
Abstract
Introduction
After decades of pushing for patients with elevated low-density lipoproteins (LDL) to achieve a target LDL concentration, the major cardiovascular organizations in the United States stepped back from this approach opting instead for statin monotherapy with an intensity of dosing predicated on baseline risk.1,2 This was driven by clinical trial evidence that was abundant for the statins coinciding with lackluster outcomes from trials assessing adjunctive therapy on top of statins at the time.1,2 However, recent clinical trial evidence suggests that a return to LDL therapy goals are warranted and this is starting to be reflected in some more recent guidelines but not yet within those from the American Heart Association (AHA) and the American College of Cardiology (ACC).2-4
In this article, we will discuss the evolution of major hyperlipidemic guidelines starting with the National Heart, Lung and Blood Institute’s National Cholesterol Education Program Adult Treatment Panel guidelines and progressing to guidelines from 2016 and 2017.1-5 The major clinical trials driving the evolution in these guidelines over time will be presented. Recommendations for clinicians trying to reconcile the 3 most recent guidelines and determining whether or not to use LDL targets, what targets to strive for, and whether or not to use adjunctive therapy with statins will be discussed. Finally, the role of the pharmacist in helping patients achieve LDL goals will be presented.
Data Sources, Study Selection, and Data Extraction
We conducted a MEDLINE search from January 1980 to May of 2017 using terms including “LDL,” “lipid,” “hypercholesterolemia,” “ezetimibe,” “PCSK9,” and “statin,” with forward and backward citation tracking. English-language clinical trials or meta-analyses of secondary prevention trials assessing LDL-lowering therapy were included if they had relevant, nonduplicative information as were guidelines on the treatment of elevated LDL cholesterol. Using the same approach we searched using the terms “cholesterol” and “management” and “pharmacist” to identify studies where a pharmacist was involved in helping patients improve their lipid therapy and achieve guideline specific levels.
National Treatment Guidelines Over Time
From 1985 through 2013, the National Heart, Lung and Blood Institute’s National Cholesterol Education Program Adult Treatment Panel (NCEP ATP) focused on achieving a target goal for LDL. 1 In the last guidelines from this group (NCEP ATP III), patients with high, moderate, and low risk of experiencing cardiovascular events (10-year risk of cardiovascular events >20%, 10% to 20%, and <20%), using Framingham risk assessment, had LDL goals defined as <100 mg/dL (<70 mg/dL as a reasonable alternative goal), <130 mg/dL, and <160 mg/dL. 1
The National Heart, Lung and Blood Institute turned over the coordination and dissemination of lipid guidelines to the AHA and the ACC. 2 The AHA/ACC guidelines were published in November 2013 and made no recommendation for or against using LDL targets, but their guidelines are not predicated on achieving specific LDL concentrations. 2
The AHA/ACC 2013 guidelines assert that statins should be the treatment of choice in hypercholesterolemia management in secondary prevention (atherosclerotic cardiovascular disease [ASCVD] defined as acute coronary syndromes (unstable angina, myocardial infarction) or stable angina, stroke or transient ischemic attack, peripheral arterial disease of atherosclerotic origin, or arterial revascularization [coronary, cerebrovascular, leg artery]) or primary prevention. 2 In patients with ASCVD, high-intensity statin therapy (atorvastatin 40 or 80 mg, rosuvastatin 20-40 mg; therapy that reduces LDL by >50%) should be initiated in people <75 years. 2 If high-intensity statin therapy is not tolerated or likely not to be tolerated, moderate-intensity statin therapy (therapy that reduces LDL by 30% to 49%) should be employed. In people >75 years with ASCVD, the balance of benefits to harms, risk of drug interactions, and patient preferences are considered when initiating moderate- or high-intensity statins, and it is reasonable to continue statin therapy in those who are tolerating it. 2
People with an LDL of >190 mg/dL but without ASCVD should be checked for secondary causes for hypercholesterolemia (dietary excess, drugs, diseases, and metabolism disorders) with treatment for the cause. 2 They should also receive the highest tolerated intensity of statin therapy, preferably high-intensity therapy. Once the maximum tolerated statin dose is achieved, an adjunctive nonstatin drug may be considered.
