
Abstract
Introduction
Dexmedetomidine is a centrally acting α2-adrenergic agonist used for sedation of mechanically ventilated patients. 1 It does not cause respiratory depression and, thus, can also be used in nonintubated patients. 2 Dexmedetomidine is given as a continuous intravenous (IV) infusion; starting doses vary based on desired level of sedation, and it is titrated every 1 to 2 hours to a typical maximum dose of 0.7 µg/kg/h. Loading doses may not be utilized because of potential for rebound hypertension and significant hypotension. 1
Evidence for the benefits of dexmedetomidine is conflicting. Some data suggest that it allows reductions in benzodiazepine or opioid requirements,3-5 but other data suggest otherwise.6,7 It has been associated with decreased ventilation times as compared with other sedatives in some studies3,7 but not in others. 8 A recent systematic review on the use of α2-adrenergic agonists in pediatric critical care did not pool results because of significant heterogeneity. 9
There is limited evidence regarding the safety of dexmedetomidine in the pediatric population. 1 Known cardiovascular adverse effects include hypotension and bradycardia; however, evidence regarding the incidence and severity in children varies.1,5-16 Because of its similar mechanism of action, dexmedetomidine can be associated with a clonidine-like withdrawal syndrome, and withdrawal effects (tachycardia, hypertension, anxiety) may develop on dexmedetomidine discontinuation.1,10-12 Clonidine can be utilized as an oral step-down agent and weaned off slowly to prevent withdrawal symptoms; however, evidence supporting this practice is limited. One study showed a trend toward lower Withdrawal Assessment Tool (WAT-1) scores in patients using transdermal clonidine post dexmedetomidine. 17 Note that the WAT-1 score has been validated for pediatric patients exhibiting withdrawal symptoms from opioids and benzodiazepines (scores >3 suggest withdrawal) but not for assessment of dexmedetomidine withdrawal. 18
Because of a relative lack of evidence and local experience with dexmedetomidine, our center put limitations on its use in September 2014. These guidelines suggested use either on a short-term basis (<24 hours) to facilitate extubation or in patients who have failed high doses of opioids, benzodiazepines, and 2 other sedative agents. The guidelines did not include suggestions for dosing, duration, or use in nonintubated patients because the purpose was to limit use to patients in highest need of additional sedation. Experience indicated that use was much higher than anticipated, and therefore, a description of use at our center was needed.
Because of safety concerns with prolonged propofol infusions in children 19 and dexmedetomidine’s lack of respiratory depression, it is an attractive agent for use in children. However, given limited evidence for the benefits of dexmedetomidine and the risk of adverse effects and withdrawal in the pediatric population, its use should be examined as it expands. This study will add to the existing literature regarding safety, efficacy, and withdrawal in the pediatric intensive care unit (PICU) setting.
The purpose of this project was to describe the use and tolerability of dexmedetomidine in a cohort of critically ill children. Associations between dexmedetomidine parameters or patient characteristics and the development of withdrawal or adverse events were examined.
Methods
A retrospective cohort study was performed on patients admitted to our PICU between October 2014 and February 2016. Our PICU is a 15-bed mixed medical-surgical (noncardiac) unit servicing a catchment area of around 3 million people, with approximately 900 admissions per year. Institutional ethics review board approval was granted with waiver of consent.
Patients were included if they received dexmedetomidine at any time in the PICU. If patients received dexmedetomidine on multiple occasions, only the first occurrence was analyzed. Patients were excluded if they were older than 18 years or received dexmedetomidine for <3 hours. Patients who died or transferred off-site while on dexmedetomidine were excluded.
Invasive ventilation was defined as any modality requiring intubation (conventional or high-frequency ventilation). Noninvasive ventilation included continuous or bilevel positive airway pressure but not high-flow nasal cannulae. Extubation on dexmedetomidine was deemed to have occurred if the patient was extubated without subsequent reintubation during dexmedetomidine administration.
Duration of dexmedetomidine infusion was calculated using start and stop times documented in the electronic health record and was considered to have been continuous if interruptions were <2 hours in duration. Weaning was considered to have occurred if there was any reduction in the dose (without any subsequent dose increase) prior to discontinuation of the dexmedetomidine infusion.
