
Abstract
Introduction
The population of the United States is growing and aging. The US population will grow by an estimated 12% to 359 million from 2015 to 2030. 1 The fastest growing population is aged ≥65 years, which is projected to grow by 55%. 1 This growth and aging of the population will increase the demand for health care services.
This is important given the critical deficiency of primary care physicians in the United States.2,3 The US health care system will face a shortage of physicians of 40 800 to 104 900 by 2030, so there is an opportunity to integrate community pharmacies across the United States in a team-based, physician-oversight model to deliver greater access and high-quality care.
Reasons for the shortage are multifactorial and appear to be protracted over the foreseeable future, requiring other professions to provide primary care healthcare services.4,5 Predictions are that there will also be insufficient nurse practitioners and physician assistants. 4 Thus delays in treatment can and will occur, significantly affecting patient care. Community pharmacies, by providing expanded primary care services, could help meet the 2 major goals of the Affordable Healthcare Act (ACA), expanding care to the insured and uninsured at a potential lower cost, with associated better health for communities.
Currently, 92% of Americans live within 1.6 miles of the 67 000 community pharmacies. 6 There are 13 billion annual visits or 530 to 570 visits daily to pharmacies. 7 For many of these visits, patients come to pharmacies seeking healthcare and drug advice and treatment for common illnesses, vaccinations, and wellness visits. To this end, community pharmacies offer point-of-care testing for infections, vital sign measurements, and medication management services to patients. If a greater access with high-quality care from an integrated team-based approach using the community pharmacy infrastructure is to be viable, 8 it is important to determine the demand for the provision of primary health care services among the pharmacists who maybe tasked with helping in making primary health care services available.
The aim of this study was to gain the perspectives of pharmacists by determining their preference for employment across community pharmacies that may offer differing levels and type of primary care services, and statically model the optimal health care services that would be of most interest to community pharmacists.
Methods
The study protocol and survey instrument were reviewed and approved as exempt following applicable guidelines involving the ethical treatment of human subjects by the University of Utah Institutional Review Board before the initiation of data collection. The University of Utah Institutional Review Board is fully accredited by the Human Research Protection Programs, Inc.
Study Design
The design of this study was a cross-sectional survey that included a Discrete Choice Experiment (DCE) conducted across the continental United States. DCEs are designed to show respondents competing scenarios that describe potential product or service offerings, and then requires they make a choice between the offerings.9-12 Rather than using respondents’ stated preference for features or services, DCEs approximate human experience decision making, whereby people make trade-off choices between offerings by taking all attributes into consideration simultaneously, and then the importance of features or attributes are derived through statistical analysis.
Sample
The sample comprised 312 pharmacists recruited from an established nationally representative panel of individuals who opted-in to be contacted for research purposes. This panel comprises over 2 million health care professionals worldwide, which includes 37 377 pharmacists practicing in the United States, 31 741 of who practice in a retail setting. Pharmacists accessed the survey electronically, through a link in an invitation e-mail, which offered a minimal honorarium for participation. Respondents were prescreened to meet the inclusion criteria: having either a baccalaureate or PharmD degree from an Accreditation Council for Pharmacy Education (ACPE)–accredited college or school of pharmacy in the United States, working at least 20 hours per week at no more than 2 separate community pharmacies, and who did not work in a closed-door, hospital or mail-order pharmacy. Between August 27, 2015 and September 21, 2015, the survey was opened to 1180 pharmacists. However, the survey was purposely capped, and the survey was closed at 312 respondents (26.4% of those eligible based on criteria above). This level of response is consistent with published data suggesting the rate of employment is approximately 15.3% of pharmacists meeting study exclusion criteria. 13 The data set was screened to remove those respondents giving nonsensical data, resulting in a final total of 291 surveys for analysis (93.3% of the 312). The demographic characteristics of the final pharmacist sample are presented in Table 1.
Attributes and Levels of Attributes Comprising Potential Pharmacy Configurations Shown to Pharmacists.
