
Abstract
Introduction
The management of HIV infection and survival rates of patients have evolved to such an extent in recent years that it is no longer considered a fatal disease but a chronic condition that can be controlled with treatment. As a result of the improved therapeutic arsenal available and better drug profiles, the life expectancy of patients with HIV infection has increased, although with a parallel increase in age-associated comorbidities. 1
In recent years particularly, the increased cardiovascular morbimortality in HIV-infected patients has generated interest and concern. Metabolic alterations such as dyslipidemia, insulin resistance, diabetes, high blood pressure, and abnormal redistributions of adipose tissue are important factors to be taken into account in the management of this type of patient. Compared with the general population, HIV-infected patients are at increased risk for cardiovascular disease (CVD). Although the exact mechanism by which vascular injury occurs is unclear, several well-known factors include a genetic component, traditional cardiovascular risk factors (CVRFs), antiretroviral treatment (ART), and variables associated with HIV infection, such as inflammatory and immunological responses, even in patients with good immune control.2-6
Although all available evidence points to an increased cardiovascular risk among HIV-infected patients, the absolute risk of CVD and myocardial infarction in young HIV-positive patients is very low. Nevertheless, as the population ages, the relative risk is also expected to increase. 7 Consequently, every effort should be made to include an evaluation of all CVRFs as a routine part of clinical practice and to intervene in those that are modifiable, always taking a multidisciplinary perspective. 8
The role of pharmacists as part of the multidisciplinary team that provides health care to HIV-infected patients and pharmaceutical care has helped improve health outcomes in this group of patients over the years. 9 At the same time, pharmaceutical care has also evolved in recent times to adapt to the new circumstances and needs of this population. 10 A new innovative strategy has been developed, using an approach based on the stratification of patients according to their needs, in accordance with their pharmacotherapeutic objectives, and supported by motivational interviews and follow-up using the new technological tools available. 11 Pharmaceutical care delivery along these lines could be useful for improving health outcomes in patients at greater cardiovascular risk. Currently, however, there are no studies that have specifically demonstrated that pharmaceutical intervention in CVRFs using this novel approach increases the number of patients who achieve the therapeutic objectives.
Aim of the Study
The aim of the study was to determine the effectiveness of an intensive pharmaceutical care follow-up program and compare it with the traditional model among HIV-infected patients with moderate or high cardiovascular risk.
Ethics Approval
