
Abstract
Introduction
Uncontrolled hypertension (HTN) is a major risk factor associated with myocardial infarction, stroke, renal failure, and death. 1 Numerous well-controlled trials describe the effectiveness and efficacy of medication therapy to curtail these risks.2-4 Race, specifically being of African American ancestry, remains a risk factor for uncontrolled HTN and poorer cardiovascular disease outcomes. 5 There is substantial interest in eliminating this inequity, including support for implementing multilevel approaches that simultaneously address multiple levels of the socioecological model to address this complex condition. 6 These strategies include practice-level interventions, such as practice facilitation, decision support, and treatment intensification, as well as patient and community level interventions, such as home blood pressure (BP) monitoring and health coaching.6-8 Prior evidence suggests value in guiding providers to more readily intensify medication therapies, avoiding challenges of clinical inertia that can unnecessarily prolong states of uncontrolled HTN. How to best measure intensification is unknown.9-11 Most prior methods of measuring treatment intensification model these changes based on point-of-care measurements but provide limited information on the specific medication changes that were made. Furthermore, there is little published on patterns of medication intensification when home BP monitoring (HBPM) data are used to evaluate medication intensification.
The Heart Healthy Lenoir project was a community-based participatory research model involving multilevel quality improvement efforts to reduce racial disparities in BP control in rural primary care practices; the methods have been previously described in detail. 8 Briefly, the study included a formative phase, where we collected qualitative data from patients, providers, and office staff on the resources and barriers affecting BP control in their region, followed by an implementation phase. During the implementation phase, we conducted a practice-based intervention using a quality improvement approach, with strategies designed to change practice (via practice-facilitator led sequential plan-do-study-act cycles with practice staff) and patient (via a trained, health coach–led protocol of telephone-based emotional support and coaching for patients) behavior. The theory-driven intervention was designed to improve BP control and reduce disparities in the targeted community, while having a limited impact on office-based patient flow. The study was approved by the Institutional Review Board at the University of North Carolina—Chapel Hill, and each patient provided written informed consent. BP control in a cohort of patients from these practices improved from baseline to 12-month follow-up in both black and white patients. Specifically, both black (−5.0 mm Hg) and white (−7.8 mm Hg) patients had a significant decrease in mean systolic blood pressure (SBP); however, the between-racial group differences were not statistically significant. 12 The purpose of the present study was to evaluate whether differential patterns of treatment intensification occurred between black and white patients in the Heart Healthy Lenoir study and to explore the use of the defined daily dose (DDD) as a methodology for defining medication treatment intensification in patients using HBPM.
Methods
Overall Study
The present data come from patients in the Heart Healthy Lenoir study, described in detail previously.8,12-14 Briefly, the study was a prospective cohort study of HTN control involving multilevel quality improvement in 6 rural primary care practices in an economically distressed county in the southeastern United States. A nonrandomized observational trial design was selected to maximize feasibility and acceptability for conducting this research in busy rural primary care practices unaccustomed to participating in research and to facilitate broad community participation, important to addressing health disparities. A sample of black and white patients (race was self-identified) from each of the 6 small- (1-3 providers) to medium-sized (4-10 providers) practices represented the impact of the system-level (quality improvement training) and patient-level (health coaching) intervention components. A total of n =525 adult patients being seen in 1 of the 6 rural primary care practices with an established HTN diagnosis and at least 1 visit in the past year with an uncontrolled SBP measurement (SBP ⩾ 150 mm Hg) based on office BP readings participated in the Heart Healthy Lenoir study. Patient data for this study were collected at enrollment and at the 6- and 12-month follow-up visits at a research center.
