
Abstract
Background
Enoxaparin is a low-molecular-weight heparin commonly used for the treatment and prophylaxis of thromboembolism in pediatric patients.1-11 Despite widespread use, pharmacokinetic data to give dosing guidance in pediatrics is sparse. The dosing of enoxaparin in pediatrics has been extrapolated from adult data and subsequently refined through clinical experience. Retrospective reviews of enoxaparin use in pediatric patients have been published and give guidance for dosing and monitoring but are often limited by their inability to incorporate significant patient covariates into their analyses, such as kidney function.1,2,4,12,13 A population pharmacokinetic analysis of enoxaparin in pediatric patients has been published in patients receiving secondary prophylaxis, but it focused on the outpatient setting and focused on body weight as a clinical covariate. 14
The current suggestions for dosing enoxaparin for treatment of thromboembolism are variable. Guidelines, publications, and dosing handbooks typically suggest a dose of 1 mg/kg/dose subcutaneously every 12 hours to treat thromboembolism and to attain an anti–factor Xa concentration of 0.5 to 1 U/mL at 4 hours after a dose in a pediatric patient greater than 2 months of age but also often list alternative dosing strategies, such as those based on age.2,4,15 -18
We aim to characterize the pharmacokinetic profile of enoxaparin in pediatric patients to improve empirical treatment dosing in hospitalized patients. We also aim to identify relevant covariates that may alter the pharmacokinetics of enoxaparin in the pediatric population.
Methods
A retrospective cohort study design was chosen, and institutional review board approval from Baylor College of Medicine and Affiliated Institutions was obtained. Patients who received subcutaneous enoxaparin for any indication were identified by querying the Texas Children’s Hospital pharmacy database from January 1, 2011, through June 30, 2016. Patients were included if they met the following criteria: were 1 to 18 years of age at initiation of subcutaneous enoxaparin therapy for treatment or prophylaxis of thromboembolism, were inpatients during the study period, and had anti–factor Xa activity levels measured. Patients were excluded if they were undergoing mechanical circulatory support or renal replacement therapy during enoxaparin therapy.
Data collected included the following: patient age, gender, height, weight, enoxaparin doses, anti–factor Xa activity levels, serum albumin, serum creatinine (SCr), hemoglobin, hematocrit, and platelet count. Hemoglobin and hematocrit were chosen as covariates because they could be markers for alterations in volume of distribution (VD). Enoxaparin has activity on platelet binding, and alterations in platelets could affect pharmacokinetic parameters. Data collection, and subsequent use as covariates, were based on review of pertinent literature and current dosing guidelines. 15 Patient location (intensive care unit or acute care floor) was also noted. Creatinine clearance was calculated according to the Schwartz equation. 19
Anti–factor Xa activity levels were measured on the STA-R analyzer using the STA—LIQUID ANTI-Xa kit (Diagnostica Stago, Asnieres, France). This assay measures the anti–factor Xa activity in a competitive system using a synthetic chromogenic substrate in plasma. The coefficient of variation for the test was 3.2%, with a lower limit of detection of 0.1 U/mL. All anti–factor Xa levels were collected as 2.7 mL of blood in a light blue sodium citrate tube. A 1:1 ratio of enoxaparin to anti–factor Xa was used based on prior publications. 14
Descriptive Analysis
The patient population was described using percentages, means, SDs, medians, and ranges, for normally and nonnormally distributed data, as appropriate. Graphical representation of the initial data was also utilized. Statistical analyses were performed using Stata IC v.12 (StataCorp, College Station, TX) and Excel 2013 (Microsoft Corp, Redmond, WA).
Pharmacokinetic Analysis
Population pharmacokinetic analysis was performed with NONMEM v.7.2 (Icon, PLC, Dublin, Ireland) and PDx-Pop 5.1 (Icon, PLC, Dublin, Ireland) using first-order conditional estimation with interaction.
The base model was developed by evaluating anti–factor Xa levels versus time after dose (Figure 1). One- and 2-compartment models, along with additive, proportional, exponential, and combined proportional/additive error models, were used and evaluated. Prior values for θ (estimates of pharmacokinetic parameters) were developed from a review of pertinent literature. Interindividual variability was modeled exponentially. Allometrically scaled weight, with an exponent of 0.75 on clearance (CL) and 1 on VD, was added to the base model with a reference value of 70 kg. 20 This served as the model for further covariate analysis.
