
Abstract
Introduction
Delaying Alzheimer’s disease (AD) would have a major public health impact.1,2 To date, pharmacological treatments for AD have shown mild to modest benefits, limited in time, on symptoms of dementia and associated functional decline. They have no effect on the progression of the disease. The onset of AD is typically preceded by a phase of progressive cognitive decline. There is evidence that individuals showing mild cognitive impairment (MCI) or cognitive impairment without meeting dementia criteria (cognitive impairment, not dementia [CIND]) are more likely to progress to AD. 3 CIND encompasses different subtypes of cognitive impairment, including those of psychiatric origin, or vascular and other specific neurological disorders. Accordingly, this preclinical phase or even earlier stages would be a logical target for early intervention against AD. 4 No medication is yet recommended either for the prevention of AD or cognitive decline.
Many studies reported an association between antioxidant nutrients, such as vitamins E and C,5-7 carotenoids including β-carotene,5,8 and flavonoids,5,9 and a lower risk of cognitive decline or AD, but few studies have investigated this association in relation to vitamin supplements. Observational studies found that the use of vitamin E and C supplements was inversely associated with subsequent risk of cognitive decline or AD10-12 but not consistently.13,14 One randomized trial found a slower progression of AD after 2 years of vitamin E treatment, 15 whereas another found no improvement in individuals with amnestic MCI after 3 years of vitamin E treatment. 16 Depending on the length of follow-up, the protective associations for AD and cognitive decline were not completely reproduced within some studies.10,11,13 A previous analysis from the Canadian Study of Health and Aging (CSHA) reported a decreased risk of cognitive decline and vascular cognitive impairment with supplemental use of antioxidant vitamins but no association for all-cause dementia or AD after a 5-year follow-up. 17 The aim of the current study was to assess the associations of the use of vitamin E and C supplements with incident cases of all-cause dementia, AD, and CIND at up to 10 years of follow-up.
Methods
The CSHA is a national, longitudinal, multicentric cohort study on dementia; field work was done in 18 centers across Canada during 3 phases, at 5-yearly intervals. 18 All phases were approved by the ethics review committees in the coordinating center and in each participating study center. In brief, representative samples of people ≥65 years old were drawn in 1991-1992 from 36 communities and surrounding rural areas. Of the 10 263 participants involved at CSHA baseline (CSHA-1), 9008 were living in the community and 1255 in institutions. Participants for the community sample were randomly selected from Medicare lists or the Enumeration Composite Records in Ontario. Institutionalized participants were randomly selected from residents in stratified random samples of institutions in each region. Community-dwelling participants were interviewed about sociodemographic information and current health problems, after which they were screened for dementia using the 100-point Modified Mini-Mental State (3MS) Examination. 19 Participants screening positive (3MS score < 78), a random sample of those who were screened negative, and all participants living in institutions were asked to attend an extensive clinical evaluation. First, a nurse readministered the 3MS and collected information on the participant’s medical and family history. Next, a physician reviewed the information collected by the nurse and conducted a standardized physical and neurological examination. Finally, those with a 3MS score of ≥50 were administered a battery of neuropsychological tests by a psychometrist, the results of which were interpreted by a neuropsychologist. Preliminary diagnoses were made independently by the physician and the neuropsychologist; final diagnosis was reached after a consensus conference.
Dementia Assessment
The diagnosis of all-cause dementia was made according to the revised third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R). 20 For AD, the criteria of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) were used. 21 DSM-III-R and the International Classification of Diseases, tenth revision criteria 22 served to make a diagnosis of CIND. Finally, participants screening negative or diagnosed cognitively normal were asked to complete at home and return by mail a self-administered risk factor questionnaire (RFQ) that covered variables related to lifestyle, including smoking and alcohol as well as a medical and family history (including antioxidant and medication use). Of the 10 263 participants enrolled in CSHA-1, 1132 participants were diagnosed with prevalent dementia, 508 screened positive but declined clinical examination, and 857 did not complete the RFQ, leaving 7766 eligible participants for the purpose of the current prospective analysis.
