
Abstract
Keywords
Introduction
Inducement programs offer cash, coupons, discounts, gifts, or points as incentives to promote a desired action. In the retail industry, inducement programs are commonly used as a marketing tool to cultivate consumer loyalty. As community pharmacies operate in a retail environment, many organizations have incorporated inducement programs into their marketing strategy. In the United States, pharmacy chains like Walgreens have offered savings on prescriptions. 1 In Canada, several pharmacy chains have inducement programs that award points for the purchase of over-the-counter products and storefront items such as health and beauty aids. Some community pharmacy–based inducement programs also include prescriptions as eligible purchases. This inclusion is based, in part, on evidence that financial incentives help shape desired health behaviors.2-4
On closer examination, however, this evidence may not be directly applicable to pharmacy-based inducement programs.2-4 Two of the systematic reviews focused on studies examining the effect of cash incentives on keeping medical appointments, maintaining smoking cessation, maintaining abstinence from substance abuse, or maintaining weight loss.2,4 None of the health behaviors studied would be considered relevant to community pharmacy loyalty or medication adherence. Although one systematic review examined the effect of cash or free medication incentives on medication adherence, the majority of the 19 studies included in this review were conducted in specialty populations. 3 For example, 6 studies examined naltrexone use for opioid dependence, 5 studies examined isoniazid use for latent tuberculosis, and 2 studies examined disulfiram use for alcohol dependence. 3 It is unclear if observations from studies of specialty populations are generalizable to patients with diabetes or cardiovascular disease, who are required to take chronic medications.
Some stakeholders have suggested that inducement programs can have a negative effect in community pharmacy,5,6 whereas others have voiced concerns about the lack of empirical evidence to directly link pharmacy-based inducement programs with patient outcomes.7-9 A comprehensive literature search of MEDLINE and EMBASE identified only 1 conference abstract evaluating the association between a community pharmacy–based inducement program and medication adherence. 1 Staskon et al 1 found that customers enrolled in an incentive program offering discounts on prescriptions, health care products, and services had a mean medication possession ratio (MPR) of 0.78 for antidiabetic medications. In contrast, customers who were not enrolled in this program had a mean MPR of 0.68 (P < 0.001). Although the observed association with adherence is encouraging, long-term clinical outcomes, such as development of end-organ damage, hospitalization, or mortality, should also be used to assess the safety and effectiveness of community pharmacy–based inducement programs.
Statins are commonly used as the medication class of interest in adherence studies because they are widely available, commonly used, and once started, should be used chronically to reduce the risk of an acute coronary syndrome (ACS) event or death.10-12 Importantly, the link between good adherence to statins and risk of cardiovascular morbidity and mortality has been well established in numerous studies. 13 Despite the known benefits, however, persistence with statins, especially in patients at high risk of cardiovascular events, is less than ideal.14-17
With these issues in mind, the purpose of this study was to examine the relationships among community pharmacy–based inducement programs, medication adherence, and health outcomes. We hypothesized that patients using pharmacies with inducement programs to obtain their prescription refills would have better adherence and a lower risk of ACS events compared with patients using pharmacies that do not have inducement programs.
Methods
Population and Setting
The University of Alberta Health Research Ethics Board approved our study protocol. The administrative health databases from Alberta, Canada, were used to conduct a retrospective cohort study. These databases are used to manage provincially funded programs that provide coverage to all Alberta residents for prescription medications, physician visits, emergency department visits, and hospitalizations. As a secondary data source, these databases have been used extensively for epidemiological studies because of the linkability and high level of accuracy and completeness of data.18-21 Briefly, the Population Registry database contains demographic information for all eligible residents; the physician claims database captures the date and medical diagnoses for a visit; the Ambulatory Care database captures the date and medical diagnoses for facility-based ambulatory care, including emergency department visits; the Discharge Abstract Database contains the admission and discharge dates as well as medical diagnoses for hospitalizations; and the Vital Statistics database contains information from birth and death records. 18 The Pharmaceutical Information Network (PIN) database was a major source of information for this study. This database captures information on prescription drug dispensations in Alberta, including the date, pharmacy, World Health Organization Anatomical Therapeutic Chemical (WHO-ATC) classification code to identify active ingredients, 22 strength, quantity, and days of supply.