Doses of all analgesic/sedative infusions were recorded immediately prior to dexmedetomidine initiation and 24 hours later. If the dose of any other sedative was lowered and no additional sedation infusions were added or increased during this period, this was considered a reduction in other analgesic/sedative doses. A reduction in analgesic/sedative infusions was assumed to have occurred if the patient was transferred to a lower level of care.
Adverse effects were monitored using vital signs recorded in the PICU electronic charting system, monitored continuously or as required, depending on patient acuity. Hypotension was defined as systolic blood pressure <5th percentile for age at the 50th percentile for height (patient height is not consistently recorded at our center), 20 and bradycardia defined as a heart rate less than first percentile according to age. 21 An episode of hypotension or bradycardia must have lasted for 2 or more sequential measurements to qualify.
Signs of withdrawal were defined as hypertension, tachycardia, or a WAT-1 score >3. 18 Hypertension was defined as a systolic blood pressure >95th percentile for the 50th percentile of height,22,23 and tachycardia was defined as a heart rate >99th percentile according to age (both had to last 2 or more sequential measurements). 21 During the timeframe of this study, there were no established guidelines regarding WAT-1 scoring, and so this was ordered at physician discretion. Restart of dexmedetomidine or receipt of clonidine within 48 hours of dexmedetomidine discontinuation were also included as signs of withdrawal to capitalize on clinician suspicion of dexmedetomidine withdrawal.
Descriptive statistics were used to describe the cohort (mean ± SD or median and interquartile range). Means were compared using Student t-tests and medians using Kruskal-Wallis tests. χ2 Tests were used to test for interactions between end points (withdrawal and adverse effects) and predetermined variables, including age group, duration category, maximum dose, and presence of weaning (for withdrawal only). Variables with significant results were subsequently entered into a binary logistic regression model for adjusted analysis.