Two follow-up evaluations were undertaken in 1996-1997 (CSHA-2), and 2001-2002 (CSHA-3). The same diagnostic process as in CSHA-1 was used. 18 Two diagnoses for each participant were made, one according to the criteria used in CSHA-1 and the other following new criteria from the fourth edition of the DSM for all-cause dementia and AD. The 3MS cut-point at CSHA-3 was set at 89/90 for a better screening of participants with cognitive impairment. Participants screening positive were invited to complete neuropsychological tests, the results of which determined participants proceeding to a clinical examination. DSM-IV criteria were used to define incident cases of dementia in AD at CSHA-2 and CSHA-3.
Vitamin Exposure
Exposure to supplements of vitamin E or C was measured at baseline using data collected either from the structured interview at the clinical examination or the self-administered RFQ. During the clinical examination, participants were asked by the nurse to list current medications (with or without prescriptions). In the RFQ, participants were asked to list medications they were currently taking for specific conditions they suffered from, to fill the name of medications on pill bottles or containers, and to include both prescription and nonprescription types, vitamins, minerals, and laxatives. No information on the dose was requested. Medications were coded using the Anatomical Therapeutic Chemical (ATC) classification. Vitamins C and E were defined using codes A11GA01 (ascorbic acid [vitamin C], plain) and A11HA03 (tocopherol [vitamin E]). Multivitamin use was defined using code A11A (multivitamins, combinations), which corresponds to products containing minimum vitamins A, B, C, and D.
Covariates
Covariates were measured at baseline using either the RFQ or the clinical examination. Smoking status was categorized as nonsmoker or ever regular smoker (cigarette, cigar, or pipe). Alcohol intake was coded as no alcohol or any regular alcohol intake (at least 1 drink per week of beer, wine, or spirits, past or current). Regular practice of physical activity was categorized as none, low, moderate, and high based on the frequency and the intensity of the activity. 23 Medical history encompassed the use of nonsteroidal anti-inflammatory drugs as previously defined (NSAIDs: yes/no), 24 history of diabetes mellitus (yes/no), and vascular risk factors (yes/no). This latter variable included at least 1 of the following conditions: history of high blood pressure or use of antihypertensive drug, cardiovascular disease, cardiac symptoms, use of hypolipemic agent, or stroke. Education (years) was treated as a continuous variable.
Statistical Analyses
Baseline characteristics were compared using Student’s t test for continuous variables and χ2 test for categorical variables. Data from the RFQ and the clinical examination were combined to create a set of 3 exposure groups (vitamins E and/or C, vitamin E only, and vitamin C only). Cox proportional hazard regression models were used to evaluate the association between use of supplements and the incidence of all-cause dementia and AD in a first data set. This data set included participants diagnosed at baseline with no cognitive impairment or CIND and those who screened negative The association with the incidence of CIND was evaluated in a second data set excluding CIND participants at baseline and participants developing all-cause dementia without being diagnosed with CIND during follow-up. Age of onset of the event was defined as the midpoint of the interval between prior examination without outcomes (all-cause dementia, AD, or CIND) and the first follow-up with outcomes. Follow-up time was censored at age of onset or at the last follow-up completed. The proportionality assumption was tested by a Kolmogorov-type supremum test based on the cumulative sums of Martingale residuals. 25 Associations were measured with the hazard ratio in 3 different models. The first model was adjusted for age, defined as the time scale. The second model was additionally adjusted for sex and education, and the third model was additionally adjusted for alcohol and tobacco, physical activity, use of NSAIDs, history of diabetes mellitus, and cardiovascular factors. Dummy variables were created for missing values of covariates. The potential modification of the association between use of vitamin supplements and incidence of diseases by NSAIDs was verified within Cox regression basic models by using interaction terms. Analyses were performed using the SAS software, version 9.2.
Results
Among the 7766 eligible people, 2497 could not be included because they died before CSHA-2 (n = 1702, 22%) or refused or could not be reached (n = 795, 10%), leaving a sample of 5269 participants. Compared with participants not remaining in the final analysis (n = 2497), participants studied were significantly younger, comprised proportionally more women, and were more educated. In the first study sample (n = 5269), 821 incident cases of all-cause dementia, including 560 cases of AD, were diagnosed. In the second study sample (n = 4364), which excluded 358 prevalent cases of CIND and 547 incident cases of dementia without a previous diagnosis of CIND, 882 participants developed CIND during follow-up.
