
Abstract
Keywords
Introduction
Atherosclerotic cardiovascular disease (ASCVD) describes the clinical manifestations of atherosclerosis, including coronary heart disease (CHD), cerebrovascular attacks, and peripheral arterial disease.1-3 Heart disease, with CHD being the most common type, is the leading cause of death, with an estimated cost of more than $200 billion in the United States each year. 4 Given the pathophysiology of atherosclerosis, treatment is focused on lowering low-density lipoprotein cholesterol (LDL-C).5,6 In 2013, the American College of Cardiology (ACC) and the American Heart Association (AHA) released a treatment guideline for blood cholesterol. 3 This new guideline has 3 notable departures from the standards established by the Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel [ATP] III). First, the guideline highlights 4 target groups who should receive secondary or primary prevention for ASCVD. Second, treatment recommendations are focused on utilizing statins over other classes of medication. Finally, unlike ATP III, the 2013 ACC/AHA guideline does not treat to achieve specific LDL-C levels. 3
The 2013 ACC/AHA guideline is estimated to make more than 12 million additional Americans eligible for statin treatment. 7 Identification and treatment of these patients would require widespread adoption of the guideline into clinical practice. However, the National Lipid Association and the American Association of Clinical Endocrinologists are 2 national organizations that have not endorsed the guideline.8,9 In the evaluation of treatment guidelines for other disease states, perhaps associated with less controversy, previous studies have found adherence rates ranging between 54.7% to 67.0%.10-13 Few studies are currently published evaluating the adherence rates to the 2013 ACC/AHA cholesterol guideline. In a study involving patients with ASCVD enrolled in a managed care plan, less than 50% were being treated with a recommended high-intensity statin. 14 Another study found that in patients with ASCVD requiring secondary prevention, only 41.8% received high-intensity statins after publication of the new cholesterol guideline. 15 These studies have shed insight into real-world uptake of the newest cholesterol guideline. However, they are limited by their focus on 1 of the 4 benefit groups outlined in the guideline. In a retrospective study, Schoen et al 16 predicted that 56% of patients who were previously being treated for hyperlipidemia according to ATP III would be considered concordant to the 2013 ACC/AHA guideline. 16 However, estimated adherence to the new guideline was based on data collected prior to its release in November 2013.
More recently, one study conducted by Ng et al 17 evaluated adherence to the 2013 ACC/AHA guideline examining all benefit groups and using data collected after the release of the guideline. This study evaluated data from a family medicine teaching clinic within a large medical group—namely, the Montefiore Medical Group (MMG). Results showed that 65.8% of statin-naïve patients were appropriately initiated on statin therapy according to the new guideline. However, adherence could vary in another clinic within the same medical group, particularly in a nonteaching practice site. Previous studies comparing teaching versus nonteaching settings have shown conflicting results on whether one is associated with greater guideline adherence.18-20 It is our goal to compare adherence rates to the 2013 ACC/AHA guideline in a teaching versus a nonteaching medical practice. In addition, this study evaluates the impact of a pharmacist-led education session on adherence to the guideline because limited data exist regarding the impact of provider education on adherence rates.
Methods
The current institutional review board–approved study is a 2-part evaluation consisting of a retrospective review of adherence to statin prescribing based on the 2013 ACC/AHA guideline and an assessment of prescribing adherence rates before and after a pharmacist-led review of the guideline. This study took place at MMG, which consists of several teaching and nonteaching outpatient clinics. The majority of clinics are located in Bronx, NY, and cater to an urban, underserved population.
For part 1 of the study, patients ≥21 years of age who visited a nonteaching outpatient primary care clinic at Grand Concourse (GC) of MMG and received a statin prescription between December 1, 2013, and November 30, 2014, were identified using our clinical information system, Clinical Looking Glass. Patients were included in the study if they had a visit within 7 days before or after receiving a statin prescription, a lipid panel obtained within 1 year before a statin prescription, and no history of statin therapy within 5 years of the statin prescription. These inclusion criteria were selected to calculate a 10-year ASCVD risk score using the Pooled Cohort Equation. 21 Because of the lack of statin intensity recommendation from the guideline, patients were excluded if they did not have clinical ASCVD and were (1) <40 or >75 years of age with LDL-C <190 mg/dL or (2) had diabetes with LDL-C <70 mg/dL. Patients were also excluded if ASCVD risk score could not be calculated because of clinical parameters being outside the limits allowed by the Pooled Cohort Equation (eg, high-density lipoprotein cholesterol [HDL-C] <20 mg/dL).
