
Abstract
Keywords
Background
Primary percutaneous coronary intervention (PCI) and dual antiplatelet therapy (DAPT) are both class I recommended therapies in patients presenting with acute coronary syndrome (ACS).1-4 The glycoprotein IIb/IIIa inhibitors (GPIs) abciximab, eptifibatide and tirofiban are potent inhibitors of platelet aggregation. 5 GPIs are recommended by international guidelines in the management of ST-elevation myocardial infarction (STEMI) downstream as a rescue strategy if there is angiographic evidence of massive thrombus, slow or no reflow, thrombotic complications, or as adjunct to primary PCI.3,4 They are also recommended to be considered in non–ST-elevation myocardial infarction (NSTEMI) and unstable angina (UA) patients when thrombotic complications occur during PCI or in patients with high-risk features such as positive troponin.1,2 GPIs are recommended by the American Heart Association (AHA) in patients with NSTEMI or UA not adequately pretreated with clopidogrel, prasugrel, or ticagrelor at the time of PCI. 1 However, these recommendations are not based on contemporary randomized trial data. The guidelines also recognize that the majority of the evidence supporting the use of GPI therapy predates trials that establish the benefits of clopidogrel or newer P2Y12 inhibitors, routine early invasive therapy, and aspiration thrombectomy.
GPI use has traditionally been driven by the benefits seen in older trials. For example, a 2002 meta-analysis of the use of GPIs in NSTEMI and UA found an association with a reduction in death or myocardial infarction (MI). 6 In contrast, studies conducted in the current era of contemporary practice have for the most part not shown a net clinical benefit of GPIs; a more recent meta-analysis of GPIs in STEMI patients undergoing primary PCI, which included trials with patients on clopidogrel, found that GPIs did not reduce 30-day mortality or reinfarction and were associated with higher risk of major bleeding complications. 7 Furthermore, a recent retrospective observational study of patients who underwent PCI for NSTEMI found that when added to DAPT, GPIs did not improve survival or reduce major adverse cardiovascular events (MACE). 8 In contrast, the ISAR-REACT 2 randomized trial found that abciximab, when added to loading doses of aspirin and clopidogrel in patients with NSTEMI or UA undergoing PCI, reduced the composite outcome of death, MI, or urgent target vessel revascularization but only in patients with a raised troponin. 9
In light of evolving evidence and the availability of more potent P2Y12 inhibitors this study aimed to determine trends in GPI use and their associated outcomes in real-world practice.
Methods
The use of GPIs in patients with ACS undergoing PCI was assessed from January 2005 through December 2013 in those who were enrolled in a large multicenter Australian registry (Melbourne Interventional Group [MIG]). The MIG registry is a collaborative venture of interventional cardiologists practicing at 6 Australian tertiary referral hospitals that was designed to record data pertaining to all PCIs and to perform follow-up at 30 days and periodically thereafter. The MIG registry has been previously described in detail.10,11 Demographic, clinical, and procedural characteristics of consecutive patients undergoing PCI are prospectively recorded on case report forms using standardized definitions for all fields.10,11 The registry is coordinated by the Centre of Cardiovascular Research and Education in Therapeutics, an independent research body within the Department of Epidemiology and Preventive Medicine, Monash University (Melbourne, Australia). An audit of 27 verifiable fields from 5% of randomly selected procedures at each institution is performed periodically by an investigator not affiliated with the institution; data accuracy was 98% on the most recent audit, which compares favorably to other large registries. 12 The registry has been approved by the ethics committee in each participating hospital and Monash University. “Opt-out” informed consent was obtained in all patients, as previously described, with very few patients opting out of our registry. The 30-day follow up was >99.5%.11,12
Patients were included in the analysis if they were undergoing PCI for an ACS in MIG hospitals. Baseline demographics and clinical and angiographic characteristics were analyzed and compared between GPI-treated patients (abciximab, eptifibatide, or tirofiban) and those who were not. Patients were allocated to the GPI group if they had received a GPI periprocedurally (including prior, during, and after PCI). Patients who did not receive a GPI at any time prior, during, and after the index PCI were allocated to the no-GPI group. Exclusion criteria included patients with cardiogenic shock, out-of-hospital cardiac arrest, or incomplete data available on the use of GPIs.
The indication for PCI was recorded and included UA, NSTEMI, and STEMI. The interventional strategy, stent selection, and antithrombotic therapy were left to the discretion of the operator in all procedures. DAPT was recommended in all cases where a stent was deployed. The primary end point was the 30-day incidence of MACE. The safety end point was in-hospital major bleeding.