Alberta residents were eligible for this study if they had at least 1 physician visit for diabetes or hypertension between April 1, 2008, and March 31, 2014. Statin therapy is often recommended for these individuals because of the higher risk of cardiovascular disease compared with the general population.10,11 Residents were included if they were aged 20 years or older, started statin therapy between April 1, 2009, and December 31, 2013, and were alive 455 days after the first statin dispensation. The new-user definition was used to identify participants starting statin therapy. 23 A statin dispensation (WHO-ATC codes C10AAxx) was considered a new therapy start if there were no statin dispensation records in the preceding year.22,23 The dispensation date for the new therapy start was used as the index date, and participants were followed until they died, moved out of the province, or March 31, 2014, the last date of our study observation period. The window of April 1, 2009, to December 31, 2012, was used to identify new statin users with a minimum of 455 days of follow-up (Figure 1).
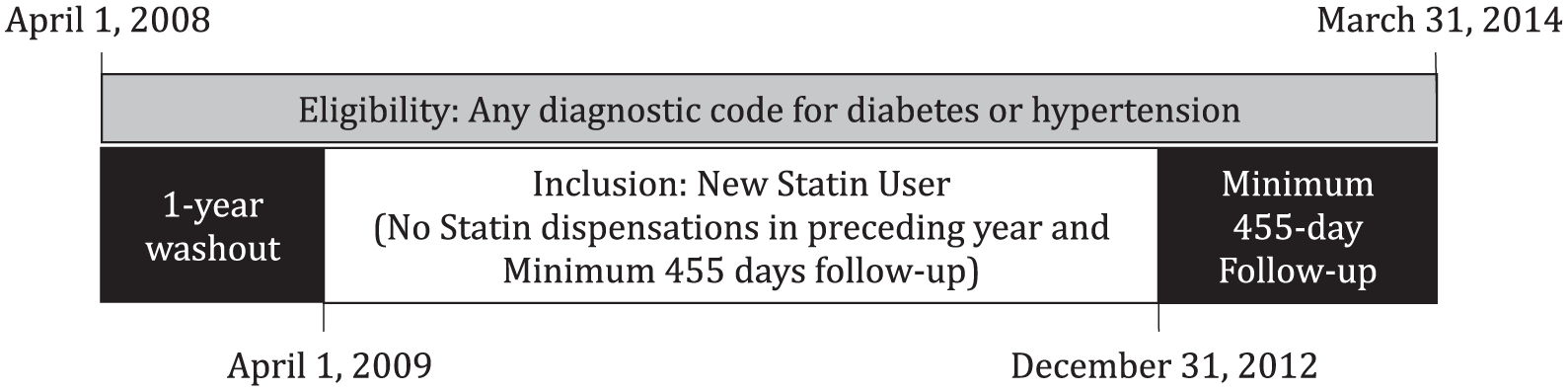
Inclusion criteria and time periods.
Exposure
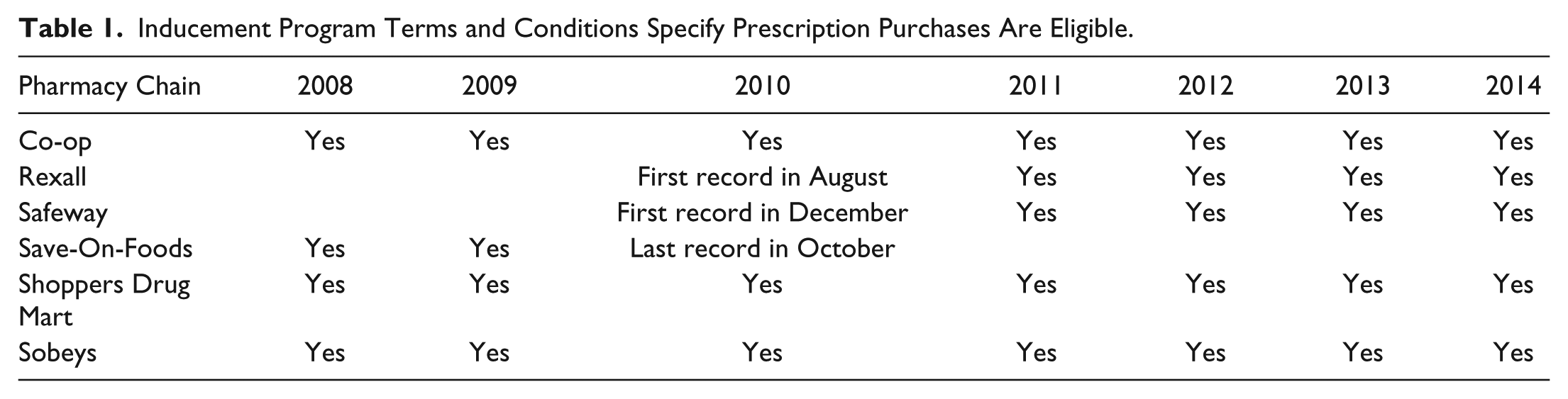
The terms and conditions for inducement programs provided by pharmacies operating in Alberta, Canada, were reviewed using Internet Archive (archive.org). This resource began archiving information from the internet in 1996 to ensure that website content remains accessible.24,25 For example, Internet Archive has been used to identify plagiarism and detect initial signals of adverse drug reactions from information posted on the internet.26,27 We searched the archive for information posted on pharmacy and inducement program websites between January 2008 and December 2014 to determine if prescription purchases were eligible for the inducement program during our study observation period. Based on historical copies of websites stored in the archive, we identified that 6 pharmacy chains included prescription drug purchases in the inducement program (appendix and Table 1). Three pharmacy chains had information that prescription purchases were included in the inducement program for the entire study observation period, 1 pharmacy chain had information up until October 2010, and 2 pharmacy chains had information beginning in 2010. Because the Internet Archive stores copies of website content at intermittent intervals, we assumed that the inducement programs for the 3 pharmacy chains with incomplete information included prescription purchases for the entire study period.
Inducement Program Terms and Conditions Specify Prescription Purchases Are Eligible.
Inducement program features were very similar for 5 of the 6 pharmacy chains (appendix). Three pharmacy chains used an external program (Air Miles [airmiles.ca] or Aeroplan [Aeroplan.com]) and 2 pharmacy chains used an internal program (Morerewards.ca or shoppersdrugmart.ca/optimum) that awarded points for money spent on purchases. The points are then exchanged for a variety of rewards, including tickets to attractions and events, merchandise, and travel. The major differences among the