The study was approved by the Andalusian ethics committee. Participants were provided with written information regarding the study and its objectives, and those who agreed to take part provided written informed consent.
Method
This was a multicenter, prospective, randomized, nonblinded study of a structured health intervention conducted between January 2014 and June 2015 with 12 months of follow-up per patient. The study was performed at 5 tertiary hospitals in Spain.
Patients
Participants were included in the study if they met the following criteria: patients with HIV infection >35 years of age; receiving active ART with at least 1 drug prescribed for the treatment of hypertension, dyslipidemia, angina pectoris, cardiovascular prophylaxis, or type 2 diabetes; and at a moderate or high risk of CVD, as measured by the Framingham risk score. 12 Patients who participated in clinical trials or who did not meet the inclusion criteria were excluded.
The sample size needed to detect a difference was calculated, assuming that the percentage of patients with high cardiovascular risk will decrease by 20%, with a statistical power of 80% and a level of statistical significance of 5%.
Study Procedures
The selected patients were randomized 1:1 to a control group or intervention group. The assignment to the different groups was done through a sequence of random numbers, generated by specific software. Patients included in the control group received the pharmacotherapeutic follow-up that was routinely applied to ambulatory care patients in the participating hospitals.
In the intervention group, intensive pharmaceutical care was provided aimed at reducing cardiovascular risk. This consisted of pharmacotherapeutic follow-up of all medication taken by the patient in order to detect and work toward the achievement of pharmacotherapeutic objectives related to cardiovascular risk and to make recommendations for improving diet, exercise, and smoking cessation. A flowchart (Figure 1) and schedule of visits (Table 1) was designed to define the pharmaceutical care intervention in terms of preventing cardiovascular risk. As additional support information, patients were given information leaflets on cardiovascular risk prevention (included information regarding smoking cessation) and an individual motivational interview to enhance this particular aspect. Finally, patients were contacted periodically by sending text messages with content related to healthy living habits and health promotion.
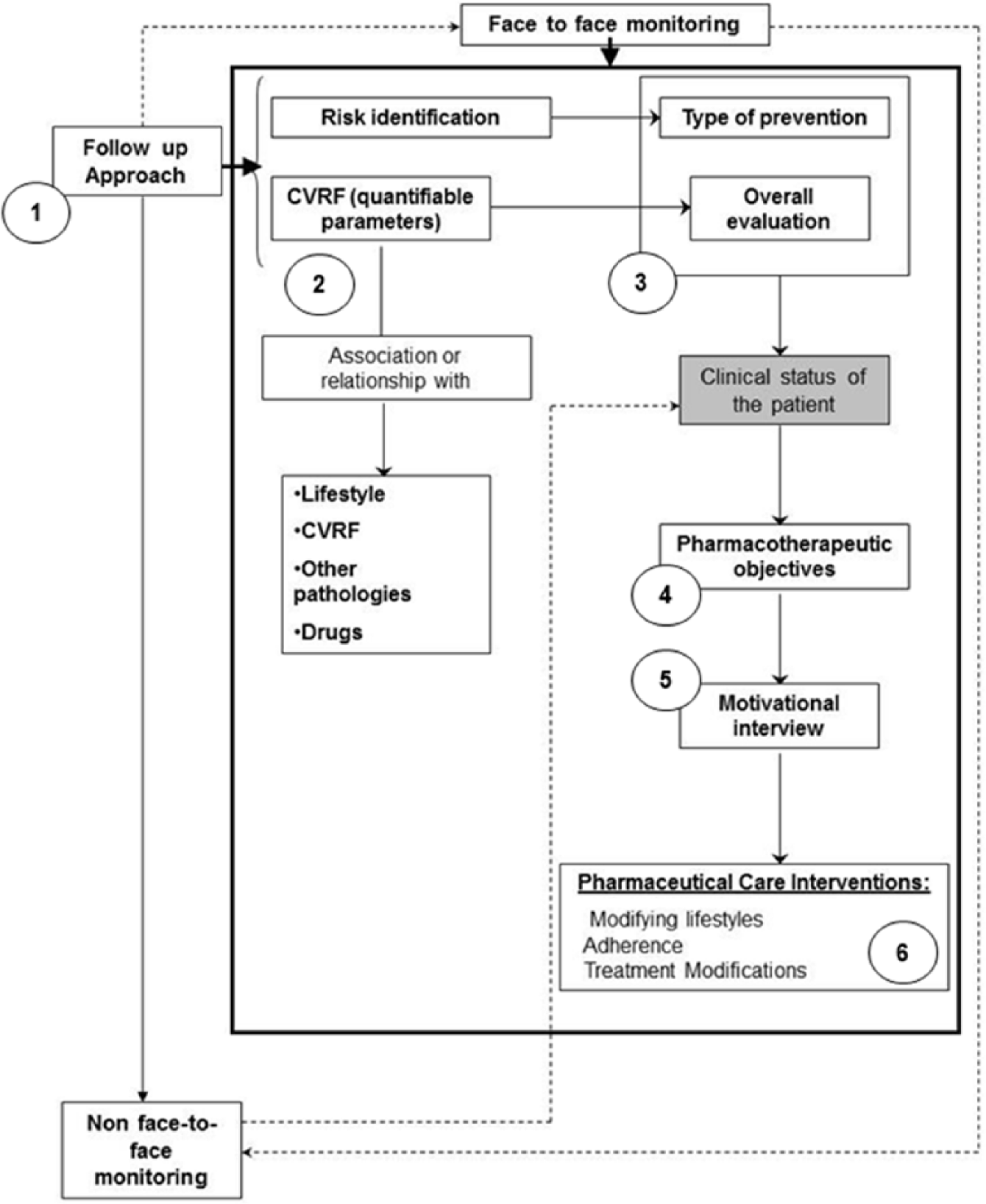
Scheme of follow-up to patients in each of the face-to-face visits and remote monitoring.
Follow-up Schedule With Variables Collected at Different Time Points During the Study.
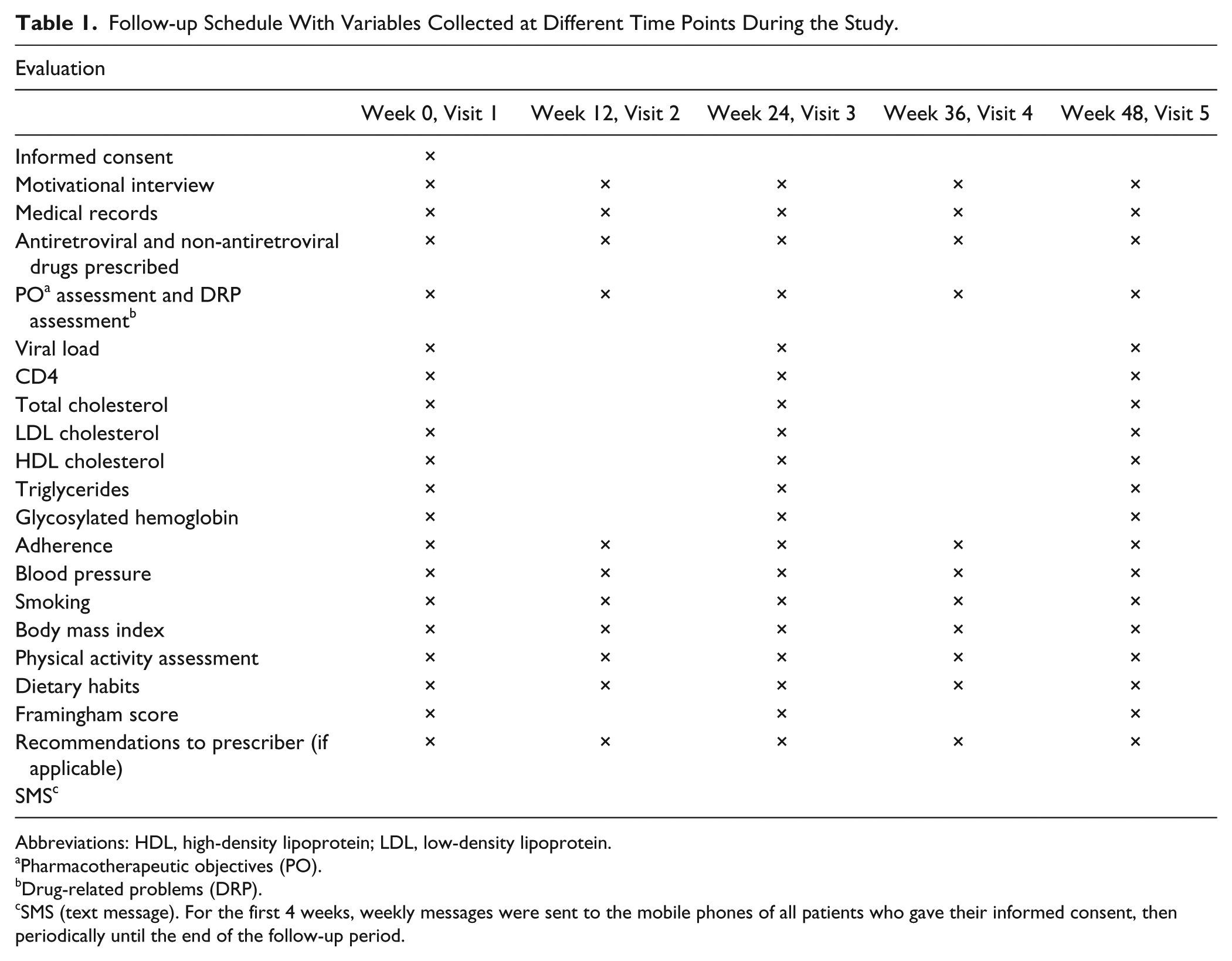
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Pharmacotherapeutic objectives (PO).
Drug-related problems (DRP).
SMS (text message). For the first 4 weeks, weekly messages were sent to the mobile phones of all patients who gave their informed consent, then periodically until the end of the follow-up period.