In-hospital complications were recorded at the time of discharge or death. The 30-day follow-up was conducted by telephone, and patient medical records were reviewed to verify events. All cardiac events were documented, including death (all-cause mortality and cardiac mortality), MI, target-lesion revascularization, target-vessel revascularization, and the composite of major adverse cardiac events (death, MI, or target-vessel revascularization).
MI post-PCI was defined as a clinically distinct event with (1) new elevation of biomarkers ≥20% above the preprocedure cardiac biomarker level (in patients with preprocedure cardiac biomarker levels no longer rising) and/or (2) significant ST-segment change, development of new Q waves in >2 contiguous electrocardiographic leads, or new left branch bundle block pattern. Major bleeding was defined by any of the following: a decrease in hemoglobin >3.0 g/dL requiring blood transfusion and/or prolonged hospital stay.12,13 Location of major bleeding was recorded as retroperitoneal, access site complications, and “others,” which included bleeding at other sites (eg, gastrointestinal). Stroke was defined by the sudden onset of persistent loss of neurological function caused by an ischemic or hemorrhagic event during or after PCI.
All data are normally distributed unless otherwise stated. Continuous variables are expressed as means ± SDs, and categorical data are expressed as numbers (percentages). Continuous variables were compared using the student’s t-test. Categorical variables were compared using the fisher’s exact or χ2 tests as appropriate. Independent predictors for 30-day clinical outcomes were determined using multiple logistic regression models for variables with a P value <0.10 in simple logistic regression models (25 clinical and procedural variables were analyzed). Propensity matching was conducted to control for differences in baseline characteristics between patients who received GPIs and those who did not. A multivariable analysis was also conducted to determine predictors of 30-day MACE and in-hospital bleeding. All calculated P values were 2 sided, and a P value less than 0.05 was considered statistically significant. Statistical analysis was performed using Stata v13.1 for Windows (College Station, TX).
Results