Each participant was given an oscillometric home BP monitor (Omron BP 785 or Omron BP 652) and was taught accurate measurement techniques at his or her baseline visit. Patients were instructed to measure and record their BP 3 times per week with some measurements reflecting both
Sample for the Present Study
In the present study, the investigators focused only on eligible patients from the Heart Healthy Lenoir study who used HBPM and who provided data at follow-up research clinic visits from at least 12 home BP measurements in each of two 6-month periods: the initial 6 months following enrollment up to the 6-month research clinic visit and the subsequent period between the 6-month and 12-month follow-up visits at the research clinic. A total of 12 measurements were considered to be the minimum number of HBPM readings necessary to consider the patient as having adopted HBPM monitoring and to characterize mean SBP, based on the guidelines published by Pickering et al. 15 Those patients with a mean SBP from HBPM in the initial 6 months following enrollment of ⩾135 mm Hg were defined as being eligible for treatment intensification based on prior published guidelines. 15
At baseline and at the 6- and 12-month follow-up research clinic visits, patients brought their prescription and over-the-counter medications to their study visits where research assistants collected the medication data. Antihypertensive medication treatment intensity for each person was quantified using a DDD approach. This method was developed for pharmacoepidemiological research by the World Health Organization 16 (WHO) Collaborating Centre for Drug Statistics Methodology and has been used in other studies to estimate the intensity of medication use for various disease states.17,18 The DDD is the assumed average maintenance dose per day for a drug used for its main indication in adults; this dose is assigned a value of 1. Therefore, patients taking half of the usual daily dose are assigned a value of 0.5 for that medication, whereas patients taking twice the usual daily dosage (as a single dose or in divided daily doses) would be assigned a value of 2 for that specific medication. For this study, the total antihypertensive DDD was computed as follows. Each patient’s antihypertensive medications were identified from their list of medications at baseline, 6-month, and 12-month follow-up visits, and the individual DDD for each individual antihypertensive medication was determined by using the WHO online library of individual DDD values for all medications (http://www.whocc.no/atc_ddd_index/). The total antihypertensive medication intensity for each patient at each time point was then computed as the sum of all individual antihypertensive medication DDD values (ie, the sum of the DDDs for each antihypertensive medication). The change in antihypertensive medication treatment intensity (ie, change in total antihypertensive medication DDD) was then computed from baseline to the 12-month follow-up visit. Data from the 12-month follow-up visit were specifically chosen because this was the period of maximal training for patients by health coaches regarding HBPM. Medication adherence was assessed at baseline using a 4-item validated scale. 19
Patient population characteristics were analyzed using descriptive statistics, including means (±SD) and proportions. Baseline characteristics were compared between study groups as follows: means for continuous measures such as age, BP, and body mass index (BMI) were compared using independent-samples t-tests, whereas proportions (eg, female sex, low household income, presence of diabetes) were compared using the χ2 test. Significance level for all comparisons was set at P ⩽0.05. Changes in mean antihypertensive DDD values were compared from baseline to 12-month follow-up in all participants and by race groups (black vs white) using independent-samples t-tests, whereas proportions of patients taking various antihypertensive classes were compared using the χ2 test, to define overall and race-specific patterns of treatment intensification. Changes in mean anti-hypertensive DDD and changes in the mean number of anti-hypertensive classes being taken were examined by Pearson correlation. Changes in mean SBP were also evaluated in those in whom treatment was intensified (ie, increase in DDD from baseline to 12-month follow-up) and these changes compared by race using independent samples t-test. A limited multivariate analysis using linear modeling was completed to examine potential correlates of mean DDD at baseline and again at the 12-month follow-up. This analysis included age, race, sex, and health insurance status (insured vs uninsured) as potential covariates of interest.
Results
Of the 509 patients in the Heart Healthy Lenoir study with complete medication data, a total of 217 (42.6%) reported regularly using HBPM and provided 12 or more home BP readings during each of two 6-month periods. The mean number of home BP readings reported during both the two 6-month time periods were not significantly different by race (initial 6 months: black = 77 ± 51 vs white = 68 ± 53 readings [P = 0.27]; second 6 months: black = 70 ± 63 vs white = 60 ± 52 readings [P = 0.22]). Of the 217 with available HBPM data, 90 patients (41%; n = 55 black, n = 35 white) were identified as “eligible” for treatment intensification based on having a mean HBPM SBP ⩾135 mm Hg during the initial 6-month period. The characteristics for these patients are given in Table 1. Black patients reported significantly lower household income and educational level as well as a greater prevalence of diabetes. Low medication adherence was reported more commonly, and BMI was modestly greater among black patients, but neither difference was statistically significant. There were modest differences in the number of antihypertensives by race, with black patients taking more antihypertensive medications than white patients. Likewise, there were differences in prescribing by therapeutic class, with a higher percentage of blacks taking diuretics and calcium channel blockers (see Table 2).