Results
A total of 243 patients were screened for inclusion; data were analyzed for 219 patients (Figure 1). The cohort median age was 25 months (Table 1). Compared with the overall cohort, patients who were intubated at the time of dexmedetomidine initiation were younger, and patients with no ventilator support at dexmedetomidine initiation were older. There were 10 infants younger than 28 days included; none of these were premature infants.
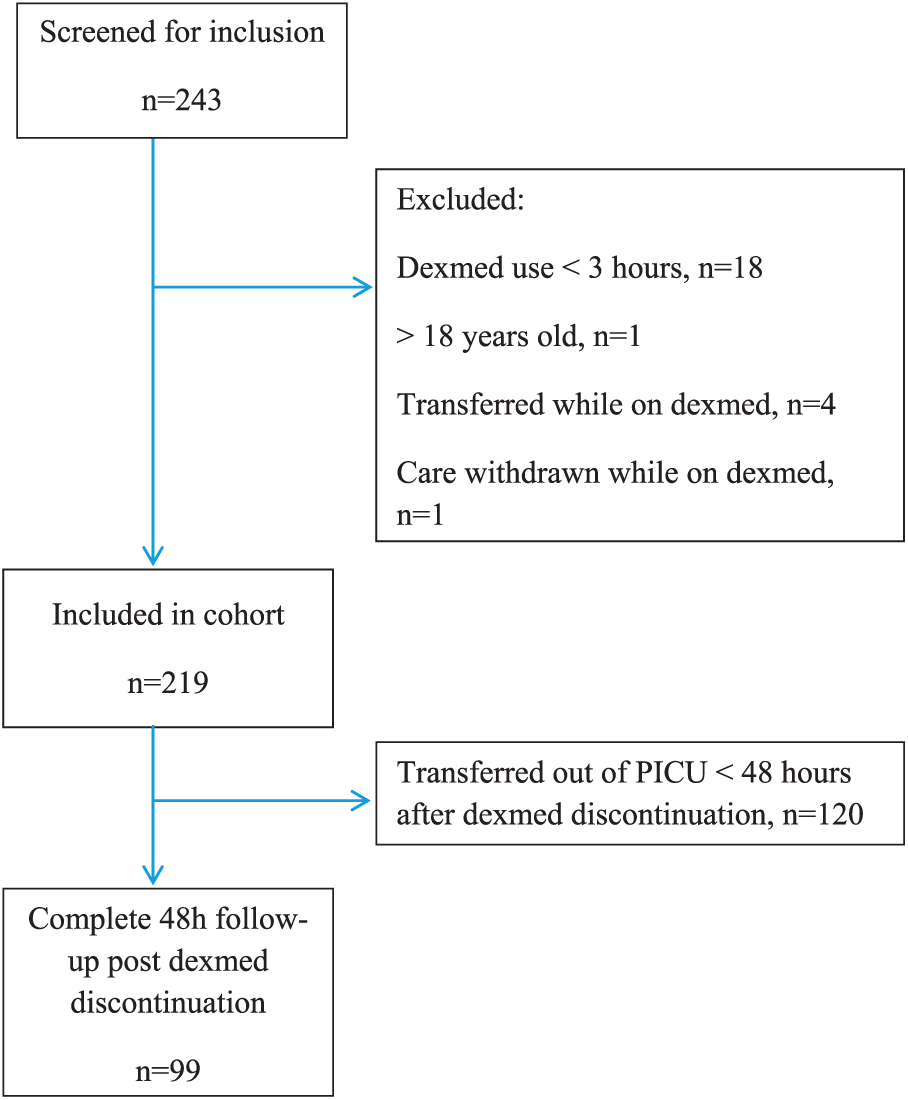
Cohort flow.
Cohort Characteristics by Ventilatory Support at the Time of Dexmedetomidine Initiation.
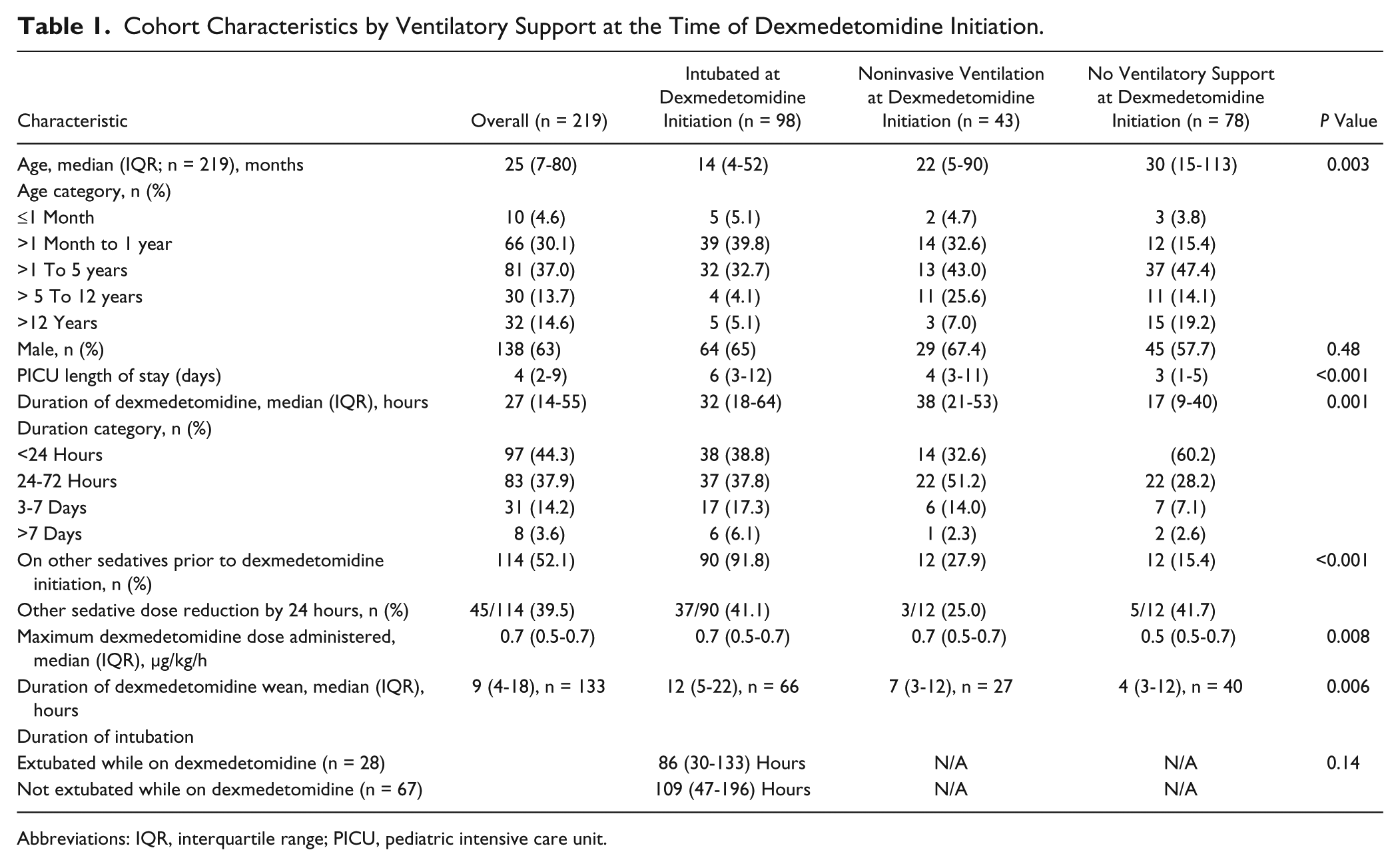
Abbreviations: IQR, interquartile range; PICU, pediatric intensive care unit.
On initiation of the dexmedetomidine infusion, 98 (45%) patients were invasively ventilated, 43 (20%) were noninvasively ventilated, and 78 (36%) were receiving no ventilatory support (Table 1). A total of 28 patients (28%) who were intubated at the time of dexmedetomidine initiation were extubated while on dexmedetomidine. The median duration of intubation for these patients was 86 hours; 9 of these patients were extubated within 24 hours of starting dexmedetomidine, and the median time from dexmedetomidine initiation to extubation was 45 hours. For the 67 (68%) patients who were intubated at the time of dexmedetomidine initiation but were not extubated on dexmedetomidine, the median duration of intubation was 109 hours; this was not statistically different from patients who were extubated on dexmedetomidine (P = 0.14).
The median duration of dexmedetomidine infusion was 27 hours (Table 1); this was shortest in patients who were on no ventilator support at dexmedetomidine initiation at 17 hours (P = 0.001). The most common (46%) maximum dose of dexmedetomidine was 0.7 (range = 0.1-1.3) µg/kg/h, and 22 patients (10%) used a maximum dose >0.7 µg/kg/h. The median maximum dose was lower in the group receiving no ventilator support at dexmedetomidine initiation, at 0.5 µg/kg/h (P = 0.008). There was no difference in the maximum dose used between age groups (P = 0.395).