Data from 12 357 patient procedures were included. GPIs were used in 5005 (40.5%) of these procedures. Table 1 highlights the baseline characteristics of the cohort. The cohort was predominantly Caucasian male, with patients more likely to receive GPIs if they were younger, presented with a STEMI, and were smokers. They had fewer comorbidities, being significantly less likely to have suffered a previous MI or have hypertension, hypercholesterolemia, heart failure, renal disease, or cerebrovascular and peripheral vascular disease. They were also less likely to have previously undergone PCI.
Patient and Procedural Characteristics.
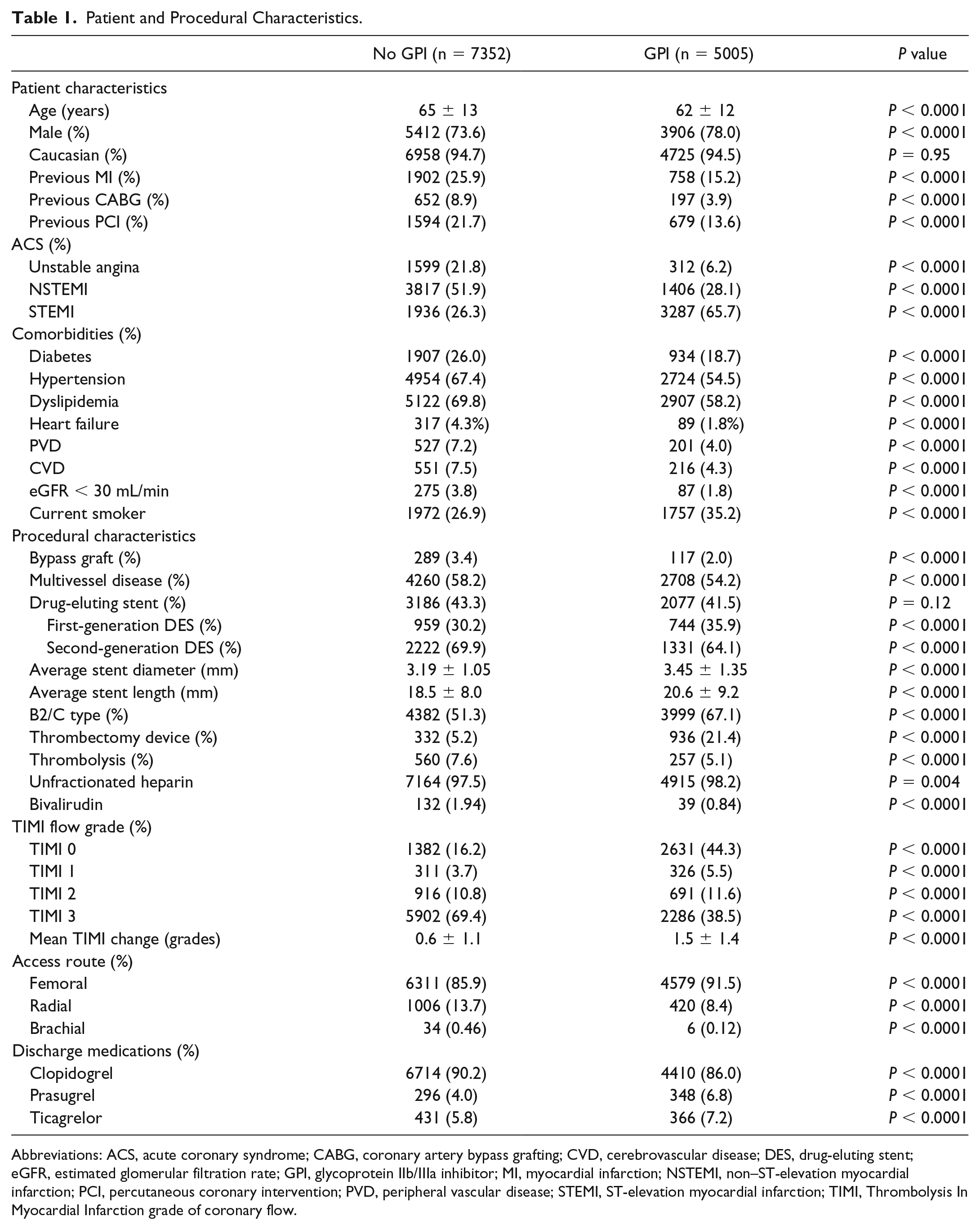
Abbreviations: ACS, acute coronary syndrome; CABG, coronary artery bypass grafting; CVD, cerebrovascular disease; DES, drug-eluting stent; eGFR, estimated glomerular filtration rate; GPI, glycoprotein IIb/IIIa inhibitor; MI, myocardial infarction; NSTEMI, non–ST-elevation myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease; STEMI, ST-elevation myocardial infarction; TIMI, Thrombolysis In Myocardial Infarction grade of coronary flow.
Procedural characteristics are outlined in Table 1. Patients treated with GPIs were significantly more likely to undergo the procedure via the femoral route, have more complex (AHA/ACC [American College of Cardiology] type B2 or C) lesions, have multivessel disease, and have an aspiration thrombectomy device used.
Most patients undergoing the procedure received unfractionated heparin (97.8%), with a small proportion of patients receiving bivalirudin (1.5%). Patients who were treated with GPIs were only slightly more likely to receive heparin (98.2% vs 97.5%, P = 0.004), and less likely to receive bivalirudin (0.84% vs 1.94%, P < 0.0001). Patients who received GPI were also more likely to be prescribed novel antiplatelets ticagrelor and prasugrel on discharge (31.6% vs 21.4% and 15.1% vs 8.0%; P < 0.0001 for both; Table 1).
GPI use was associated with greater improvement in mean Thrombolysis in Myocardial Infarction (TIMI) flow (1.5 vs 0.6 grades, P < 0.0001) at the completion of the PCI. The primary end point of MACE was higher in patients receiving GPI (4.9% vs 4.1%, P = 0.03), driven by 30-day target-vessel revascularization (2.7% vs 2.0%, P = 0.005; Table 2). GPI use was also associated with more major bleeding complications (3.6% vs 1.8%, P < 0.0001) but no difference in stroke (0.4% vs 0.3%, P = 0.47). The difference in bleeding rates was driven by “other” bleeding, with no difference in retroperitoneal or access site bleeding.
Clinical Outcomes.