ASCVD Risk Score Calculation and Patient Categorization
After initial screening, the 10-year ASCVD risk score was estimated in eligible patients using the Pooled Cohort Equation based on age, gender, race, HDL-C, total cholesterol, systolic blood pressure, smoking status, treatment of hypertension, and a diagnosis of diabetes. Subsequently, patients were categorized into 1 of 4 statin benefit groups. The clinical ASCVD group included patients with a history of acute coronary syndromes, myocardial infarction, unstable or stable angina, coronary or other arterial revascularization procedures, stroke, transient ischemic attack, or peripheral arterial disease who require secondary prevention. The second group included patients with LDL-C ≥190 mg/dL without clinical ASCVD. Diabetic patients between 40 and 75 years old whose LDL-C was 70 to 189 mg/dL but without clinical ASCVD were assigned to the third group. The final group comprised of patients with 10-year ASCVD score ≥5% who were between 40 and 75 years old and did not have clinical ASCVD, diabetes, or LDL-C ≥190 mg/dL.
Based on the aforementioned indications for statin therapy, patients were assigned into moderate-, moderate- to high-, or high-intensity statin therapy groups according to 2013 ACC/AHA guideline recommendations. 3 Finally, patients were assigned into low-, moderate-, or high-intensity statin groups according to the statin prescriptions they received. 3
Therapeutic Outcome Determination
The 2013 ACC/AHA cholesterol guideline recommends repeat LDL-C determination 4 to 12 weeks after initiation of statin therapy. According to the guideline, therapeutic goals of high-, moderate-, and low-intensity statin therapy are reduction of LDL-C by ≥50%, 30 to <50%, and <30% from baseline, respectively. For patients with repeated LDL-C at any time after initiation of statin therapy, percentage reduction from baseline was determined. Achievement of LDL-C reduction was determined based on guideline-recommended statin intensity (not statin intensity received).
Pharmacist-Led Review of Guideline
The second part of the study assessed the effect of pharmacist-led education on the adherence rate to guideline statin prescribing. A postgraduate year 2–trained clinical pharmacist presented a 1-hour inservice on the 2013 ACC/AHA guideline to physicians at GC. The inservice included review of the 4 statin benefit groups, appropriate statin intensity based on indications, and recommended monitoring for therapeutic efficacy. Using the criteria and methods in part 1 of the study, rates of adherence to guideline prescribing were compared in patients who were initiated on statin 3 months before and after the pharmacist-led education session.
Outcomes Assessment
The primary objective of the study was to evaluate the adherence rate to statin prescribing based on the 2013 ACC/AHA guideline at GC. Adherence is defined as accurately prescribing statins as recommended in the guideline. The prescribing adherence rate of the nonteaching clinic at GC was compared to that determined at another teaching clinic of MMG in a study conducted by Ng et al. 17 Secondary outcomes evaluated in this study included the quarterly guideline prescribing adherence rates at GC to determine if a trend exists, the proportion of patients with follow-up LDL-C, and the percentage of patients able to achieve goal LDL-C percentage reduction in the guideline-adherent and guideline-nonadherent groups. Finally, the rates of guideline-adherent prescribing 3 months before and after a pharmacist-led educational session were compared.
Statistical Analysis
Categorical variables were analyzed using Fisher’s exact and Pearson’s χ2 tests. For continuous variables, data were evaluated for normality using the Shapiro-Wilk test and visual inspection of data distribution. Because most of the continuous data were nonnormally distributed, the Wilcoxon rank-sum test was used for between-group comparisons. A P value <0.05 was considered statistically significant. For multiple comparisons, Bonferroni correction was used to determine significant P values. All statistical analyses were performed using GraphPad Prism, version 7.02 (GraphPad Software, La Jolla, CA).
Results
A total of 325 patients who received a new statin prescription between December 2013 and November 2014 were screened for inclusion for the first part of the study. Among them, 52 patients were excluded because of inability to calculate their 10-year ASCVD risk score because of clinical parameters outside the limits of the Pooled Cohort Equations risk assessment. Another 40 were excluded because of lack of guideline-based indication for statin therapy. The remaining 233 patients were included in the study and evaluated for receipt of guideline-adherent statin therapy.