Patients who failed to attend 2 prearranged pharmacotherapeutic follow-up visits were withdrawn from the study and considered dropouts. These patients were not replaced by new participants in the study. The variables for which data were collected were the following: demographic (age, sex, body mass index [BMI]); lifestyle habits (alcohol use, tobacco use, dietary habits according to the KIDMED Scale, and physical activity); analytical data such as metabolic profile, plasma viral load (copies/mL), and CD4 cell count (cells/µL); and clinical variables (blood pressure) and pharmacotherapeutics, such as type of ART therapy, concomitant medications prescribed and adherence, switching treatment, and type of drug-related problem. Adherence to ART was measured with the simplified medication adherence questionnaire (SMAQ) and pharmacy dispensing records, and adherence to concomitant medication with the Morisky-Green questionnaire and pharmacy dispensing records. In both cases, patients were considered adherent, both to ART and to concomitant treatment, if they obtained a positive score using the appropriate measurement instrument. Blood pressure and BMI were measured by the hospital pharmacist.
The primary end point was calculated according to the Framingham score to estimate the 10-year risk of developing coronary heart disease. This tool included the individual risk of developing coronary heart disease, such as acute myocardial infarction, angina, or death from coronary and cardiovascular causes, including stroke, congestive heart failure, and peripheral arterial disease Analytical and pharmacotherapeutic data for the study were extracted from medical records. With respect to analytical data, if these were not available on the exact date of the visit, those closest to the date of visit were taken as reference. The rest of the required information was obtained during the interview, held during the periodic dispensing of ART medication in the pharmacy service of participating centers, and in accordance with the methodology stipulated in the study protocol. Drug-related problems were identified at each visit and classified according to the II Granada Consensus. 13
End Points
The primary end point for the study was the percentage of patients who managed to reduce the cardiovascular risk index, calculated according to the Framingham score to estimate the 10-year risk of developing coronary heart disease.
Other secondary objectives included the following: determining the mean reduction in absolute cardiovascular risk, the percentage of patients who achieved optimal blood pressure, blood lipid levels and glycosylated hemoglobin levels (according to their clinical situation); determining the mean decrease in lipid levels, blood pressure, and glycosylated hemoglobin values obtained during the study; and determining the mean decrease in BMI. Rates of patients who stopped smoking, improved sports activity, and walked regularly were assessed. Finally, the percentage of patients who increased adherence to HIV and non-HIV treatments prescribed during follow-up was also identified.
Statistical Analysis
Measures of central tendency and dispersion were calculated for numerical variables, and absolute and relative frequencies for qualitative ones. To compare whether there were measurable differences in the main numerical variables between the intervention/nonintervention groups, the Student t-test (for independent samples) was calculated. The normality of the data was checked beforehand using the Kolmogorov-Smirnov test to determine the use of parametric or nonparametric tests. In the case of qualitative variables, Pearson’s χ2 test was used. For all comparisons, a value of P <0.05 was considered to be significant. Data were analyzed using IBM SPSS Statistics version 22.0 software.
Results
A total of 53 patients were included in the study (24 in the intervention group and 29 in the control group; Figure 2). Of the patients who did not complete the study, 5 were lost to follow-up, and 1 died from causes beyond the scope of the study. In all, 90.6% were male, with a mean age of 53.6 ± 13.0 years. Variables assessed during the study, for both groups, with mean values and variations, are shown in Table 2.
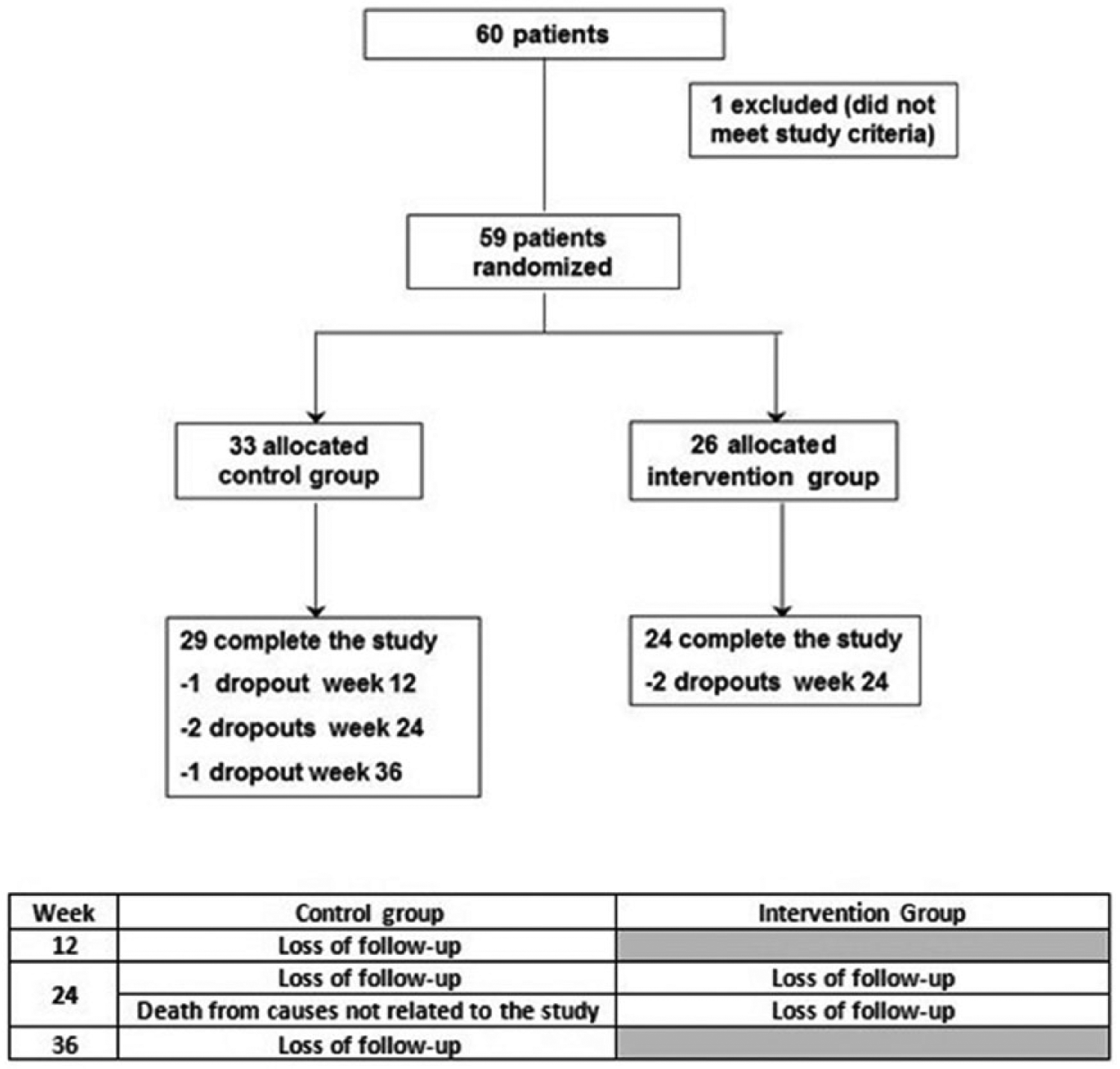
Randomization and follow-up.