A total of 114 (52%) patients had been on at least 1 sedative or analgesic agent prior to dexmedetomidine initiation; 61 (28%) patients received concomitant opioid and benzodiazepine, and 43 (20%) had received 2 other (ie, nonopioid, nonbenzodiazepine) additional sedatives prior to receiving dexmedetomidine. Prior use was highest in the group who were intubated at the time of dexmedetomidine initiation, at 91.8% (P < 0.001; Table 1). Prior sedatives or analgesics included (either as continuous infusions, intermittent doses, or both; agents may have been used concurrently) the following: hydromorphone (n = 81), fentanyl (n = 15), morphine (n = 31), ketamine (n = 67), propofol (n = 13), and midazolam (n = 26), lorazepam (n = 46), and oral clonidine (n = 11). Note that clonidine would have been stopped prior to dexmedetomidine initiation. Of the patients on a sedative or analgesic infusion immediately prior to dexmedetomidine, 39.5% had a dose reduction measured 24 hours later.
In all, 91 (42%) patients experienced an adverse effect while on dexmedetomidine (Table 2), with 59 (27%) experiencing hypotension, 47 (21%) experiencing bradycardia, and 15 (7%) experiencing both. The median number of episodes per day of hypotension and bradycardia were 0.97 and 1.04, respectively. χ2 analysis indicated differences in the rate of adverse effects between age (P = 0.001) and dexmedetomidine duration subgroups (P < 0.001); these were entered into a binary logistic regression model. Patients aged 1 month to 1 year were more likely to experience an adverse event as compared with children older than 12 years (odds ratio = 3.46; 95% CI = 1.30-9.21), and the odds of developing an adverse event increased with dexmedetomidine duration. The mean maximum dose in patients who experienced an adverse effect was 0.66 µg/kg/h, which was not different from patients who did not experience an adverse event (0.59 µg/kg/h; P > 0.05).
