
Abstract

High-dose methotrexate, defined as doses ≥500 to 1000 mg/m2, is used to treat a variety of malignancies. High-dose methotrexate can cause significant nephrotoxicity. Volume depletion and acidic urine are major risk factors for acute kidney injury. Precipitation of methotrexate crystals is most likely to occur in acidic urine when pH drops below 5.5. Increasing urine pH from 6.0 to 7.0 has been demonstrated to increase the solubility of methotrexate and its metabolites by 5- to 8-fold. Continuous intravenous (IV) sodium bicarbonate has been a simple long-term solution for urinary alkalization, allowing rapid titration to accommodate fluctuations in urinary pH.1,2
A recent breakdown in the supply chain of IV sodium bicarbonate has become a health care crisis compromising patient care. Sodium bicarbonate 8.4% and 7.5%, 50-mL syringes were estimated to remain on back order until at least early August 2017. Although limited supply has become available, it is being reserved for use in critically ill patients at our institution. Alternative sources, such as sodium acetate, are in limited supply as well.3,4 In a small case series, acetazolamide 500 mg IV every 6 hours was reported to achieve adequate urinary alkalization; however, efficacy of such a regimen has not been examined in a large population. 5 Our lack of IV sodium bicarbonate created an urgent need to establish a practical alternative for urinary alkalization in patients receiving high-dose methotrexate. We designed a pilot algorithm for urinary alkalization in patients undergoing high-dose methotrexate therapy (Table 1). The algorithm relies on administration of IV acetazolamide and oral sodium bicarbonate to rapidly induce urinary alkalosis. 5
