
Abstract
Background
Telemedicine, defined by the American Telemedicine Association (ATA) as “the remote delivery of health care services and clinical information using telecommunications technology” can provide the opportunity for improvements in patient outcomes. 1 Health care professionals have utilized telemedicine to bridge the gap between patients and optimal health care by performing interactive physician visits remotely, providing patients the ability to view laboratory values online, and building alert systems to prompt bedside evaluations. Medication management might be enhanced with telemedicine or mobile technology to provide counseling services or to enhance medication adherence.2,3 Pharmacists are embracing this novel health care approach to aid in providing patient-centered care for safe and effective medication use.
Telepharmacy is a subset of telemedicine and defined by the Model State Pharmacy Act and Model Rules of the National Association of Boards of Pharmacy as “the provision of pharmacist care by registered pharmacies and pharmacists located within U.S. jurisdictions through the use of telecommunications or other technologies to patients or their agents at distances that are located within U.S. jurisdictions.”4(p e236) Telepharmacy has been instrumental in the outpatient setting to improve outcomes such as increased access to care in rural areas, patient satisfaction with chronic disease state management, and medication adherence. 3 However, the application of telepharmacy services in the acute care setting, including both intensive care units (ICUs) and non-ICUs, is not clear because of differing patient needs, monitoring parameters, and medication use and greater risk of medication-related events. 5 For example, TeleICUs, or “network of audiovisual communication and computer systems that provide the foundation for a collaborative, interprofessional care model focusing on critically ill patients”6(p 972) are growing in number, but lack long term data.6,7 It is, therefore, likely that the structure of inpatient telepharmacy services and pertinent outcomes also differ. Telepharmacy in the ICU poses an additional opportunity to work collaboratively within a clinical team and provide consistent pharmacy expertise to expand continuity of evidence-based patient care in line with clinical model guidelines.6,7
Despite limited data regarding inpatient telepharmacy, stakeholders are interested in implementing these technologies. During the assessment of 58 systematic reviews concerning telemedicine services, the Agency for Healthcare Research and Quality identified mortality and quality of life benefits but emphasized the paucity of corresponding reviews within the inpatient setting and consequent lack of understanding of its impact in this environment. 8 The American Society of Health-System Pharmacists has also recognized and made a push to strengthen telepharmacy services in its incorporation of the Practice Advancement Initiative. 4 The purpose of this systematic review of telepharmacy services in the acute care setting is to broadly define the effect, highlight opportunities for pharmacists, and compare the different services offered in both general wards and ICUs.
Methods
Adhering to the PRISMA guidelines for a systematic review, the authors set out to identify articles that fit the population, intervention, comparison, and outcome (PICO) question as follows: What impact does the provision of inpatient clinical pharmacy services delivered via telemedicine technologies have on patient outcomes compared with standard of care? EMBase, MEDLINE (via PubMed), and SCOPUS databases were reviewed with the search terms telepharmacy or telehealth or telemedicine or telephone and either pharmacist or pharmacy.
This search includes data from the inception of databases to April 2018 and was conducted in 2 phases, as depicted in Figure 1. Titles and abstracts selected from the initial search of all studies were reviewed for appropriateness and bias using the Risk of Bias in Non-randomised Studies—of Interventions (ROBINS-I). 9 Articles were included in this review if they were written in English, utilized telemedicine technologies (as defined by ATA), and incorporated a pharmacist in a capacity beyond the traditional roles of medication dispensing or preparation. Publications were excluded if they did not include patient interaction or care and if they did not take place in an inpatient setting (eg, occurred solely in clinics or community pharmacies and/or referenced medication therapy management). Studies were also excluded if they did not report a comparator, defined as previous standard of care and/or baseline statistics. Titles and abstracts were then reviewed, and the remaining articles were read in full. Extraction of relevant information, particularly facility setting, type of communication platform used, participants involved with the intervention, a description of the intervention, comparator group, brief summary of outcomes, and study design was done manually. Additional comments were made when necessary to provide context and clarity. Both phases of review were completed by 2 independent reviewers. Discrepancies in selection were resolved by discussion between reviewers until consensus was reached. A meta-analysis was planned a priori but was not performed because of heterogeneity of the included studies. The authors did not obtain any funding for the production of this systematic review and have no financial or nonfinancial conflicts of interest to disclose.
