
Abstract

Osimertinib is a third-generation tyrosine kinase inhibitor (TKI) recently approved as a first-line treatment for EGFR-mutated non–small cell lung cancer (NSCLC). Osimertinib exhibits a mild to large interindividual variability in its pharmacokinetics. 1 The onset of severe toxicities such as diarrhea and rash are associated with increased osimertinib plasma concentrations. 1 Osimertinib is mainly metabolized by cytochrome P450 3A4 (CYP3A4), and thus, is a candidate for drug-drug interaction (DDI) with CYP3A4 inhibitors or inducers.2,3 A limited impact of itraconazole (200 mg twice daily) on osimertinib pharmacokinetics (24% increase in area under the curve) has been reported. 2 However, the clinical relevance of this DDI could be enhanced in elderly patients.
Here, we report the case of an 86-year-old woman presenting with a stage IV lung adenocarcinoma with bone metastases, harboring 2 activating mutations of EGFR (exon 19 deletion and T790M mutation). Despite the T790M EGFR mutation, she was first treated with erlotinib in May 2015 because osimertinib was not approved yet as a first-line treatment in France. Predictably, erlotinib was rapidly discontinued because of disease progression, and osimertinib was started in November 2015 at the recommended dose of 80 mg daily. The only comedication was propranolol (20 mg twice daily). One month later, the patient experienced dry cough, a potential osimertinib-related adverse event. Esomeprazole (40 mg/d), desloratadine (5 mg/d), and azithromycin (250 mg/d for 10 days) were introduced as treatments of the cough, and osimertinib dosing was decreased to 40 mg/d. The patient consequently remained asymptomatic for almost 2 years. In July 2017, the cough reappeared, and bronchoscopy revealed an Aspergillus infection requiring the introduction of low-dose itraconazole (200 mg/d); osimertinib dosing (40 mg/d) was not modified. In October 2017, the patient’s quality of life (QoL) was significantly altered because of grade 2 diarrhea and debilitating cough. Osimertinib trough concentration (Cmin) in plasma 4 was 316 ng/mL, which was approximately 1.7-fold higher than