Rates of Adverse Effects Observed During Dexmedetomidine Infusion.
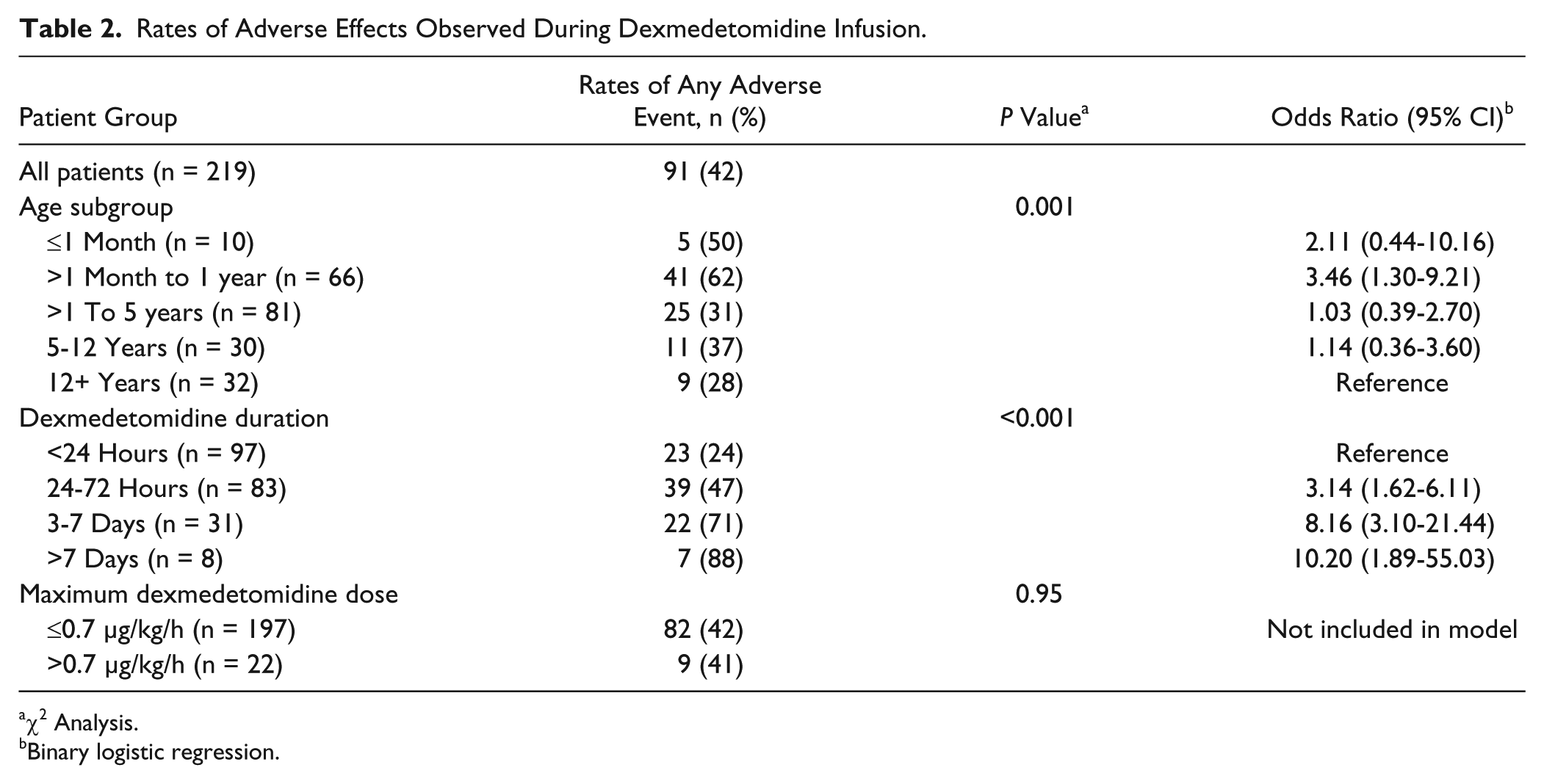
χ2 Analysis.