Urine Alkalinization Algorithm for Patient Management and Dose Modifications During Administration of High-Dose Methotrexate.
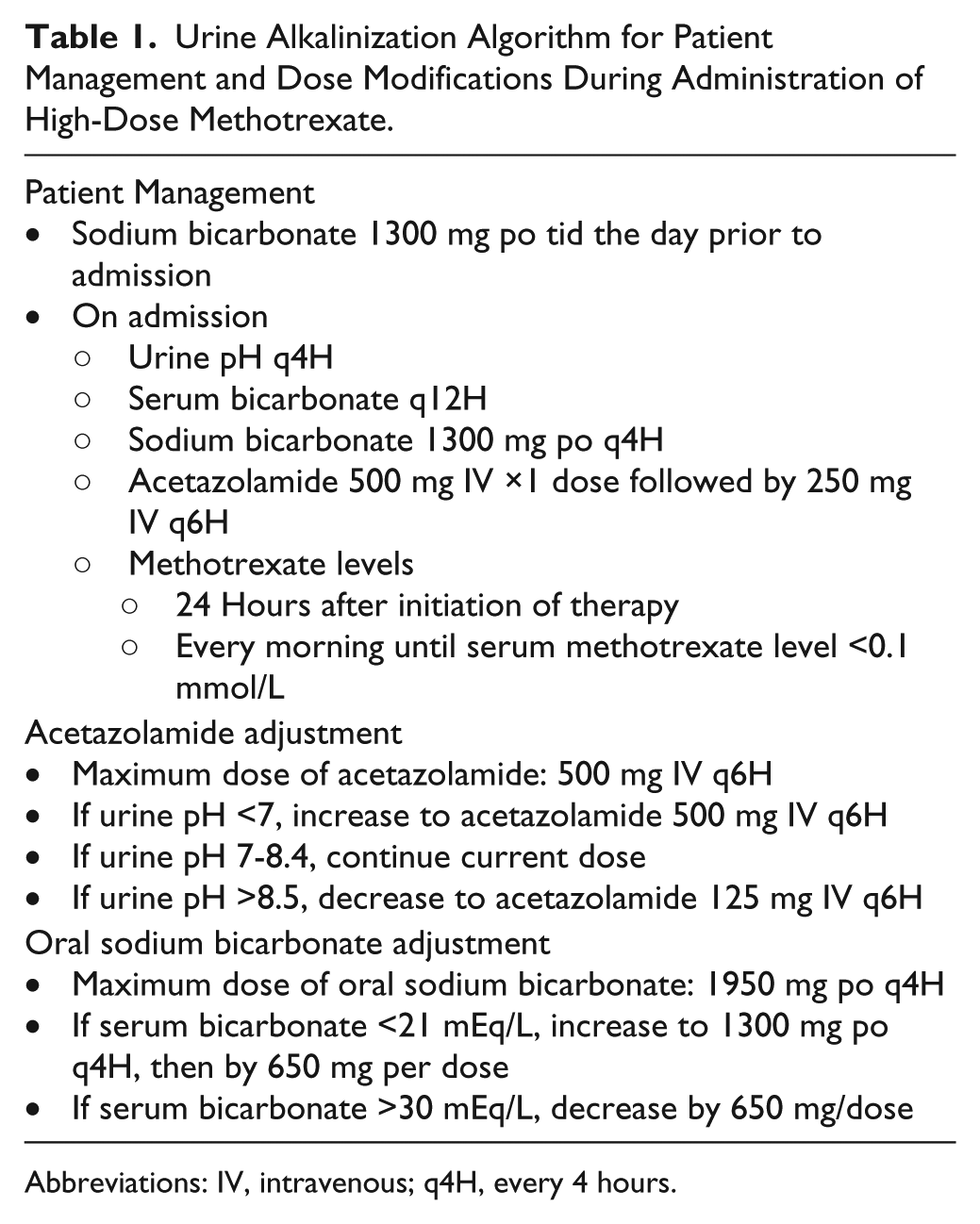
Abbreviations: IV, intravenous; q4H, every 4 hours.
Our algorithm was utilized in 1 patient on 3 separate encounters, all of which involved administration of high-dose methotrexate (8 gm/m2 IV) for primary central nervous system lymphoma. Time to urine pH ≥7 using acetazolamide was <2.5 hours allowing prompt initiation of therapy on admission. Urine pH <7 was seen once while on IV bicarbonate compared with a total of 5 times on our pilot algorithm; however, the urine pH never dropped below 6.5 on our algorithm (Table 2). The average length of stay was similar between both groups (5 days with IV bicarbonate and 4.67 days with our algorithm). No cycles resulted in elevations of serum creatinine (estimated creatinine clearance >100 mL/min before and after high-dose methotrexate administration), liver function tests, or mucositis. Additionally, we used the same algorithm for a patient with T-cell lymphoblastic lymphoma treated with hyperCVAD part B. Therapy with high-dose methotrexate (2 gm/m2 IV ×1) resulted in prompt clearance of methotrexate within 48 hours without complications (data not presented). Utilizing a maximum dose of IV acetazolamide and oral sodium bicarbonate required for these patients, wholesale acquisition drug cost comparison for 24 hours of therapy is fairly similar when comparing our algorithm ($81) with IV sodium bicarbonate ($60).
