
Abstract

Leukopenia, neutropenia, and thrombocytopenia are uncommon but well-known adverse effects of rifamycins. 1 However, little information is available concerning cross-reactivity between agents in the rifamycin class. This report describes a case of successful rifampin challenge after possible rifabutin-induced leukopenia and neutropenia.
A 24-year-old woman with a past medical history of Bartter syndrome, esophagitis, and gastroparesis with gastrostomy tube placement was found to have transaminitis with granulomatous disease in a liver biopsy and migrating nodules on a computed tomography (CT) scan of her chest. Mycobacterium lentiflavum was isolated from 4 acid-fast bacillus sputum cultures, and treatment was held while awaiting susceptibility testing. Three months later, the patient was readmitted for fevers and vomiting and was found to have progressive disease, with repeat chest CT scans revealing new pulmonary nodules. Because of multidrug resistance of the isolate, ongoing consultation with disease experts, and drug acquisition, formulation, and toxicity concerns, the patient was discharged pending confirmation of the treatment plan.
One month later, the patient was readmitted for planned stepwise initiation of antimycobacterial therapy. The initial treatment regimen consisted of azithromycin 250 mg daily and rifabutin 300 mg daily on day 1, amikacin 22 mg/kg twice weekly on day 3, and clofazimine 50 mg daily on day 7. A baseline white blood cell count (WBC) was 9400 cells/µL.
On day 5, the WBC began to decrease, and on day 13, the WBC was 1600 cells/µL, with an absolute neutrophil count of 610 cells/µL (Figure 1). Rifabutin was thought to be the most likely cause of leukopenia and was discontinued. On day 17, the WBC recovered to 3800 cells/µL, and rifampin 600 mg daily was initiated. The WBC continued to increase to 6800 cells/µL and remained stable for at least 8 months of treatment.
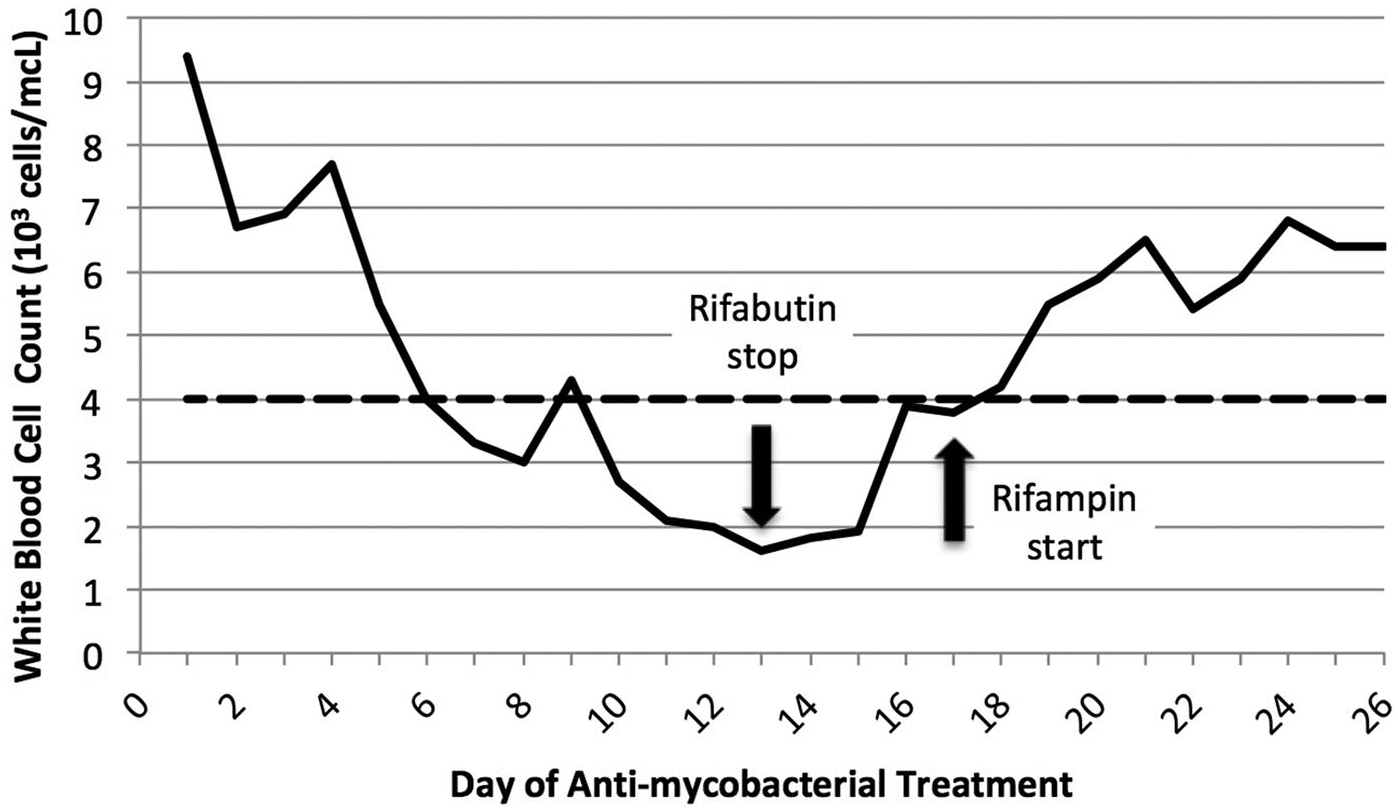
White blood cell count trend during antimycobacterial treatment. The dashed line denotes the lower limit of the reference range (<4000 cells/µL).
This case resulted with a “possible” association between rifabutin and leukopenia on the Naranjo scale. Leukopenia and neutropenia, with objective evidence (+1), developed after rifabutin initiation (+2) and improved with drug discontinuation (+1), although there were possible alternative explanations, including other antimycobacterial medications such as azithromycin (−1). However, rifamycins, specifically rifabutin, are most commonly associated with leukopenia and neutropenia in the literature (+1). Chitre and Berenson 2 described a case of rifabutin-induced leukopenia in a 68-year-old man with M avium complex infection. The WBC decreased to 1500 cells/µL after 3 weeks of therapy, increased after discontinuation, and decreased after reduced-dose rifabutin. Apseloff and colleagues terminated their randomized clinical trial examining drug interactions between rifabutin and macrolides early because of neutropenia in 47% of patients receiving rifabutin, including severe neutropenia in 30% of cases.3,4 Hafner et al 1 also noted neutropenia in 66% of patients receiving rifabutin and azithromycin, including 7 grade 3 and 1 grade 4 events. Finally, LeBel et al 5 observed significantly more neutropenia, leukopenia, and thrombocytopenia with rifabutin versus rifampin in healthy women taking oral contraceptives. To our knowledge, this is the first case report that describes a lack of cross-reactivity between rifamycins after rifabutin-induced leukopenia.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MVM is a member of the advisory board for Melinta Therapeutics, Tetraphase Pharmaceuticals, Inc, Roche Diagnostics, and CutisPharma, Inc, and has received research funding from Merck & Co. All other authors: none to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.