They then describe the approach to patients without ASCVD but with an LDL of 70 to 189 mg/dL. If they have diabetes mellitus they should have moderate intensity statin therapy. 2 If their 10-year ASCVD risk (as determined by the my.americanheart.org/cvriskcalculator) is >7.5%, high-intensity statins rather than moderate-intensity statins can be employed. For those patients <40 or >75 years, the benefits and risks, drug interactions, and patient preference should be considered before using a statin. In people with the same LDL levels (70-189 mg/dL) who are 40 to 75 years but without diabetes mellitus, the ASCVD risk calculation is needed to determine therapy. Those with a >7.5% risk of ASCVD should receive moderate- to high-intensity therapy, while those with a 5.0% to 7.4% risk can consider using a moderate-intensity statin. These guidelines are currently the ones used by most clinicians in the United States. 2
A 2016 ACC expert consensus document assessed the role of adjunctive therapy and made the following recommended alterations of the AHA/ACC 2013 guidelines. 5 They state that ezetimibe or PCSK9 inhibitors can be considered for patients with ASCVD, with or without comorbidities, in patients not achieving ≥50% LDL reduction with statins. This is if adherence, lifestyle modifications, and patient preferences are assessed thoroughly. They also say a clinician “may consider” an LDL a goal of <100 mg/dL in ASCVD patients when secondary causes are absent and the LDL level is <190 mg/dL or <70 mg/dL when secondary causes are present or the LDL level is ≥190 mg/dL, respectively. Ezetimibe is recommended as the first drug added with PCSK9 inhibitors and only utilized if statin and ezetimibe therapy is insufficient, regardless of how far away the patient is from reaching the stated LDL goal on statin alone. Patients without ASCVD or secondary causes but an LDL ≥190mg/dL, diabetes, or a 10-year ASCVD risk ≥7.5% may consider an LDL goal of <100 mg/dL but should nonetheless achieve LDL reductions of 50% in the first 2 scenarios and 30% to 49% in the third. Ezetimibe and PCSK9 inhibitors could be used in scenarios 1 and 2 but only ezetimibe (with a bile acid sequestrant as second-line therapy) is recommended in the third scenario. 5
In August 2016, the European Society of Cardiology (ESC) along with the European Atherosclerosis Society (EAS) developed their guideline. Its recommendations are a hybrid of the NCEP ATP III and the ACC/AHA 2013 approaches. 3 Patients with ASCVD, diabetes mellitus, or chronic kidney disease are considered high or very high risk. For all other patients, they recommend using the Systematic COronary Risk Evaluation (SCORE) system, which estimates the 10-year cumulative risk of a first fatal ASCVD event (scoring criteria given in ESC/EAS 2016 guidelines), unlike the ACC/AHA CV risk calculator, which estimates fatal and nonfatal event risk. The SCORE assessment has been validated in several different populations and country-specific calibrated versions are also available, but a US version does not currently exist. 6 Patients with low and moderate ASCVD death risk have a 10-year risk of “<1%” and “1% to <5%,” while those with risks of “5% to <10%” and “10% or greater” are classified as high or very high risk, respectively. All patients with ASCVD are considered very high risk, as are those with diabetes mellitus who have target organ damage such as retinopathy or nephropathy. Patients with a marked elevation in total cholesterol (>310 mg/dL) or blood pressure (>180/110 mm Hg) would be considered high risk even if the SCORE risk was <5%, as would all other patients with diabetes mellitus. In patients at very high ASCVD risk, an LDL goal of <70 mg/dL or a 50% or greater reduction from baseline if the LDL is 70 to 135 mg/dL is recommended. In patients at high ASCVD risk, an LDL goal of <100 mg/dL or a 50% or greater reduction from baseline if the LDL is 100 to 200 mg/dL is recommended. In subjects at low or moderate risk, a target LDL of <115 mg/dL is recommended. Statins are considered the preferred baseline therapy in all patients not achieving their goal, and the dose should be maximized to achieve the LDL goal or to the maximum tolerated dose. Unlike the ACC/AHA 2013 guideline, the ESC/EAS 2016 guideline specifically recommends adjunctive therapy if the LDL goals are not achieved and recommends that ezetimibe be the preferred second-line therapy for resistant patients. 3
In April of 2017, the American Association of Clinical Endocrinologists (AACE) along with the American College of Endocrinology (ACE) released a guideline. 4 Like the ESC/EAS 2016 guideline, it establishes LDL goals based on cardiovascular risk categories; however, unlike previous guidelines, it creates an extreme risk category. Patients are categorized as extreme risk if they have clinical cardiovascular disease in addition to diabetes, stage 3-4 chronic kidney disease or heterozygous familial hypercholesterolemia, progressive ASCVD despite reaching an LDL <70 mg/dL, or developed ASCVD before the age of 55 years for men or 65 years for women. The remaining categories require an assessment of risk factors (identified in the Framingham Heart, MRFIT, and INTERHEART studies or previous guidelines), and the calculation of 10-year coronary event risk (which may be determined using several tools including the Framingham Risk Assessment Tool). Low-risk patients have no risk factors, whereas those with 1 to 2 risk factors but a 10-year risk <10% are considered moderate risk. High-risk patients have either ≥2 risk factors and a 10-year risk of 10% to 20% or they have diabetes or stage 3-4 chronic kidney disease with no risk factors. Patients with diabetes or stage 3-4 chronic kidney disease and risk factors as well as those with a 10-year risk >20%, heterozygous familial hypercholesterolemia, recent acute coronary syndrome, or vascular disease (coronary, carotid, or peripheral) are classified as very high risk. 4
In patients at extreme risk, an LDL goal <55 mg/dL is recommended, with an LDL goal of <70 mg/dL given for patients at very high risk. In those at either high or moderate risk, a target LDL of <100 mg/dL is recommended, whereas those at low risk are given an LDL goal <130 mg/dL. 4 Similar to the ESC/EAS 2016 guideline, statins are considered the primary agent and ezetimibe is specifically recommended as adjuvant therapy for reducing LDL.3,4 A notable difference in the AACE/ACE 2017 guideline, however, is the recommendation for adjuvant PCSK9 inhibitor therapy, which may be considered in patients with clinical cardiovascular disease who have not achieved LDL targets on maximally tolerated statin therapy. 4
Clinical Trial Evidence Supporting Guideline Evolution
The NCEP ATP guidelines were based primarily on epidemiologic evidence linking elevations in LDL to increasing risks of cardiovascular outcomes but they were supported by clinical trial evidence showing that lowering LDL with statins also lowered risk. 1 The results of major placebo controlled trials in secondary prevention (eg, CARE, LIPID, HPS, GREACE trials) show that statins reduce the occurrence of subsequent coronary events and mortality.7,8 In people with hypercholesterolemia but no current cardiovascular disease (primary prevention), major placebo controlled trials (eg, WOSCOPS, AFCAPS/TexCAPS, ASCOT-LLA trials) show that statin use reduces subsequent coronary events and may reduce mortality as well.7,8
The AHA/ACC 2013 guidelines were heavily influenced by direct comparative clinical trials such as the TNT, PROVE-IT, SEARCH, IDEAL, and JUPITER trials showing that higher intensity statin therapy was associated with better outcomes than lower intensity statin therapy (Table 1).2,9-15 While they selected people within strict LDL limits at baseline and based on the expected percent reduction the final LDLs that would be achieved, they did not titrate therapy to a set LDL level and therapy was neither titrated down or up based on the LDL achieved.9-13
Study Outcomes From Major Secondary Prevention Trials of Higher Versus Lower Intensity LDL Loweringa,7-11,16,17.