Approximately 10% (n = 524) of participants reported taking vitamin E or C supplements, the majority taking either vitamin supplement alone. The mean follow-up time was 5.2 ± 1.7 years (range = 1.8-11.4 years). Because most participants screening negative in CSHA-1 were not invited to the clinical examination, the main source of information on exposure was the RFQ. For participants with information collected from both the clinical examination and the RFQ (n = 482), the κ coefficient between the 2 sources of information was estimated at 0.38 for vitamin C, 0.51 for vitamin E, and 0.40 for any vitamins.
Table 1 summarizes baseline characteristics of the 2 study samples. In the first study sample, incident cases of all-cause dementia and AD were significantly older, less educated, and more likely to be female than participants without dementia. They reported significantly less frequent use of tobacco, were less likely to be regular alcohol drinkers, were physically active, and were using fewer NSAIDs. No difference between groups for history of diabetes mellitus and vascular risk factors was observed. Compared with participants without dementia, those who developed all-cause dementia reported taking significantly fewer supplements of vitamin E or C, vitamin E only, or vitamin C only; similar results were observed for incident cases of AD. In the second study sample, incident cases of CIND were significantly older and less educated than participants without dementia. They were less likely to be ever regular smokers, more likely to be diabetics and less physically active, and were using fewer NSAIDs. No difference between groups was observed for sex, alcohol intake, and vascular risk factors. Incident cases of CIND reported using significantly fewer supplements of vitamin E or C, vitamin E only, and vitamin C only than participants without dementia.
Baseline Characteristics of Participants Without Dementia and Incident Cases of All-Cause Dementia, AD, or CIND in the 2 Study Samples.
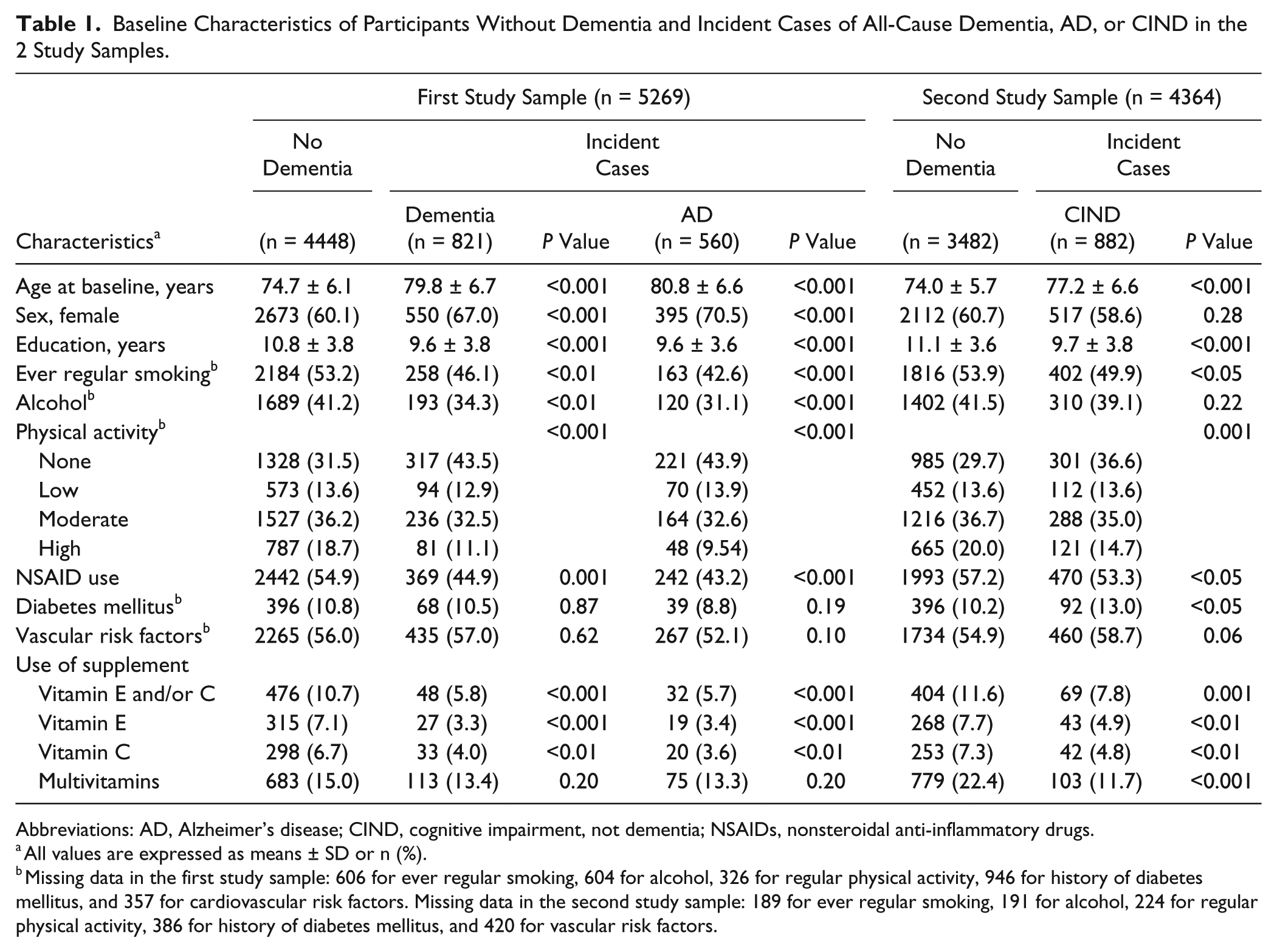
Abbreviations: AD, Alzheimer’s disease; CIND, cognitive impairment, not dementia; NSAIDs, nonsteroidal anti-inflammatory drugs.
All values are expressed as means ± SD or n (%).
Missing data in the first study sample: 606 for ever regular smoking, 604 for alcohol, 326 for regular physical activity, 946 for history of diabetes mellitus, and 357 for cardiovascular risk factors. Missing data in the second study sample: 189 for ever regular smoking, 191 for alcohol, 224 for regular physical activity, 386 for history of diabetes mellitus, and 420 for vascular risk factors.
Compared with the reference group (no use of vitamin E or C), the use of vitamin E and/or C supplements was significantly associated with 40% and 42% reduced risks of all cause-dementia and AD, respectively (Table 2). The use of either vitamin was significantly associated with 47% and 36% decreased risks of all-cause dementia and with 46% and 43% decreased risks of AD for vitamins E and C, respectively. All results remained significant when additional adjustment was made for sex and education (model 2) and other potential confounders (model 3).