Patient demographics and baseline characteristics of the 233 patients are summarized in Table 1. The majority of the study population was composed of African Americans (49.8%), with only a small number of Caucasians (5.2%). Approximately 40% and 66% of patients had a history of diabetes and treatment of hypertension, respectively. Patients who were prescribed guideline-adherent therapy had a significantly higher baseline median LDL-C (164 vs 140 mg/dL, P < 0.01) and were less likely to be diabetics (17.0% vs 56.4%, P < 0.01). Other baseline and demographic characteristics were comparable between groups.
Baseline Patient Characteristics: Study Part I.
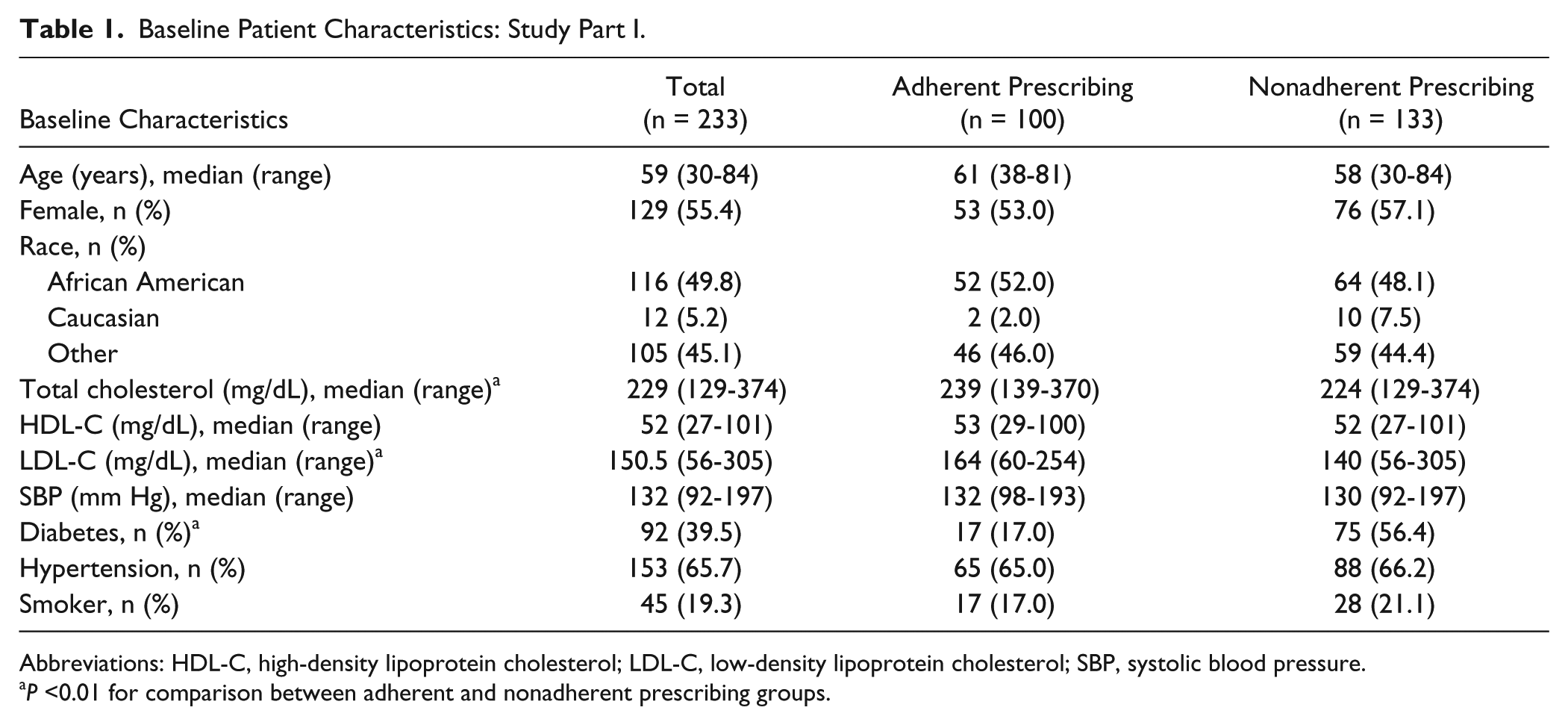
Abbreviations: HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure.