Values of Variables Collected During the Study: Control and Intervention Groups.
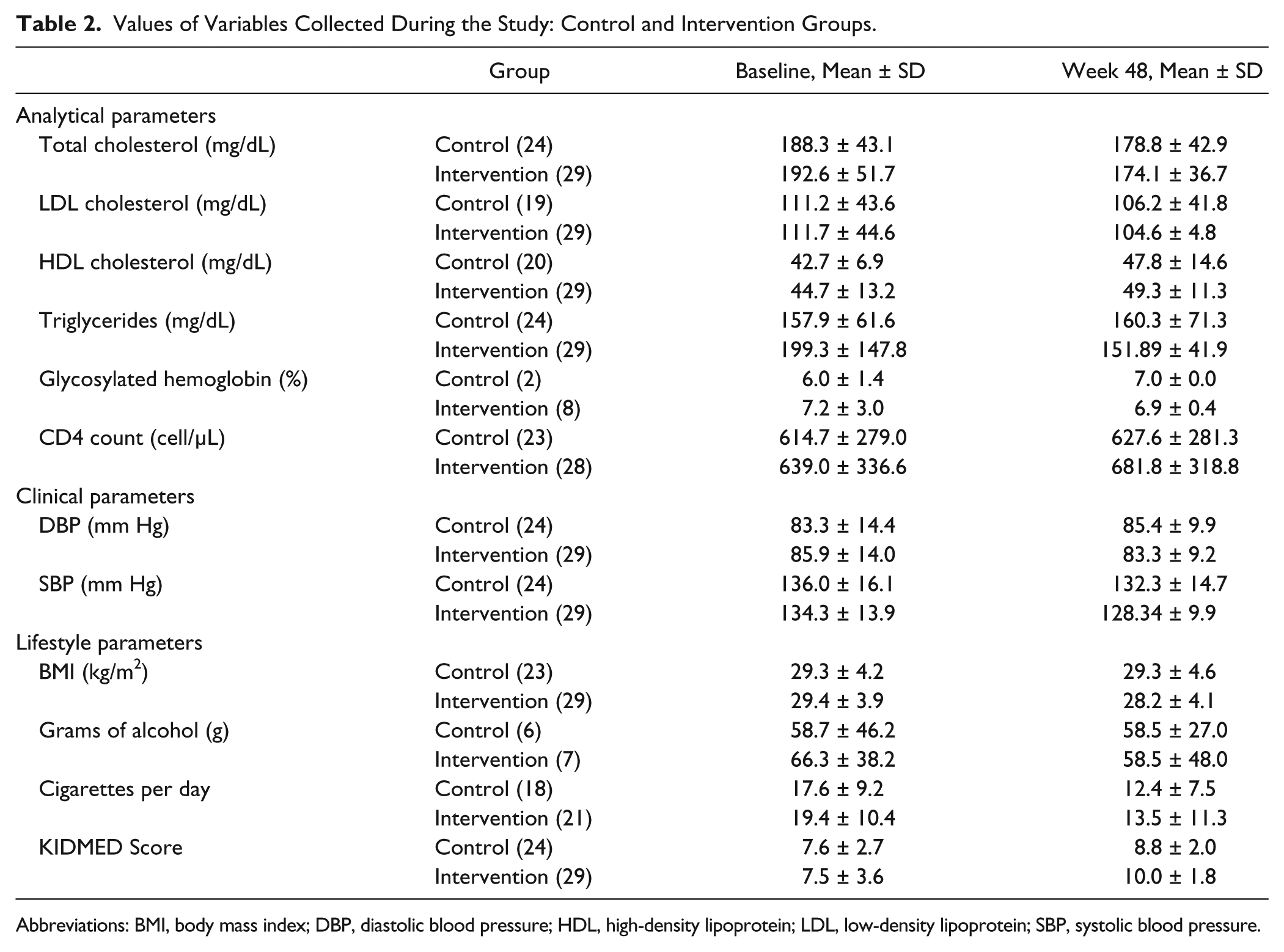
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure.