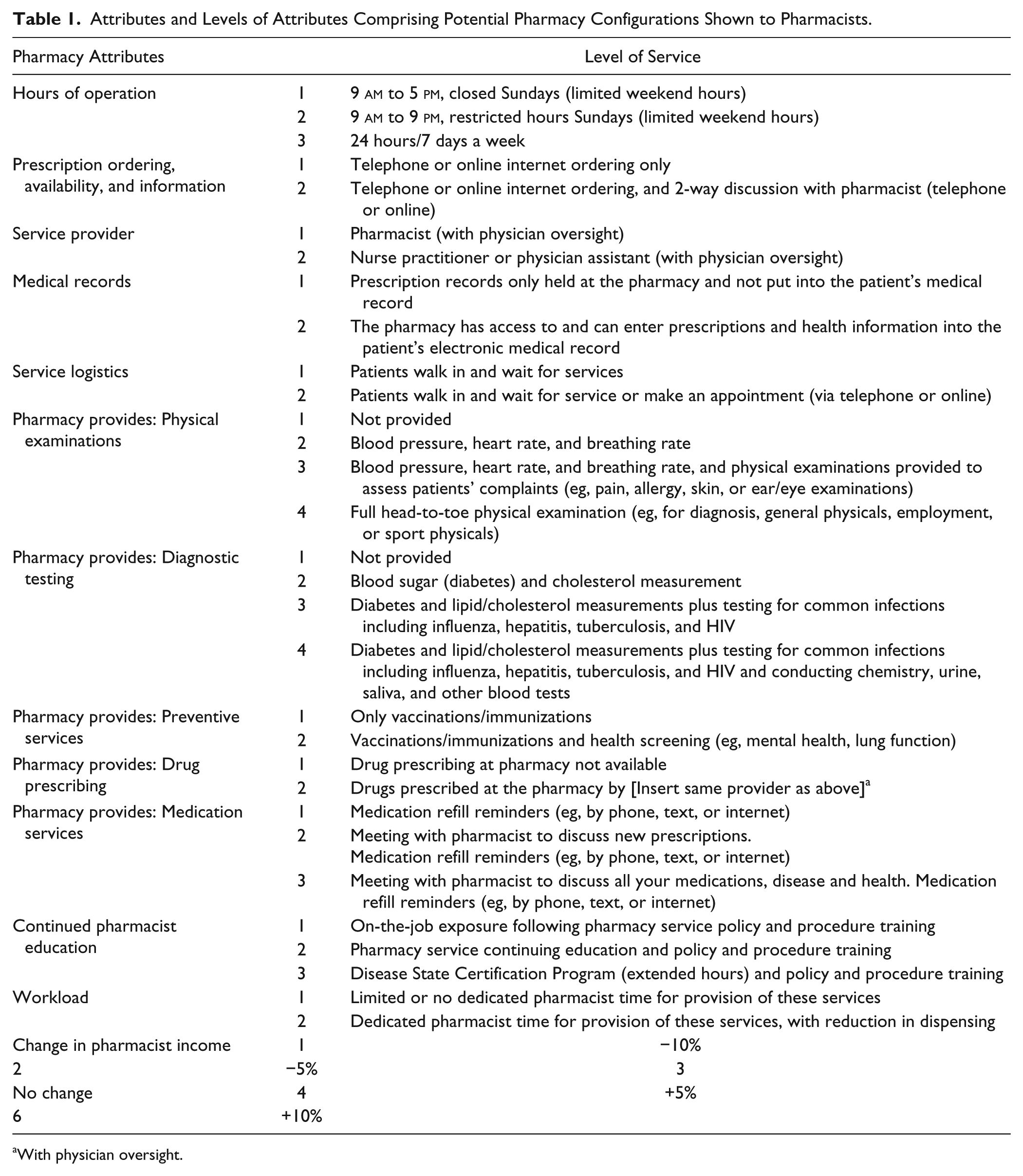
With physician oversight.
Questionnaire Design
The questionnaire was informed by prior qualitative interviews using an online bulletin board with 20 pharmacists, presented elsewhere.14,15 The quantitative survey took approximately 30 minutes to complete. Questions addressed occupational satisfaction, pharmacy services currently offered at location of employment, role in providing health care services at the pharmacy, attitudes toward pharmacies, and occupation and demographics. The DCE utilized a “dual response none” format, 16 so for each task, respondents were first asked to indicate which of three pharmacies displayed they would be most prefer to work in, and then were asked to rate how likely they would be to switch from working in their current pharmacy to working in the one selected on a 5-point scale (1 = not at all likely to 5 = extremely likely).