the mean expected Cmin (190 ng/mL) for an 80-mg daily dose. 1 We postulated that the patient was overexposed, and dosing was modified to 40 mg every 48 hours, resulting in a complete resolution of diarrhea. One and 3 months later, osimertinib Cmin values were 227 and 176 ng/mL, respectively (Figure 1). In February 2018, itraconazole was discontinued, and osimertinib dosing was concurrently increased to 40 mg daily. Seven days later, osimertinib Cmin was 242 ng/mL. According to the Drug Interaction Probability Scale, 5 the DDI was possible. Then, 15 days later, the patient died because of respiratory distress, probably related to disease progression.
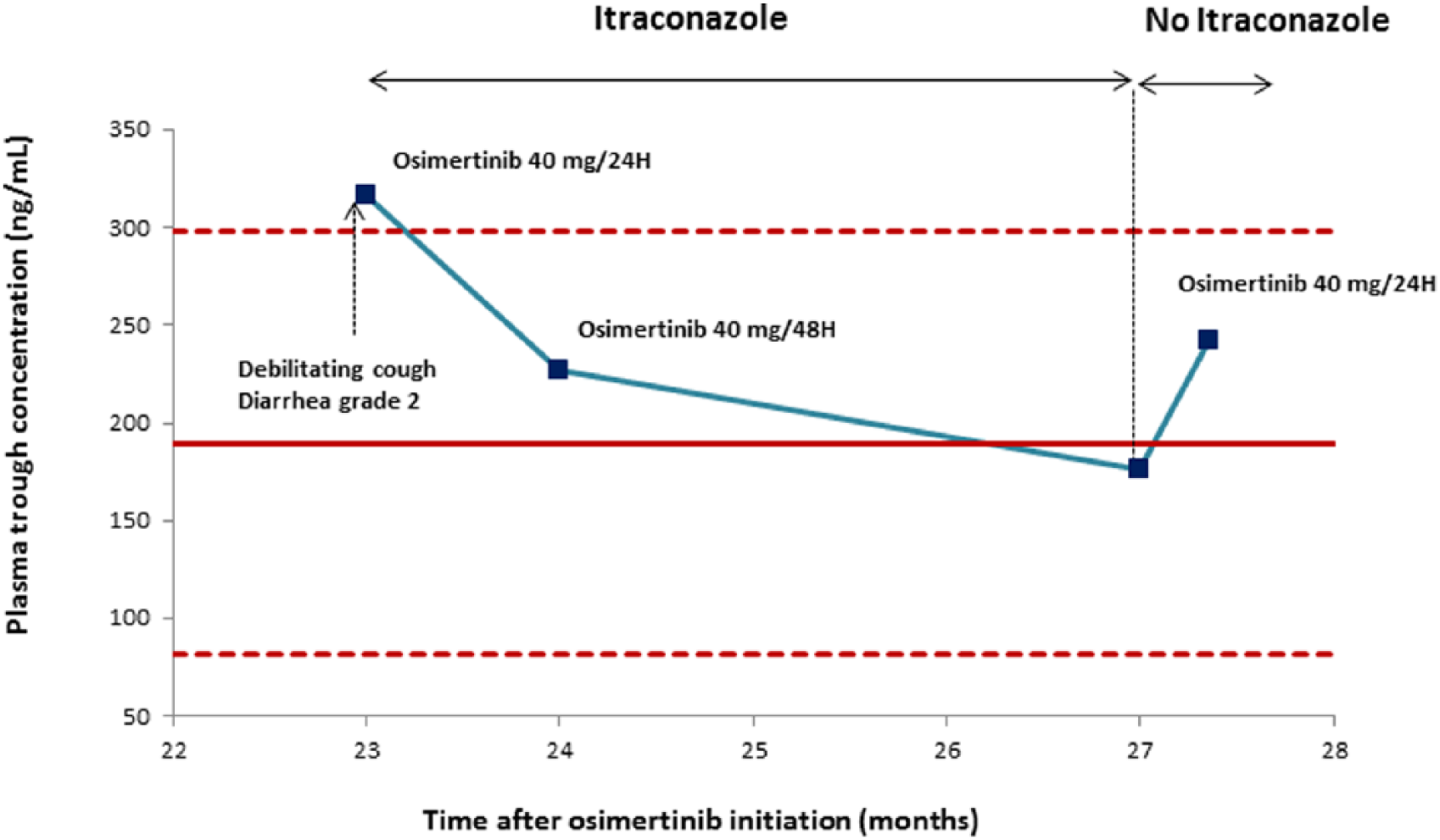
Osimertinib trough concentration in plasma over time during and after itraconazole therapy. The dots delimit the expected osimertinib plasma trough concentration area at the recommended daily dose of 80 mg according to the European Medicines Agency assessment report. 1
Osimertinib has substantially improved the life expectancy of elderly NSCLC patients. Maintaining an acceptable QoL in elderly patients receiving cancer treatment has always been a challenge. Here, 40 mg of osimertinib every 48 hours was enough to achieve both antitumor efficacy (overall survival of 27 months) and acceptable QoL in an 86-year-old patient concomitantly treated with low-dose itraconazole. Different factors such as age, sarcopenia, and itraconazole-mediated CYP3A4 inhibition could have contributed to the lower metabolic clearance of osimertinib in our patient. A high incidence of toxicity-induced treatment discontinuation (33%) related to plasma overexposure was recently reported in >75-year-old NSCLC patients under erlotinib, another EGFR TKI. 6 In this context, plasma drug monitoring of osimertinib could be helpful in elderly patients, especially in those concomitantly treated with itraconazole and more widely with potent CYP3A4 inhibitors. In these cases, when access to plasma drug monitoring is limited, we recommend starting osimertinib at half dose, then increasing if tolerated to 80 mg daily.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.