incentive programs were the ratio of dollars spent to points awarded and the number of points required for a reward. The remaining pharmacy chain is operated as a cooperative, with customers purchasing a one-time investment to become a member-owner of the cooperative. Each year, the cooperative distributes its profits to the member-owners, with the portion awarded dependent on the value of all purchases made at the cooperative throughout the year. Thus, members with a larger amount of purchases over the year receive a larger portion of the cooperative profit.
The remaining pharmacies operating in Alberta were categorized as noninducement pharmacies because there was information available to indicate that prescription purchases were not eligible for the inducement program or the pharmacies did not have an inducement program.
Prior to releasing the administrative data, Alberta Health reviewed the PIN data and provided a variable to indicate if the prescription was obtained from an inducement pharmacy or a noninducement pharmacy. Although this process ensured that the investigators were blinded to the identity of the dispensing pharmacy, it could introduce misclassification if a prescription was obtained when prescription purchases were not included in the inducement program. As a sensitivity analysis, we restricted the study observation period to 2011 to 2014 because 5 of the 6 pharmacy chains had clear information that prescription purchases were included in the inducement program (appendix and Table 1).
All statin dispensations in the first year following the participant’s index date were reviewed for group assignment. Participants were assigned to the inducement group if they obtained all statin dispensations from pharmacies with inducement programs. Similarly, participants were assigned to the noninducement group if they obtained all statin dispensations from pharmacies that did not have inducement programs. Those who obtained statin dispensations from both inducement and noninducement pharmacies during the first year of follow-up were excluded from further analyses.
Outcomes
Our first major outcome was discontinuation of statin therapy within the first year of the index date. We assumed that a study participant discontinued statin therapy within the first year if there was no statin dispensation record during a 180-day window, between 275 and 455 days after the index date. This window was chosen for 3 reasons. First, statin persistence at 1 year is an important treatment milestone that is associated with a lower risk of long-term mortality.14-17 Second, many studies define treatment discontinuation as a 180-day gap with no dispensation records. 28 We operationalized this definition by centering the 180-day window over our 1-year treatment milestone. Third, a preliminary assessment of our database identified that the mean days supplied for statin dispensations was 57.9 (±38.1) days, and 75% of the refill intervals were 98 days or less. Therefore, it was reasonable to assume that no record of dispensation within a 90-day interval before and after the 1-year milestone was a strong indicator of treatment discontinuation by 1 year.