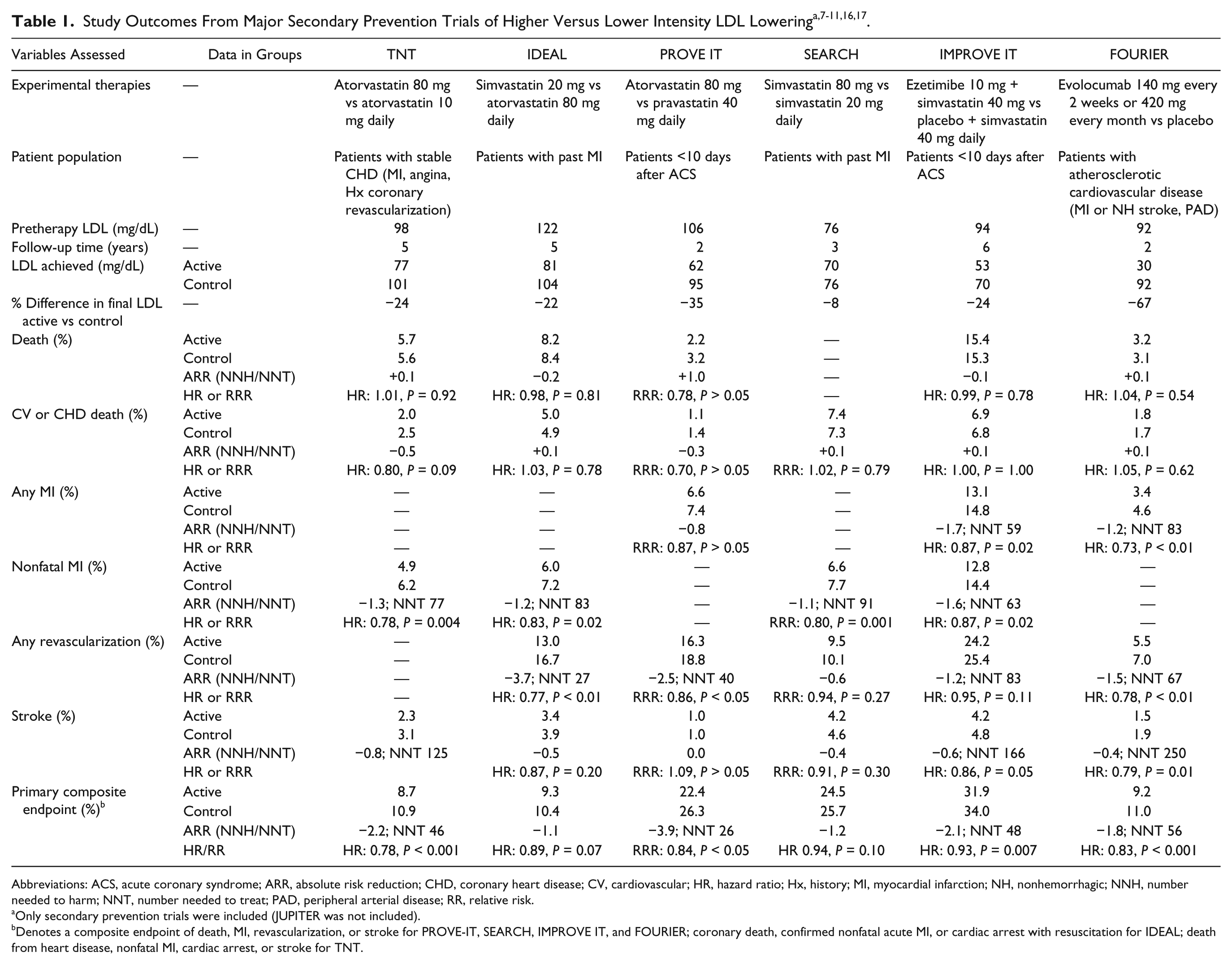
Abbreviations: ACS, acute coronary syndrome; ARR, absolute risk reduction; CHD, coronary heart disease; CV, cardiovascular; HR, hazard ratio; Hx, history; MI, myocardial infarction; NH, nonhemorrhagic; NNH, number needed to harm; NNT, number needed to treat; PAD, peripheral arterial disease; RR, relative risk.