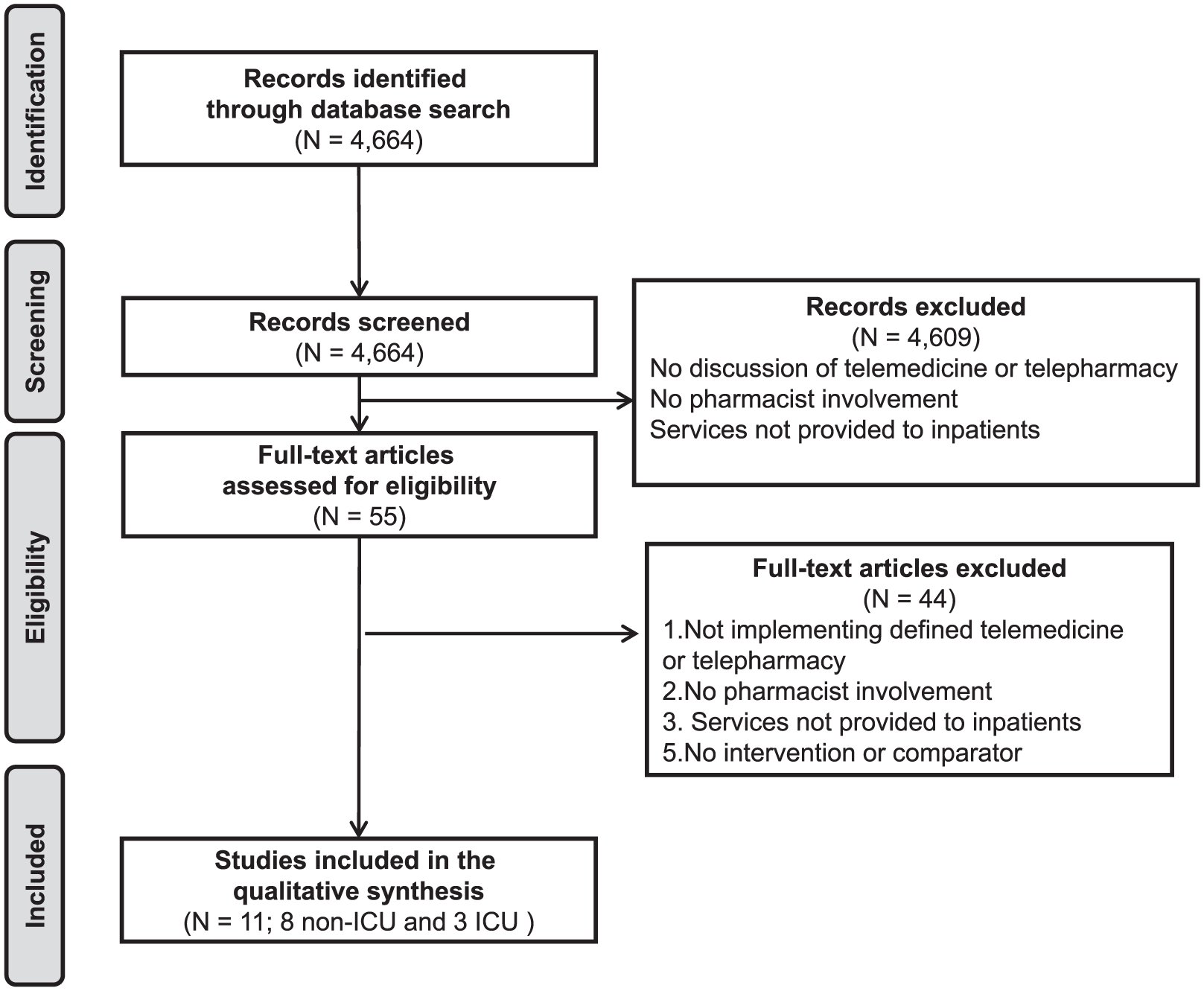
PRISMA flow diagram describing study selection process.