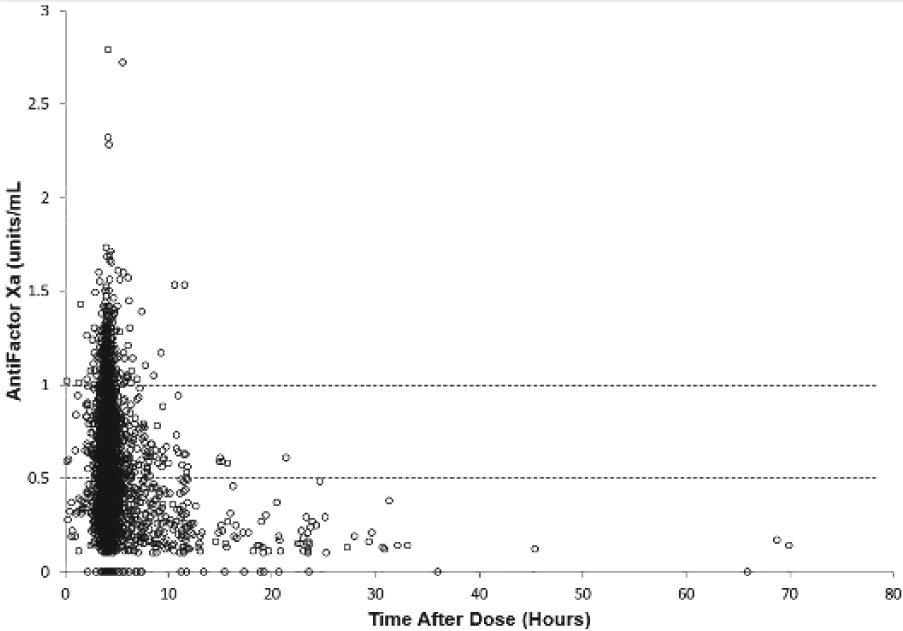
Anti–factor Xa concentrations (U/mL) versus time after dose (hours).
Initial covariate analysis occurred by plotting empirical estimates of pharmacokinetic parameters against clinically or pharmacologically relevant covariates and visually identifying potential relationships prior to using linear, linear proportional, and power models normalized to the population median. Categorical covariates were modeled exponentially.
A reduction of the objective function value (OFV) by >3.84 was considered to be statistically significant (P < 0.05) on addition of a covariate. A full model was developed, then covariates were retained if during a stepwise backward elimination an increase of OFV from the full model of at least 10.83 (P < 0.001) occurred. 21 Scatter plots of dependent variables versus individual predicted (IPRE) anti-Xa levels, as well as predicted versus conditional weighted residuals were created to evaluate model goodness of fit and detect bias. Bootstrap simulations were performed (n = 1000) on the final model with calculation of 95% CIs. A simulation was run (n = 10 000) on the final model on virtual patients, developed from median values of covariates. Different doses, from 0.5 to 1.5 mg/kg/dose every 12 hours, were evaluated to identify mean anti–factor Xa activity levels and the percentage of time the dose would result in a 4-hour postdose anti–factor Xa level of 0.5 to 1.0 U/mL in patients who had an estimated creatinine clearance of >30 mL/min/m2 and for patients with reduced creatinine clearance (≤30 mL/min/m2) based on current recommended dosing guidelines for adult patients. 15
Results
Descriptive Analysis
A total of 853 patients (2652 anti–factor Xa activity level measurements) met study criteria and received a mean enoxaparin dose of 0.86 ± 0.31 mg/kg/dose for a median of 12 doses (interquartile range [IQR] = 6-28). All patients received enoxaparin subcutaneously at a concentration of 100 mg/mL. A median of 3 (IQR = 1-5) anti–factor Xa levels were sampled at a mean of 4.4 ± 1.3 hours after a dose. The mean anti–factor Xa level was 0.52 ± 0.23 U/mL, and 1.3% of the anti–factor Xa levels were below the detectable limit of the assay. Because so few of the anti–factor Xa samples were below the assay limit, they were treated as zero (Figure 1). Patients were located in the intensive care unit for 18.3% of the doses administered. Other demographic and laboratory data are summarized in Table 1.
Demographic Variables.