Additional adherence-related outcomes were used in sensitivity analyses to test robustness of our main definition for discontinuation. First, we calculated a MPR based on dispensation records in the first year of statin therapy and using a standard formula. 28 Good adherence to statins in the first year of therapy was defined as a MPR ≥0.8. Second, we defined discontinuation as failure to obtain a second dispensation. Third, we defined discontinuation as the absence of a subsequent dispensation record within 150% of the days supplied. 28 Fourth, we excluded all participants with ≥1 hospitalization during the observation period because this would be considered immeasurable time and could lead to misclassification. 29 Fifth, we applied our main definition for discontinuation to a different drug class by identifying new metformin users who stopped therapy within the first year.
Our second major outcome was the occurrence of an ACS event between 456 days and 3 years following the index date. Participants with a nonfatal ACS event during the period used to identify treatment discontinuation were excluded from this analysis. A hospitalization, emergency department visit, or death was considered attributable to an ACS event if there were International Classification of Diseases (ICD) codes to indicate a myocardial infarction (ICD-9 codes 410.xx or ICD-10 codes I21.xx or I22.xx) or unstable angina (ICD-9 codes 411.xx or ICD-10 codes I20.xx). These codes have been used in previous studies and are strongly predictive of an ACS event.30,31 As a composite outcome, we only counted the first event and used the hospital admission date or date of death for the event date. We also examined the risk of all-cause hospitalization or death because there are concerns that inducement programs may have a negative impact on health outcomes.5,6 This outcome would provide a balanced assessment of the risks and benefits associated with inducement programs. 32
Covariates
Covariates were selected based on availability in the Alberta Health databases and previous evidence suggesting an association with either adherence or ACS event risk. 13 Participant demographic information, including age on index date and sex, was obtained from the Population Registry database. Dispensation records from the PIN database were used to identify cardiovascular and antidiabetic medications used within the year prior to the participant’s index date. Physician visits, emergency department visits, and hospital admissions within the year before the index date were used to identify comorbid conditions. We used the ICD-9 and ICD-10 codes in the diagnostic fields to identify a prespecified list of comorbidities. 33 We also included the overall number of hospitalizations within the year before the index date. Finally, we used the participant’s forward sortation area to identify urban or rural residence and estimate household income based on the 2006 Census Canada median household income.
Statistical Analyses
Descriptive statistics were calculated for baseline characteristics to compare participants according to the type of pharmacy used to obtain all statin dispensations in the first year of therapy. Between-group differences were measured using standardized differences, calculated as the difference in means or proportions divided by the pooled estimate of the SD for the variable. Standardized difference has an advantage over significance testing because it is not influenced by sample size, and it is useful for comparing cohorts in large observational studies. 34 Values of 0.1 or less indicate a negligible difference between groups. 35
Logistic regression models were used to estimate the unadjusted and adjusted odds ratios and 95% confidence interval (95% CI) for statin discontinuation according to the type of pharmacy used to obtain all statin dispensations in the first year of therapy. Participants in the noninducement group served as the reference group. The multivariable analysis was constructed to determine if use of pharmacies with inducement programs was an independent predictor of discontinuation after adjusting for all covariates described previously. In each sensitivity analysis, we used the same multivariable logistic regression model but replaced the dependent variable with the additional adherence-related outcome variables described previously.
We used survival analyses and Cox proportional hazards regression models to estimate the hazard ratio and 95% CI of an ACS event according to type of pharmacy used to obtain statin dispensations in the first year of therapy and according to discontinuation of statin therapy. The latter analysis was conducted to ensure our models replicated previous studies demonstrating a higher risk of ACS associated with the discontinuation of statin therapy. 13 The multivariable hazard ratio models included all covariates described previously. In our sensitivity analyses, we replaced ACS events with all-cause hospitalization or death as the dependent variable to examine risk according to type of pharmacy used to obtain statin dispensations and according to discontinuation of statin therapy.
All analyses were conducted using SAS 9.4 (SAS Institute Inc, Cary, NC). A P value <0.05 was considered statistically significant.