P <0.01 for comparison between adherent and nonadherent prescribing groups.
Primary Outcome
The overall guideline-adherent prescribing rate for the current study was 42.9% (100 of 233 patients) at a nonteaching primary care clinic. In comparison to a study previously conducted by Ng et al 17 at a teaching primary care clinic, the adherence rate observed in this study was significantly lower (42.9% vs 65.8%, P < 0.0001).
Characteristics of statin therapy prescribed in this study are summarized in Table 2. The most common indication for statin therapy was 10-year ASCVD risk score ≥5% (37.8%), followed by diabetes (33.5%). A significantly lower percentage of patients with diabetes (12 of 78 patients, 15.4%) were prescribed guideline-adherent statin therapy compared with those with baseline LDL-C ≥190 mg/dL (21 of 47 patients, 44.7%; P < 0.0005) or with ASCVD risk score ≥5% (59 of 88 patients, 67.0%; P < 0.0005). Of note, less than half of the patients (8 of 20 patients, 40%) who required secondary prevention because of ASCVD were prescribed guideline-adherent statin therapy. According to the treatment guidelines, 54.1% of the study patients should have been on high-intensity statins. However, most of these patients (55.4%) were started on moderate-intensity statins rather than high-intensity statins (16.7%). The highest rate of guideline-adherent prescribing was observed in patients who received high-intensity statin therapy (89.7%) compared with those who received moderate- (50.4%) and low-intensity (0%) statin therapy.
Characteristics of Statin Therapy: Study Part I.
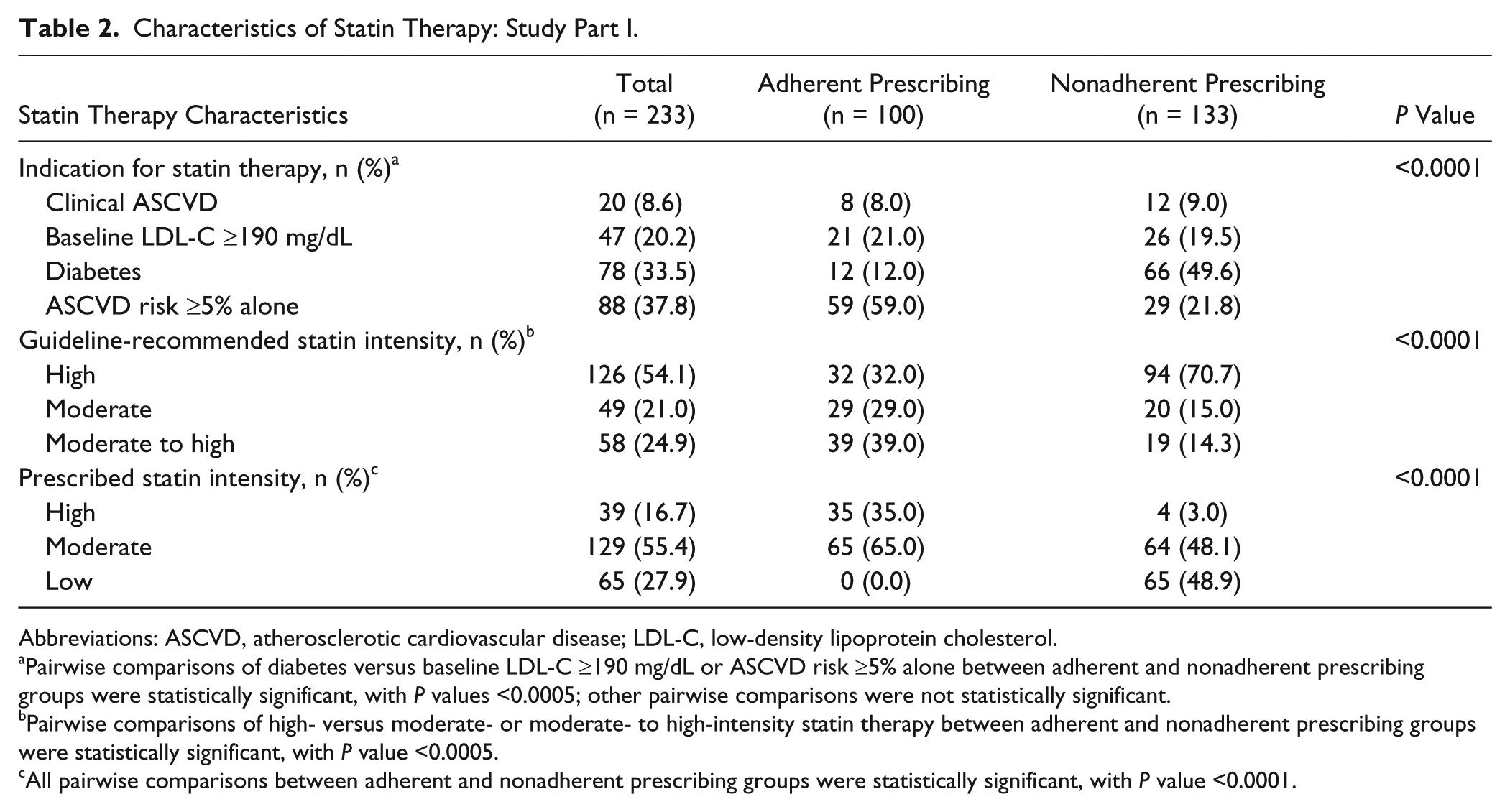
Abbreviations: ASCVD, atherosclerotic cardiovascular disease; LDL-C, low-density lipoprotein cholesterol.
Pairwise comparisons of diabetes versus baseline LDL-C ≥190 mg/dL or ASCVD risk ≥5% alone between adherent and nonadherent prescribing groups were statistically significant, with P values <0.0005; other pairwise comparisons were not statistically significant.
Pairwise comparisons of high- versus moderate- or moderate- to high-intensity statin therapy between adherent and nonadherent prescribing groups were statistically significant, with P value <0.0005.