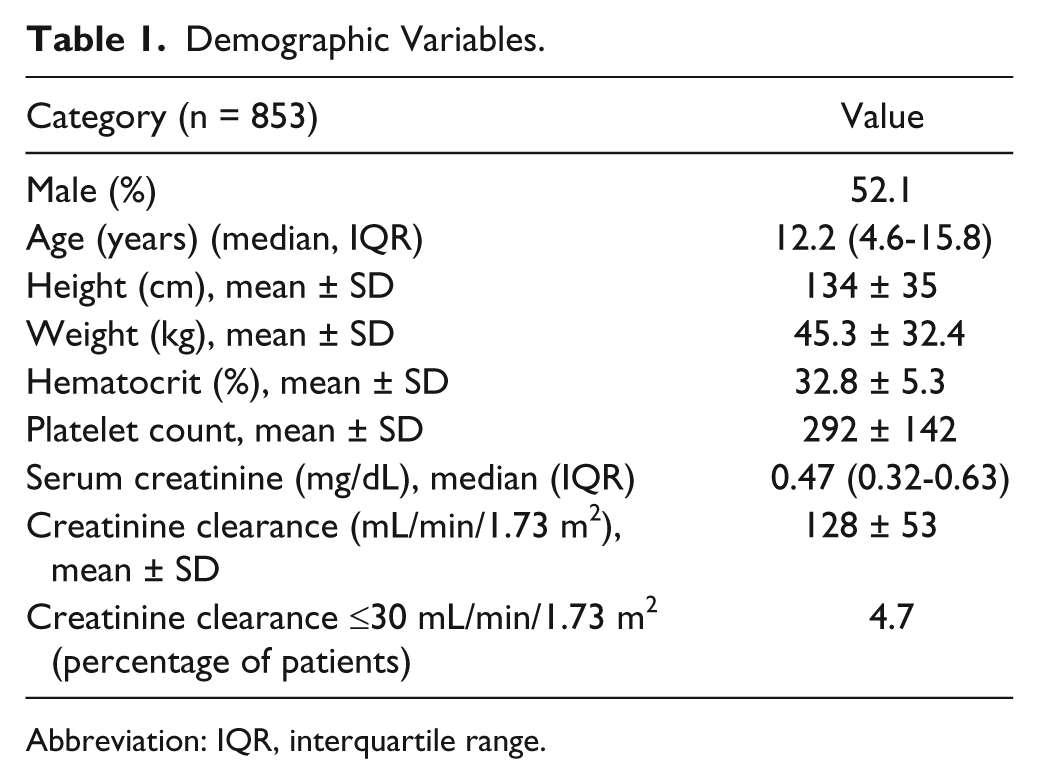
Abbreviation: IQR, interquartile range.
Pharmacokinetic Analysis
A 1-compartment proportional and additive error model with interindividual variability modeled on CL and VD best fit the data. Initial covariate analysis included significant relationships between gender, SCr, platelets, and hematocrit on CL. Intensive care unit location did not result in a significant reduction in OFV (−3.158). Age demonstrated a mild trend in CL when graphically evaluated but did not result in significant reductions in OFV (Figure 2). SCr was noted to be inversely related to CL (mL/kg/h; Figure 3). Covariates significantly affecting VD included age, hematocrit, and platelet count. As the full model was being assembled, it was noted that the hematocrit had a greater reduction in OFV as a covariate on CL as compared with VD (−67.739 vs −21.926) and that platelets had a greater reduction in OFV when placed as a covariate on VD as compared with CL (−32.156 vs −26.768). Subsequently, the full model used hematocrit on CL and platelets on VD. After backward elimination, allometrically scaled weight, SCr, hematocrit, and platelets were included in the final model (Table 2). Diagnostic graphs were completed and demonstrated a good model fit (Figures 4 and 5). Bootstrap analysis with 1000 runs was completed (Table 3).
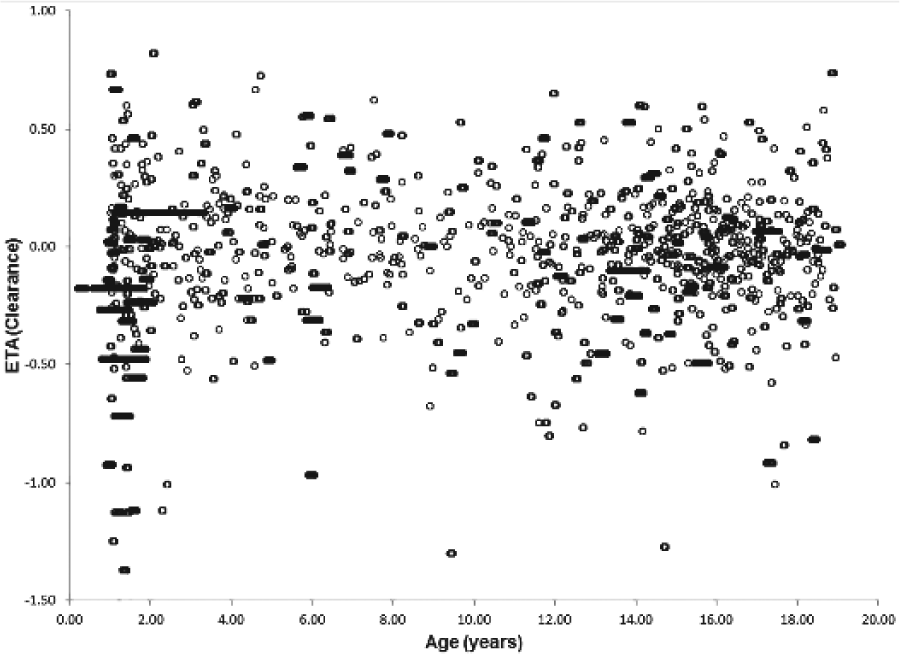
Age (years) versus ETA (clearance).