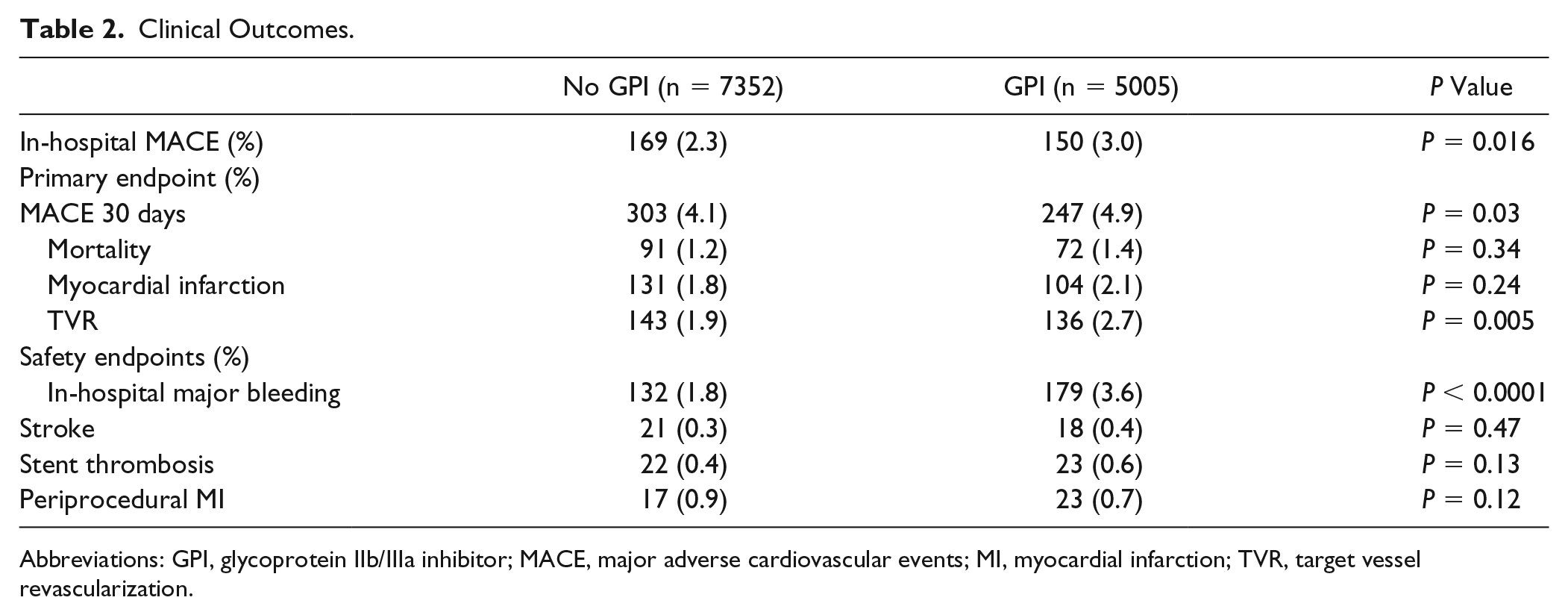
Abbreviations: GPI, glycoprotein IIb/IIIa inhibitor; MACE, major adverse cardiovascular events; MI, myocardial infarction; TVR, target vessel revascularization.
Figure 1 shows the annual use of GPIs as well as highlights the publication of a key thrombectomy trial, the Thrombus Aspiration during Primary Percutaneous Coronary Intervention (TAPAS) trial, and the introduction of the newer antiplatelet agents onto the Australian market.14-17 With the exception of 2005, the annual percentage in GPI use decreased over the study period with a statistically significant P for trend (<0.0001). Despite this decrease, the TAPAS trial and the introduction of prasugrel and ticagrelor did not appear to temporally influence GPI use.
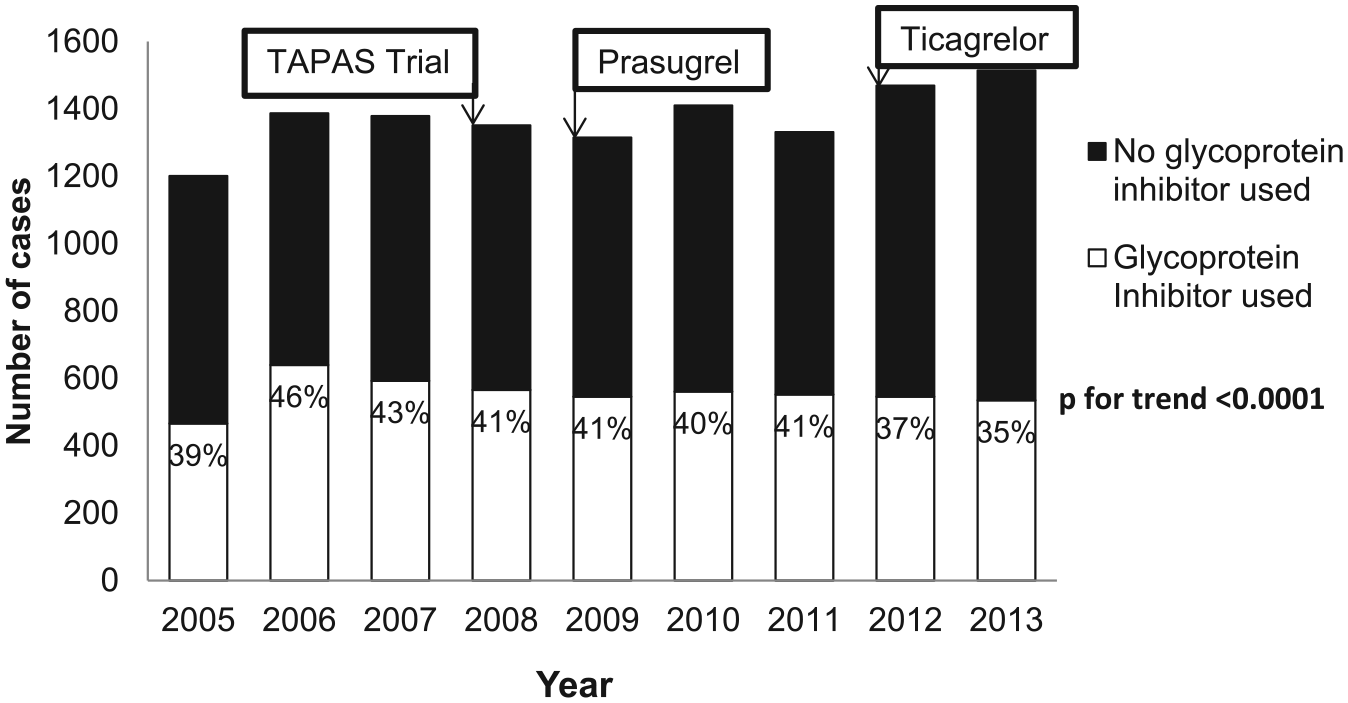
Annual use of GPIs (P for trend <0.001). A. Thrombus Aspiration during Primary Percutaneous Coronary Intervention (TAPAS) trial. B. Prasugrel available in Australia. C. Ticagrelor available in Australia.
Propensity score matching revealed no difference for GPI treatment effects estimation in 30-day mortality and 30-day MACE (odds ratio [OR] = 1.00, 95% CI = 0.99-1.004, and OR = 1.01, 95% CI = 0.99-1.02, respectively). It revealed a statistically significant increase in postprocedural in-hospital major bleeding for patients who received GPIs (OR = 1.01; 95% CI = 1.01-1.02). The multivariable predictors of MACE were chronic total occlusion, chronic renal impairment, disease extent, left anterior descending lesion, type B2 or C lesion, diabetes, STEMI, and clopidogrel use (Table 3). The multivariable analysis did not find the use of GPI to influence 30-day MACE. Predictors of in-hospital bleeding included the use of GPIs, age, sex, renal impairment (defined as estimated glomerular filtration rate <30 mL/min), left anterior descending lesion, and bypass graft disease. Bivalirudin was not a multivariable predictor of MACE or major bleeding.