Results
A total of 4423 articles were retrieved from the databases. After applying the PICO question and inclusion criteria, 11 articles were ultimately included in this review (Figure 1). Overall bias was assessed as either low (n = 1), moderate (n = 9), or serious (n = 1), but no studies fell in the range of critical. All these articles involved inpatients with 3 (27.3%) specifically including patients within an ICU. Seven studies (63.6%) included patients from institutions self-identified as rural, community, or critical access hospitals, and 1 (9.1%) took place in a long-term acute care hospital.
Telepharmacy staff received information (Tables 1 and 2)10-20 either by remote access to the electronic medical record (n = 4), faxed or scanned documents (n = 2), picture/webcam (n = 1), or some combination (n = 4). On the other end, communication between telepharmacists and institutional personnel was conducted either by email/electronic communication or facsimile (n = 2), video/picture review (n = 1), telephone (n = 1), some combination (n = 6), not explained (n = 1). Studies were mostly prospective and observational in design (n = 8), but also included interrupted time series analyses (n = 1), prospective proof-of-concept (n = 1), and retrospective cross-sectional (n = 1) studies.
Articles Included in Systematic Review, ICU Setting.
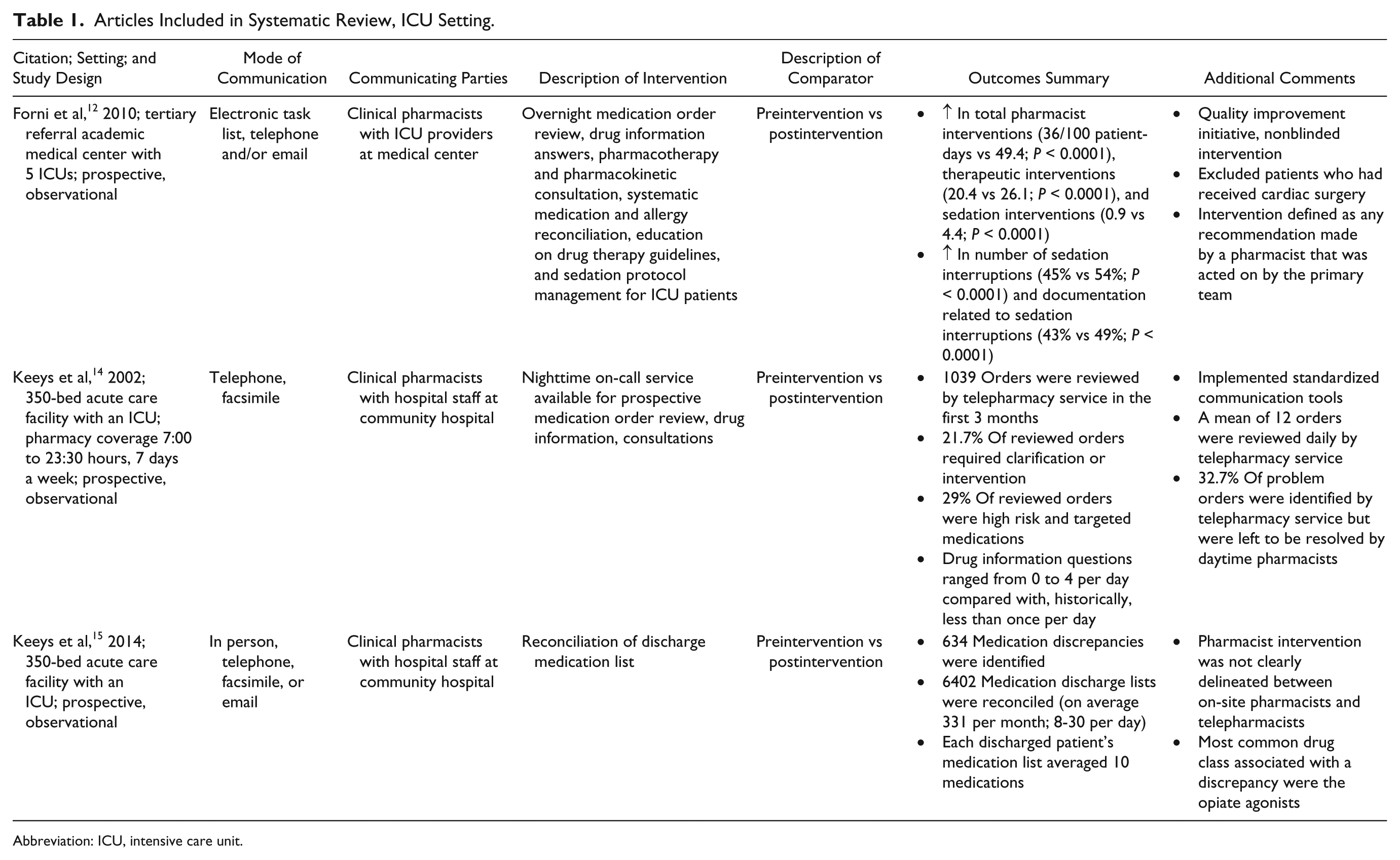
Abbreviation: ICU, intensive care unit.