All pairwise comparisons between adherent and nonadherent prescribing groups were statistically significant, with P value <0.0001.
Secondary Objectives
Examination of guideline-adherent prescribing rates by 3-month intervals did not reveal a significant trend. The rate of adherent prescribing was 40.9% between December 2013 and February 2014 and increased to 51.7% during the subsequent 3 months, but declined to only 30.5% in June to August 2014, and finally rebounded back to 44.4% in the last quarter of the study period.
Among the 233 patients included in the study, follow-up lipid panel was obtained in 198 (85.0%) patients after initiation of statin therapy. Of these patients, target percentage of LDL-C reduction was achieved only in 65 (32.8%) patients. The proportions of patients with follow-up lipid panel were comparable between the guideline-adherent and nonadherent groups (87.0% vs 83.5%). Patients who were prescribed guideline-adherent therapy had a significantly higher rate of goal LDL-C percentage reduction compared with those who did not (41.4% vs 26.1%, P = 0.03).
For the second part of the study, 91 patients who received a new statin prescription before and after a pharmacist-led education session on the 2013 ACC/AHA guideline were evaluated for rates of guideline-adherent prescribing. The adherence rate was 53.5% before the educational session and remained essentially unchanged (54.2%) after the educational session.
Discussion
The introduction of the 2013 ACC/AHA guideline ushers in a new paradigm in the management of hyperlipidemia. This new guideline represents a significant departure from prior guidelines and was met with considerable controversy after its publication. As such, many prescribers may be unwilling to adapt the 2013 ACC/AHA guideline into clinical practice. We conducted the current evaluation to examine the level of guideline compliance in an outpatient clinic of our health system and whether prescriber education can have an impact on compliance rate.
