
Abstract
Evidence-based medicine (EBM) has been positively accepted by clinicians; however, there are barriers to practicing EBM that create gaps between EBM and current clinical practice. A pharmacist-led drug information (DI) service initiative was established to overcome common barriers to practicing EBM. The service utilizes technology and a collaborative model among otherwise independent academic DI centers to provide efficient high-quality service to health care professionals. It was piloted at a large health care system with positive user satisfaction. The unique technological collaborative has shown several benefits, including increased efficiency and peer learning among DI pharmacists.
Keywords
Evidence-based medicine (EBM) is defined as “conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”1(p 710) Since its introduction, EBM has been the new paradigm in clinical education and practice. 2 EBM is associated with improved clinical and patient-oriented outcomes, such as reduced mortality and length of hospital stay.2-8 Despite these benefits, a gap between EBM and current clinical practice is often reported in the literature, with inadequate skills and lack of time being among the most commonly identified barriers to practicing EBM.2,3,9,10 Yet simply providing additional training opportunities to improve the necessary skills may not immediately translate to improved patient outcomes. 3 A study comparing mortality and length of stay between an EBM-trained unit and non-EBM units showed significant benefits in EBM-trained units. The mortality rate in EBM units was 6.27% compared with 7.75% in non-EBM units (P < 0.001), and the mean length of stay was 6.01 days versus 8.46 days (P < 0.001). 3 Interestingly, when these outcomes were assessed during the 3 years while the practitioners in the EBM unit were being trained for the necessarily skills, these outcomes did not differ between the 2 units. 3 During that time, the mortality rate in the EBM unit was 7.4% versus 8.34% in the non-EBM unit (P = 0.1), and the mean length of stay was 9.15 days in the EBM unit versus 10.2 days in the non-EBM unit (P = 0.13). The authors suggested that the lack of difference may be a result of the time it takes to develop the necessary skills in addition to other factors, such as organizational elements and processes. 3
The sheer volume of available evidence is another barrier to integrating EBM into everyday practice.2,11 In 2002, the estimated number of articles practitioners would have to read to stay current was 7287 articles per month, which translates to 29 hours of daily reading. 12 Moreover, the National Library of Medicine reported that 904 636 citations were added to MEDLINE database in 2018, making 25 239 968 cumulative citations in total. 13 In the end, clinicians are left to choose between time spent in providing direct patient care versus searching and reading the literature to stay current with best practices, which seems counterintuitive.
To continue to practice EBM without compromising patient care time, one of the solutions could be to delegate the most time-consuming processes. For instance, searching the available literature for patient and circumstance-specific data and evaluating the quality of the available evidence can be readily delegated, and doing so allows the use of high-quality, preappraised evidence. This is the fundamental concept of InpharmD Drug Information Service. The service was established in 2015 by a faculty member at Mercer University College of Pharmacy and is currently managed by a group of drug information (DI) pharmacists. Pharmacists who specialize in DI are trained to retrieve, evaluate, and disseminate information efficiently in an effort to develop evidence-based recommendations and assist in patient care decisions. Because of this skill set, DI pharmacists are uniquely equipped to provide support for EBM decision making in a rapid and reliable fashion. In addition to the commercially available EBM tools that provide preappraised literature evidence (eg, DynaMed), the DI service provides an added layer of support for health care professionals to practice EBM, especially in complex clinical situations. Whereas practitioners may utilize the point-of-care EBM tools for general clinical questions, finding literature evidence for more complex inquiries (eg, specialty topics, unique patient cases) often poses a challenge. When clinicians are unable to retrieve literature evidence via a simple search on point-of-care EBM tools by utilizing the DI service, they will be able to receive tailored literature evidence that has been evaluated by trained DI pharmacists. Furthermore, these inquiries are researched and formulated offsite, allowing clinical pharmacists within the health system to continue engaging in activities more directly related to patient care. The service also uses a web-based portal and a mobile app to receive and disseminate the DI responses, which further enhances the efficiency of the process by eliminating unnecessary time spent in the process.
Use of technology is a unique feature of the service; however, the most innovative feature of this practice is the collaboration among DI pharmacists at 4 otherwise unrelated DI centers (DICs) across the nation. To our knowledge, this is the first “network” of academic DICs in the United States from independent institutions that work as a group to provide DI services to health care systems. There are several benefits of this practice model. First, it allows distribution of workload among the DICs, so that no one DIC is overrun with requests and other workloads. Although all academic DICs strive to be available at all times, most academic DICs have one DI pharmacist, often a faculty member, who is responsible for providing the service, maintaining the center, and teaching and precepting students on top of research and scholarship. 14 Because of limited manpower, centers may choose to not accept inquiries on certain days or may be unable to provide timely service, especially when there are multiple complex questions. 14 With the network of DICs, individual centers can choose to identify themselves as available on the DI portal available through InpharmD, which allows the algorithm to assign inquiries as they are received. If no center is available, the algorithm is set to assign all inquiries to a designated DIC. In such cases, the pharmacist in charge can reach out to the network to redistribute the inquiries as needed.
The model creates opportunities for pharmacists at these separate institutions to share ideas and expertise to foster peer learning and development. Through monthly meetings, standard operating procedures are continually refined and potential issues that affect day-to-day operations of the service are addressed. Each DI pharmacist utilizes their individual backgrounds and expertise to facilitate a better service and ensure a more efficient and effective workflow. Furthermore, this collaborative infrastructure is not only beneficial to the pharmacists but also to the health care professionals requesting information because it allows them to have access to a larger group of DI specialists.