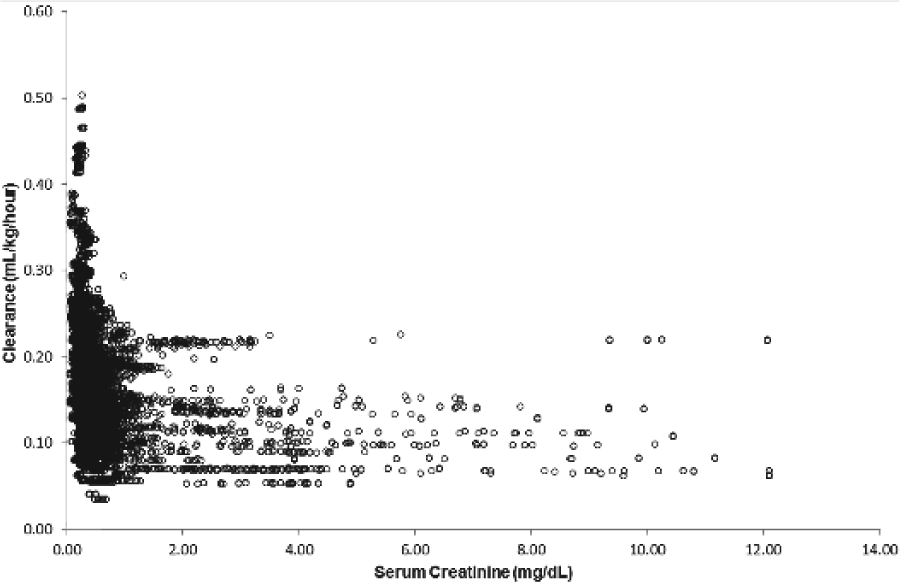
Serum creatinine (mg/dL) versus clearance (mL/kg/h).
Final Model.
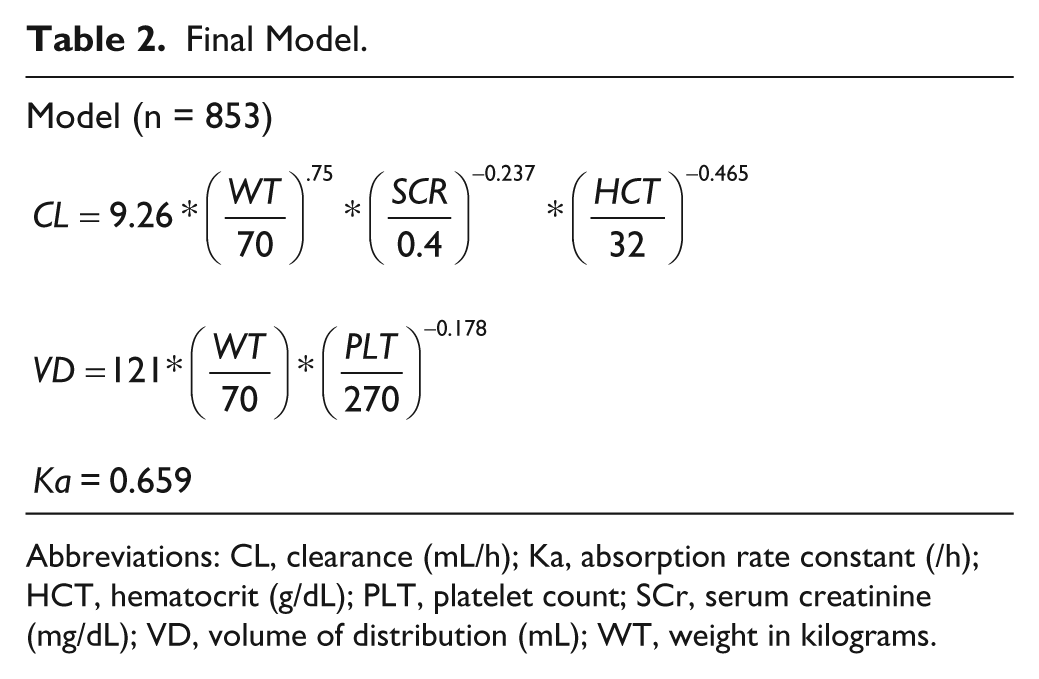
Abbreviations: CL, clearance (mL/h); Ka, absorption rate constant (/h); HCT, hematocrit (g/dL); PLT, platelet count; SCr, serum creatinine (mg/dL); VD, volume of distribution (mL); WT, weight in kilograms.