Results
A total of 168 868 participants started statin therapy between April 1, 2009, and December 31, 2013, and 159 998 (94.7%) participants obtained all their statin refills from either an inducement pharmacy or noninducement pharmacy during the first year. The mean age of the study group was 60.2 (±13.7) years; 67 534 (42%) were women; 132 545 (83%) lived in an urban setting; and the mean household income was $66 296 (±$18 590). In comparison, the mean age of adult Canadians living with diabetes or hypertension is 61.9 (±0.4) years; 48% are women; and 82% live in an urban setting36,37; the median household income in Alberta was $69 669. 38 After reviewing the source of statin dispensations in the first year of therapy, 77 803 (49%) participants obtained all their dispensations from pharmacies with inducement programs (Table 2). These inducement group participants were more likely to live in urban settings (standardized difference 0.42) and have a higher household income (standardized difference = 0.22). The remaining demographic characteristics, concurrent medications at baseline, and disease burden were similar between inducement group participants and noninducement group participants (standardized difference <0.1 for all comparisons).
Baseline Characteristics by Type of Pharmacy Used for Statin Dispensations in the First Year of Therapy.
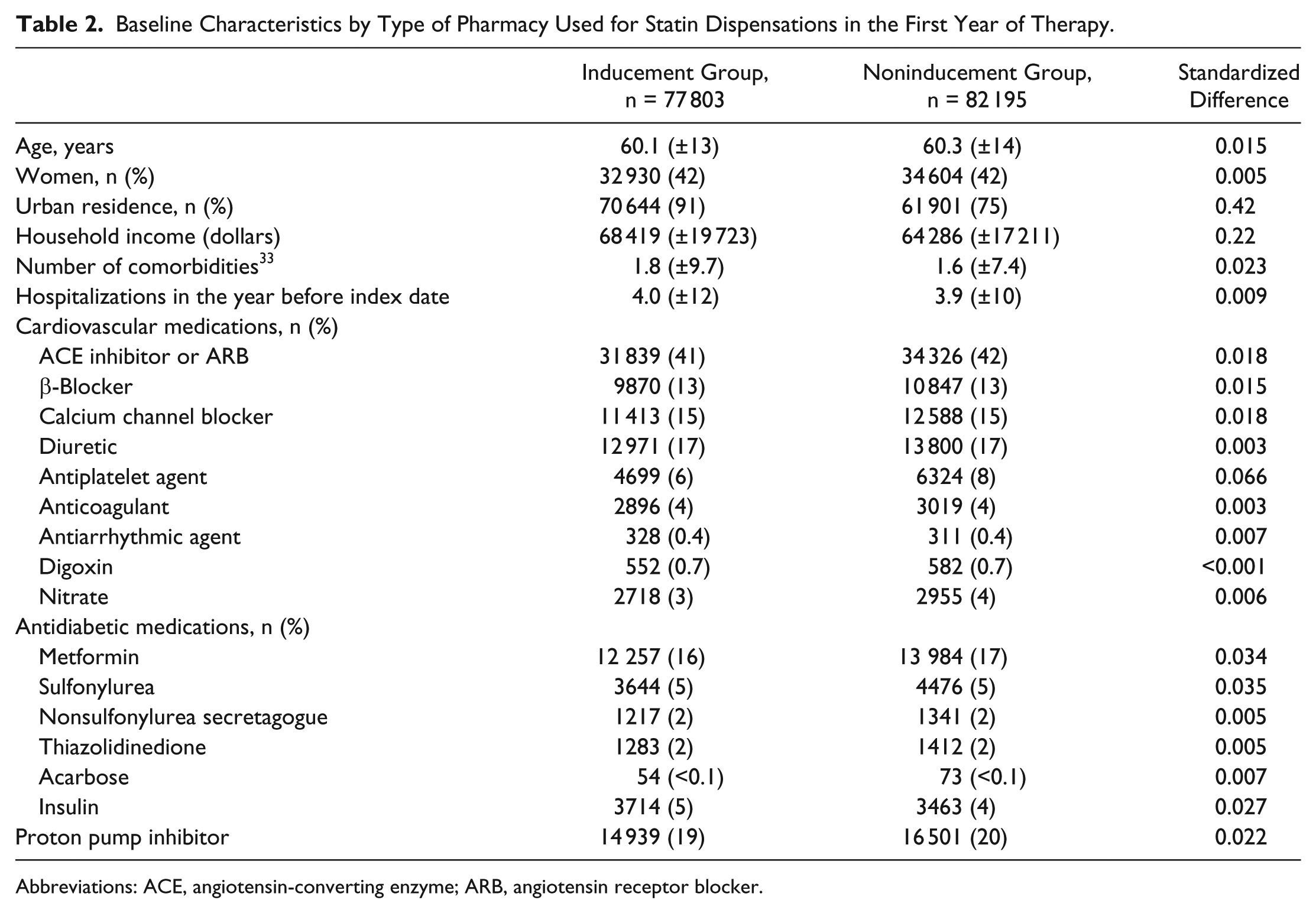
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker.