Binary logistic regression.
A total of 133 (61%) patients were weaned off dexmedetomidine using a dexmedetomidine dose taper, and 9 (4%) were weaned off using oral clonidine (1-2 µg/kg/dose every 6 hours titrated to effect). The choice of agent was based on IV access and ability to tolerate enteral medication; a standard weaning protocol was not in place. The median duration of weaning was 9 hours and was longest in the group that was intubated at the time of dexmedetomidine initiation at 12 hours (P = 0.006). Among all patients (including those who were weaned and those who were not), 39 (18%) restarted dexmedetomidine within 48 hours; 36 (16%) patients were receiving clonidine within 48 hours of stopping dexmedetomidine.
Only 99 (45%) patients had a full 48 hours of vital sign monitoring and WAT-1 scoring after dexmedetomidine discontinuation. The remainder of the patients were discharged from PICU within that timeframe (vital signs recorded on the general wards were not available; Table 3). In all, 79 (80%) patients experienced either hypertension, tachycardia, or a WAT-1 score >3 during this period; 52 (53%) of these patients experienced hypertension, 52 (53%) experienced tachycardia, and 27 (27%) experienced both. Of the 40 patients who had documented WAT-1 scores throughout their dexmedetomidine wean and for a full 48 hours following discontinuation, 15 (38%) had a WAT-1 score >3. χ2 analysis showed no association between signs of withdrawal and age, duration of dexmedetomidine, maximum dose, or presence of weaning.
Rates of Withdrawal Signs During Dexmedetomidine Wean and for 48 Hours After Discontinuation.
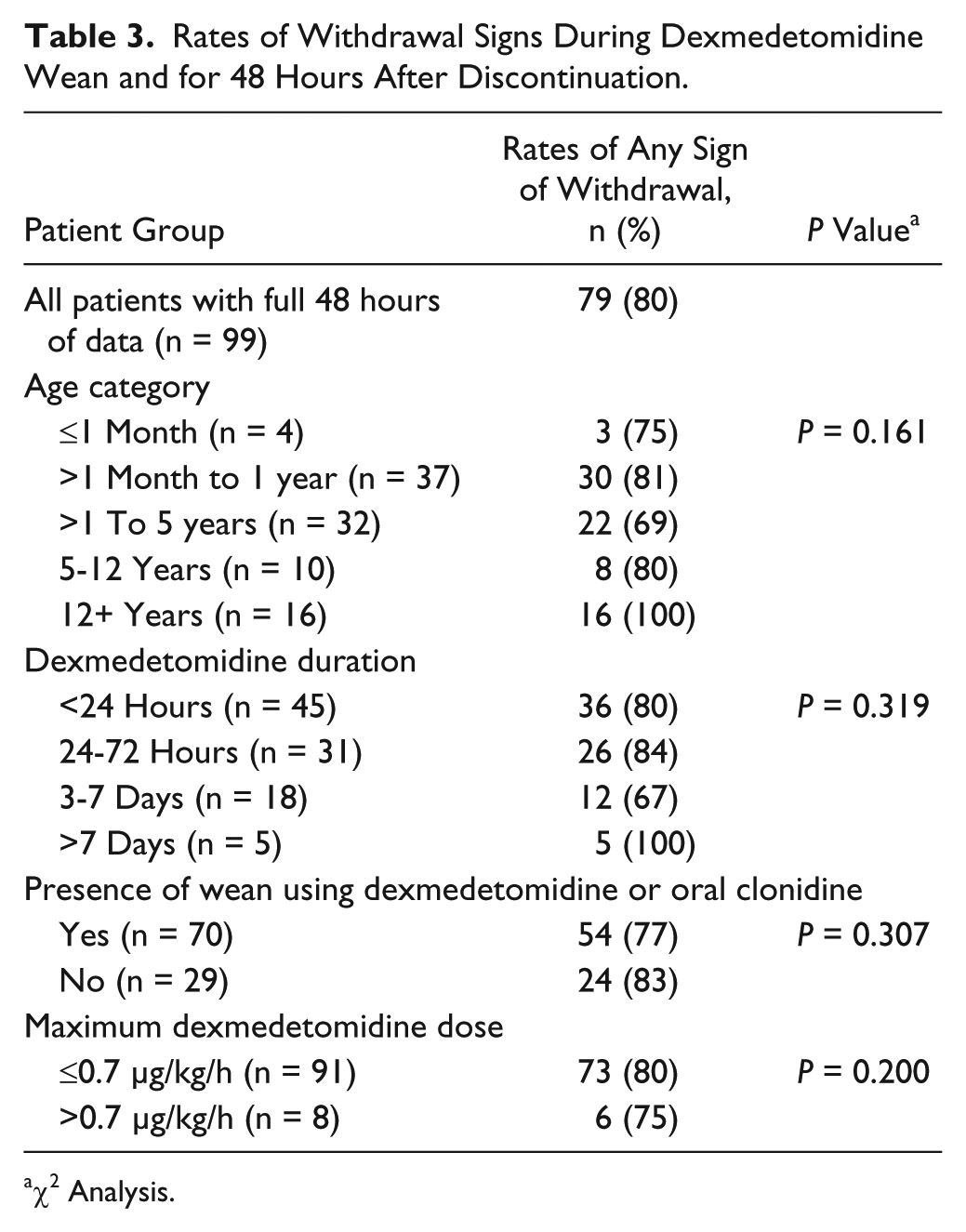
χ2 Analysis.
Discussion
We report data from a large cohort of critically ill children receiving dexmedetomidine. More than half of the patients using dexmedetomidine were not intubated at the time of initiation (20% noninvasively ventilated, 36% no ventilatory support). Presumably this use was to facilitate face mask tolerance. Given that the use of noninvasive ventilation is common and increasing in pediatric critical care, we suspect that this has become a common indication for dexmedetomidine beyond our center.24,25 Dexmedetomidine was also commonly used in patients receiving no ventilatory support at all. This group used dexmedetomidine for a shorter duration of time and at lower doses than patients with invasive or noninvasive ventilation. The utility and safety of the use of dexmedetomidine in these presumably less sick patients warrants further study.