Only secondary prevention trials were included (JUPITER was not included).
Denotes a composite endpoint of death, MI, revascularization, or stroke for PROVE-IT, SEARCH, IMPROVE IT, and FOURIER; coronary death, confirmed nonfatal acute MI, or cardiac arrest with resuscitation for IDEAL; death from heart disease, nonfatal MI, cardiac arrest, or stroke for TNT.
The AHA/ACC 2013 guidelines were also affected by major clinical trials assessing the value of adjunctive therapy with statins. 2 These drugs were being added primarily to enhance high-density lipoproteins, reduce very low density lipoproteins, and/or to shift the relative mix of circulating LDL particles rather than trying to further lower LDL concentrations. These trials (ACCORD, AIM-HIGH, HPS-THRIVE, ILLUMINATE) did not show additional benefit when fenofibrate, niacin, or experimental torcetrapib were used with statins versus using statins alone.2,18-21 Thus aside from statins, there were no clinical trial data to evaluate whether lowering LDL through the use of adjunctive therapy along with statins were better than using maximally tolerated statins alone. 2
The ESC/EAS 2016 guidelines and the AACE/ACE 2017 guidelines were affected by 4 studies unavailable to the AHA/ACC 2013 guideline writing group that directly assessed lower LDL with adjunctive therapy on top of a statin versus a statin alone.2-4 In 2015, there were 3 published trials that assessed the lower LDL hypothesis: the ODYSSEY Long Term, OSLER, and IMPROVE IT trials.14,16,17 The ODYSSEY Long Term and OSLER trials gave the first glimpses into the role that adjunctive PCSK9 inhibitors would have on final health outcomes but were not designed to primarily assess for final health outcomes, aside from assessing a composite cardiovascular endpoint. The ODYSSEY Long Term trial included 2341 patients who were given statins at their maximum tolerated dose before being randomized to alirocumab (150 mg every 2 weeks for 78 weeks) or matching placebo. 16 The OSLER trials included 4465 patients who were included in 2 long-term extension trials (median follow-up 11 months) where they received evolocumab 140 mg every 2 weeks or 420 mg monthly plus standard therapy versus standard therapy alone (70% received statins and 13% to 15% received ezetimibe). 17 In both trials, the LDL was reduced from a baseline around 120 mg/dL to approximately 50 mg/dL.16,17 In these trials the incidence of major adverse cardiovascular events (composite including death, major coronary and cerebrovascular events) was significantly reduced by 49% and 52%, respectively.16,17
The IMPROVE IT and FOURIER trials are included in Table 1 because they were primarily designed to assess final health outcomes.9-15 In the IMPROVE IT trial, patients (n = 18 144; median follow-up, 6 years) within 10 days of a recent myocardial infarction (MI) or unstable angina event were randomized to receive ezetimibe 10 mg daily plus simvastatin 40 mg or simvastatin 40 mg alone. 14 The primary endpoint was a composite of cardiovascular death, nonfatal MI, unstable angina requiring rehospitalization, coronary revascularization, or nonfatal stroke. Those receiving ezetimibe plus simvastatin had a lower on-treatment LDL (53.7 mg/dL vs 69.5 mg/dL, P < 0.001) and fewer ASCVD events (32.7% vs 34.7%, P = 0.016) than those receiving simvastatin alone. These patients had a very high risk for recurrent ASCVD events, having just experienced one within the past 10 days, and they compared adjunctive therapy with ezetimibe on top of moderate- rather than high-intensity statin therapy. 14
The recent FOURIER trial randomized 27 564 patients to evolocumab (either 140 mg every 2 weeks or 420 mg monthly) or placebo. 15 Patients were required to have a history of MI, nonhemorrhagic stroke or peripheral artery disease, and ≥1 major (eg, diabetes, smoking, age ≥65 years) or 2 minor (eg, metabolic syndrome, high-density lipoprotein [HDL] <40, ≥40% residual stenosis in ≥2 large vessels) cardiovascular risk factors. The trial only included those with an LDL ≥70 mg/dL despite an optimized lipid lowering regimen consisting of a statin at least as potent as 20 mg of atorvastatin. The primary composite endpoint was identical to that utilized in the IMPROVE IT trial, while the key secondary endpoint was a composite of cardiovascular death, nonfatal MI, or nonfatal stroke.