Predictors of 30-Day MACE.
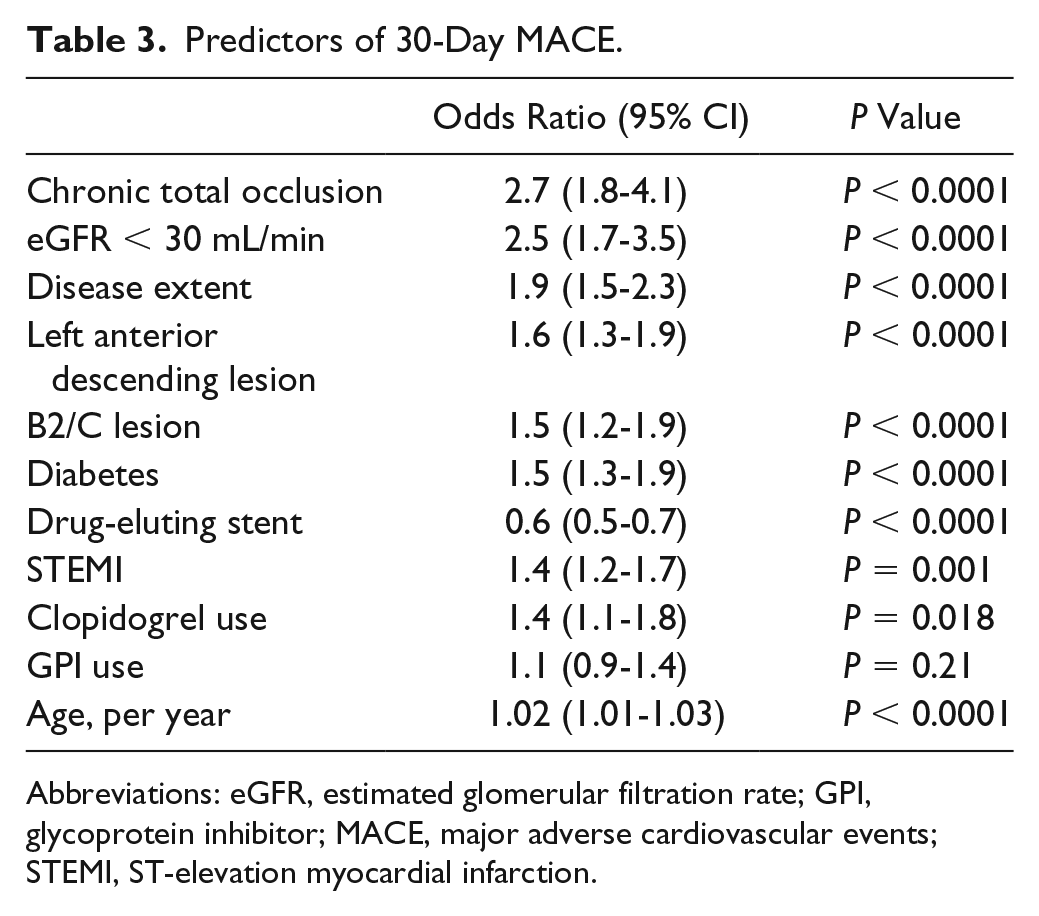
Abbreviations: eGFR, estimated glomerular filtration rate; GPI, glycoprotein inhibitor; MACE, major adverse cardiovascular events; STEMI, ST-elevation myocardial infarction.
Discussion
This longitudinal study from a large multicenter registry showed that use of GPIs in patients presenting with ACS was associated with a gradual decline in the use of GPIs over time. The result is in contrast to that reported by Motivala et al, 18 who showed an increase in GPI use between an earlier time period of 1999 to 2004. As in our study, they also found an increase in major in-hospital bleeding between 2002 and 2004, which appeared to be associated with GPIs. Although there did not appear to be a direct temporal relationship between the introduction of newer P2Y12 inhibitors or the use of aspiration thrombectomy and GPI use in ACS in our study, overall, the advances in strategies to manage patients with ACS have changed. This has likely resulted in the difference seen in our results, with a study period between 2005 and 2013.
Our study showed that GPIs appear to be used less frequently in patients with high-risk clinical features, and this may be considered a missed opportunity. A meta-analysis by Roffi et al 19 suggested that the use of GPI in NSTEMI and UA was associated with a reduction in death and nonfatal MI at 30 days in patients with diabetes. That meta-analysis evaluated 6458 patients with diabetes and showed that GPI use was associated with a significant mortality reduction