Articles Included in Systematic Review, non-ICU Setting.
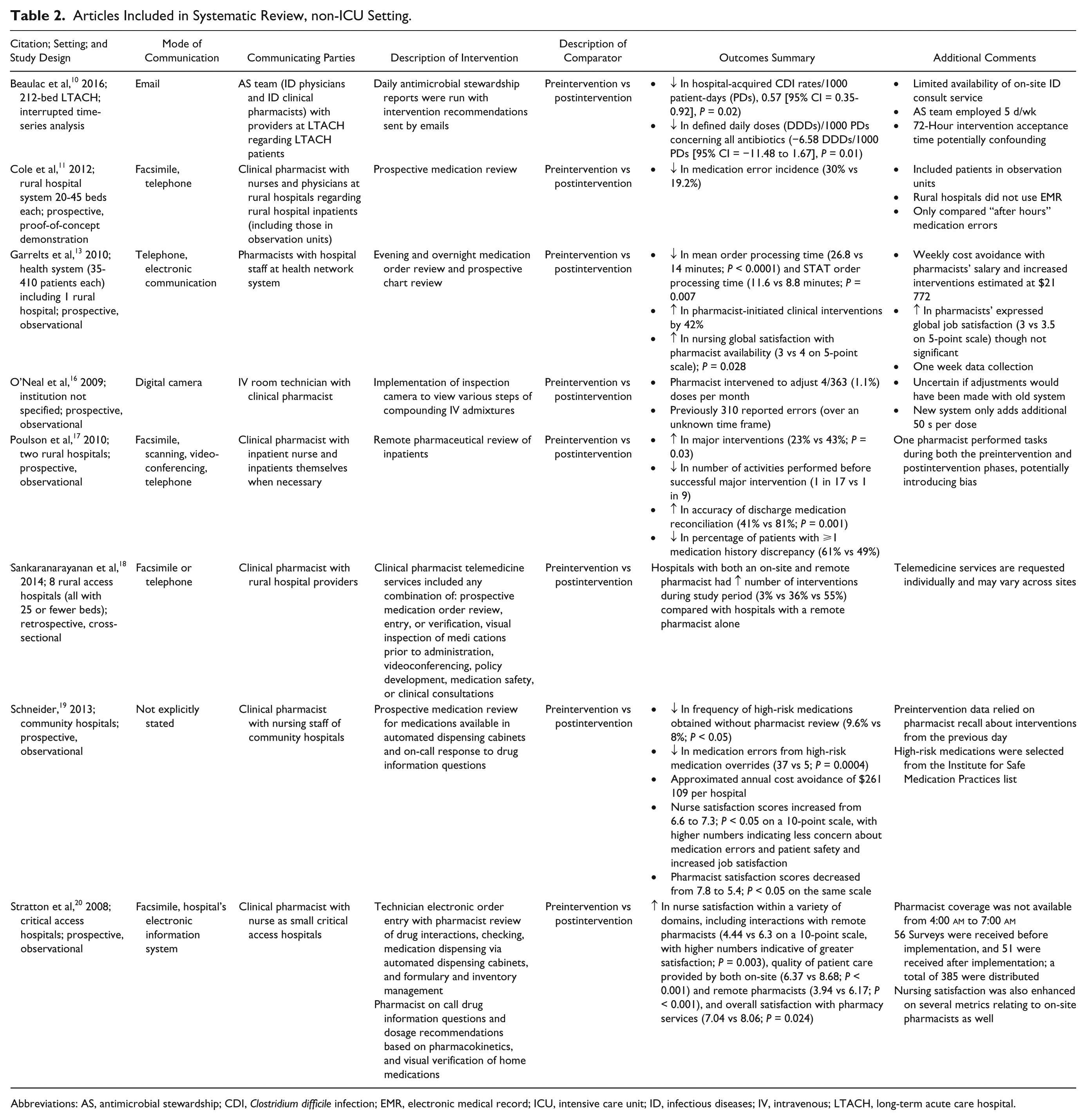
Abbreviations: AS, antimicrobial stewardship; CDI, Clostridium difficile infection; EMR, electronic medical record; ICU, intensive care unit; ID, infectious diseases; IV, intravenous; LTACH, long-term acute care hospital.
Table 1 provides detailed information included in the 3 articles containing patients within the ICU. Two of these studies identified direct benefits to inpatient care during their stay.12,14 One study 12 demonstrated that during these times, the number of pharmacist interventions (broadly defined as any recommendation made by a pharmacist that was acted upon), therapeutic interventions (defined as any intervention relating to medication management), and sedation interruptions were all increased. Another study of nighttime telepharmacy services 14 pointed out that more than 20% of orders reviewed required clarification or pharmacist intervention, and nearly 30% of all orders were classified as either high risk or targeted medications.
Table 2 provides detailed information included in the remaining 8 articles involving general ward patients. One study, through the introduction of remote antimicrobial stewardship, decreased hospital-acquired Clostridium difficile infections and defined daily doses of antimicrobials. 10 Other studies used remote order verification that decreased medication error incidence,11,16,19 mean order processing time, 13 and medication cost. 19 These same remote services also demonstrated an increased pharmacy-based clinical intervention rate,13-18 medication history and discharge completion and accuracy, 17 and cost avoidance between $21 772 weekly 13 and $261 109 annually. 19 Nursing satisfaction with telepharmacy was enhanced,13,19,20 but pharmacist satisfaction was mixed.13,19 One study suggested that telepharmacists benefited hospitals with current pharmacists on staff by providing care that was even more patient centered. 18
Discussion
The applicable studies that have effectively used a comparator to assess patient-centered outcomes have demonstrated a positive impact of telepharmacy for a variety of outcomes in a diverse collection of inpatient settings. Notably, telepharmacists in the ICU setting were able to expand on existing services. For example, remote telepharmacists expanded pharmacist coverage throughout the overnight hours. Critically ill patients require intensive care around the clock. Pharmacists aid with this care, most commonly during first and second shifts, but it stands to reason that they can also do so during the overnight hours when patients remain critically ill. Pharmacist care can also be operationalized, as performing interventions and assisting with protocol review. In the non-ICU setting, telepharmacists were able to improve patient outreach, particularly to remote areas. In understaffed or underserved areas, off-site pharmacists implemented services previously not provided to these institutions. Examples include antimicrobial stewardship, prospective medication review, and discharge medication reconciliation. These services were also completed during off hours where on-site pharmacists may not be physically present. Overall, the use of telepharmacy services may be further explored following the Health Information Technology for Economic and Clinical Health (HITECH) Act as well as expansion of electronic health records and growing interoperability.