HRs for the Association Between Vitamin E and C Supplements and the Incidence of All-Cause Dementia and AD.
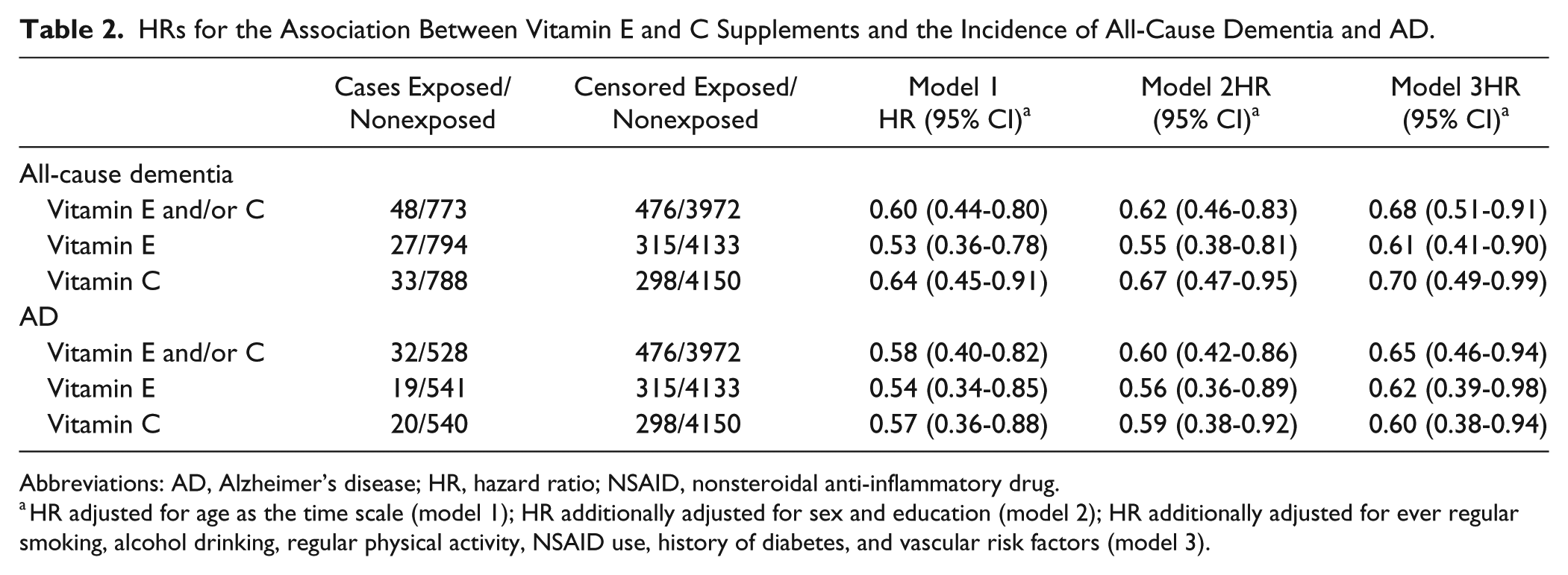
Abbreviations: AD, Alzheimer’s disease; HR, hazard ratio; NSAID, nonsteroidal anti-inflammatory drug.
HR adjusted for age as the time scale (model 1); HR additionally adjusted for sex and education (model 2); HR additionally adjusted for ever regular smoking, alcohol drinking, regular physical activity, NSAID use, history of diabetes, and vascular risk factors (model 3).
The risk of CIND was significantly decreased by 30% with the use of supplements of vitamin E and/or C compared with the reference group (model 1; Table 3). Intakes of either vitamin were similarly associated with a 32% and 31% reduced risk of CIND for vitamins E and C, respectively. After additional adjustment for sex and education, reduced risk of CIND remained significant in the group of any vitamin and vitamin E only. In all fully adjusted models, the risk of CIND was not associated with any category of vitamins.
HRs for the Association Between Vitamin E and C Supplements and the Incidence of CIND.
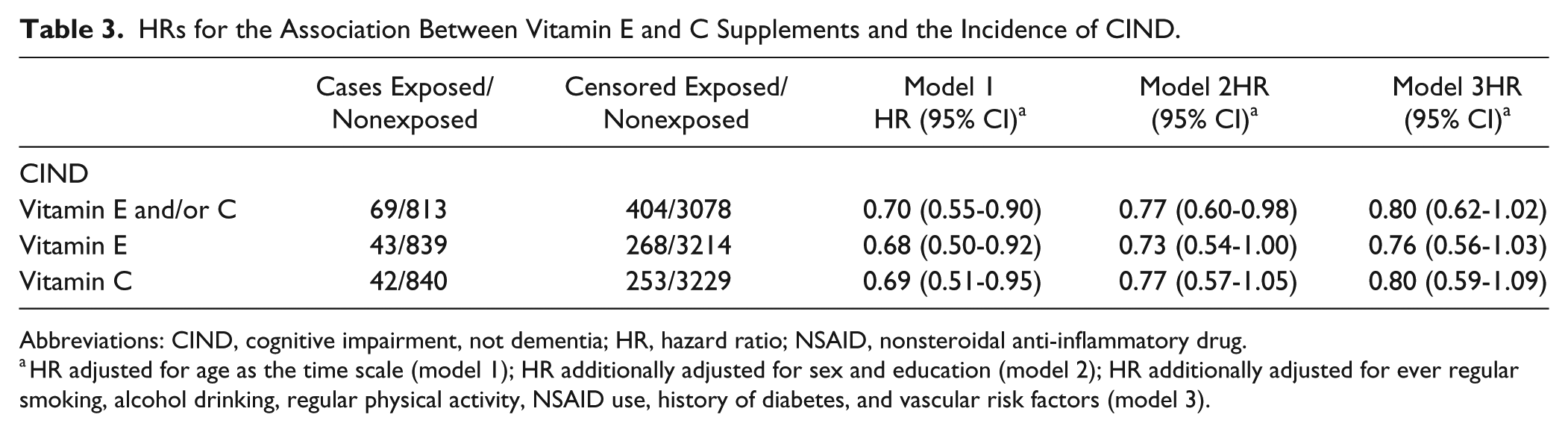
Abbreviations: CIND, cognitive impairment, not dementia; HR, hazard ratio; NSAID, nonsteroidal anti-inflammatory drug.