Baseline Characteristics of Patients with a Mean HBPM Systolic BP ⩾135 mm Hg During the Initial 6-Month Period.

Abbreviations: BP, blood pressure; CVD, cardiovascular disease; HBPM, home BP monitoring.
Baseline Use of Antihypertensives, by Class With Overall AH DDD.
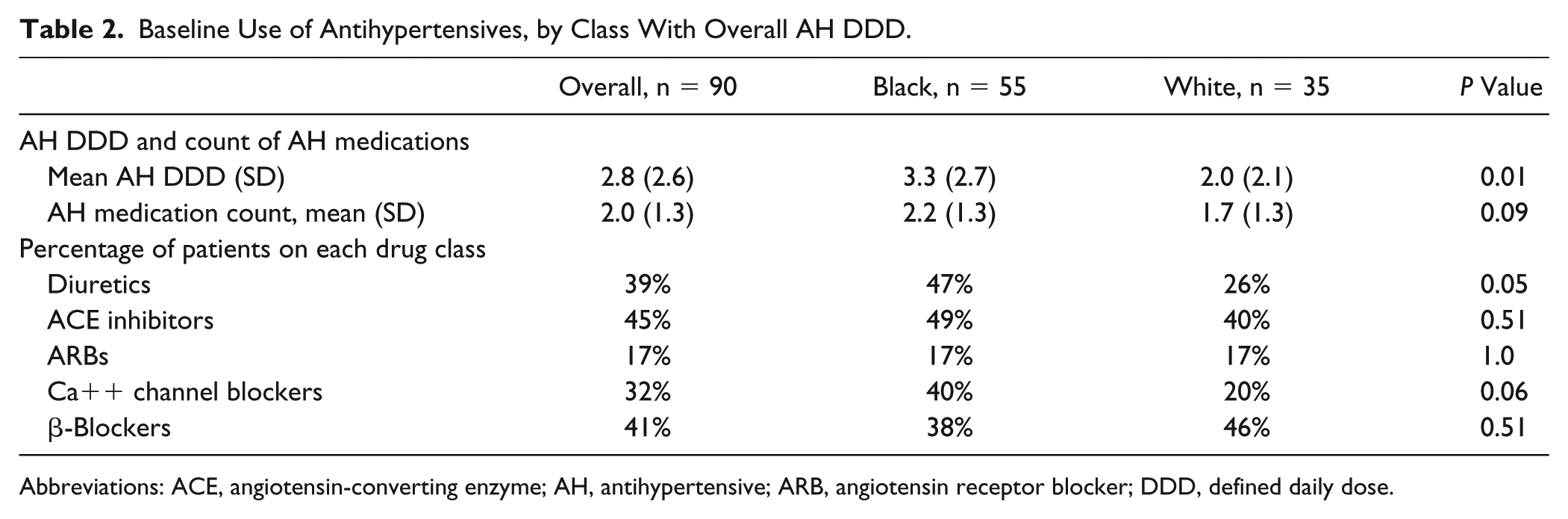
Abbreviations: ACE, angiotensin-converting enzyme; AH, antihypertensive; ARB, angiotensin receptor blocker; DDD, defined daily dose.