From a nursing perspective, remote access to pharmacists and the use of telepharmacy demonstrated self-reported improvements in job satisfaction.13,14,19,20 The authors of these studies commented that nurses felt more comfortable when traditional pharmacist tasks they were asked to perform were designated to the telepharmacist instead. Pharmacists had some mixed reviews on their job satisfaction for unclear reasons but were mostly in favor of the additional service.14,19,20
Benefits from the use of telepharmacy were maintained at institutions that already employed on-site clinical pharmacists. One study specifically demonstrated a net benefit of interventions at hospitals that employed both on-site and remote pharmacists. 18 With this structure, off-site pharmacists are able to free up on-site pharmacists to complete other tasks, such as providing enhanced patient care, serving on hospital committees, and educating future students and practitioners. This example suggests that telepharmacy can benefit hospitals with varying pharmacy staff resources.
Justifying the cost of an added on-site pharmacist is a major barrier that can be exacerbated in remote areas struggling to retain or obtain the services of full-time pharmacists. 11 This review identified both indirect and direct cost savings gained through the use of telepharmacy (Tables 1 and 2), which may make pharmacist utilization slightly more feasible. Another barrier cited to the implementation of telepharmacy is that of purchasing and implementing the necessary technology. 13 These factors were not apparent because the studies reviewed predominantly relied on remote access to the local institution’s electronic health record, and communication was primarily driven by fax, email, or telephone. Demonstrated cost savings to an institution provide the fiscal backing for the implementation of telepharmacy. One final concern that is beyond the scope of this article is the potential for malpractice and violation of pharmacy law. More specifically an added risk, such as communication errors, is introduced into an already hectic work environment. There is little precedent relating to such possible malpractice claims. 21
Use of the ROBINS-I tool demonstrated varying degrees of potential bias among the studies, as depicted in Table 3. This tool, specifically designed for nonrandomized studies follows a structured assessment of 7 key domains to determine if there is the potential for bias at either the preintervention, at intervention, or postintervention phase. It is likely, though not confirmed, that any bias would favor a positive result and demonstrate a stronger benefit of telepharmacy. Taking into account that this bias assessment was subjective, it should not take away from the overall conclusions.
Bias Assessment of Articles Included in Systematic Review. a
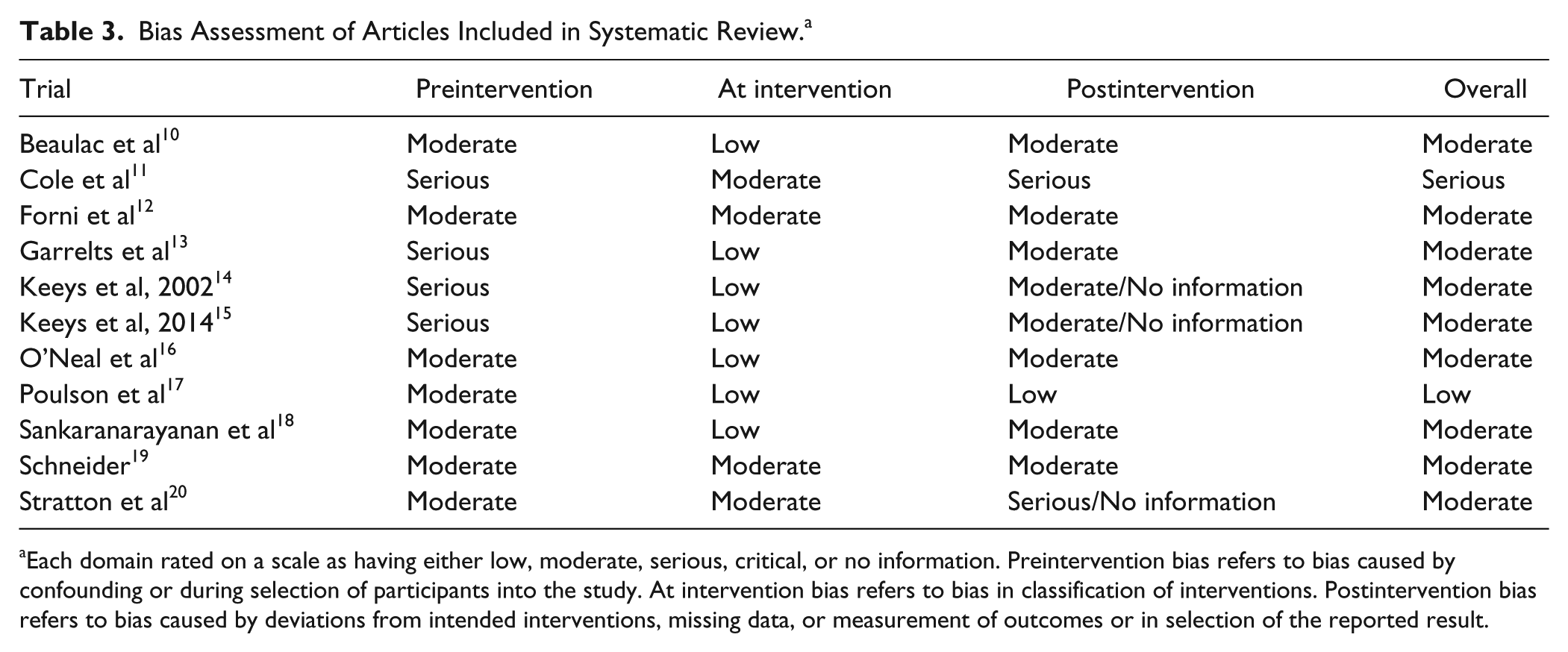
Each domain rated on a scale as having either low, moderate, serious, critical, or no information. Preintervention bias refers to bias caused by confounding or during selection of participants into the study. At intervention bias refers to bias in classification of interventions. Postintervention bias refers to bias caused by deviations from intended interventions, missing data, or measurement of outcomes or in selection of the reported result.