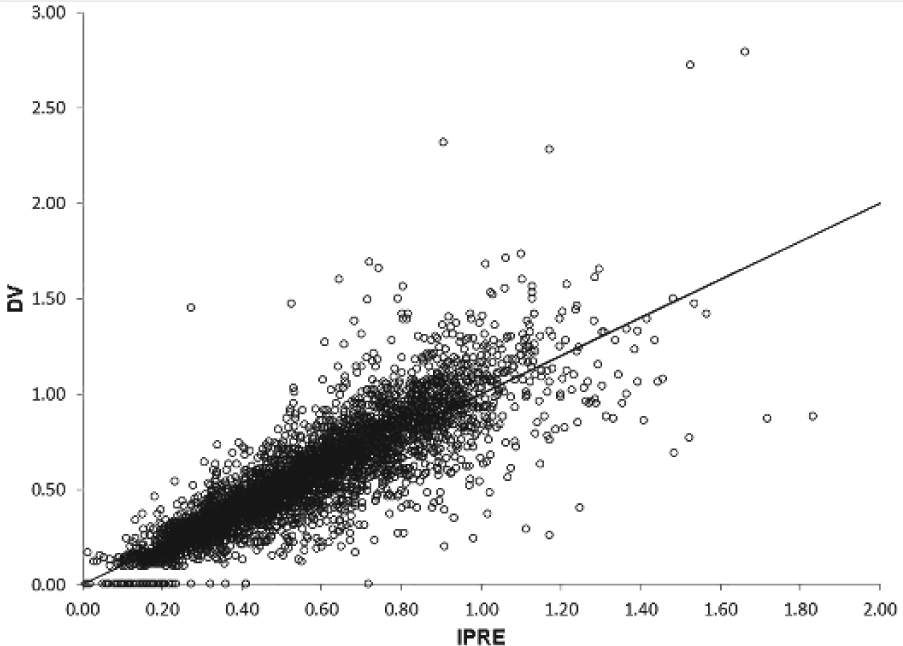
Anti–factor Xa concentrations (dependent variables [DVs]) versus individual predicted concentrations (IPRE).
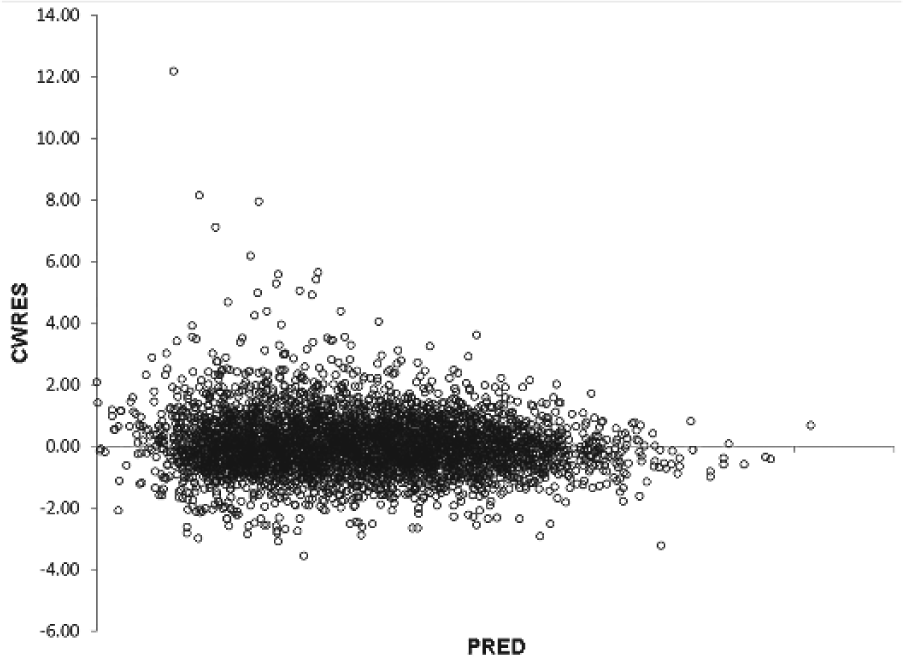
Conditional weighted residuals (CWRES) versus predicted concentrations (PRED).