Treatment Discontinuation
A total of 48 271 (30%) new statin users discontinued therapy within the first year. Comparisons of discontinuation and adherence according to type of pharmacy used to obtain statin dispensations are presented in Table 3. Among inducement group participants, 22 455 (28.9%) discontinued statin therapy, whereas 25 816 (31.4%) noninducement group participants discontinued statin therapy (P < 0.001). Inducement group participants were also more likely to have better adherence rates (MPR ≥ 0.8) compared with noninducement group participants (P < 0.001). When we changed the definition used to identify discontinuation, excluded patients who were hospitalized during the first year of statin therapy, restricted our study observation window to 2011 to 2014, and changed our indicator medication to metformin, the observed associations were consistent in direction, magnitude, and statistical significance to our main analysis (Table 3).
Treatment Discontinuation and Adherence by Type of Pharmacy Used for Statin Dispensations in the First Year of Therapy.
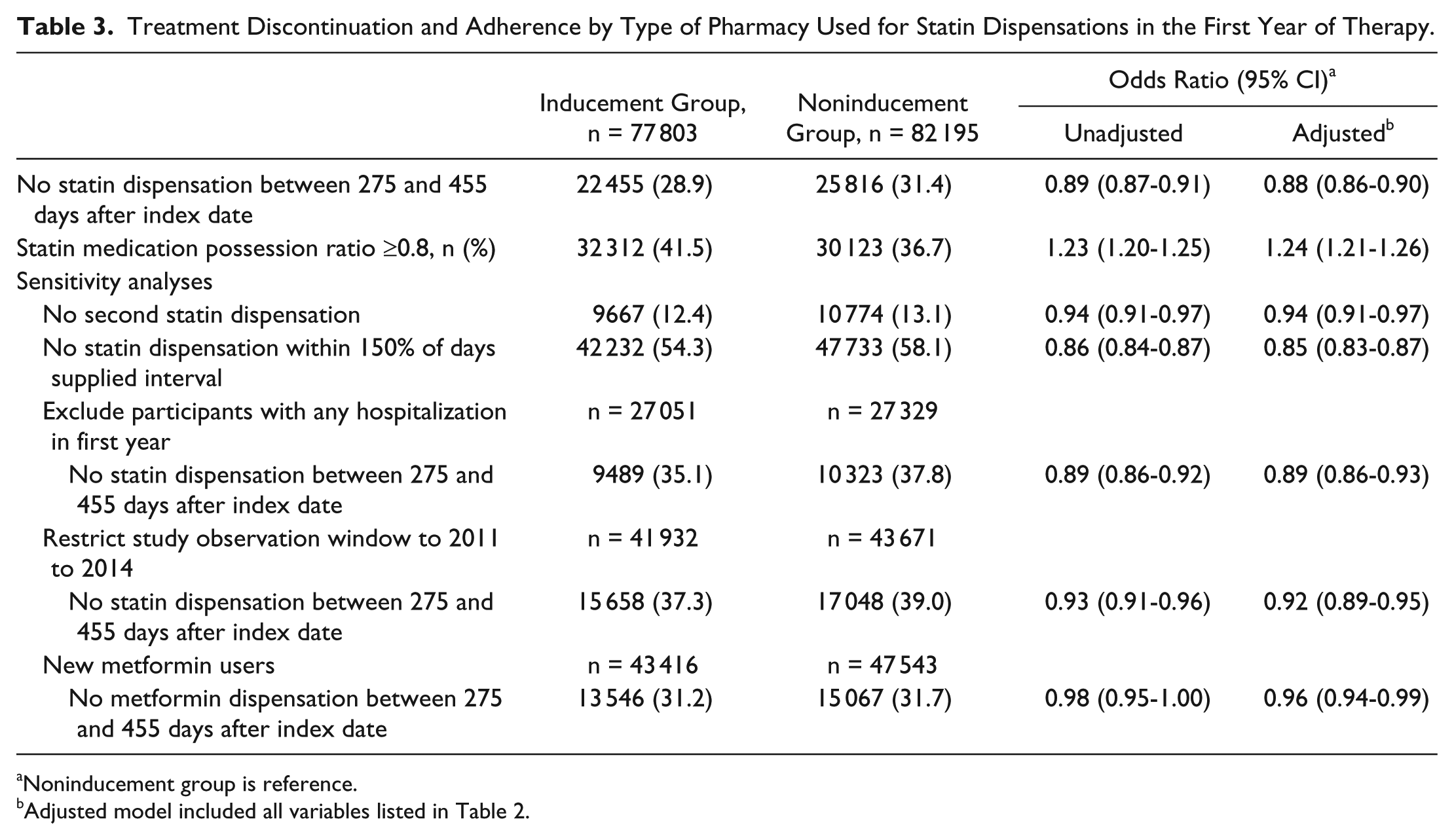
Noninducement group is reference.