There were several limitations to the studies reviewed. Primarily, the majority of these studies were retrospective and small in nature making broad-scale conclusions potentially difficult to ascertain. The heterogeneity of these studies and telepharmacy operations may have also compounded the comparison difficulty and potential impact of inpatient telepharmacy. On the other hand, there is a risk of publication bias because these studies had predominantly positive results. Assessment methods included nonspecific outcomes such as “interventions” or “discrepancies” that may not necessarily share the same definition across studies or institutions.
Additionally, there are possible limitations associated with the search terms used to capture trials for inclusion in this review. Terms such as remote pharmacy or remote dispensing were used in some studies but were not identified a priori in our search. A large number of studies were excluded because they failed to meet the designed PICO question. It is possible that the implementation of novel and innovative telepharmacy services are derived out of necessity to bridge a gap and consequently lack any baseline comparison. Finally, the technical definition of telepharmacy is reserved for pharmacists or services with US jurisdiction. Several of these studies took place outside of this jurisdiction, but for the sake of comparison, the authors felt comfortable broadly applying this definition to those studies as well.
A core function of a pharmacist is to enhance patient safety through prospective medication review. At minimum, increasing pharmacist access whether on-site or remotely, increases the accessibility of this safety feature and adds a greater deal of order scrutiny. However, there is much more potential in this field. At the current state, few institutions take advantage of telepharmacy despite clinical, operational, safety, emotional, and financial benefits. In most cases, only relatively basic technology has been implemented. Further research should examine other ways in which these pharmacists and additional technology can aid the health care system. With a landscape shifting toward patient-reported outcomes as a quality measure clouded by an unclear financial future, telepharmacists are in a unique position to bridge this gap. Stakeholders are interested in this technology and may provide the support necessary to move forward. Once established, telepharmacy services presence can be leveraged with current clinical pharmacist duties to expand care into different areas and further improve patient outcomes.
Relevance to Patient Care and Clinical Practice
The available studies illustrate that telepharmacy services in all settings (ICU vs non-ICU) improved specific patient outcomes, led to greater nursing satisfaction, and expanded the provision of services. With increasing financial pressures on the health care system, inpatient telepharmacy is a useful tool to enhance current pharmacist services.
Conclusion
Technology and communication methods were similar in both ICU and non-ICU settings and assisted with the expansion of services in the former and improved patient outreach, particularly to remote areas in the latter. It is important to understand the clinical and financial benefits of inpatient telepharmacy services and how telepharmacy and in-person pharmacist services can complement each other. This review serves as a call to further examine in a rigorous manner the impact telepharmacy services may have on inpatient settings, including ICU and non-ICU populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.