Bootstrap Analysis.
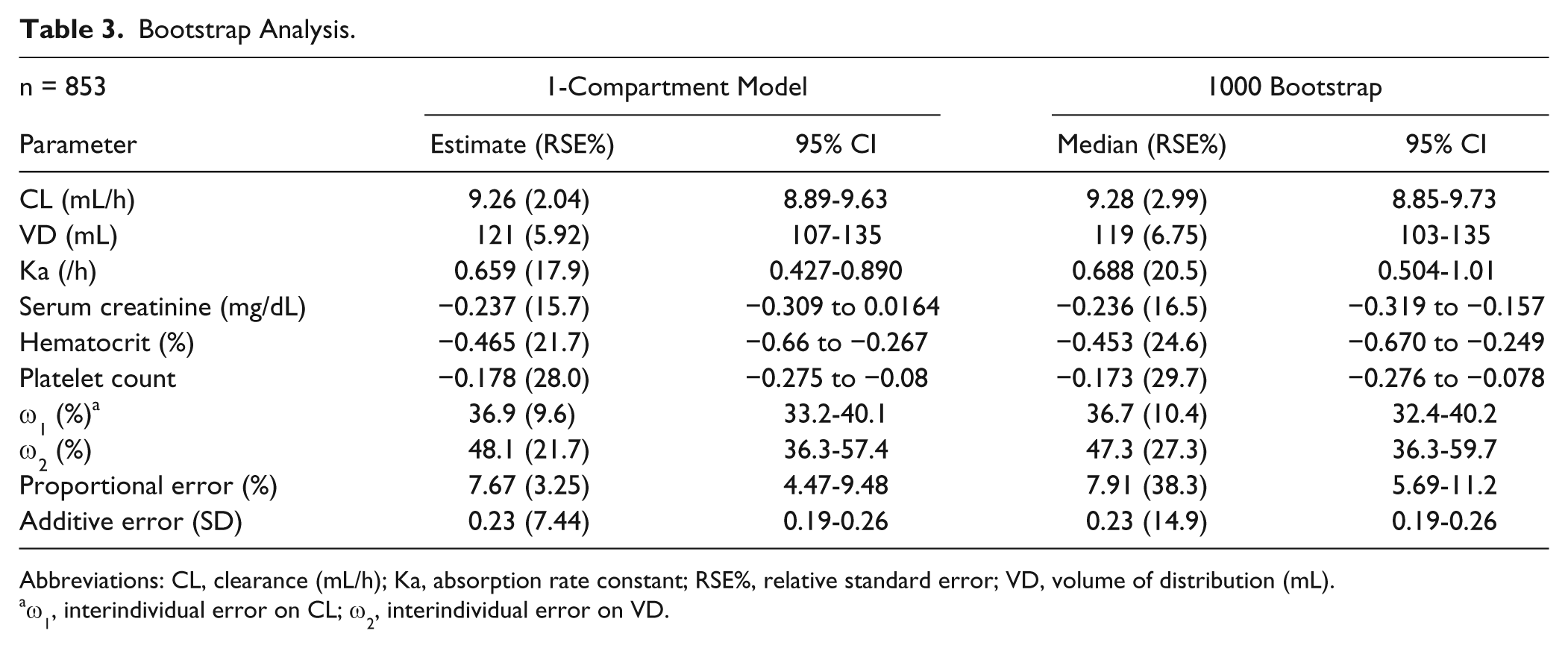
Abbreviations: CL, clearance (mL/h); Ka, absorption rate constant; RSE%, relative standard error; VD, volume of distribution (mL).
ω1, interindividual error on CL; ω2, interindividual error on VD.
A simulation data set evaluating different dosing regimens demonstrated that many patients would achieve a therapeutic anti–factor Xa level at 4 hours after administration with 1 mg/kg/dose every 12 hours. For patients with an estimated creatinine clearance of ≤30 mL/min/1.73 m2, reducing the dose by approximately 30% led to anti-Xa levels in the target range (Table 4).