HR adjusted for age as the time scale (model 1); HR additionally adjusted for sex and education (model 2); HR additionally adjusted for ever regular smoking, alcohol drinking, regular physical activity, NSAID use, history of diabetes, and vascular risk factors (model 3).
Sensitivity analyses were performed including multivitamins in the exposure to vitamins E and/or C and vitamin C only. For dementia and AD, consideration of multivitamins resulted in slightly less protective associations and the loss of significance for most associations (Table 4). In contrast, consideration of multivitamins for CIND showed similar and statistically significant protective associations in all models. Other sensitivity analyses were performed to explore the possibility of misclassification of the exposure considering data source (clinical evaluation, which was a structured interview; n = 747 and 399 for dementia and CIND, respectively) versus the RFQ, which was self-administered (n = 3688 and 3407 for dementia and CIND, respectively). Although CIs were wider because of the reduction in sample size, all estimates of associations for either the clinical evaluation or the RFQ remained within 5%, on average, of those observed in Table 4 (data not shown). There was no global effect modification of NSAIDs or smoking on the relation between vitamins and all-cause dementia, AD, or CIND (data not shown).
HRs for the Association Between Vitamin E and C Supplements, Including Multivitamin Use and the Incidence of Dementia and CIND.
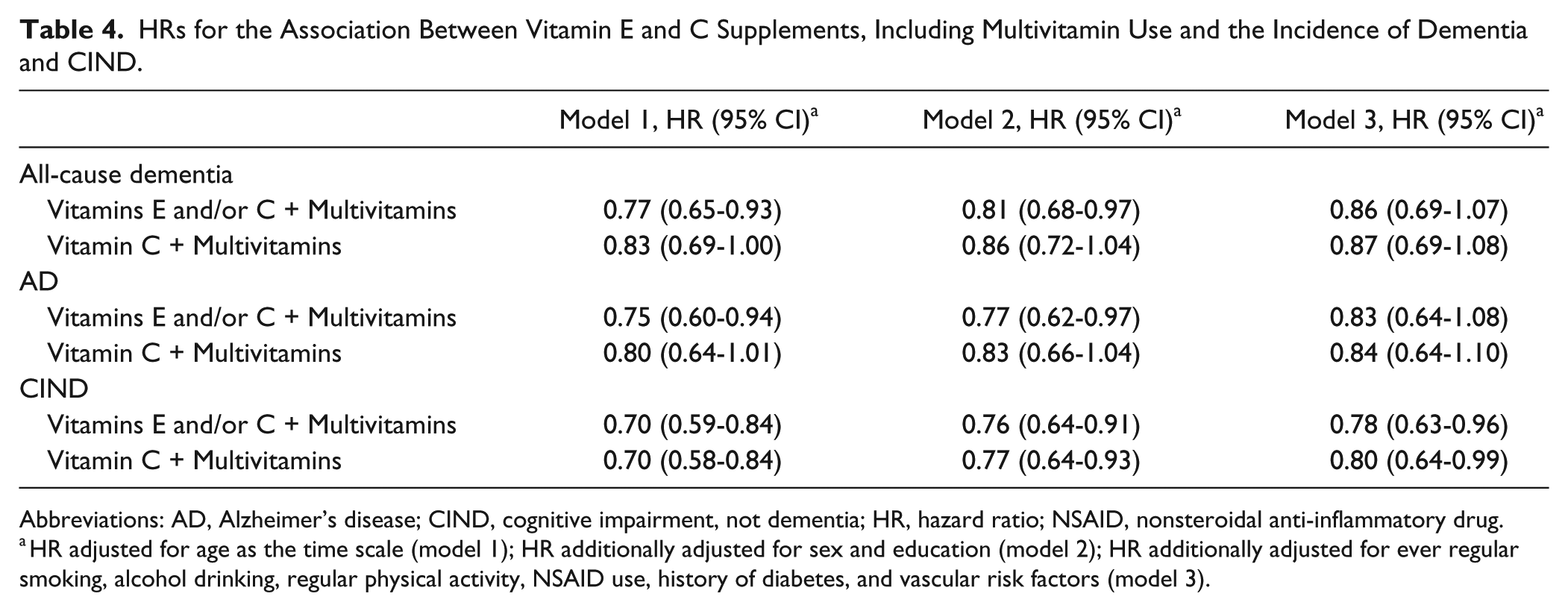
Abbreviations: AD, Alzheimer’s disease; CIND, cognitive impairment, not dementia; HR, hazard ratio; NSAID, nonsteroidal anti-inflammatory drug.