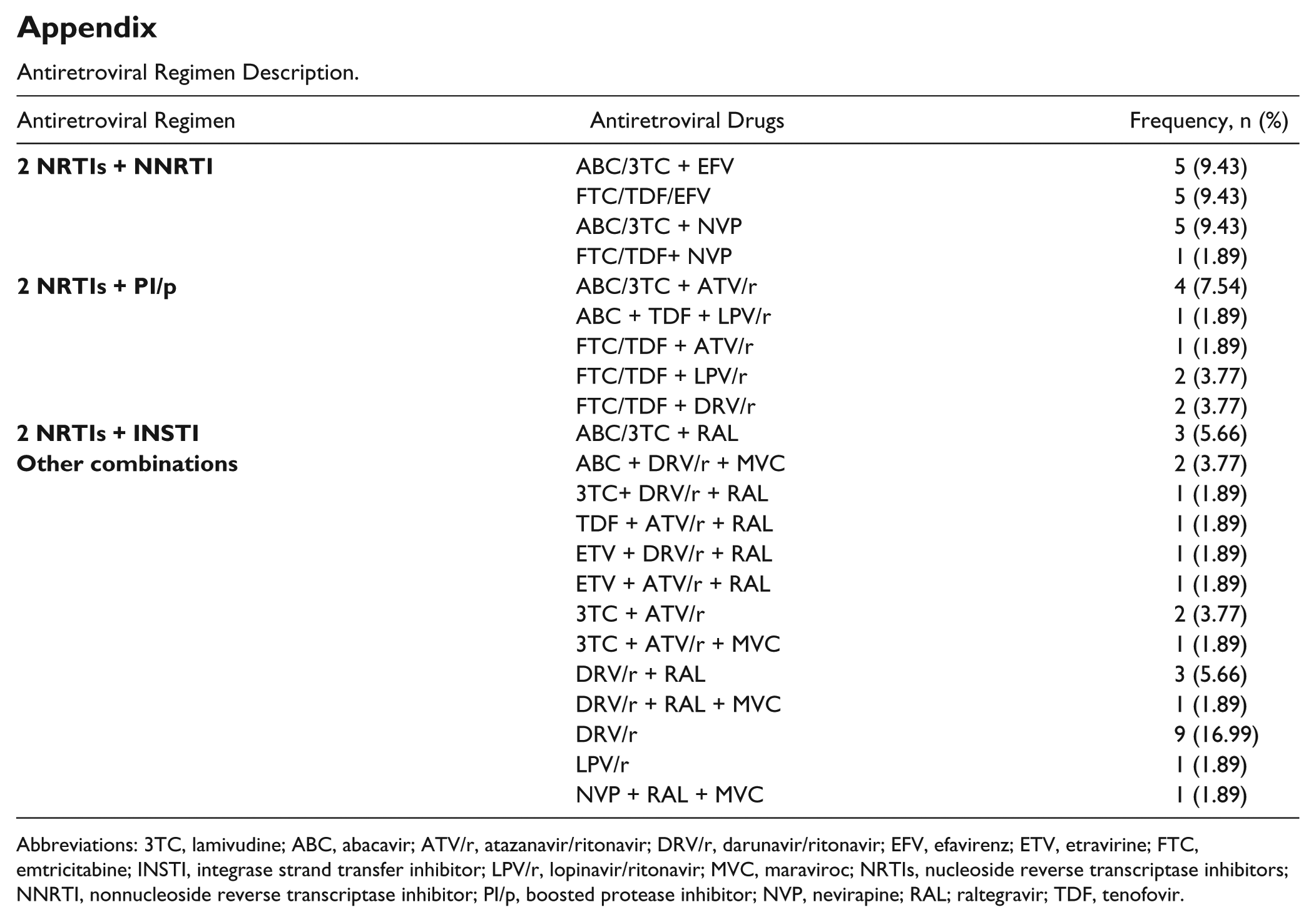
The type of ART therapy, by drug class, prescribed for the control and intervention groups, respectively, was as follows: 2 nucleoside reverse transcriptase inhibitors (NRTIs) plus a nonnucleoside reverse transcriptase inhibitor, 29.2% versus 31.0%; 2 NRTIs plus a boosted protease inhibitor, 29.2% versus 10.3%; 2 NRTIs plus an integrase strand transfer inhibitor, 0% versus 10.3%; and other combinations, 41.7% versus 48.3%; there were no statistical significant differences between the 2 groups (P > 0.05). The description of all ART regimens used is shown in the appendix. There were 8 treatment changes during the study period: 3 in the control group (1 clinical decision and 2 unknown) and 5 in the intervention group (4 clinical decisions and 1 adverse effect). The mean number of concomitant medications prescribed was 3.6 ± 2.4 in the control group and 3.4 ± 1.9 in the intervention group. The most frequently prescribed therapeutic drug classes were lipid-modifying agents (28.0%), followed by drugs for acid-related disorders (10.0%), antithrombotic agents (9.0%), oral blood glucose–lowering drugs (8.0%), anxiolytics (6.0%), β-blockers (4.0%), antidepressants (4.0%), angiotensin converting enzyme inhibitors (4.0%), and drugs belonging to other therapeutic groups (27%).
A total of 136 drug-related problems were identified during the study (60 in the control group vs 76 in the intervention group), classified as follows: 98 quantitative ineffectiveness, 16 untreated health problems, 8 caused by the effect of unnecessary medication, 5 nonquantitative unsafe, 5 quantitative unsafe, and 4 nonquantitative ineffectiveness.
The evolution of the main variables is shown in Figure 3. In the intervention group, 20.7% of patients reduced their Framingham scores from high/very high to moderate/low cardiovascular risk versus 12.5% in the control group.
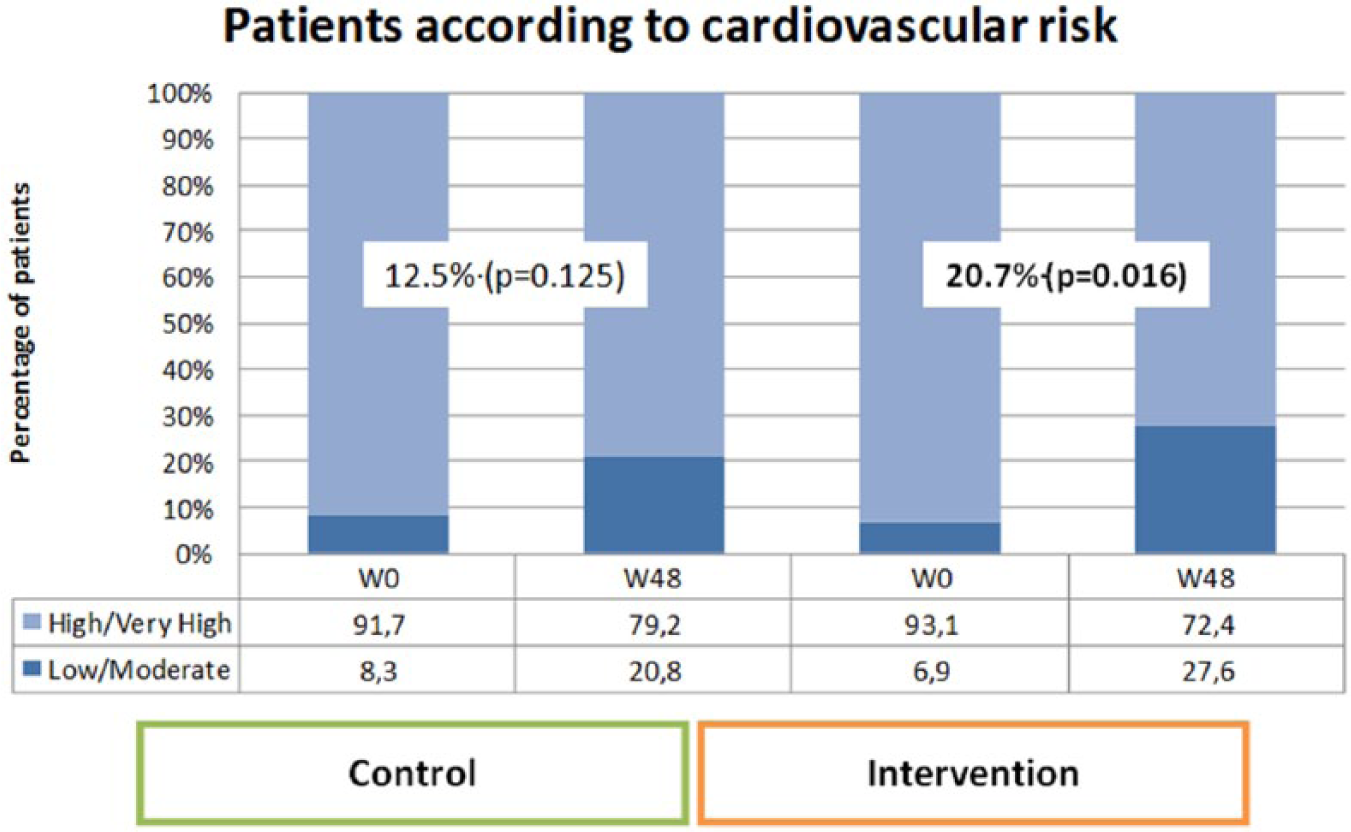
Distribution of study patients according to their cardiovascular risk.