Adjusted model included all variables listed in Table 2.
Risk of ACS Event
We excluded 21 833 (13.6%) participants from this analysis because they were hospitalized or visited an emergency department for an ACS event within 455 days of starting statin therapy. There was no difference in the number of participants excluded according to type of pharmacy used to obtain statin dispensations in the first year of therapy (P = 0.18). Baseline characteristics of this subgroup with no history of an ACS event up to 455 days after starting statin therapy are presented in a Supplemental Table (available at http://aop.sagepub.com/supplemental). As with the full cohort, inducement group participants were more likely to live in urban settings (standardized difference = 0.42) and have a higher household income (standardized difference = 0.22). The remaining demographic characteristics, concurrent medications at baseline, and disease burden were similar between inducement group participants and noninducement group participants (standardized difference <0.1 for all comparisons).
After a mean of 2.3 (±0.9) years of follow-up, 2284 participants were hospitalized or died because of an ACS event between 456 days and 3 years after starting statin therapy. Among inducement group participants, 1079 (1.6%) had an ACS event, whereas 1205 (1.7%) participants in the noninducement group had an ACS event (P = 0.91; Table 4). Participants who discontinued statin therapy within the first year were more likely to have an ACS event compared with participants who did not discontinue statin therapy (P = 0.0029). Participants with good adherence to statin therapy (MPR ≥ 0.8) were less likely to have an ACS event compared with participants with poor adherence (P < 0.001). When we examined the risk of all-cause hospitalization or death (Table 4), there were no significant associations with type of pharmacy used to obtain statin dispensations (P = 0.79) or discontinuation of statin therapy (P = 0.91).
Risk of Clinical Outcomes Between 456 Days and 3 Years After Starting Statin Therapy According to Participant Group.

Adjusted model included all variables listed in Table 2.
Participants with a hospitalization or emergency department visit for an acute coronary syndrome event within 455 days of starting statin therapy were excluded.
Reference group.
Participants with a hospitalization or emergency department visit for any reason within 455 days of starting statin therapy were excluded.
Discussion
This study examined the relationships among pharmacy inducement programs, medication adherence, and health outcomes in a population-based group of participants starting statin therapy. We found a lower risk of discontinuation associated with the use of pharmacies with inducement programs. This observed association persisted regardless of the definition used to identify discontinuation of statin therapy or switching to metformin as the medication of interest. We also found that participants using pharmacies with inducement programs were more likely to have better adherence to statin therapy. Use of pharmacies with inducement programs did not, however, have any significant association with risk of ACS events or all-cause hospitalization or death.