HR adjusted for age as the time scale (model 1); HR additionally adjusted for sex and education (model 2); HR additionally adjusted for ever regular smoking, alcohol drinking, regular physical activity, NSAID use, history of diabetes, and vascular risk factors (model 3).
Discussion
In this study, we found that the use of vitamin E and C supplements was associated with decreased risks of all-cause dementia and AD. These associations remained significant after adjustment for potential confounders such as demographics, lifestyle variables, NSAID use, and comorbidities. We also found that the use of vitamin E and C supplements was modestly associated with a lower risk of CIND. In contrast, sensitivity analyses suggested that when exposure to multivitamins was considered in the definition of the combined exposure (vitamin E and/or C) and vitamin C only, these exposures were rather protective in CIND when compared with all-cause dementia and AD, no matter what the data source. These results are based on a large representative sample of older people followed for up to 11 years (mean of 5 years). The strengths of CSHA include the random selection of participants, high response rates at the 3 phases, and careful standardization of screening and clinical assessments. 18
Our results are generally consistent with earlier reports from population-based studies,10,11,17,26 but not all,14,27,28 that provided much of the evidence for a protective effect of both vitamin E and C supplements against AD and cognitive decline. In contrast to other studies, vitamin supplement use taken alone was also associated with reduced risks. These results extend the previous findings on AD by suggesting a protective association at an earlier phase of the disease process, with the reduction of risk for CIND. In the Cache County study, significant reduction of AD risk was observed with concurrent use of vitamins but not distinct use of either one. 11 In a cohort of older community-dwelling women from the Nurses’ Health Study, the global score of the cognitive tests was significantly higher among those who had taken supplements of vitamin E and C for ≥10 years than among those who had never taken vitamins. 10 There was a significant dose-response up to longer duration (P for trend = 0.04, with categories of <5, 5-9, and ≥10 years). For women using vitamin E only, little evidence of benefits with increased duration of use was found. This association was also reported in another population-based study. 12 This investigation further reported an improved cognitive performance in participants taking vitamin E and C supplements combined with NSAIDs than in those taking vitamins alone; this association was significant only among participants carrying the apolipoprotein E ϵ4 allele.