Figure 1 shows the change in treatment intensity (mean total antihypertensive DDD) in this subgroup by race at both baseline and at 12-month follow-up. Black patients had significantly higher mean total antihypertensive DDD values at both baseline (3.34 vs 1.99; P = 0.015) and at 12-month follow-up (4.02 vs 2.80; P = 0.027). Multivariate linear modeling that examined age, race, sex, and health insurance status as potential correlates of mean DDD at both baseline and 12-month follow-up time points demonstrated similar relationships, and notably that race was the only significant independent correlate at both time points (see Table 3). However, the change in mean total antihypertensive DDD from baseline to 12-month follow-up was not statistically significantly different by race (see Figure 1; +0.72 vs +0.65, P = 0.83). The proportion of black patients with any increase in mean total antihypertensive DDD was slightly higher than in white patients (66.7% vs 56.3%, respectively), but this difference was not statistically significant. However, there was a modest but significantly greater change in mean total antihypertensive DDD from baseline to 12-month follow-up by gender, with male patients having more treatment intensification (+1.1 ± 1.4 in males vs +0.40 ± 1.5 in female patients; P = 0.03). Only 12 (21%) black patients versus 4 (11%) white patients (P = 0.27) had any decrease in mean total antihypertensive DDD or de-escalation of treatment from baseline to 12-month follow-up.
Comparison of 2 Multivariate Linear Models Examining Potential Correlates of Mean Total Antihypertensive DDD as the Outcome of Interest. a
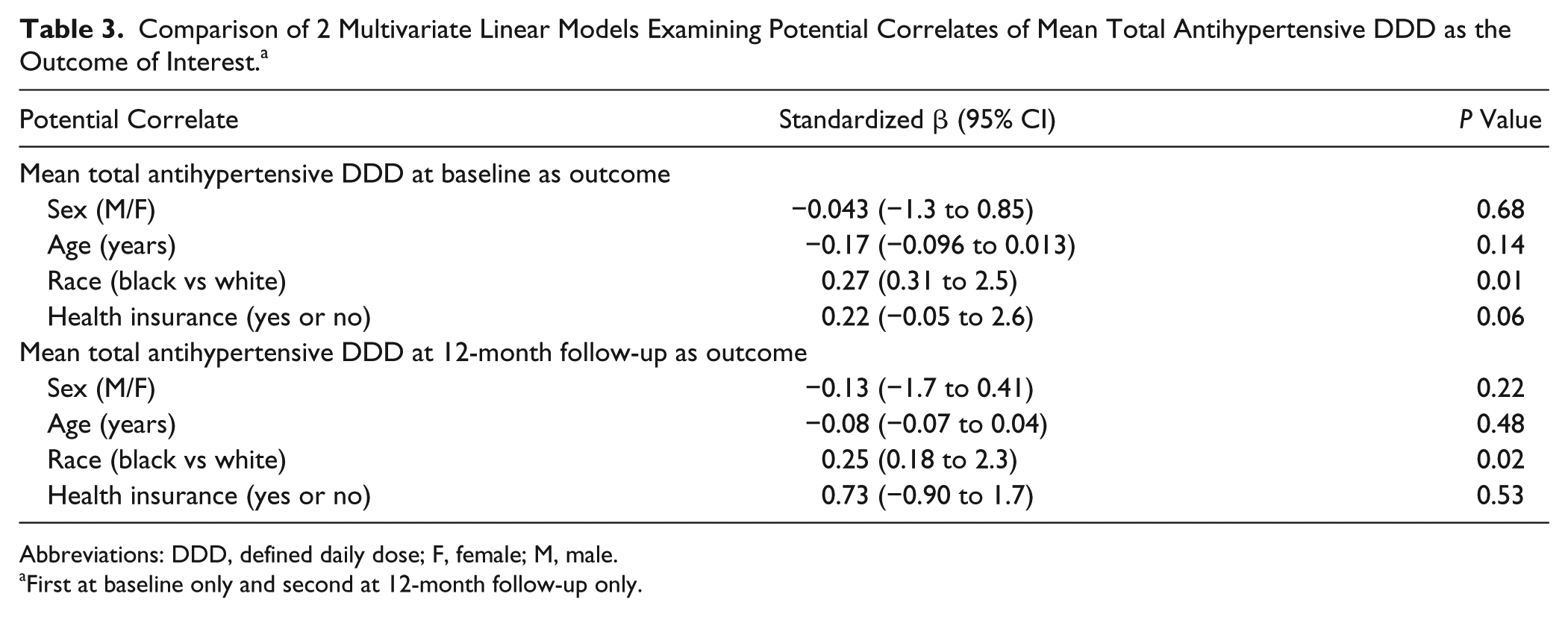
Abbreviations: DDD, defined daily dose; F, female; M, male.