Discrete Choice Experiment
To design the pharmacist DCE, 13 attributes or features of potential pharmacies were developed and levels were assigned to each attribute (see Table 1), which when systematically varied, generated the future pharmacy configurations (276 480 possible combinations) (Figure 1). Each pharmacist respondent was provided an introduction to the DCE, which indicated that a private area would be provided for all point-of-care testing and physical examinations, with adequate support staff, and all providers would be suitably trained and approved to provide services by state and federal laws and regulations, with physician oversight. To compare preferences for the future “optimal care services” configuration, a “base” pharmacy was established that offered the minimal level of healthcare services. An experimental design for each pharmacist choice task was generated using Sawtooth Software’s Choice-Based Conjoint (CBC) design engine within their SSI Web programming framework (Sawtooth Software, Inc, Orem, UT). This resulted in 20 separate design versions of 14 tasks in 3 future pharmacy configurations for evaluation by each respondent, evaluated in the simulator.
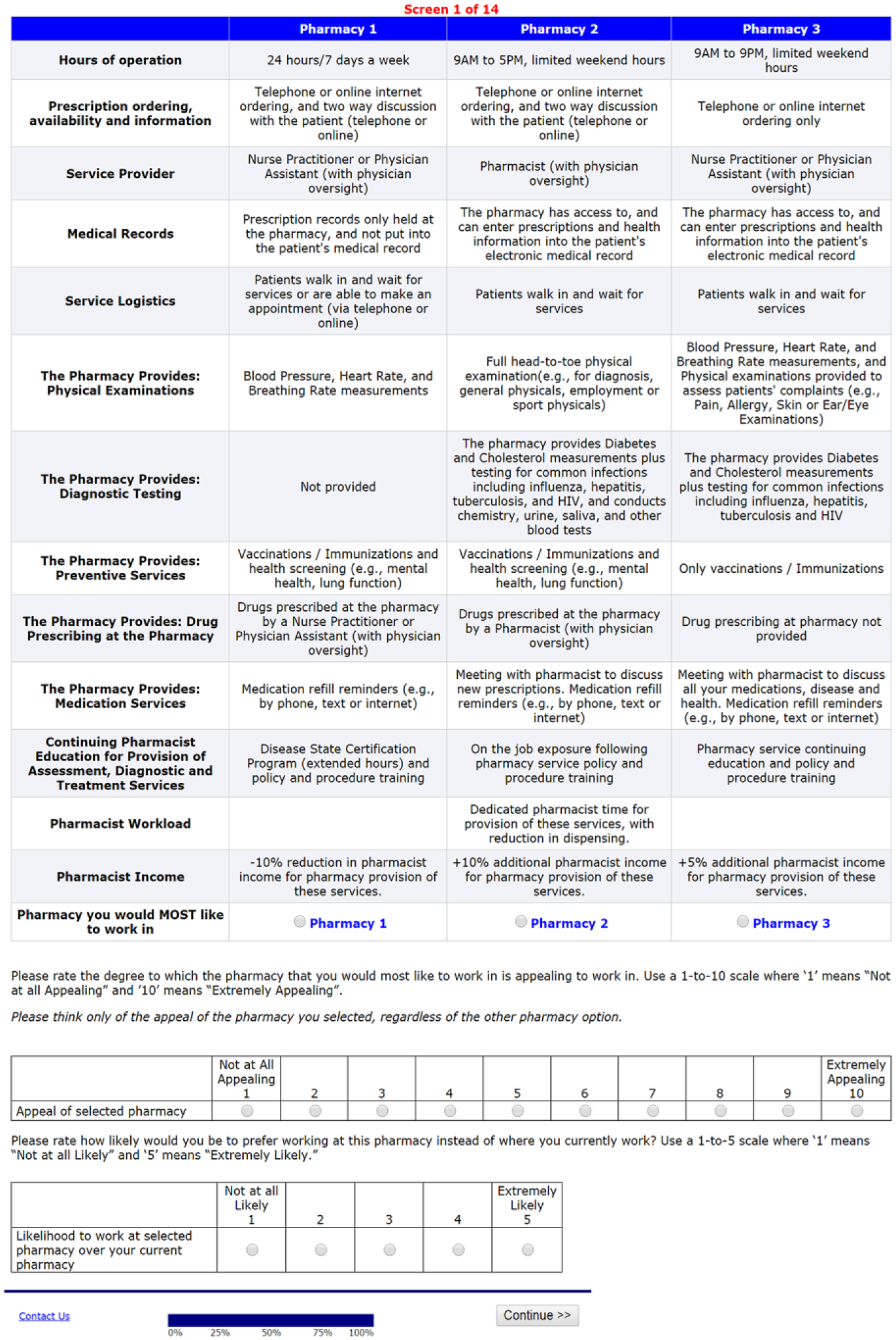
Pharmacist choice task example.