Patient’s Experience on Urine Alkalinization Protocol. a
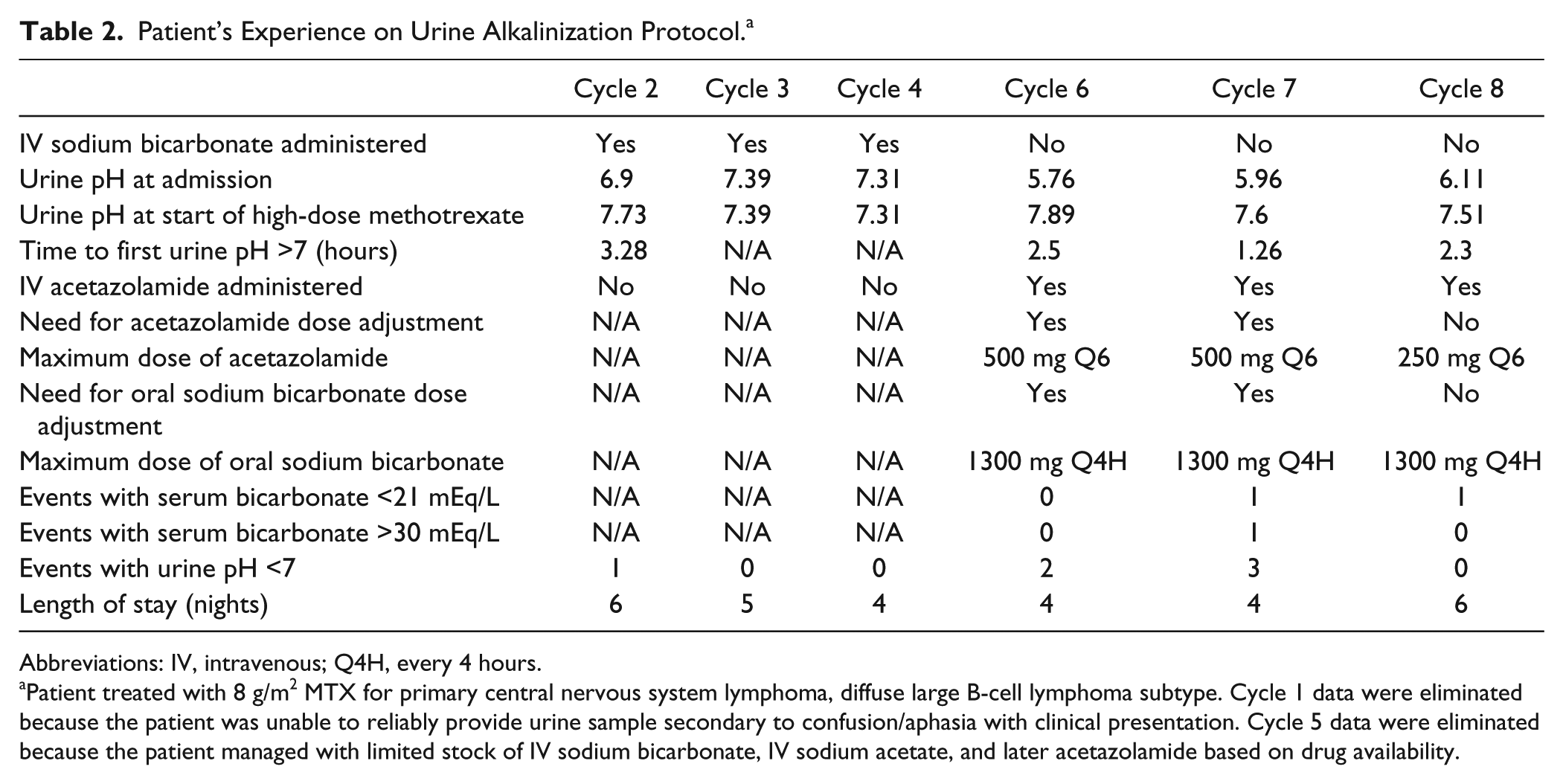
Abbreviations: IV, intravenous; Q4H, every 4 hours.
Patient treated with 8 g/m2 MTX for primary central nervous system lymphoma, diffuse large B-cell lymphoma subtype. Cycle 1 data were eliminated because the patient was unable to reliably provide urine sample secondary to confusion/aphasia with clinical presentation. Cycle 5 data were eliminated because the patient managed with limited stock of IV sodium bicarbonate, IV sodium acetate, and later acetazolamide based on drug availability.
In summary, our pilot algorithm for urine alkalization demonstrated that using IV acetazolamide with oral bicarbonate is a tolerable and effective alternative to the use of continuous bicarbonate infusion when treating patients with high-dose methotrexate. The algorithm allowed safe treatment of patients with high-dose methotrexate at our institution during a period of no access to IV bicarbonate. Our observations include prompt urine alkalization, effective control of urine pH >7, ease of administration and tolerability, and rapid reductions in plasma methotrexate concentrations. Limitation to the widespread use of acetazolamide includes metabolic acidosis, though not seen in this limited experience. Notwithstanding this limitation, our algorithm demonstrates a viable alternative to bicarbonate infusion and clearly merits further investigation.