at 30 days, from 6.2% to 4.6% (OR = 0.74; 95% CI = 0.59 to 0.92; P = 0.007). Conversely, the analysis showed that 23 072 nondiabetic patients had no survival benefit (3.0% vs 3.0%). Interestingly, in 1279 patients with diabetes undergoing PCI during index hospitalization, the use of GPIs was associated with a mortality reduction at 30 days from 4.0% to 1.2% (OR = 0.30; 95% CI = 0.14 to 0.69; P = 0.002). However, this finding was based on a nonrandomized assessment, so it can only be considered hypothesis generating.
Our study showed a small but significant increase in 30-day MACE in the unadjusted cohort, driven by target-vessel revascularization. However, this did not persist in the propensity matching or multivariable analyses. In a meta-analysis of more than 30 000 patients with ACS (24% of whom underwent PCI), Boersma et al 20 found that treatment with GPIs led to a 9% reduction in the relative risk of death or MI, with a 1% absolute increase in major bleeding. In the meta-analysis of high-risk patients with STEMI by Sethi et al, 21 they showed that GPI use in more than 7000 patients undergoing primary PCI was associated with a 25% reduction in mortality. Winchester et al 22 performed a meta-analysis of GPI use in ACS and PCI on the basis of trials performed in the contemporary era of stents and DAPT. Among patients with ACS, GPI use was associated with a significant reduction in nonfatal MI and an increase in minor bleeding but no differences in mortality or major bleeding. Despite the numerous differences in patient populations, timing of drug administration, and concomitant medical therapy, these meta-analyses suggest that GPI use in ACS patients undergoing PCI leads to some benefit but at the cost of increased bleeding.