First at baseline only and second at 12-month follow-up only.
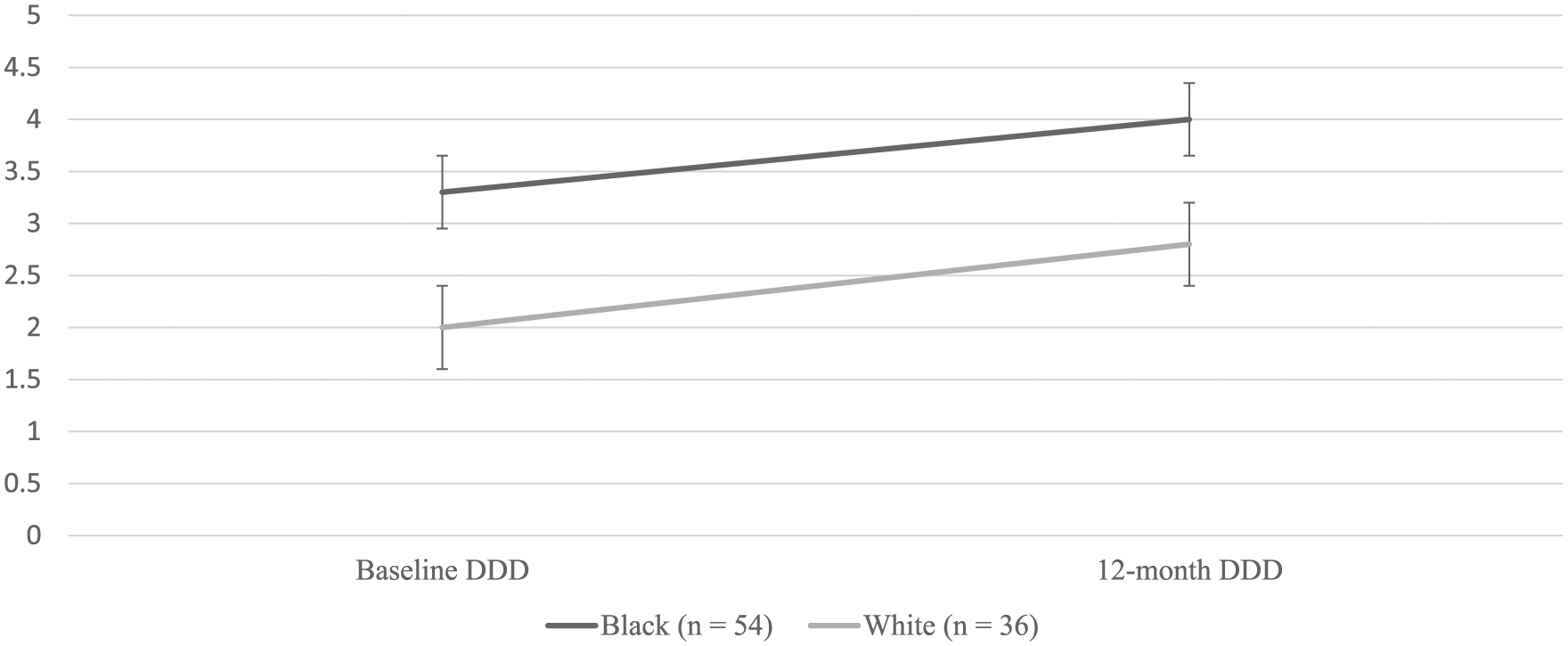
Change in mean (±standard error) total antihypertensive defined daily dose (DDD) values by race from baseline to 12-month follow-up in all patients (n = 90) with initial 6-month period mean home-measured systolic blood pressure readings ⩾135 mm Hg.