Simulation Data Set. a
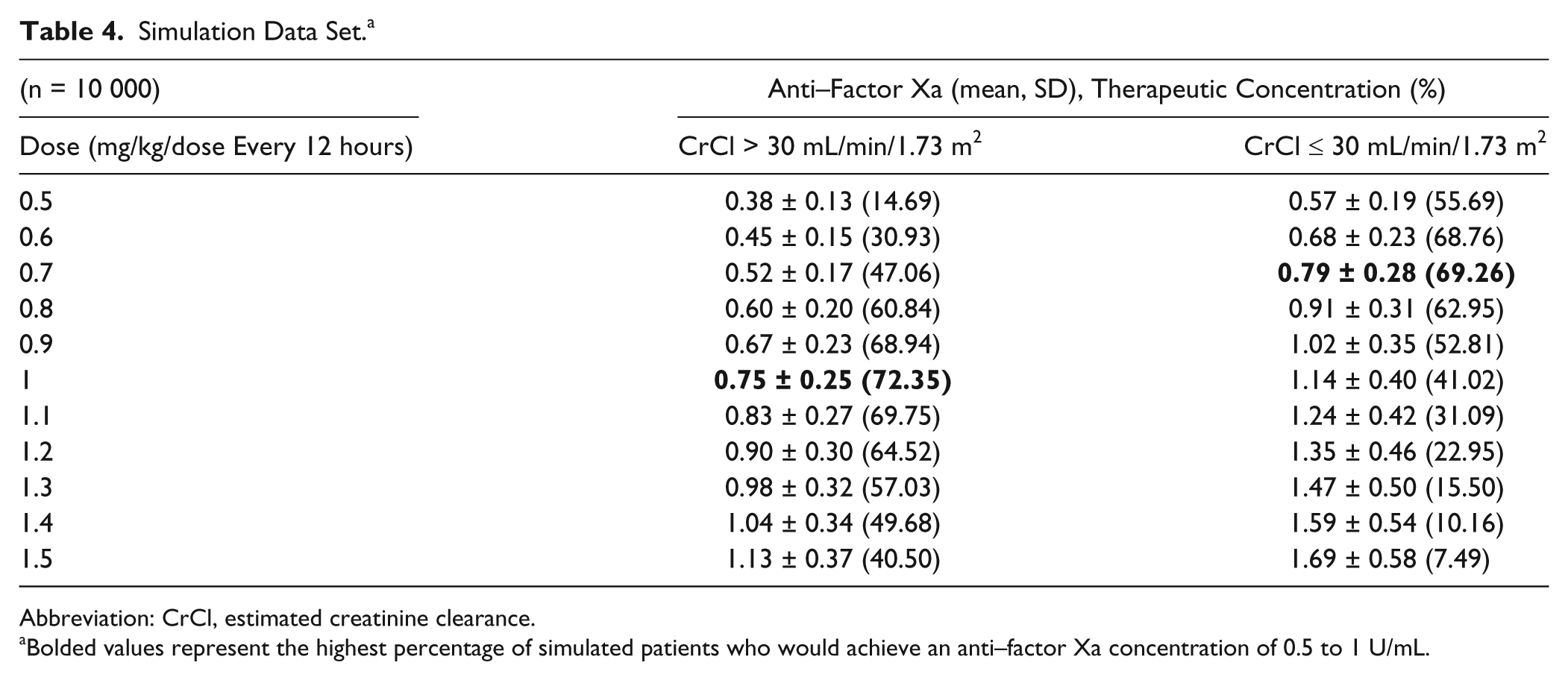
Abbreviation: CrCl, estimated creatinine clearance.
Bolded values represent the highest percentage of simulated patients who would achieve an anti–factor Xa concentration of 0.5 to 1 U/mL.
Discussion
This is the first population pharmacokinetic analysis of exclusively pediatric inpatients receiving enoxaparin therapy and the largest such study of pediatric patients receiving enoxaparin. The values for CL and VD are similar to those in other published models. Trame et al 14 reported a CL of 15.2 mL/kg/min, which is slightly higher than the value from our data set, calculated at 9.7 mL/kg/min. 14 This is likely because of the fact that our population was inpatient, compared with outpatients in the study by Trame, and CL could have been reduced because of patient comorbidities. These values are similar to the values reported in adults of 15 mL/min. 15 The estimate for VD in our population was 121 mL, which was also slightly lower than other reported values in the Trame study (169 mL). 14 All these values are much larger than what has been described in adult patients—61.4 mL—when adjusting for a 70-kg patient. 15
We chose to use a pharmacokinetic model, as opposed to a pharmacodynamic model, based on prior publications and to improve the clinical utility and relevance of a model.14,22 The end point of anti–factor Xa is a concentration (U/mL), which lends itself to pharmacokinetic analysis. The data presented validate empirical enoxaparin treatment dosing schemes for pediatric patients. Based on our model, a dose of 1 mg/kg/dose subcutaneously every 12 hours for patients with normal kidney function has the highest probability (72.35%) of achieving an anti–factor Xa level of 0.5 to 1 U/mL 4 hours after a dose, with 13.1% of patients achieving a level less than 0.5 U/mL, and 14.55% with a level above 1 U/mL. This treatment dosing scheme is our current practice standard, and we would advocate this dose as an empirical starting point for the pediatric population without reduced kidney function. However, we would also advocate routine anti–factor Xa monitoring in this patient population. Based on the model simulation, ~30% of patients will not achieve an anti-Xa level within the target range at this starting dose.