At baseline, ~69% of patients in the FOURIER trial were on high-intensity statin therapy and nearly all remaining patients received moderate-intensity statins. A total of 5% of patients were on adjuvant ezetimibe. By 48 weeks, median LDL in those receiving evolocumab had fallen from a baseline value of 92 mg/dL to 30 mg/dL (absolute mean difference vs placebo = 56 mg/dL, P < 0.001), with reductions maintained throughout the trial. Over a median follow-up of 2.2 years, evolocumab therapy reduced the occurrence of both the primary (9.8% vs 11.3%) and key secondary (5.9% vs 7.4%) endpoints versus placebo (P < 0.001 for both). Those receiving evolocumab underwent fewer coronary revascularization procedures (5.5% vs 7.0%, P < 0.001) and had fewer MIs (3.4% vs 4.6%, P < 0.001) and strokes (1.5% vs 1.9%, P = 0.01) versus placebo; however, there was no difference in cardiovascular death between groups (P = 0.62). Injection-site reactions occurred in 2.1% of patients taking evolocumab versus 1.6% of those taking placebo (P < 0.001) but there were no between-group differences in any other safety endpoint, including neurocognitive events.
A key limitation of the FOURIER trial is its short duration (ie, ~2 vs ≥5 years in previous trials assessing lipid lowering therapy).9,13,14 This is important as 2 years may not be long enough to capture adverse events resulting from evolocumab use. Furthermore, like many randomized controlled trials, FOURIER was not designed to measure patient preferences, which is a factor that clinicians considering PCSK9 inhibitors may take into account. 5 Last, ~75% of patients were male and 85% were Caucasian, limiting the applicability of the results to patients with gender and ethnic diversity.
While the benefits on combined major cardiovascular events are proven, there seems to be no reduction in either cardiovascular mortality or overall mortality in any of the clinical trials comparing higher versus lower intensity LDL lowering (Table 1).9-15 Whether these effects will materialize with longer term therapy remains to be seen because even trials of 4 to 6 years have not shown trends toward better survival results than those with less follow-up.
What Should Clinicians Do?
The first question we would like to address is what drug you should start with? The various guidelines agree that starting with a statin, unless contraindicated, is a critical first step when pharmacologic therapy is warranted.2-4 Ezetimibe and PCSK9 inhibitors have not been shown to reduce final health outcomes as monotherapy, ezetimibe is not potent enough to achieve a large enough reduction in LDL alone, and the PCSK9 inhibitors are too expensive to use before statins have been maximized.
The second question is whether intensifying lipid lowering is beneficial and whether the magnitude of benefit from intensifying statin therapy is similar, better, or worse than using an adjunctive agent? Clinical trial data show clearly that further lowering of LDL is better than remaining at higher levels.9-15 This is true whether a higher intensity of statin therapy is given instead of lower intensity statin therapy and is also true when adjunctive therapy with ezetimibe or a PCSK9 inhibitor is given on top of a statin versus the same intensity of statin therapy given alone.9-15
In a meta-analysis of 27 statin trials, the Cholesterol Treatment Trialists (CTT) found that higher intensity statins were more effective than lower intensity statins. 7 Furthermore, they found a linear relationship where every 39 mg/dL reduction in LDL yielded a 22% reduction in major cardiovascular events over 5 years of therapy. The average risk reduction over 5 years takes into consideration the lower risk reduction during the first year of therapy, which was only 12% and then increases over the next couple of years before leveling off and maintaining that benefit. 7 Applying data from the ODYSSEY Long Term, OSLER, and IMPROVE IT trials to the aforementioned CTT meta-analysis does not change the relationship between LDL reduction and major cardiovascular events after 5 years of therapy or the magnitude of that reduction. 8 According to the FOURIER investigators, their 2-year major cardiovascular event results are also in line with the projected benefits from the CTT meta-analysis based on the magnitude of lipid reduction. 15