The service was piloted in 2 metropolitan hospitals from May 2015 to December 2017. At any given time, it was estimated that there are more than 1000 health care practitioners between the 2 facilities. A total of 773 users registered to the service, and a total of 1266 inquiries were submitted. Further analysis showed that most users are general practitioners (55%; family medicine, internal medicine, nonspecialized physicians assistants, PharmDs, and nurse practitioners). This may be a result of the fact that generalists are responsible for knowing evidence across disease states compared with specialists who may focus on a single therapeutic area. Based on an analysis of inquiries submitted between February and August 2017, the top 3 inquiry categories were the following: (1) opioids and general pain, (2) infections and antibiotics, and (3) metabolic and cardiovascular conditions. Other highly represented inquiry categories included anticoagulation, medications and conditions affecting the central nervous system, and drug formulation or administration. Regarding user satisfaction, voluntary user responses have been collected starting May 2017. When they receive the inquiry response, users were asked to rate their satisfaction on a 5-point scale, with 5 being the highest satisfaction. A total of 175 responses were received until December 2018. The results are summarized in Figure 1. In general, users were satisfied with the inquiry response provided, with 71% rating 5/5 and 21% rating 4/5.
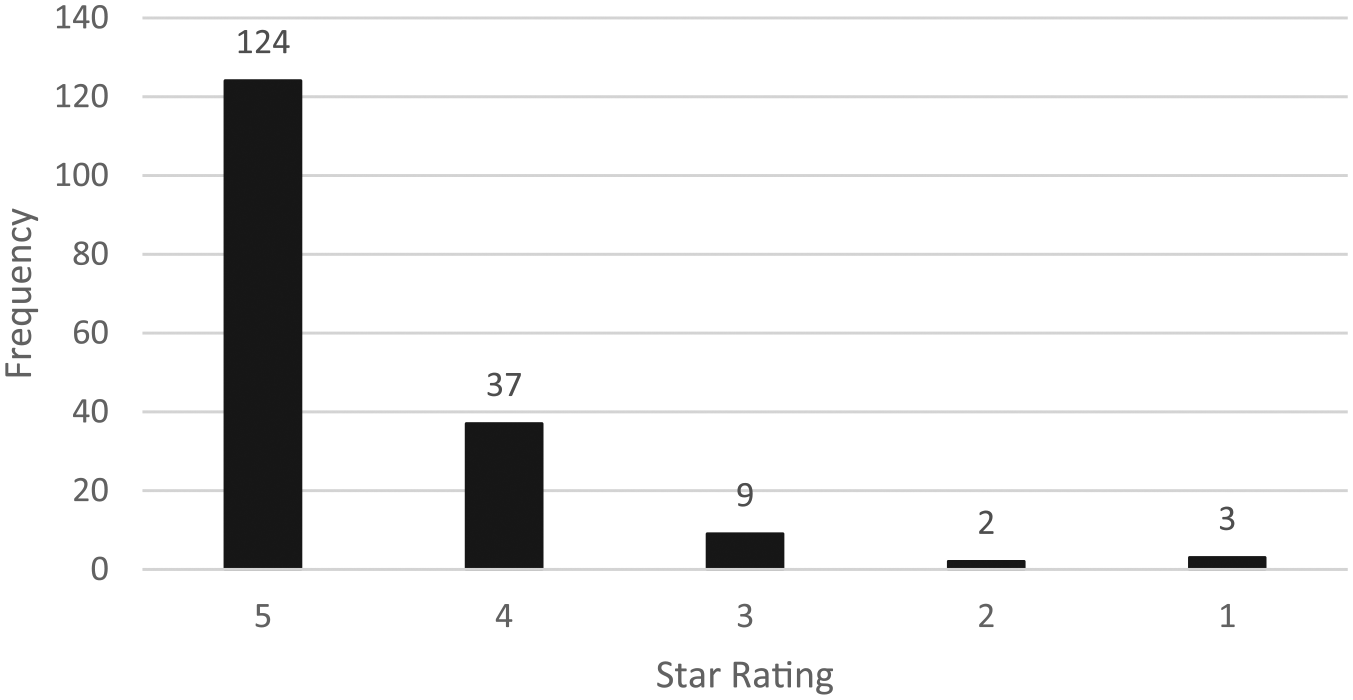
User satisfaction rating between May 2017 and December 2018.
Furthermore, the DI portal may also serve as a database to monitor which therapeutic areas practitioners may benefit from further training within the institution by analyzing commonly asked questions. This will allow pharmacists to identify opportunities for in-service education that may be most needed at the institution. For instance, in the institution where this service was piloted, based on commonly asked questions, education on multimodal pain management and overview of antibiotic therapy/stewardship may prove to be beneficial for the general practitioners. With the expansion of the service, the data will be collected from various health institutions and may reflect the needs of practitioners at a larger scale rather than institutional specific needs.
In the future, characteristics of the technology and the organization that enhance or impede the use of this service will be evaluated further in the next phase of the project. Inquiry volume and use of the mobile application and website are anticipated to increase because the service will be expanding to additional hospitals. The platform is also pursuing additional academic DICs collaborators to expand its network and meet the expected growth in use.
Here we described a unique collaborative model within the provision of DI. As previously discussed, this model may be beneficial in expanding resources and sharing knowledge among health care professionals. It is also our opinion that this model facilitates a collaboration between pharmacy schools and health care systems to further optimize EBM practice.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kim completed a drug information residency with InpharmD from 2017 to 2018. Drs Hoover, Perkins, and Kim are drug information faculty at institutions that are affiliated with InpharmD. Dr Advani is the founder of InpharmD. There were no specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.