Dexmedetomidine has been utilized to facilitate extubation because of its lack of respiratory depression. 2 Less than 10% of our cohort was extubated within 24 hours of dexmedetomidine initiation, and of those who were extubated while on dexmedetomidine, the duration of intubation was not different from those who were not extubated on dexmedetomidine. However, other studies have suggested that there may be a role for dexmedetomidine in facilitating extubation. In a prospective observational study by Buck and Willson, 26 15 patients were started on dexmedetomidine to facilitate extubation, with 87% of these patients being successfully extubated within 24 hours. Grant et al 7 found that when dexmedetomidine was used as primary sedative agent to facilitate extubation, the duration of mechanical ventilation was reduced. These differences in the effect on extubation may reflect differences in practice. With less than half of our cohort invasively ventilated at the time of dexmedetomidine initiation, it appears that clinicians at our site are not utilizing dexmedetomidine solely to facilitate extubation.
About half our cohort received another sedative/analgesic agent prior to initiating dexmedetomidine, with the lowest rate in patients receiving no ventilatory support (15%) and the highest rate in intubated patients (92%). This degree of first-line use is noteworthy because our local guidelines suggest that dexmedetomidine be used only after other sedatives have failed. Whereas some studies have suggested that dexmedetomidine may allow for reduction in benzodiazepine or opioid requirements in children,3-5 others have not, 6 and the largest study published to date describing the use of dexmedetomidine in intubated PICU patients demonstrated that only when dexmedetomidine was used as a primary sedative agent were patients exposed to less opioids (secondary use was associated with higher opioid exposure). 7 In our cohort, when dexmedetomidine was added to other sedative/analgesic combinations, about 40% of the patients had a dose reduction in other sedatives by 24 hours, which may or may not represent a reduction in opioid or benzodiazepine exposure overall. Reductions in opioid and benzodiazepine exposure may be beneficial because there is evidence that these agents may be harmful to neurodevelopment.27,28 Emerging literature suggests that dexmedetomidine may actually be neuroprotective to developing brains.28,29 Our study did not include collection of long-term neurological outcomes, and therefore, we cannot comment on any potential neurodevelopmental impact.