Age has been reported as a variable that should be taken into account when empirically dosing enoxaparin in pediatric patients.4,15,17 Our analysis noted a graphical trend associating decreased CL with increasing age, but this was not significant in the final model. Trame et al 14 similarly reported a trend in age with CL that was not significant in a population pharmacokinetic model. However, unlike prior population pharmacokinetic analyses, allometrically scaled weight was a significant covariate in our pharmacokinetic model. The use of weight appears to be a better marker for enoxaparin pharmacokinetics than age. For patients 1 year old and older, the use of age when selecting initial enoxaparin dose does not appear to be as appropriate a strategy. Dosing per kilogram of body weight is the more appropriate method for selection of empirical enoxaparin treatment doses.
SCr, as a marker of kidney function, was a significant covariate in our analysis. It is well known from the adult literature that adjustment of enoxaparin dosing is required in patients with kidney dysfunction. 15 We chose the breakpoint of 30 mL/min/1.73 m2 as a reference point from the adult literature, and we would suggest an approximate 30% reduction in dose for patients with creatinine clearance values less than this. Additionally, as kidney function is on a wide spectrum of values, we would encourage monitoring of anti–factor Xa concentrations in any patient who exhibits any decrease in kidney function.
Platelet count and hematocrit were both identified as significant covariates. These were unexpected findings, both of which had an influence on pharmacokinetic parameters. An increase in platelet values was associated with a decrease in VD, and an increase in hematocrit was associated with decreased CL. There are several hypotheses we propose for this finding. This could potentially be an artifact of low plasma volume in the venipuncture sample secondary to high red blood cell and platelet count, which results in a higher concentration of anti–factor Xa per mL of blood. Additionally, patients with alterations in platelet or hematocrit could have also had alterations in antithrombin III concentrations, though this is speculation. Overall, a low plasma volume resulting from changes in total body fluid composition could have affected the pharmacokinetic parameters and should be investigated further.
The normal limitations associated with a retrospective review apply to this report. We did not evaluate patients younger than 1 year of age because of the variability in pharmacokinetics and dosing that have been previously reported.16,17 This patient population is being evaluated separately to account for potential developmental changes in pharmacokinetics. We only evaluated data from inpatient stays, which allowed for precise determination of dosing and laboratory times, but cannot conclusively confirm the applicability of these data alone for long-term outpatient therapy. In prior investigations evaluating outpatient enoxaparin therapy in obese pediatric patients, it was noted that dosing requirements tended to decrease over time, possibly as a result of patient growth. 23 We also cannot comment on the clinical validity of attaining an anti–factor Xa level in the commonly accepted target range. A goal of 0.5 to 1 U/mL is the practice standard at our institution for treatment of thromboembolism and is the standard in many centers. Patients should be clinically evaluated for attainment of therapeutic goals (ie, thrombus resolution or prevention) along with therapeutic drug monitoring information. Additionally, subcutaneous site of injection was not available for collection and analysis and could influence patient pharmacokinetic parameters. Finally, specific disease states were not evaluated, although particular pathophysiological states, such as congenital heart disease and acute burns, have been shown to require alterations in dosing.3,24,25 We did not collect concomitant disease states or indications for enoxaparin in this study, and there could potentially be diverse pathophysiologies in our patient sample.
Overall, the developed model and the empirical dosing recommendations provided based on simulation offer guidance to clinicians on appropriate initial treatment dosing of enoxaparin in the pediatric population.
Conclusions
An enoxaparin dose of 1 mg/kg/dose subcutaneously every 12 hours is an appropriate dose for initiation of therapeutic anticoagulation therapy in pediatric patients 1 to 18 years of age. Reductions in dose of approximately 30% are necessary in patients with reduced kidney function. Monitoring of anti–factor Xa levels should be performed in pediatric patients to attain targeted anti-Xa levels.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.