Discrete Choice Experiment Statistical Analysis
Customized hierarchical Bayes estimation software was used to estimate coefficients for the individual-level utilities of each attribute level. Prior to model estimation, the 5-point rating scale for likelihood to switch employment to the future pharmacy in place of pharmacist’s current pharmacy were recoded into a probabilistic scheme, whereby a 5 is recoded to 0.75, a 4 to 0.25, a 3 to 0.10, a 2 to 0.05, and 1 to 0.02. Thereby, a respondent who indicated that they would definitely switch (5) employment to a new pharmacy configuration has a likelihood of 75% for truly switching versus definitely would not switch (1) a 2% probability of switching. This conversion is commonly used to provide more realistic and conservative estimates of true switch likelihoods. 17
Individual-level point estimates (means) from the “results” iterations were imported into a simulator to predict choices pharmacists would make for any of the possible pharmacy configurations. The model estimated “switch rates” (the likelihood a respondent would switch from employment in their current pharmacy to the new one offering expanded services) at the individual level and then averaged to produce the final aggregate switch rates.
Bayesian precision intervals (BPIs) around each of the switch rates were computed empirically by running multiple simulations for a particular pharmacy configuration, taking random draws from the final saved iterations for each respondent; the results were saved and ranked, and the 95% precision interval was determined by examining the results for the 2.5th and 97.5th percentiles among the set of ranked predictions. Significance was set at a P value of <0.05.