In the entire sample (n = 90), the mean increase at 12 months in number of antihypertensive medication classes (+0.4 ± 0.9 in white patients vs +0.3 ± 1.0 in black patients; P = 0.60) was not significantly different by race. Table 4 shows antihypertensive medication classes by race at baseline and 12-month follow-up in the subset of patients (n = 52) who received treatment intensification (ie, higher total antihypertensive DDD at 12-month follow-up). These data suggest modest increases in multiple medication classes (angiotensin-converting enzyme [ACE] inhibitor, diuretic, calcium channel blocker, etc) as part of intensification, without a significant difference by race. Furthermore, there was a significant positive correlation between the change in DDD and the change in the mean number of antihypertensive medication classes that were reported being used from baseline to 12-month follow-up (Pearson correlation = 0.37; P = 0.001).
Change in Percentage of Patients (PTS) Receiving Various Antihypertensive Medication Classes in the Subset of Patients With Home BP Monitoring Data Who Were Eligible for and Received Treatment Intensification, by Race (n = 52).
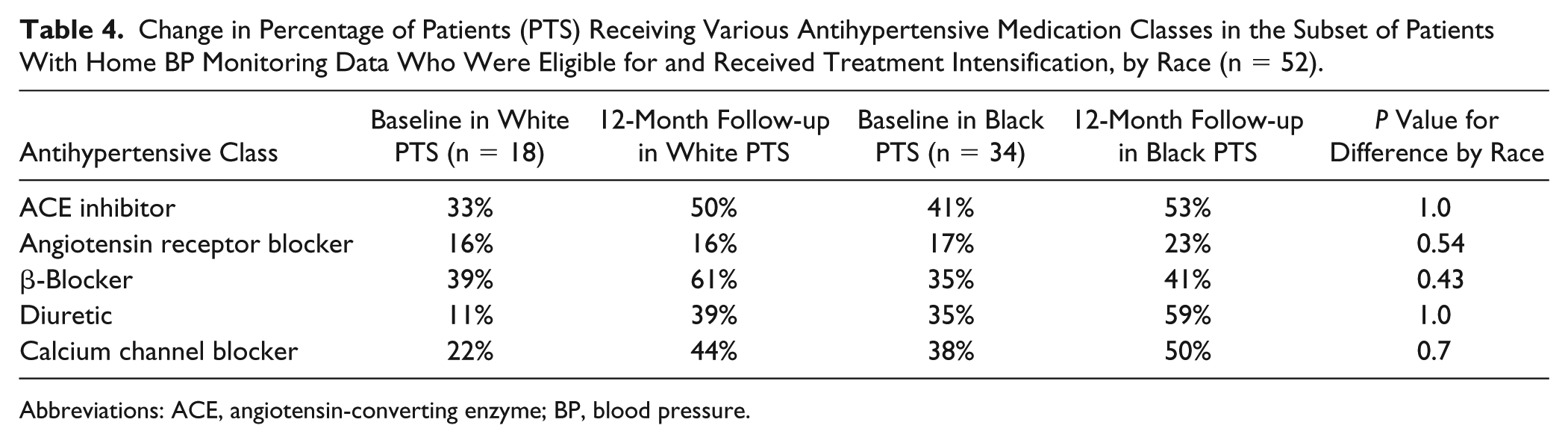
Abbreviations: ACE, angiotensin-converting enzyme; BP, blood pressure.