Our findings are consistent with the study by Staskon et al, 1 which reported a significant association between use of an inducement program and better medication adherence. Although we extended our analysis to clinical outcomes, we did not find an association between use of pharmacies with inducement programs and risk of ACS events or all-cause hospitalization or death. The absence of a statistically significant difference may have been a result of the relatively short follow-up time (mean = 2.3 years) and small absolute difference in the proportion of participants experiencing an ACS event (0.1%) or all-cause hospitalization or death (1.1%). However, we did reaffirm the link between poor adherence to statins and higher risk of adverse cardiovascular outcomes that has been demonstrated in more than 25 observational studies. 13 Collectively, these findings support the premise that pharmacy-based inducement programs promote good adherence to prescribed medications, which may indirectly lower a patient’s risk of adverse events.13,39
There is substantial interest in the role inducement programs may play in community pharmacy practice.5-9 For example, the Colleges of Pharmacy in Alberta and British Columbia have called inducement programs unprofessional and unsafe, suggesting that inducement programs could have a negative impact on treatment goals and health outcomes.5,6 In fact, both colleges have taken steps to prohibit inducement programs in pharmacies. However, consumer groups, pharmacists, and pharmacy chains have challenged this decision, in part because of a lack of empirical evidence of harm.8,9,40-42 Whereas this study found a definitive lack of harm for pharmacy-based inducement programs, the positive association with medication adherence is also worth noting. Inducement programs may provide a patient-level incentive that encourages medication adherence.
Our observations should be interpreted in light of the study limitations. First, the observational study design limits our ability to infer a causal link between use of pharmacies with inducement programs and better medication adherence. We are unable to rule out the possibility of selection bias as well as the influence of unmeasured confounding at the patient and pharmacy levels. For example, other factors apart from an inducement program could influence a patient’s decision to use a specific pharmacy, including the location, store environment, professional services provided, and trust in the pharmacist.43,44 At the pharmacy level, daily prescription volume, number of pharmacists and pharmacy technicians, time spent counseling, and other factors may result in consistent management across patients. Although a hierarchical analysis could account for clustering of patients within a pharmacy and control for some of these factors, 45 we do not have information to identify the dispensing pharmacy. It would, therefore, be important to test the hypothesis generated from this cohort study in a randomized controlled trial. Second, although about 95% of Alberta pharmacies submit data to PIN, <5% of prescribers submit prescriptions to this database. 18 Primary nonadherence, the failure to fill an initial prescription, is an important influencing factor in overall persistence and adherence measurements.46,47 Future work in this area should examine the influence of inducement programs on primary nonadherence. Third, we assumed that website content stored in Internet Archive accurately described historical terms and conditions of the inducement programs. Fourth, website content stating prescription purchases were eligible for the inducement program was available for only half of the study observation period for 3 pharmacy chains. In the main analysis, we assumed that these 3 pharmacy chains included prescription purchases in the inducement program for the entire study period, which could introduce misclassification if study participants obtained dispensations when the inducement program did not include prescription drugs. However, a sensitivity analysis designed to minimize the risk of misclassification bias produced results that were consistent in direction, magnitude, and statistical significance to our main observation. Fifth, the use of forward sortation area to estimate income is more prone to misclassification compared with other methods, such as enumeration area. 48 However, Alberta Health only provides the first 3 digits (or the forward sortation area) of the Canadian postal code, and all 6 digits are required to identify enumeration area. Finally, as with any observational study of medication adherence, we assumed acquisition of medication supply with dispensation records indicates consumption. This assumption would overestimate adherence if people do not use the medications they obtained from pharmacies. The possibility of misclassifying this outcome is most likely similar between inducement and noninducement groups but would not have a substantial effect on the observed association.
In summary, this population-based study found an important association between use of pharmacies with inducement programs and better medication adherence. Although we did not observe a direct association between use of pharmacies with inducement programs and health outcomes, our study confirms previous observations that better adherence is associated with a lower risk of adverse cardiovascular outcomes.
Footnotes
Appendix
Copies of Website Content Retrieved From Internet Archive.
| Table of Contents | |
|---|---|
| Co-op Membership Benefits | |
| (May 2007 to March 2011) | Page 1 |
| (February 2012 to May 2015) | Pages 2-4 |
| Rexall Pharmacy Aeroplan Miles (August 2010 to July 2014) | Pages 5-6 |
| Safeway Air Miles (December 2010 to December 2015) | Pages 7-8 |
| Save-on-Foods Save On More Rewards (May 2007 to October 2010) | Pages 9-11 |
| Shoppers Drug Mart Optimum Program Terms and Conditions | |
| (February 2003 to April 2010) | Pages 12-18 |
| (May 2010 to February 2015) | Pages 19-28 |
| Sobeys Aeroplan Miles (September 2008 to March 2015) | Pages 29-30 |
Acknowledgements
This study is based in part on data provided by Alberta Health. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta. Neither the Government of Alberta nor Alberta Health express any opinion in relation to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was investigator initiated and not funded.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.