Results
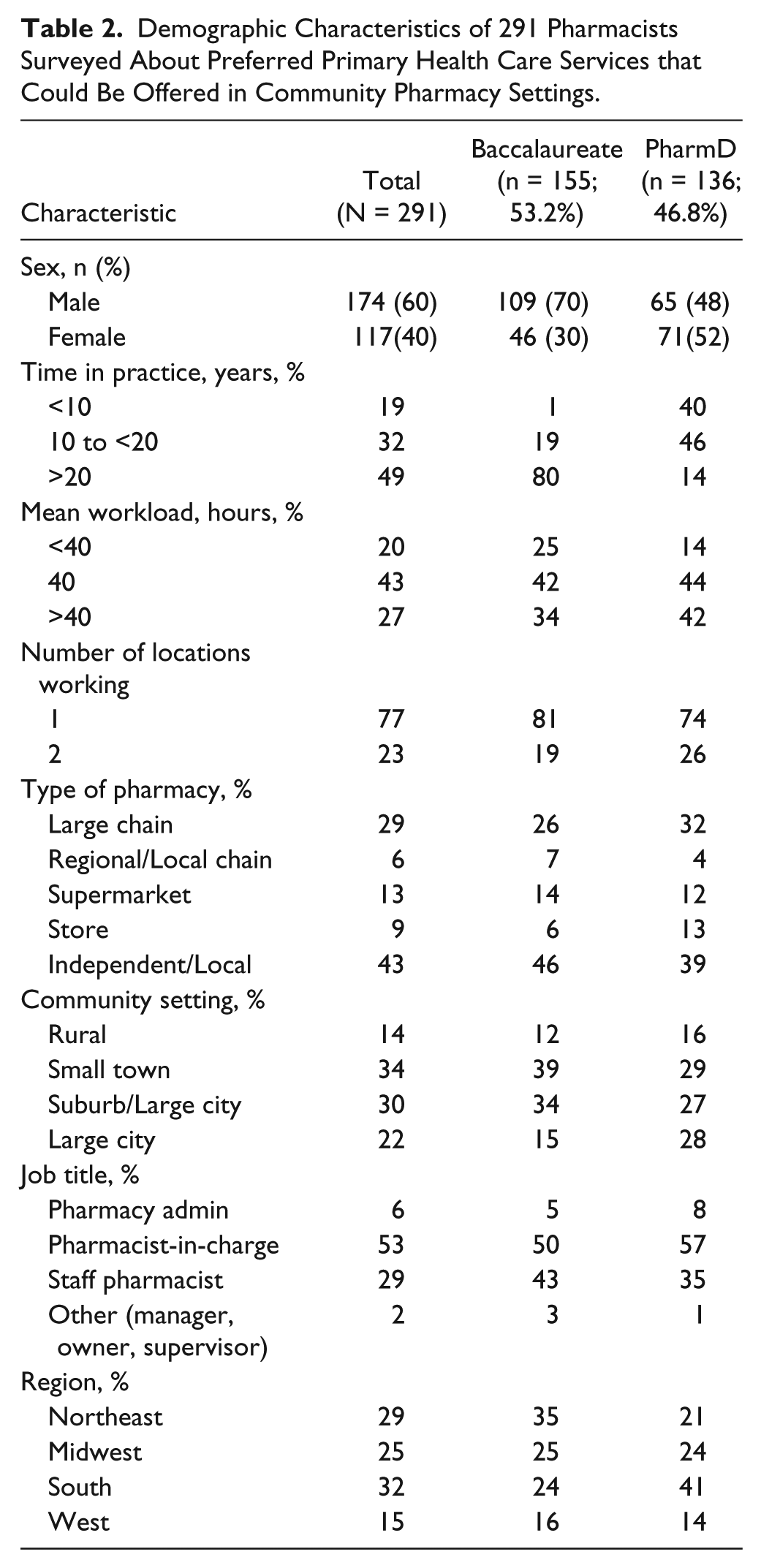
Pharmacists participating in the study were principally male, slightly more holding a baccalaureate degree, having practiced for >20 years, and were practicing more frequently in small towns and suburbs of large cities (Table 2). Most were in positions of pharmacist-in-charge or staff positions. The pharmacist’s occupational activities were primarily filling prescriptions (50.4%), counseling on prescriptions (11.1%), handling claims (9.7%), participating in managerial activities (7.9%), counseling on over-the-counter medications (6.1%), health and wellness (6.1%), or administering vaccinations (4.4%). Clinical activities such as taking vital signs, medication therapy management counseling, prescribing medications, conducting point-of-care laboratory testing, health screenings, or physical examinations were all being conducted at ≤ 1% of time. Reimbursement for these services was highest for medication therapy management counseling at approximately 12% to 14%, whether insured or uninsured, with most patients paying out-of-pocket expenses of $15 to $30.
Demographic Characteristics of 291 Pharmacists Surveyed About Preferred Primary Health Care Services that Could Be Offered in Community Pharmacy Settings.
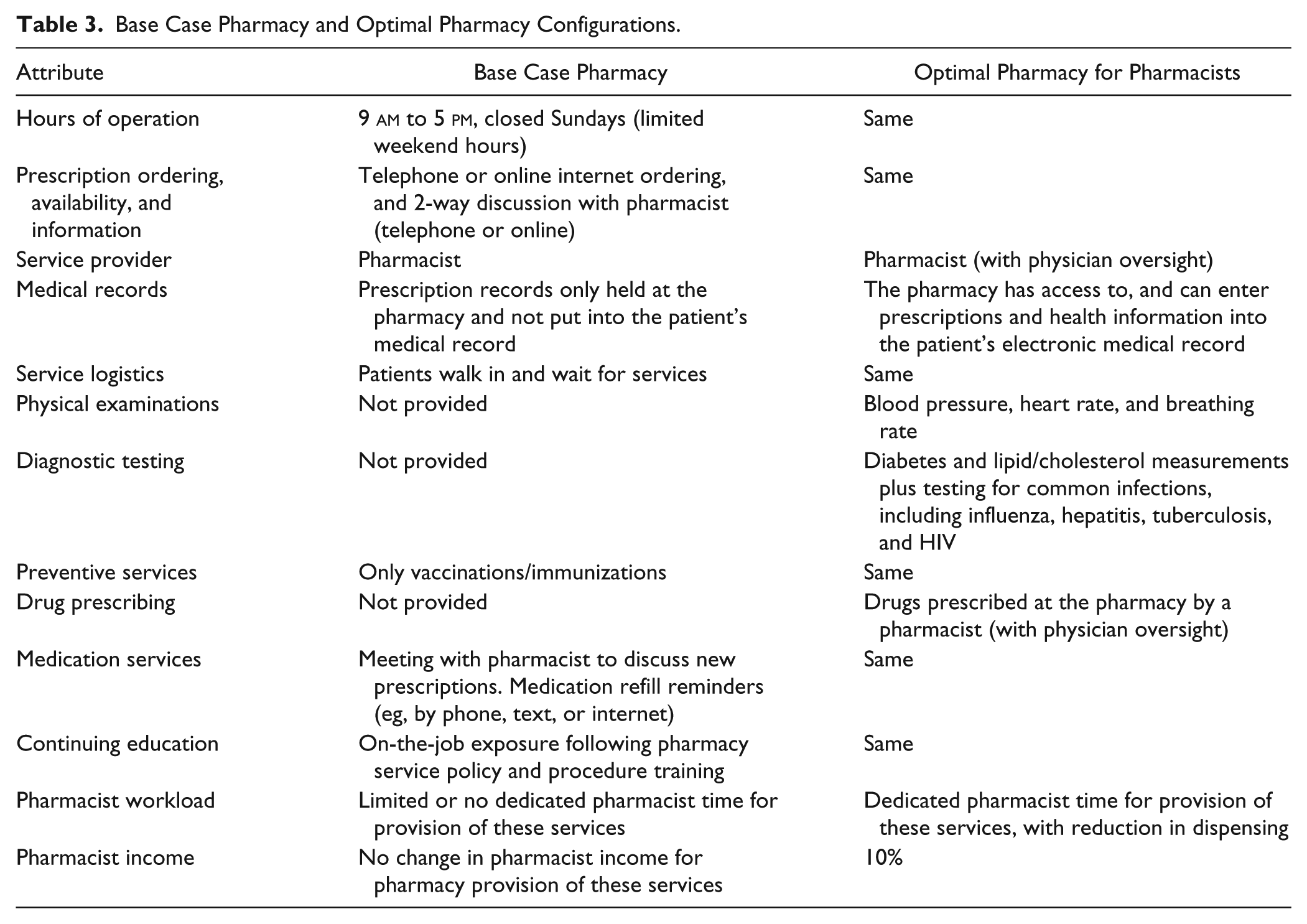
Optimal care services for pharmacists to be delivered at a community pharmacy setting were determined through statistical modeling in the simulator, giving the combination of attributes that would maximize the probability that pharmacists would switch employment from their current pharmacy to one offering different set of patient care