The number and size of trials quantifying the benefits of higher versus lower intensive statin therapy and our familiarity with this class of drugs is much better than the alternative adjunctive agents.9-17 As such, pushing to the maximum statin dose or the maximum tolerated dose before moving to adjunctive therapy is reasonable.2-4 After so many years, we can now say with confidence that people who cannot tolerate high- or moderate-intensity statins or have not fully responded to statins can benefit from ezetimibe or PCSK9 inhibitor adjunctive therapy.14,15 This means that the AHA/ACC 2013 guidelines should no longer be used to justify only using high- or moderate-dose statins based on baseline risk. 2 People should be treated to some LDL target level even if it means adjunctive therapy is required.3,4 The ACC 2016 consensus recommendations support this move although they also say that clinicians may consider using an LDL goal rather than supporting such a move outright. 5 However, the FOURIER results were not yet available at the time of their literature assessment. Niacin and fibric acid derivatives should not be considered adjunctive agents solely for the lowering of LDL or the raising of HDL given the lackluster results of their clinical trials and the benefits of adjunctive bile acid sequestrants is not known.18-20
The third question is how low should you go? Since there seems to be a linear relationship between lowering LDL cholesterol in people achieving LDLs of 30 mg/dL and greater, there may be a tendency to attempt to get every patient to an LDL goal of 30 mg/dL.7-15 However, none of the older or newer guidelines advocates this approach.2-4 That is because a 20% reduction in the risk of a major cardiovascular event affects patients with high baseline risk to a much greater extent than someone with a lower baseline.7,8 This is demonstrated in an assessment of the number of patients needed to treat (NNT) with greater intensity of LDL lowering for 5 years to reduce 1 additional major adverse cardiac event. 8 In Figure 1, the NNT for a patient at different baseline levels of ASCVD event risk are estimated using the CTT relationship between LDL lowering and major adverse cardiovascular events. This 20% reduction in LDL can be achieved by using adjunctive ezetimibe or by increasing the statin from low- to high-intensity therapy (doubling the statin dose 3 times; eg, atorvastatin 10 vs 80 mg). The 50% reduction is for patients receiving adjunctive PCSK9 inhibitors. This figure shows that the NNT goes down substantially if the patient’s baseline LDL is high, the patient’s baseline risk of ASCVD events is high, and the intensity of LDL lowering is large. 8 Placing 200 patients on a combination of statins, ezetimibe, and PCSK9 inhibitors for 5 years to only prevent one major adverse cardiovascular event without affecting overall mortality or cardiovascular mortality is not pragmatically or economically reasonable. It is more rational to determine a target LDL level where the resultant chance of preventing an ASCVD event with lipid lowering therapy is higher.3,4 The ACC 2016, ESC/EAS 2016, and the AACE/ACE 2017 specify realistic targets, although the ACC targets should be recommended rather than simply considered.3,4
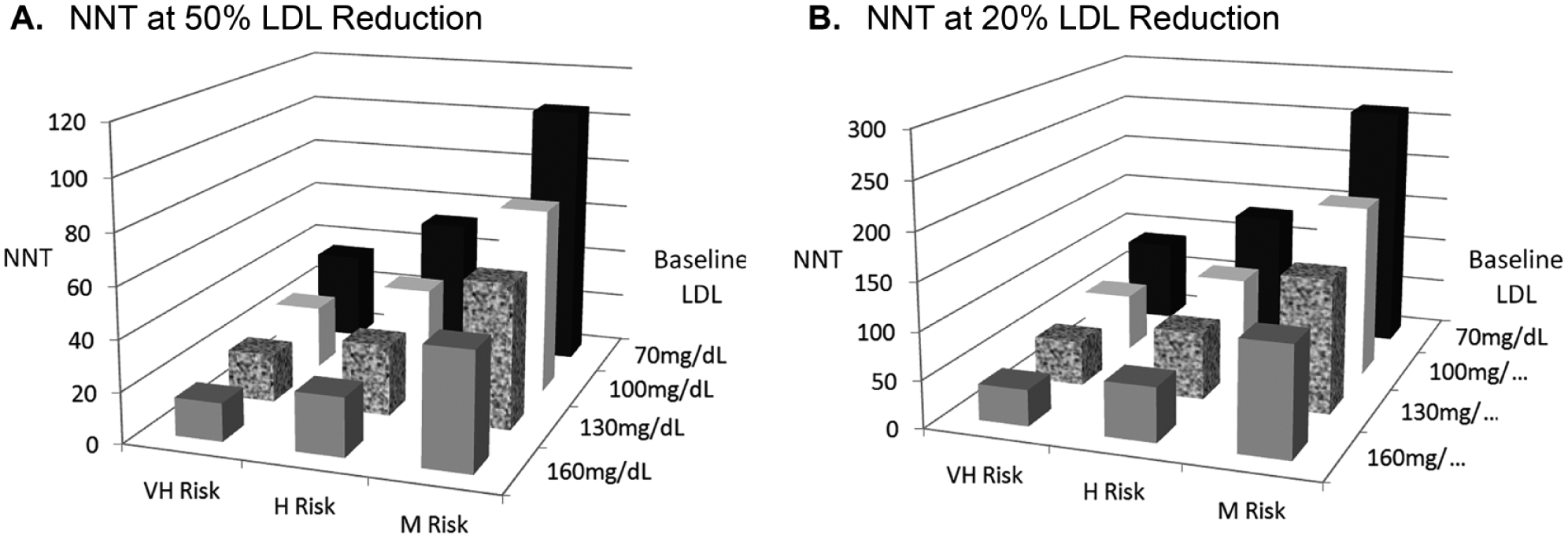
NNT for 5 years to prevent one cardiovascular event. 6
Should the target LDL levels from the ACC 2016 consensus document or the guidelines from the ESC/EAS 2016 or AACE/ACE 2017 be used? The LDL goals for very high and high risk patients with these documents are similar, and no data exist comparing the impact of the nuances from these recommendations on outcomes.3-5 The ACC 2016 recommendations are the flip side of the ESC/EAS 2016 guideline.3,5 The ESC/EAS guidelines incorporate LDL goals for patients who at baseline are further away from the target goal where the target is specified and for patients who start out near their goal where a flat 50% reduction from baseline is advocated. 3 The ACC 2016 recommendations give primacy to the percent reduction in LDL with a consideration for the ultimate LDL level achieved. 5 The ESC/EAS 2016 and ACC 2016 LDL goals of <70 mg/dL and <100 mg/dL for very high and high risk patients is achievable with evidence-based pharmacotherapy with reasonable NNTs.3,5 An advantage of the ACC 2016 recommendation would be that the ASCVD risk scoring tool includes all important cardiovascular events, not just fatal cardiovascular events, and is more commonly understood and used by clinicians in the United States.