Compared to an adherence rate of 65.8% to the 2013 ACC/AHA guideline in a similar study conducted by Ng et al 17 at an outpatient teaching practice site, the adherence rate observed in our study, which took place at a nonteaching practice site, is significantly lower at 42.9%. This observation is consistent with results from a study that analyzed >270,000 patients, which showed that implementation of guideline-concordant care was higher at teaching hospitals compared with nonteaching hospitals. 18 It is possible that practitioners at teaching hospitals are more inclined to review established guidelines for academic purposes and, thus, are more familiar with and are more likely to implement guidelines into their practices. The highest concordance rate (67.0%) to the 2013 ACC/AHA guideline in our study was observed in group 4, where patients with 10-year ASCVD risk scores ≥5% were considered to be guideline concordant if they were on either high-intensity or moderate-intensity statins. It is concerning that only about 15% and 40% of patients with diabetes and ASCVD, respectively, were prescribed the appropriate statin intensities because these patients are at high risk for CHD and are most likely to benefit from appropriate statin intensity treatments. As recommended by authors from the Ng et al 17 study, calculations of 10-year ASCVD scores for all diabetic patients 40 to 75 years of age may help prompt appropriate intensity of statin prescribing in these patients. Although the guideline adherence rate was low at only 40% in our ASCVD patients, this observation is consistent with findings from other studies.14,15
In contrast to the low percentage of patients (31.6%) who had a follow-up lipid panel observed in the study by Ng et al, 17 a majority of patients (85.0%) in our study had a follow-up lipid panel. A reason for the low follow-up in the former study could be a result of a transition of care from a teaching service to more permanent primary care providers. Because our study was conducted in a nonteaching practice site, patients were more likely to return for appointments with their long-term health care providers and, thus, a higher percentage of follow-up lipid panels were obtained. Nevertheless, of the patients who had a follow-up lipid panel in our study, only 32.8% of patients were able to reach target percentage LDL-C reduction goals, which warrants efforts to improve on this result. Of note, patients who were prescribed guideline-adherent therapy had a significantly higher rate of goal LDL-C percentage reduction in our study. This finding suggests that the adherence to the 2013 ACC/AHA guideline could help more patients achieve appropriate cholesterol goals, which could translate to better cardiovascular outcomes. A trend in guideline-adherent prescribing rates was not identified during the study period, suggesting that awareness and/or acceptance of this guideline have not changed over time. In an effort to increase familiarity with the 2013 ACC/AHA guideline, a 1-hour pharmacist-led education session on this guideline was conducted. However, the rate of adherence to the guideline did not change in the 3 months after the inservice. This observation suggests that a one-time education session may not be sufficient to promote adherence to guidelines. Periodic review and discussion of guidelines or case-based learning between prescribers and the clinic pharmacists may be necessary to encourage and improve adherence.
There are several limitations to this study. First, we did not identify or exclude patients with New York Heart Association class II to IV heart failure or those undergoing maintenance hemodialysis even though there were no clear recommendations on statin therapy for these patients as stated by the 2013 ACC/AHA guideline. Second, adherence to statin therapy was not evaluated in this study. Because poor adherence rates have been demonstrated in patients receiving hyperlipidemia therapy, it is possible that some of our patients were not taking their statin therapy as prescribed. 22 In addition, 9 patients in our study were on concomitant nonstatin lipid-lowering agents, and this could have affected our findings on therapeutic response. Our study also did not identify reasons for the low adherence rate to the 2013 ACC/AHA guideline. The Pooled Cohort Equation has been a source of controversy because some clinicians are concerned that it may overestimate risk when applied to a more contemporary US population, leading to overtreatment of some patients such as the elderly.23,24 Some clinicians and patients may prefer specific lipid goals, which are not offered by the 2013 ACC/AHA cholesterol guideline. Another possible reason for low adherence could be a lack of familiarity with this guideline. Often, physicians decide on optimal therapies for specific conditions and convey these plans to patients. However, it is ultimately the patient who must understand the risks and benefits of these therapies and agree to initiate treatment. This shared decision-making process is vital in patient care but was not evaluated in this study. 25 We also did not evaluate nonstatin therapies, drug interactions, or intolerance to statin therapy, which are factors that may have influenced provider decisions when it came to prescribing statins. Knowing the reasons for nonadherence to guidelines could possibly help improve future adherence. Finally, this study examined data in 1 clinic with a relatively small number of patients. It is possible that these results could vary, yet again, in another practice site with a different patient population or health care providers.
Conclusion
Fewer than 50% of patients received guideline-adherent statin therapy in a nonteaching outpatient clinic, which was significantly lower than that in a teaching clinic within the same medical group. A one-time educational session conducted by a clinical pharmacist did not significantly improve adherence rates to the 2013 ACC/AHA cholesterol guideline.
Footnotes
Authors’ Note
This work has never been presented as an abstract or poster.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.