastatic melanoma with BRAFV600E or V600K mutation. As more data from various ongoing studies become available, clinicians will be better equipped to determine whether immunotherapy, targeted therapies, or combinations of both should be the preferred frontline therapy. Future research should focus on identifying the optimum combination or sequence of therapy with other targeting therapies or immunotherapy. The combination of kinase inhibitors and immunotherapy has shown higher-than-expected toxicities in various studies; hence, cautious and prudent evaluation of these therapies will be critical in the future.26-28
Summary
The development of MEK inhibition with cobimetinib in combination with vemurafenib is an important addition to the armamentarium for managing unresectable or metastatic melanoma with BRAF V600E or V600K mutation, a disease with limited availability of treatment options and poor prognosis. It should be considered a frontline therapy for patients with aggressive and symptomatic disease. Cobimetinib is also being investigated with other targeted therapies and immunotherapy for a variety of solid tumors, including metastatic colorectal cancer and non–small-cell lung cancer. As results from various ongoing studies become available, the role of cobimetinib will likely expand.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.