The final question is what therapy should you preferentially choose? The choice is predicated on how much of a reduction is needed to achieve the LDL goal (Table 2). If a 20% LDL reduction will get a patient to goal, ezetimibe should be the preferred adjunctive therapy because it has evidence reducing final health outcomes, can achieve this level of LDL reduction, has a strong safety and tolerability profile, and is a much cheaper option than a PCSK9 inhibitor. 14 If a patient needs a 35% reduction to achieve their goal, things become more complicated. 8 Adjunctive ezetimibe plus bile acid sequestrant therapy can achieve the target LDL goal as can the use of a PCSK9 inhibitor.7,8 According to the CTT relationship between LDL and event reduction, ezetimibe plus bile acid sequestrant should yield similar event reductions as a PCSK9 inhibitor but at a much lower cost. 8 however, this adjunctive combination has not been evaluated in large clinical trials so the comparative and cost-effectiveness of this approach is unclear and adherence could be affected by the inconvenience of taking 2 drugs instead of one and the palatability of bile acid sequestrant therapy. Alternatively, the PCSK9 inhibitor would match or surpass this level of LDL reduction and has proven event reductions but at $14 000 per year is cost prohibitive. If a patient needs a ≥50% reduction to achieve their LDL goal, adjunctive PCSK9 inhibitors are the only options available but again can be cost prohibitive. 8
Recommended Adjunctive Therapies When Statins Do Not Achieve Goal a .
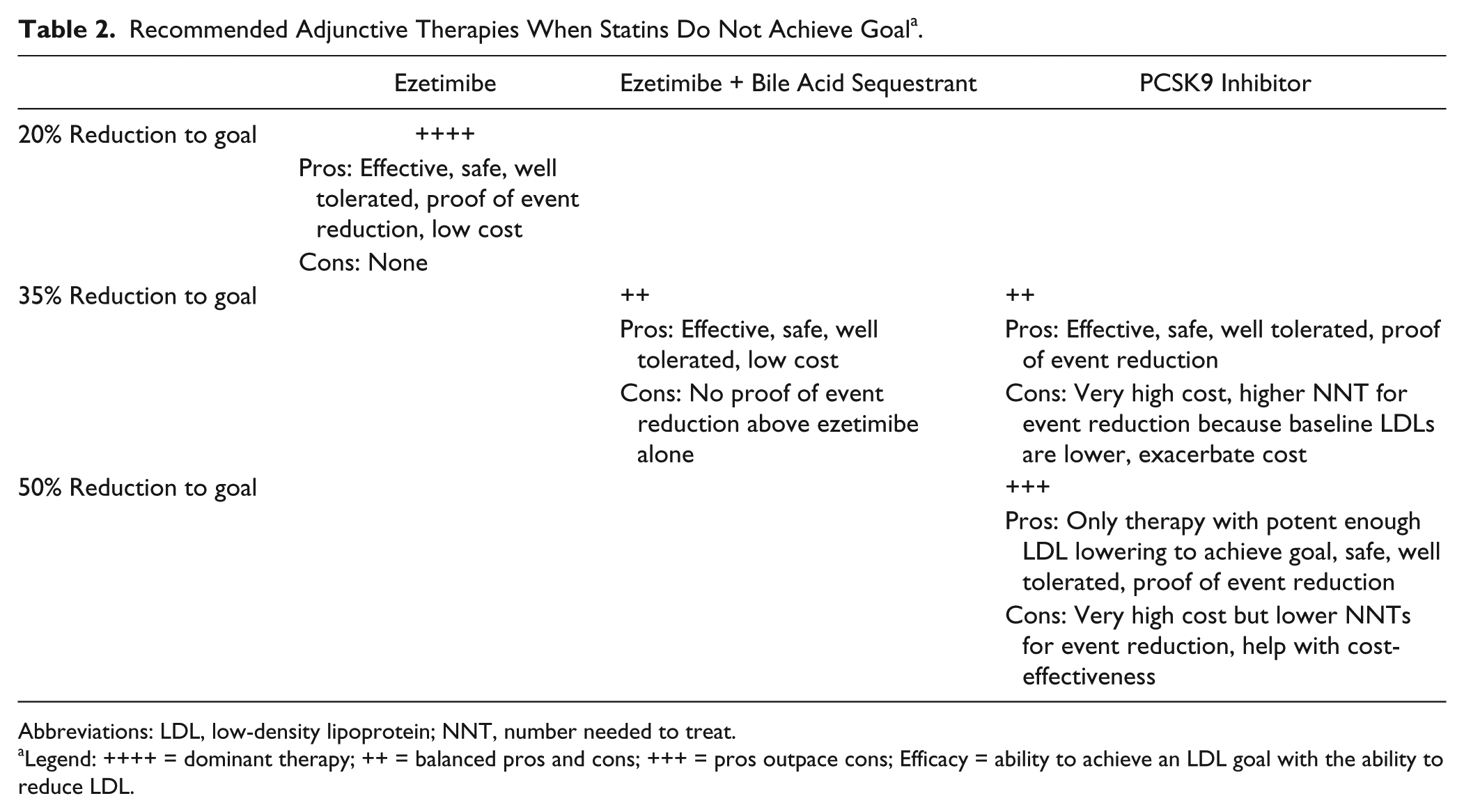
Abbreviations: LDL, low-density lipoprotein; NNT, number needed to treat.
Legend: ++++ = dominant therapy; ++ = balanced pros and cons; +++ = pros outpace cons; Efficacy = ability to achieve an LDL goal with the ability to reduce LDL.