The biological plausibility of a beneficial effect of antioxidant vitamins on cognitive function has been supported by the endogenous capacity of these compounds to reduce neuronal damage and death caused by oxidative stress, which contributes to the pathogenesis of dementia. 29 Some research showed that pathological AD changes are already well established in the brain in a substantial fraction of people diagnosed with cognitive impairment. 30 In addition, low blood levels of vitamins E and C are associated with a memory deficit in older dementia-free persons.31,32 Two clinical trials of supplementation of vitamin E in AD participants reported beneficial effects,15,33 although not related to cognition. The Alzheimer’s Disease Cooperative Study on 341 patients with moderate AD found that vitamin E, as well as its combination with selegiline, delayed progression to institutionalization compared with placebo. 15 The TEAM-AD VA cooperative randomized trial on 613 participants (97% male, 50% apoE4 carriers) under treatment with acetylcholinesterase inhibitors showed that vitamin E resulted in slower functional decline and decreased caregiver burden compared with placebo. No effect was observed with memantine or its combination with vitamin E. 33 In another clinical trial of 769 amnestic MCI patients, no difference between use of vitamin E and placebo was seen on the progression toward AD over 3 years. 16
Several limitations of our study deserve mention. Of the eligible participants, approximately a third of the sample was lost to follow-up because they died (22%) before the first 5-year follow-up, refused, or were not able to be reached; a selection bias is, therefore, possible. Because the 3MS is a screening test for dementia and not CIND, participants with CIND at CSHA-1 and CSHA-2, when the cut-point was set lower, might have been missed. Indeed, participants screening negative might have been classified cognitively normal despite the presence of cognitive impairment or dementia because they were not clinically assessed. The cut-point was set at 89/90 at the second follow-up for a better screening of cognitively impaired participants. Additionally, CIND is a heterogeneous syndrome, making no distinction between various etiologies of cognitive impairment. It is, thus, possible that antioxidant vitamins offer protection just for some subtypes of cognitive impairment. The lack of information about duration of use of the supplement, consistency of and adherence to use, and dosing is a major limitation. The use of multivitamins included other vitamins as well as vitamin C. It is, therefore, difficult to know whether the associations reflect those related to vitamin C or to other vitamins. The information on vitamin E included in multivitamins was not available. Information on supplement use was mostly self-reported, with no validation. Recall bias cannot be excluded, although the information was collected before the onset of the disease. This nondifferential misclassification of exposure biases toward the null. In addition, vitamin exposure was ascertained only once. It is possible that it does not reflect long-term practices, which are more likely to influence disease risk. The RFQ was completed at home by participants in contrast to the clinical examination, which was administered by a nurse. In some participants, information was available from both the clinical examination and the RFQ. Correlation analyses were performed, and slight agreements were found between the 2 sources of exposure. Low values of κ may in part be explained by methodological issues. Clinical evaluations were mostly done at a clinic where the nurse collected the information on medication, whereas the RFQ was to be completed at home with vitamin supplements at hand. Accordingly, based on a subsample of participants with both data sources, the use of vitamin supplements was declared more frequently in the RFQ than in the clinical evaluation. More than 90% of the available information in this study comes from the RFQ. Finally, we cannot exclude the potential for unmeasured confounders (eg, dietary intake of vitamins, the presence of apolipoprotein E ϵ4 allele, vitamin D concentrations/bone mineral density, socioeconomic status) and residual confounding despite adjustment for several covariates.
Conclusions
This study supports a protective role of vitamin E and C supplements in the risk for AD and all-cause dementia. In addition, these supplements may contribute to a reduced risk of CIND. Overall, these findings indicate additional support for the use of antioxidants as a preventive strategy against cognitive decline. Supplements of vitamins C and E are generally safe, inexpensive, and may provide a number of health benefits, although hemorrhagic effects have been related to vitamin E supplements. 34 Moreover, vitamin C and E supplements are known to interact with several types of medications, 34 which may put elderly people at risk. Given that information about supplement duration of use, consistency of and adherence to use, and dosing were major limitations in our study, further research is warranted before suggestion in the clinical practice in order to determine the appropriate dose, form, dose response, and target population. Moreover, it would be interesting to examine potential interactions between vitamins, other components of diet, and various modulators of disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The core funding for phases 1 and 2 of the Canadian Study of Health and Aging was provided by the Seniors’ Independence Research Program through the Health Canada’s National Health Research and Development Program (NHRDP). Other funding was provided by Pfizer Canada Incorporated, Bayer Incorporated, and the British Columbia Health Research Foundation. The core funding for phase 3 was provided by the Canadian Institutes of Health Research (CIHR). Other funding was provided by Merck-Frosst and Janssen-Ortho. LLB was supported by the Fonds d’enseignement et de recherche, Faculty of Pharmacy, Laval University. DL was supported by a scientist award from the Fonds de recherche du Québec—Santé (FRQS).