services (Table 3). These services included vital sign measurements, point-of-care laboratory testing for cholesterol and glucose, providing immunizations, and medication prescribing. Pharmacists were ≥4 times likely to switch employment to this pharmacy (switch rate of 20.3%; 95% BPI = 15.4%-24.7%) than to the base pharmacy not offering these services (switch rate of 4.9%; 95% BPI = 3.0%-7.3%).
Base Case Pharmacy and Optimal Pharmacy Configurations.
The demand for switching to the pharmacy offering optimal services was higher for: those with a PharmD (22.7%, 95% BPI = 16.6%-27.6%) as compared with baccalaureate pharmacists (18.3%, 95% BPI = 13.5%-22.7%); those with less than 20 years’ experience (22.4%, 95% BPI = 16.3%-27.4%) versus those with more than 20 years’ experience (18.1%, 95% BPI = 14.2%-22.3%); those working more than 40 hours per week (22.3%, 95% BPI = 17.4%-27.9%) compared with those working 40 hours per week (18.5%, 95% BPI = 13.9%-23.2%), or part time less than 40 hours per week (19.5%, 95% BPI = 12.1%-25.0). Demand was highest for those working in rural communities (22.6%, 95% BPI = 14.6%-29.6%) versus nonrural settings (20.0%, 95% BPI = 14.8%-24.6%). The switch rate was independent of pharmacist gender. When comparing regions of the country, all were equivalent with the exception of the Midwest with a slightly lower switch rate.
The optimal pharmacy for pharmacists included the attribute of having designated pharmacist time for the provision of primary health care services, and a maximal salary increase of 10% (20.3%, 95% BPI = 15.4%-24.7%). Nonetheless, a high rate of switching was still seen at a 5% salary increase (14.4%, 95% BPI = 10.1%-18.8%).