Registry studies have also been conducted to evaluate the real-world use of these therapies. A registry study of 3047 patients receiving dual-antiplatelet therapy who underwent PCI for NSTEMI found results similar to those of our study. 8 Their study also found that patients treated with GPIs were younger with fewer comorbidities. Over a mean follow-up of 4.6 years, GPI use was associated with improved outcomes, although multivariate analysis (including propensity scoring) showed no benefit for either survival (P = 0.14) or MACE (P = 0.61). Similar to our study, GPI use was associated with an increased risk of major bleeding (P = 0.02).
In our study, GPIs appear to be used more frequently in patients with complex lesions and when thrombectomy devices are used, which reflects their higher use in the STEMI cohort in this study and is likely appropriate given current guideline recommendations.3,23 However, the recent neutral results of 2 thrombectomy trials may change this particular recommendation.24,25 The lack of a clear temporal association with reduced GPI use with the introduction of the newer antiplatelet agents ticagrelor and prasugrel in our study suggests that the availability of these more potent oral agents did not affect GPI prescribing habits.
The mechanisms of platelet inhibition in GPIs and P2Y12 inhibitors are distinct. P2Y12 inhibitors prevent adenosine diphosphate–dependent activation and expression of glycoprotein IIb/IIIa (GPIIb/IIIa) receptors. 26 GPIs, however, act on the final step of platelet aggregation by antagonizing GPIIb/IIIa receptors on activated platelets. 27 In light of this, guideline-recommended P2Y12 inhibitor pretreatment of patients presenting with ACS prior to PCI may partly explain the observed lack of efficacy of GPIs in this setting.
TIMI flow improved more in our patients following PCI in the cohort that received GPIs; however, this did not translate to an associated reduction in 30-day MACE. The small increase in 30-day MACE, driven largely by target-vessel revascularization, seen in the unadjusted cohort is likely reflective of the patient group who received them. Patients presenting with STEMI were more likely to receive GPIs and as such are at increased risk of 30-day MACE, particularly stent thrombosis, though there was no excess of stent thrombosis in our study. Of note, this higher MACE rate did not persist following propensity matching and in the multivariable analysis. Predictors of 30-day MACE from our multivariable analysis are consistent with those from other published registry studies, including diabetes and chronic renal impairment. 8 We observed clopidogrel use to be an independent predictor of 30-day MACE. Studies have previously demonstrated mortality benefit with the newer more potent antiplatelet agents prasugrel and ticagrelor. Although this mortality benefit may partly explain the perceived risk of MACE with clopidogrel, more in-depth analysis of this association is needed.15,16
GPI use was also associated with a significant increase in bleeding complications, which persisted in the adjusted analysis and is consistent with other published literature.8,28 Access site and retroperitoneal bleeding did not differ between patients treated with GPIs as compared with those who were not in our study; however, other (non–access site) bleeding did. Previous studies have shown that other non–access site bleeding is predominantly made up of gastrointestinal bleeding.29,30 Although other large registry studies have not looked at bleeding trends over time, the MIG registry recently showed that bleeding has increased over time. 31 This is an interesting finding given our trend in the reduction in use of GPIs. As the complexity of patients undergoing PCI increases with time, bleeding may persist despite a decline in GPI use.
More recently, analysis of the National Cardiovascular Data Registry of GPI use conducted by Safley et al, 28 included more than 970 865 patients. In that study unadjusted in-hospital mortality and major bleeding were more common with a GPI (2.4% vs 1.4% and 3.7% vs 1.5%, respectively; P < 0.001 for both). In contrast, GPI use was associated with lower in-hospital mortality on adjusted analyses, with relative risks ranging from 0.72 (95% CI = 0.50 to 0.97) with instrumental variable analysis to 0.90 (95% CI = 0.86 to 0.95) with propensity-matched analysis. The association of GPI use with bleeding remained in adjusted analyses (multivariable relative risk: 1.93, 95% CI = 1.83 to 2.04; propensity-matched relative risk: 1.83, 95% CI = 1.74 to 1.92; and instrumental variable analysis relative risk: 1.53, 95% CI = 1.27 to 2.13). A subgroup analysis revealed enhanced risk reduction in patients with a STEMI, high predicted mortality, and heparin-based anticoagulation. That registry-based study evaluated in-hospital mortality, whereas our study looks at 30-day MACE and may partially explain the difference in end points seen. Additionally, their study had a significantly larger sample size than ours, and this may be why a reduction in mortality was seen. The persistence of an excess of major bleeding is consistent with our data.
