
Abstract
Introduction
Psoriasis is a chronic, immune-mediated disease affecting approximately 7.4 million adults in the United States. 1 The most common type of psoriasis is psoriasis vulgaris (also known as plaque psoriasis), which comprises 90% of cases. 1 It is clinically characterized by sharply demarcated, erythematous, pruritic plaques with overlying silvery-white scale most frequently distributed on extensor surfaces of the elbows, knees, scalp, and intertriginous areas. 1 In addition to its cutaneous manifestations, psoriasis affects patients’ mental health, presenting as anxiety, depression, or low self-esteem.2,3 Furthermore, its association with several comorbidities, including psoriatic arthritis, diabetes, cardiovascular disease, and metabolic syndrome, highlights the importance of adequate treatment. 4
Psoriasis is characterized by chronic inflammation leading to epidermal hyperproliferation and abnormalities in keratinocyte differentiation.5,6 The tumor necrosis factor-α/interleukin 23/Th17 axis is important in the pathophysiology of plaque psoriasis. 5 Accordingly, treatments primarily combat the chronic inflammatory processes. Treatments include topical agents, phototherapy, and systemic therapies, including biologics targeting specific inflammatory pathways. Whereas modality selection is dependent on disease severity, comorbidities, and patient preference, topical therapies are often first-line for mild disease and used in combination with systemic agents for more severe presentations. Topicals provide symptomatic relief and decrease the need for higher doses of systemic agents. 7
Despite the large impact of psoriasis on patients’ lives, adherence to topical therapy can be as low as 61%, even lower with long-term use of topicals.8,9 Poor adherence can be explained in part by fear of side effects, disaffection with efficacy, inconvenience of application, dislike of the vehicle, cost, and complexity of regimens.10,11 Lack of accountability via early follow-up appointments, which may compel patients to be more adherent, may play a large role too. Combinational topical therapies that reduce the complexity of treatment and the risk of side effects may improve adherence and efficacy.
A combination treatment of halobetasol propionate (HP) and tazarotene (TAZ) was approved by the United States Food and Drug Administration in April 2019. The HP formulation used in Duobrii is a high- to super-high-range corticosteroid (per vasoconstrictor assays) with anti-inflammatory effects. Its side effects include skin atrophy, leukoderma, folliculitis, telangiectasias, and possible suppression of the hypothalamic-pituitary-adrenal (HPA) axis. 12 TAZ, on the other hand, is a vitamin A derivative that improves psoriasis primarily via effects on keratinocyte differentiation. TAZ side effects include application site irritation. 13 Compared with regimens of topical corticosteroids or TAZ, using both topicals is more efficacious and tolerable than either one alone. 14 However, adherence to 2 separate topical products is worse than adherence to 1 combined product. HP/TAZ was developed to address this barrier. In this systematic review, we present and assess phase II and phase III clinical trial data pertaining to efficacy and safety of HP/TAZ combinational topical therapy.
Methods
A systematic review (January 2005 to July 2019) was conducted using the terms halobetasol, tazarotene, halobetasol propionate/tazarotene (DuobriiTM), Duobrii, and IDP-118 in MEDLINE (PubMed) and EMBASE databases. Articles written in English were extracted. As a supplemental search strategy, ongoing and unpublished studies were identified using the publicly available web page ClinicalTrials.gov. Articles included in the review were limited to phase II and phase III trial results (Table 1).
Review of Phase II and III Clinical Trials of HP/TAZ Combination in the Treatment of Moderate to Severe Plaque Psoriasis.