The results for the first secondary objective of the study are shown in Figure 4. The median decrease in absolute cardiovascular risk was 1.0 points for the control group versus 1.5 points for the intervention group. Significant differences in favor of the intervention group were observed, with observable improvements starting at week 24 of follow-up (P < 0.001).
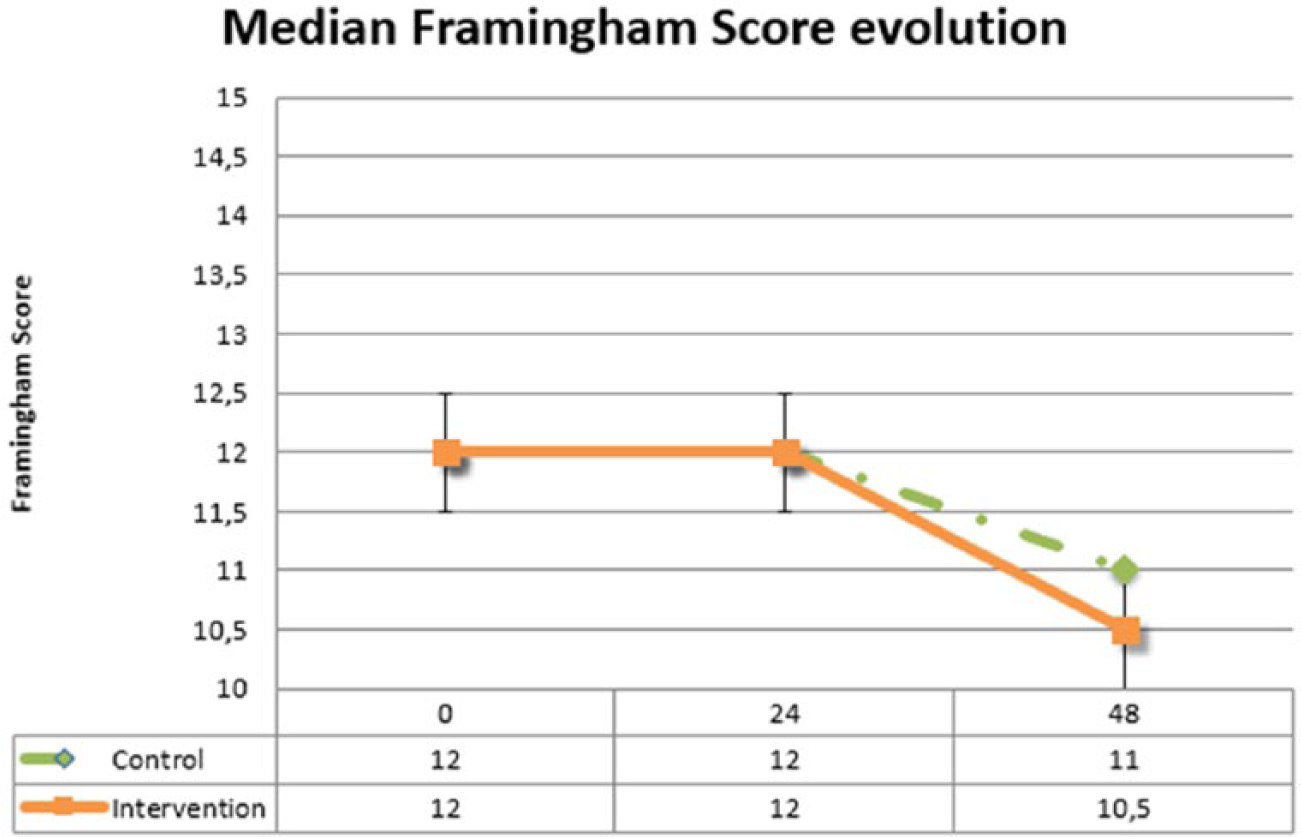
Evolution of the Framingham scores for study patients.
With respect to the remainder of the secondary objectives, the mean value of decrease in BMI was −0.05 in the control group and −1.15 in the intervention group (P < 0.001). The number of patients whose blood pressure levels were in accordance with their stated objectives increased by 32.1% (P = 0.012) in the intervention group; 37.9% of patients overall stopped smoking in the intervention group (P = 0.001) versus 12.5% in the control group. In terms of number of cigarettes, patients in the intervention group reduced the mean number of cigarettes smoked by 12 cigarettes per day and control patients by 8 per day. At 48 weeks, the number of patients in the intervention group who went for regular walks as a healthy habit increased by 38.0% (P = 0.003). Finally, at week 48, concomitant medication adherence among intervention patients was 87.7% overall, with a 39.4% increase in adherence at the 48-week follow-up compared with baseline (P = 0.002). Other variables included in the study are shown in Table 3. Because of the low number of diabetic patients, glycosylated hemoglobin was not included in the analysis.