The data in the MIG registry are collected prospectively, and a limitation of our study includes the retrospective, observational nature of this analysis, which therefore may be influenced by unmeasured confounding factors. We attempted to control for this through propensity matching and multivariate analysis. Following these additional analyses, the only significant effect that remained from GPI use was the increased risk of bleeding. An additional limitation of this study is that our registry does not capture the specific GPI used or the timing of use. Thus, we are unable to comment on differences in GPIs or upstream versus intraprocedural administration. GPI as well as P2Y12 doses were also not captured in our registry data, which would be useful to determine a relationship between respective medication dosages and clinical outcomes.
Our definition of bleeding is based on other registries, including the National Cardiovascular Data Registry and, thus, does not follow the Bleeding Academic Research Consortium (BARC) bleeding definition. 32 The reason for this is 2-fold: the bleeding definition established by BARC was developed after the development of this registry, and retrospective collection of this information was not possible. Additionally, the BARC definition was developed for clinical trials and is, therefore, not well suited for registry data collection. In addition to this, our registry did not record data regarding oral anticoagulant use at discharge. Thus, we are unable to determine if patients on these medications were at greater risk of bleeding complications.
Conclusion and Relevance
We have demonstrated that there has been a gradual reduction in GPI use over time. These data also suggest that GPI use appears to be associated with ACS type and lesion complexity, as opposed to high-risk comorbidities. The use of GPIs was associated with a small but statistically significant increase in 30-day MACE in the unadjusted cohort, driven by target-vessel revascularization, though this did not persist in the propensity matching or multivariable analyses. In-hospital major bleeding increased with the use of GPIs. Based on our data, GPIs do not appear to improve 30-day MACE and are associated with increased bleeding. These results suggest that use of GPIs should not be recommended routinely in the present management of an ACS; however, evaluation via randomized controlled trials in the era of more potent oral antiplatelet agents may clarify this further.
Footnotes
Acknowledgements
Professor Duffy’s and Professor Reid’s work are funded by National Health and Medical Research Council of Australia Grants.
Authors’ Note
Melbourne Interventional Group Investigators
MIG Data Management Centre, CCRE, Monash University: Professor Chris Reid, Dr Nick Andrianopoulos, Ms Angela Brennan, Ms Vibhasha Chand, Dr Diem Dinh.
MIG Steering Committee: Professor Chris Reid, Associate Professor Andrew Ajani, Professor Stephen Duffy, Associate Professor David Clark, Dr Melanie Freeman, Dr Chin Hiew, Dr Nick Andrianopoulos, Dr Ernesto Oqueli, Ms Angela Brennan.
The following Investigators, Data Managers and Institutions participated in the MIG Database:
Alfred Hospital: SJ Duffy, JA Shaw, A Walton, A Dart, A Broughton, J Federman, C Keighley, C Hengel, KH Peter, D Stub, W Chan, J O’Brien, L Selkrig, K Rankin, R Huntington, S Pally
Austin Hospital: DJ Clark, O Farouque, M Horrigan, J Johns, L Oliver, J Brennan, R Chan, G Proimos, T Dortimer, B Chan, V Nadurata, R Huq, D Fernando, A Al-Fiadh, M Yudi, H Sugumar, J Ramchand, H Han. S Picardo, L Brown
Ballarat Base Hospital: E Oqueli, C Hengel, A Sharma, B Zhu, N Ryan, T Harrison
Box Hill Hospital: M Freeman, L Roberts, M Rowe, G Proimos, Y Cheong, C Goods, D Fernando, A Teh, S Parfrey, J Ramzy, A Koshy, P Venkataraman, D Flannery
Geelong Hospital: C Hiew, M Sebastian, T Yip, Michael Mok, C Jaworski, A Hutchinson, C Cimenkaya, P Ngu, B Khialani, H Salehi, M Turner, J Dyson, B McDonald, D Van Den Nouwelant, K Halliburton
Monash University: H Krum, C Reid, N Andrianopoulos, AL Brennan, V Chand, D Dinh, BP Yan
Royal Melbourne Hospital: AE Ajani, R Warren, D Eccleston, J Lefkovits, R Iyer, R Gurvitch, W Wilson, M Brooks, S Biswas, J Yeoh
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Yudi is supported by a combined National Health and Medical Research Council and National Heart Foundation Postgraduate Scholarship. The Melbourne Interventional Group acknowledges unrestricted educational grant funding from: Abbott Vascular, Astra-Zeneca, Medtronic, MSD, Pfizer, Servier, and The Medicines Company. These companies do not have access to the data and do not have the right to review manuscripts before publication.