Delineating the incidence and severity of adverse effects from dexmedetomidine has been challenging, which is reflected in the variable incidence and clinical significance of bradycardia and hypotension published.5-11,14,30 Our data are limited in that the effects of dexmedetomidine could not be separated from those of other medications or clinical condition. Our study showed similar rates of bradycardia (21% vs 25%) but a lower rate of hypotension (27% vs 53%) than a previously reported retrospective cohort study. 10 Other retrospective cohort studies have shown similar rates of hypotension (22% and 27%) and variable rates of bradycardia (15% and 56%).11,14 Our data were congruent with others in that the incidence of adverse effects was higher in younger patients. 10 The relationship between adverse effects and infusion duration seen in our cohort was replicated in 1 study 10 but not in another, 11 although the latter study did find an association with ICU length of stay. What is consistent in the literature is that hypotension and bradycardia occur often during dexmedetomidine infusions in the PICU, and careful monitoring is warranted.
Signs of withdrawal appeared to be common in our cohort, with 80% of patients experiencing either hypertension, tachycardia, or a WAT-1 score >3 (where scoring was documented). This is similar to previously reported withdrawal incidence (83%) 10 ; however, another retrospective study showed lower rates of hypertension (35%) and tachycardia (27%) despite the fact that the median infusion duration was much longer than that in the present cohort (median 5.8 days vs 27 hours). 12 Possible explanations for these differences include differences in monitoring time (12 vs 48 hours) and wean duration (median 43 vs 9 hours). 12
Although this high rate of withdrawal effects could have significant negative effects on patients, it is important to understand that there is no clear guidance on the detection and prevention of withdrawal from dexmedetomidine in the pediatric population, and although we have used cardiovascular signs as well as WAT-1 scores, these have not been validated for dexmedetomidine withdrawal. Second, patients with well-documented WAT-1 scores (only 45% of our cohort) were likely ordered this monitoring because of a higher risk of withdrawal, and so our WAT-1 scoring data are subject to selection bias. Finally, cardiovascular signs of dexmedetomidine withdrawal (tachycardia and hypertension) are common in PICU patients, and therefore, it is difficult to definitively assign to dexmedetomidine withdrawal. These challenges highlight the need for clear definitions of dexmedetomidine withdrawal and recommendations for its identification, prevention, and management.
Our analysis of factors associated with withdrawal did not show a difference in the rates of withdrawal between age groups, dexmedetomidine duration, maximum dose, or patients who were weaned using dexmedetomidine/oral clonidine or not. These results possibly reflect the fact that clinicians selected patients at higher risk for withdrawal for weaning. In contrast to our results, Burbano et al 12 reported that the presence of weaning reduced the incidence of tachycardia. 12 Similarly, Lardieri et al 17 reported that clonidine used to prevent withdrawal symptoms after dexmedetomidine resulted in less tachycardia but did not affect WAT-1 scores.
Our study was subject to some inherent limitations. There was considerable intrapatient dosing variability; thus, weaning duration was hard to define and subject to underestimation or overestimation. We were unable to collect complete data on patients who were transferred off-site or who died on dexmedetomidine, and thus, these patients were excluded (n = 5). Finally, we did not compare dexmedetomidine with other agents, which makes it difficult to draw conclusions regarding the specific effects of dexmedetomidine.
Conclusions
Our cohort includes a large number of PICU patients on dexmedetomidine, both intubated and nonintubated. We saw a significant incidence of adverse effects that appear to be higher in younger patients and those with prolonged infusions. Withdrawal effects were also common, with no predictors among age, duration of infusion, maximum dose, or presence of weaning. Use of dexmedetomidine in patients receiving noninvasive ventilation or no ventilator support was common. Controlled studies are needed to better understand the optimal use of dexmedetomidine as it pertains to prevention and management of adverse effects and withdrawal and especially to use in nonintubated patients.
Footnotes
Authors’ Note
This article was presented in poster format at the Canadian Association of Pediatric Health Centres Conference in Halifax, Nova Scotia, from October 23-25, 2016.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.