Among the 90 patients eligible for intensification, the mean change in SBP at 12-month follow-up was greater in those with an increase in antihypertensive treatment (ie, DDD increased; n = 52) compared with those who had no change or a lower antihypertensive treatment intensity (DDD same or lower, n = 38; −5.2 ± 9.4 vs −2.6 ± 12.4 mm Hg; P = 0.30), although this did not achieve statistical significance. In this group, the decline in SBP among those with an increase in DDD was greater, although nonsignificantly, in white patients than in black patients (−8.2 ± 9.1 vs −3.9 ± 9.4; P = 0.14) despite relatively comparable changes across races in mean DDD (+0.72 vs +0.65; P = 0.83). Furthermore, 73% (n = 38/52) of those with an increase in mean DDD had some degree of decline in SBP between baseline and 12-month follow-up. With respect to goal BP achievement, 54% (n = 19) of white patients versus 44% (n = 24) of black patients achieved target BP values (<140/90 mm Hg) at the 12-month follow-up research visit (P = 0.50). Specifically, the percentage of patients meeting target BP values increased in both race groups from baseline to 12-month follow-up (white patients increasing from 34% to 54%; black patients increasing from 33% to 44%). The proportion of patients reporting low medication adherence was unchanged from baseline (35%) to 12-month follow-up (36%), with no significant differences by race at either time point.
Discussion
Differences in HTN control by race persist and may be associated with disparate cardiovascular outcomes. When BP control is determined to be inadequate during office-based visits, providers may have questions or concerns related to medication adherence, adverse effects, affordability, and so on. Regardless of these potential causes of elevated office BP readings, antihypertensive therapy is often intensified during that office visit. In addition, HBPM is often recommended as an important strategy in HTN management because of its improved consistency with 24-hour ambulatory BP measures, improved reproducibility, and better correlation with target organ damage and because it helps overcome the challenges associated with using only office-based measurement. 15 However, it is unclear the extent to which HBPM use and the associated encouragement of patients to share HBPM readings with their provider influences treatment intensification and whether differential patterns of treatment intensification may occur by race in this situation, particularly in rural primary care settings. The present study is unique in that it examines treatment intensification patterns by race in rural primary care patients who use HBPM and who have been specifically encouraged to share those readings with their providers.
Furthermore, the present study uses an innovative numerical measure of antihypertensive treatment intensity (total antihypertensive DDD) that has only been tried in 1 prior study, 20 which was outside the United States. This metric allows more careful examination of both total antihypertensive medication use as well as which medication classes are used/changed in treatment intensification efforts. This use of the DDD measure for antihypertensive medications was initially used by McManus et al 20 in their trial of HBPM and antihypertensive self-titration by hypertensive patients in the United Kingdom. The present findings demonstrate the utility of the total antihypertensive DDD for characterizing the intensity of antihypertensive treatment and its changes across a 1-year follow-up period. There was a good correlation between increasing DDD values and increases in the mean number of antihypertensive medication classes used. Although the mean number of antihypertensive medications is useful, the value of the DDD is that it also allows for measuring treatment intensification associated with dosage increases for antihypertensive medications. The total antihypertensive DDD consolidates information from the number of medications, classes of medications, and dosage into a single numerical measure that can be tracked over time. The DDD can also be used to characterize treatment intensity with individual therapeutic classes of antihypertensive medications, providing insight into the race-specific or other subgroup prescribing of various classes as shown in this study.
In this study, black patients reported taking more antihypertensive medications at both time points, but changes in the pattern of use of various antihypertensive medication classes in the subset of patients in whom intensification occurred was not significantly different by race. ACE inhibitor and ARB use increased in both racial groups, whereas diuretic and calcium channel blocker use remained higher in black patients at both time points. This pattern of greater prescribing of diuretics and calcium channel blockers in black patients is consistent with the recommendations of the committee originally empaneled for JNC 8. 1 Also, β-blockers were utilized more frequently than anticipated, especially for intensification in white patients, although the extent to which other indications for β-blocker use were present is not clear.
Mean SBP was slightly higher among black patients at baseline, even though they were younger, but this difference was not statistically significant. Antihypertensive medication intensity was higher at baseline and at 12-month follow-up among black patients, but the magnitude of treatment intensification (mean change in total antihypertensive DDD) was not different by race. This suggests that rural primary care providers intensify medication therapy for patients with a history of uncontrolled HTN, regardless of race. This finding is consistent with that reported by Blair et al 21 who showed that clinician’s level of implicit bias did not influence treatment intensification for HTN for African American patients in routine office care in an urban setting. The present study extends these findings and demonstrates a similar lack of bias in treatment intensification in rural practice in patients who were encouraged to share HBPM data with their provider.