Evolution of the Variables Evaluated for the Secondary Objectives of the Study (Percentage of Patients Who Achieved the Different Objectives).
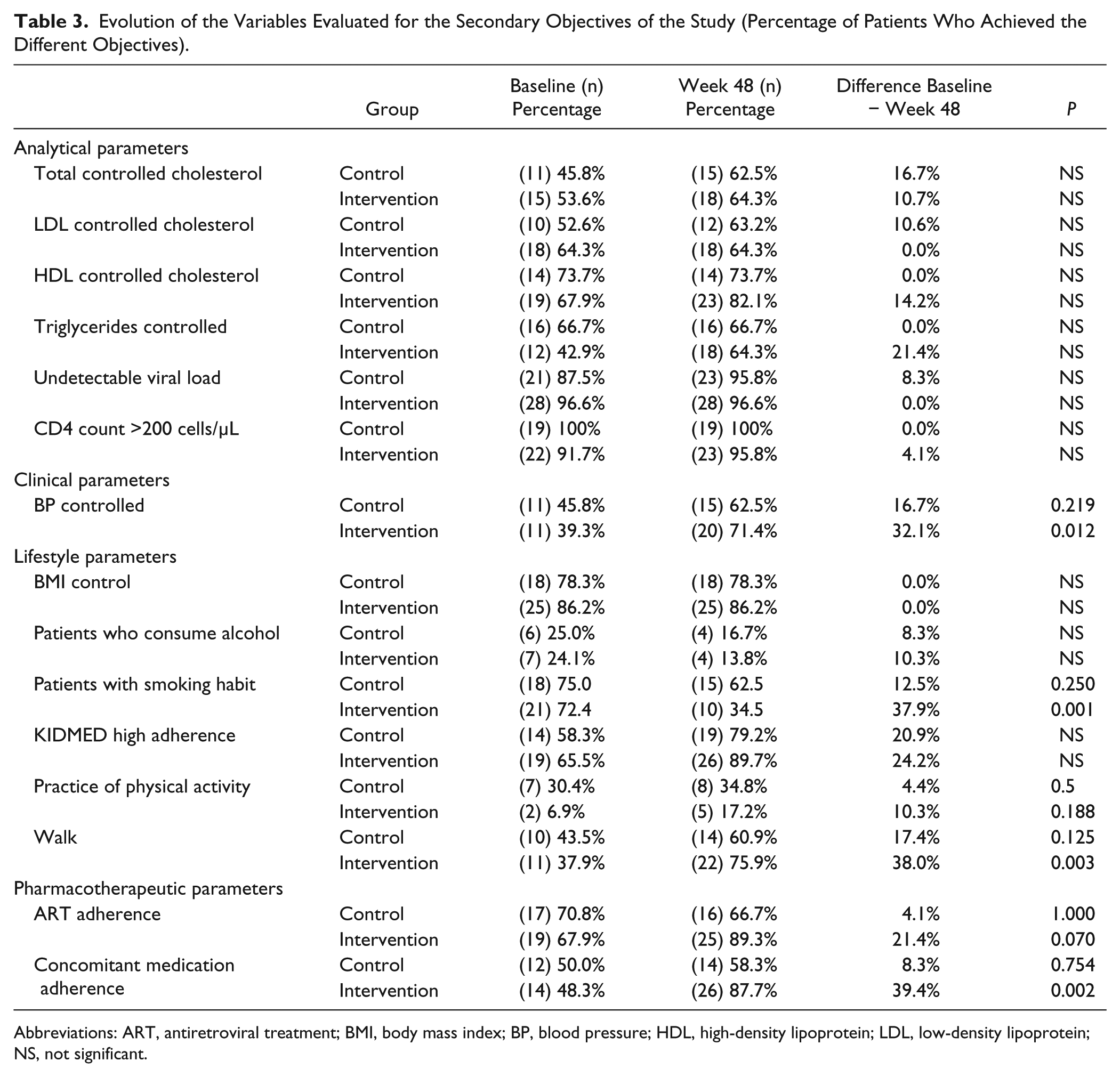
Abbreviations: ART, antiretroviral treatment; BMI, body mass index; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NS, not significant.
Discussion
The present study demonstrated that an intensive pharmacist-led follow-up, based on patient stratification, motivational interview techniques, and use of new technologies, helped improve the cardiovascular risk of HIV-infected patients, especially those at greatest risk of CVD.
Our results are similar to those published by Domingues et al, 14 who also found that a 12-month follow-up improved the cardiovascular risk profile of HIV-infected patients, although exclusively those >50 years old. Their study had 2 fundamental limitations that have been overcome by our study design and the results presented here. First, it was performed in a single cohort of patients from 1 hospital only, and second, there was no control group and no patient randomization. Our research design took both these aspects into account.
Although our study found statistically significant improvements in the main variable and certain secondary variables, the clinical relevance of the improvement obtained should be interpreted with caution because, to be prudent, it should be correlated with an improvement in long-term health outcomes.