The survey contained a list of questions related to pharmacist attitudes associated with provision of greater clinical activities to patients. Pharmacists are willing to complete more education if it meant that they would receive more compensation (74% affirmative), feel that consumers would trust them to prescribe medications (69% affirmative), monitor patients’ healthcare information through multiple information technology mediums (44% affirmative), and to deliver a wider range of health care services (57% affirmative). Pharmacists also want more time to spend with consumers (61% affirmative). However, pharmacist showed concerns including, time to complete these additional services (56% affirmative) and personnel liability (55% affirmative).
Discussion
This discrete choice study shows that pharmacists are genuinely positive about increasing primary care services in community pharmacies, those with a PharmD, and those in rural settings. These advanced service results were principally driven through offering vital signs (blood pressure, heart rate, and breathing rate), point-of-care testing (blood sugar and cholesterol measurement), and having the pharmacists prescribe medications (under physician oversight).
The optimal service delivery model for pharmacists did not include more advanced patient contact services such as offering complete, employment, or sport physical examinations or diagnostic testing including chemistry, urine, saliva, and other blood tests. This is despite physical examination training being an ACPE accreditation requirement of all pharmacy graduates for a number of years, 18 and studies showing that pharmacists want to develop and sustain patient care services,19,20 and pharmacist demonstrated improved outcomes when compared directly to physician-driven standard of care.21-25 However, these results are consistent with the observation that the profession is changing over time. Early studies showed that pharmacists were closely aligned with product services. 26 In 2010, a DCE study showed pharmacists would provide medication management services as long as job security and satisfaction were preserved. 27 Our results support an even greater move to providing primary care services through vital sign measurements, diagnostic testing, and vaccinations at the community pharmacy setting with dedicated time and a modest income increase. Furthermore, pharmacists believe that consumers will trust the care they deliver, 14 but understand that additional training and increased liability may come with this change in practice. Pharmacists are well positioned to be providers of primary care. 28
Pharmacists have the education and training in basic pathophysiology, physical assessment, basic and complex diagnostic testing, pharmacotherapy, diagnosis of ailments requiring over-the-counter medications, information technology systems, and wellness services, making them valuable to primary care. Collaborative practice agreements (CPAs) are in place in 47 of 50 states, although limitations of CPAs exist in many states. 29 Pharmacists can legally immunize adults and/or children in all states. 30 Pharmacists are well trained to provide chronic care management—including disease state patient education and associated medication non-adherence and preventative care counseling. Moreover, projected graduation rates of pharmacists in 2015-2016 appear to be sufficient to fill the projected 9% fall in primary care clinicians by 2020, but there we remain a critical need for primary care physician oversight of pharmacists.31,32
Another potential advantage of a primary care community pharmacy model is the potential to lower health care costs by retrofitting primary care delivery systems into existing community pharmacies as opposed to building centralized community clinics. The result could be lower costs to patients, greater access to healthcare personnel, an improved team-based delivery of care, and greater continuity of care through incorporation of the pharmacy records into the patient’s medical record and greater communication lines with physicians. This model is not in contrast to the patient-centered medical home and can in fact be built into that model.33-35 Future integrative research should focus on how community pharmacies could be incorporated into the existing medical home model.
Limitations of this study are its descriptive nature. DCEs are approximates of real-world decision making, the design cannot equate to actual experience of pharmacist providing primary care services in the pharmacy setting. Furthermore, the exercise is futuristic and assumes 100% awareness and availability of all possible advanced service options. Therefore, the results may accentuate demand. The application of these results should be assessed in the context of the study population that was principally male, a higher ratio of baccalaureate to doctorate-level training, and working more than 20 hours per week.
Conclusion
This pharmacist DCE study provides empirical support for the provision of primary care services through a community pharmacy setting. The main focus of primary care is the diagnosis and treatment of patients. The profession will need to consider how best to embrace and even champion innovation within community pharmacy practice to deliver primary care.
Footnotes
Acknowledgements
The authors extend their appreciation to Greg Jones, PharmD, Jaime Montuoro, PharmD, Paige Patterick, BS, RPh, and the faculty of the Department of Pharmacotherapy for their input into the selection of attributes for inclusion in this study.
Authors’ Note
Part of this study were presented at the American Pharmacists Association Annual Meeting and Exposition, San Francisco, CA, March 2017 (JAPhA May, 2017 scheduled publication) under the title “Patient, Pharmacist and Payer Preferences for Healthcare Delivery through Community Pharmacy: OPTiPharm Study.” The study sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Skaggs Institute for Research, and Skaggs Foundation for Research.