Intensification of treatment led to a reduction of SBP in most patients, and this is consistent with the findings of Daugherty et al, 22 who demonstrated that intensification was more likely to result in improved BP control. As a result, however, among those who received treatment intensification, reduction in SBP was modestly greater in white than in black patients. Furthermore, our findings showed that, despite intensification similarities, a smaller percentage of black patients achieved targeted BP values. The findings in this study are consistent with those reported by Cené et al, 12 who demonstrated that 62% of white patients versus 52% of black patients with uncontrolled BP at baseline achieved targeted BP values at 12-month follow-up. These results are similar to previous reports demonstrating some racial differences in the magnitude of response to various antihypertensive agents.23,24 It remains unclear whether specific pharmacological or pharmacogenetic mechanisms contributed to the modestly different SBP responses observed by race in this subset or whether other factors such as lifestyle behaviors, BMI, age, and/or medication adherence may have contributed. Regardless, based on the present findings and that of others, it seems appropriate to support guideline 25 indicated intensification of antihypertensive treatment using carefully selected antihypertensive agents as detailed in recent guideline documents.1,25
The present study is important in that it examines specific patterns of treatment intensification by race using a method not previously utilized in HTN disparities research. However, the study also has important limitations. First, using a cut-point of 12 home BP measures that may have occurred at any time in the initial 6-month period may have been inadequate to accurately characterize patients as HBPM users and potentially in need of medication intensification. However, the patients in this study had substantially more readings than 12 in both time periods (eg, mean = 73 in the initial time period), and the selection of 12 readings as a cut-point follows the general guidelines for HBPM clinical decision making published by Pickering et al. 15 There are also no data to quantify the extent to which patients actually shared HBPM data with their providers or if primary care providers actually utilized HBPM results in evaluating and managing patients, including whether this specifically influenced their intensification decisions or office-based prescribing changes between visits. Furthermore, actual in-office BP measurements by the primary care provider were also not available to the investigators. The authors also acknowledge that use of the DDD may have limitations. For some medications, it may be difficult to determine what actually constitutes a “standard dose,” and the DDD score may overestimate the significance of a dosage change compared with the addition of another medication. However, as noted above, this DDD metric may also have unique value beyond prior strategies to characterize intensification. Because the study had limited sample size, caution is observed in the interpretation of these findings, and additional research is needed to compare treatment intensification patterns in larger samples. No data were available on changes in sodium intake, changes in BMI, or other clinical factors that may have influenced the BP response between baseline and 12-month follow-up. Finally, this study was carried out in a rural community involving only black and white patients with HTN, and extrapolation to other racial and ethnic groups or urban communities may be limited.
Conclusion and Relevance
In conclusion, the present study demonstrates that rural primary care physicians intensify antihypertensive treatment to a similar degree in both black and white patients with elevated home BP readings. Furthermore, we have demonstrated the functionality of the DDD and the total antihypertensive DDD as a single metric for characterizing the extent to which treatment in hypertensive patients is intensified between 2 time points. The classes of antihypertensive agents used in this rural primary care cohort and in the subgroup with treatment intensification are consistent with recommended treatment patterns. The magnitude of reduction in SBP following treatment intensification was greater in white than in black patients, but the reasons for this require further investigation.
Footnotes
Authors’ Note
This work was previously presented at the North American Primary Care Research Group, Practice Based Research Network Conference, Bethesda, MD, June 2016.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by National Heart Lung and Blood Institute, NHLBI 1P50HL10584–01. The funding body had no role in the collection, analysis, and interpretation of study data, nor did they play a role in the writing of the manuscript or the submission of the manuscript for publication. Trial registration: ![]() NCT01425515.
NCT01425515.