Over the years, different studies have provided support for a positive association between the involvement of the HIV pharmacist and improvements in different health outcomes in HIV patients. These outcomes include ART adherence, viral load suppression, reductions in the use of medical resources (hospitalization, doctor’s visits, number of hospital days, visits to the emergency department), and pill burden and inappropriate discontinuation of outpatient medications as well as improved inpatient documentation of medication at home and accuracy of ART dosing. 9
The traditional pharmaceutical care model includes a large number of recommendations by pharmacists, which have typically been accepted by the doctor or health care team. Traditional standard of care for HIV patients was based on providing pharmaceutical care at the beginnings or at treatment discontinuation, the identification of drug-related problem, and the enhancement of adherence. 15 Most of the pharmacist’s functions involve ART dosing, detecting drug interactions or adverse reactions, providing information about the drug, ART adherence counseling, and training on the use of adherence enhancement tools. 16
This study suggests that the contribution of the HIV pharmacist in this area is also positive and may have a favorable impact on the clinical evolution of this type of patient. HIV-infected individuals are at increased risk of cardiovascular events, and some experts advocate including HIV infection as an independent risk factor for CVD. The effects of ART therapy on lipid profiles and the potentially increased risk of cardiovascular events must be taken into account when selecting treatment for HIV-infected individuals. There is increasing evidence that chronic immune activation and inflammation play a role in the pathogenesis of CVD in the context of HIV infection. 17
A large number of cohorts of HIV-infected patients worldwide have shown that the prevalence of modifiable risk factors remains high, especially smoking and dyslipidemia, the latter resulting mainly from low levels of high-density lipoprotein cholesterol and the increase in total cholesterol. However, age is the main determinant of high cardiovascular risk assessed using risk scales. As the HIV-infected population gradually ages, CVD is expected to become progressively more significant over time, and so the control of modifiable risk factors will be crucial for preventing the development of future complications.18,19 For this reason, regular coronary heart disease and/or CVD risk assessment should be performed on patients with HIV, especially during ART therapy.8,20 This should also be taken into consideration when outlining what sort of pharmaceutical care should be given to different types of patients in follow-up 21 because, as we have seen, the study achieved improvements in determinants of health such as stopping smoking and improving diet and exercise. With respect to pharmacotherapy, the risk of non-adherence to prescribed concomitant treatment is especially important, particularly in dyslipidemia, because it has been observed that, in this kind of patient, increased pharmacotherapeutic complexity is directly related to lower achievement of pharmacotherapeutic objectives. 22
This study identified that the main drug-related problem of this kind of patient was to use a lower dose or treatment regimen than was needed, and it is important, therefore, to stress the importance of taking all the prescribed medication correctly, not just the ART, and to inform patients of the objectives of concomitant medication. The high prevalence of comorbidities associated with cardiovascular risk and ineffective pharmacological control are the main risk factors for CVD. 23 The study by Neto et al 24 demonstrated that a pharmaceutical care program gives better clinical measurements and reduced cardiovascular risk scores in elderly diabetic and hypertensive non-HIV patients over a 36-month period.
Various studies have shown the importance and possible consequences of inflammation associated with HIV infection in atherogenesis and suggest that certain biological markers of inflammation, endothelial activation, and thrombosis may be useful for assessing risk and predicting preclinical atherosclerosis. 8 However, because these factors were not available in all participating studies, it was not possible to incorporate them into the analysis.
Our study has certain limitations, including those related to the individualization of interventions. Text messages sent to patients were not individualized, and the same information was sent to all patients regardless of other characteristics and their evolution. Also, given the characteristics of the study design, it was not possible to correlate the improved results in the main variable with patient survival, for which a longer follow-up period would be necessary.
Certain problems with recruitment prevented us from obtaining a large sample size. Therefore, this study should be taken as a proof of concept. A study with a larger sample size is necessary to extrapolate these results. Although other studies used other cardiovascular risk assessment indexes, such as SCORE and REGICOR, our study considered the Framingham score exclusively. This tool was used universally to assess the follow-up of all patients participating in the study. It is important to recognize, however, that none of the risk equations includes variables associated with HIV infection able to influence cardiovascular risk, such as degree of viral replication, proinflammatory status, and associated immune activation.
Taking the positive results into account, subsequent studies will enable us to determine whether individualized risk assessment and the use of new information and communication technologies as well as learning and knowledge technologies based on visual information and sharing of emotions between individuals in the same clinical situation will improve the health outcomes of patients of this type.
Conclusion and Relevance
In conclusion, the pharmaceutical care model presented in this study could improve the health outcomes of HIV-infected patients at greater risk of CVD and should therefore become standard in follow-up care.
HIV patients are aging and, thus, have several comorbidities. However, for many reasons, clinical practice does not usually include the evaluation of all CVRFs and intervenes in those that can be modified. It is necessary to define new models of pharmaceutical care approaching this aspect always from a multidisciplinary perspective. In conclusion, the pharmaceutical care model presented in this study, led by the hospital pharmacist, based on the stratification of patients according to their needs, in accordance with their pharmacotherapeutic objectives, and supported by motivational interviews and follow-up using the new technological tools available, might lead to improved health outcomes in HIV+ patients at greater cardiovascular risk.
Footnotes
Appendix
Antiretroviral Regimen Description.
| Antiretroviral Regimen | Antiretroviral Drugs | Frequency, n (%) |
|---|---|---|
|
|
ABC/3TC + EFV | 5 (9.43) |
| FTC/TDF/EFV | 5 (9.43) | |
| ABC/3TC + NVP | 5 (9.43) | |
| FTC/TDF+ NVP | 1 (1.89) | |
|
|
ABC/3TC + ATV/r | 4 (7.54) |
| ABC + TDF + LPV/r | 1 (1.89) | |
| FTC/TDF + ATV/r | 1 (1.89) | |
| FTC/TDF + LPV/r | 2 (3.77) | |
| FTC/TDF + DRV/r | 2 (3.77) | |
|
|
ABC/3TC + RAL | 3 (5.66) |
|
|
ABC + DRV/r + MVC | 2 (3.77) |
| 3TC+ DRV/r + RAL | 1 (1.89) | |
| TDF + ATV/r + RAL | 1 (1.89) | |
| ETV + DRV/r + RAL | 1 (1.89) | |
| ETV + ATV/r + RAL | 1 (1.89) | |
| 3TC + ATV/r | 2 (3.77) | |
| 3TC + ATV/r + MVC | 1 (1.89) | |
| DRV/r + RAL | 3 (5.66) | |
| DRV/r + RAL + MVC | 1 (1.89) | |
| DRV/r | 9 (16.99) | |
| LPV/r | 1 (1.89) | |
| NVP + RAL + MVC | 1 (1.89) |
Abbreviations: 3TC, lamivudine; ABC, abacavir; ATV/r, atazanavir/ritonavir; DRV/r, darunavir/ritonavir; EFV, efavirenz; ETV, etravirine; FTC, emtricitabine; INSTI, integrase strand transfer inhibitor; LPV/r, lopinavir/ritonavir; MVC, maraviroc; NRTIs, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI/p, boosted protease inhibitor; NVP, nevirapine; RAL; raltegravir; TDF, tenofovir.
Authors’ Note
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was awarded €15 000 in the call for aid for working groups of the Spanish Society of Hospital Pharmacy (SEFH) in 2012.