In an analysis, the cost-effectiveness of the PCSK9 inhibitors was estimated and directly related to the NNT to reduce an event using the CTT relationship. 8 If the NNT on PCSK9 inhibitor therapy is 30 to 50, 15 to 29, or 10 to 14, therapy would cost ~$300 000, ~$280 000, or ~$150 000 per quality adjusted life year (QALY) at $14 000 per year. 8 The cost/QALY willingness to pay limit in the United States has not been firmly set but <$50 000/QALY, <$100 000/QALY, and <$150 000/QALY have been proposed as reasonable. Another important consideration is the level of discounting or rebating that a health plan negotiates. Using a NNT of ~25, a PCSK9 inhibitor discount of 50% is needed to achieve the $150 000/QALY level and a 77% reduction is needed to truly be considered cost-effective at $50 000/QALY. Assuming that a health plan is getting a 50% discount, the LDL reduction from baseline is 50%, and the NNT is 30 or less, PCSK9 inhibitor therapy will be <$150 000/QALY for very high risk patients with baseline LDLs ≥100 mg/dL and for high-risk patients with baseline LDLs >130 mg/dL but would be cost prohibitive in moderate-risk patients even at a baseline LDL of 190 mg/dL. 8
The Role of the Pharmacist in Achieving LDL Goals
Clinical pharmacists are valuable health care team members involved in performing patient assessments and evaluating medication therapy. 22 As such, they are integral in assessing patient compliance and statin intolerance as well as selecting appropriate adjunctive and alternative therapies. This process should include not only the available evidence and laboratory parameters but also patient preferences. Patients unable or unwilling to pay for a therapy, to take multiple medications, or tolerate a drug should factor in the drugs selected. Without this, patients will not have buy-in and adherence will suffer. With the tide turning back to LDL goal attainment, the pharmacist will continue to be a valuable health care team member in the care of these patients but their role may be expanded.
Previous studies have shown that ~70% of patients achieved their LDL goals under the NCEP ATP III guidelines. However, only a third of patients with coronary heart disease achieved an LDL goal of <70 mg/dL.23-26 Given the morbidity and mortality associated with cardiovascular disease, greater goal attainment, especially in high-risk individuals, is needed. Pharmacists have been shown to help achieve LDL goals through pharmacist-managed clinics, collaborative physician and pharmacist teams, and medication therapy management programs.
Pharmacist-managed clinics across different treatment settings and populations have been successful in increasing the number of patients reaching their LDL goals.27-36 For example, 2 analyses of pharmacy dyslipidemia programs versus usual care in Veterans Affairs (VA) medical centers showed that significantly more patients under pharmacist care achieve their LDL goals (study 1: 64.3% vs 15.7%, P < 0.001; study 2: 80.3% vs 65.3%, adjusted odds ratio = 2.6, 95% confidence interval [CI] = 1.6-4.3).27,28 Furthermore, the time to achieve LDL goal is significantly shorter in pharmacist-managed clinics (risk ratio = 1.8, 95% CI = 1.2-2.8). 28 Similar successes have also been seen in private health maintenance organizations and cardiology clinics as well as in disease-specific populations such as patients with diabetes or patients undergoing hemodialysis.29-32 The achievement of LDL goals through pharmacist-managed clinics has also been accompanied with provider and patient satisfaction as seen in a VA survey with 91.4% and 87.8% of patients and providers, respectively, reporting feeling strongly or somewhat satisfied with pharmacist-provided care. 33
Pharmacists can also help patients achieve their LDL goals through collaborative teams with physicians.37-40 In teams where the pharmacist and physician routinely meet to discuss patients’ cholesterol management, there are 2- to 4-fold increases in the percentage of patients reaching their goals versus teams without such collaboration (43% vs 21%, P < 0.05, and 72% vs 18%, P < 0.001).37,38 In patients with diabetes, pharmacists have also influenced LDL goal achievement rates through serving as physician extenders or remote team-based care with electronic communication.39,40
Lastly, pharmacist medication therapy management (MTM) programs can increase patients’ LDL goal attainment.41,42 For example, in a program where patients received education and long-term MTM services, the percentage of patients at goal LDL from baseline to end of follow-up increased from 49.9% to 74.6%. 41 In another study of Medicare Part D patients with diabetes, MTM was conducted via telephone and 69.0% of MTM participants achieved an LDL of less than 100 mg/dL versus 50.0% and 54.1% (P < 0.001) in control patients of eligible non-MTM participants and those not eligible due to Part D criteria, respectively. 42
Conclusion
Lipid guidelines had moved away from set LDL goals but are now coming back to embrace them. These moves were driven by clinical trials, and the latest guidelines from 2016 and 2017 reflect what clinicians should use in contemporary practice. Statins are safe and effective drugs that are the mainstay of initial therapy, but if patients achieve the maximum dose, or the maximum dose they can tolerate, and are not at their goals, adjunctive therapy with ezetimibe and PCSK9 inhibitors can further reduce cardiovascular events. If ezetimibe can bring patients needing a <20% LDL reduction to achieve their goal, it would be the dominant strategy given its cost-effectiveness. Pharmacists are poised to fill a niche with solid data affirming their ability to work collaboratively to help patients achieve their LDL goals.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.