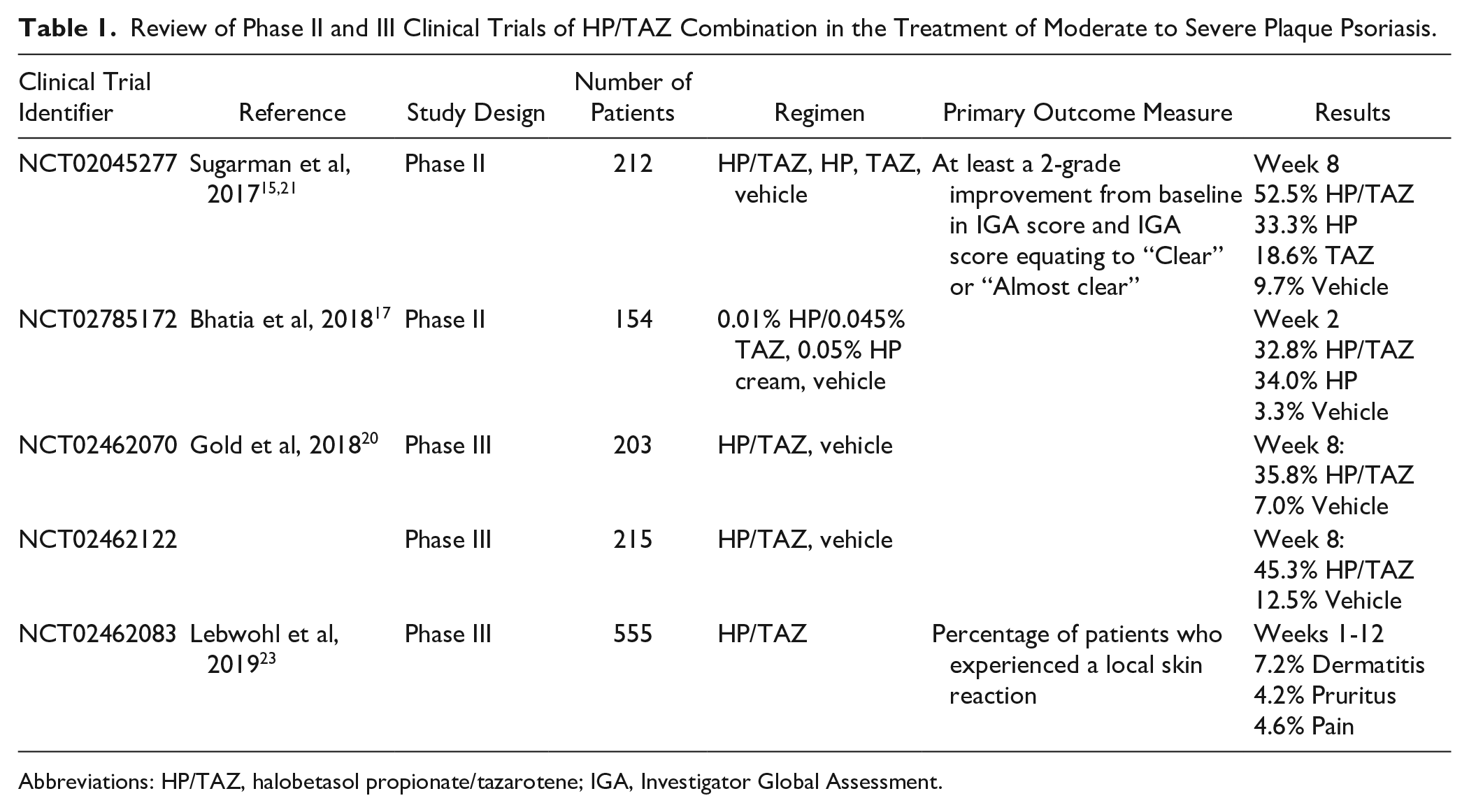
Abbreviations: HP/TAZ, halobetasol propionate/tazarotene; IGA, Investigator Global Assessment.
Results
Phase II Clinical Trials
A phase II multicenter, randomized, double-blinded clinical trial (NCT02045277) was conducted with 212 adult patients with moderate or severe plaque psoriasis. 15 Participants had baseline Investigator Global Assessment (IGA) scores of 3 or 4, with affected body surface area (BSA) of 3% to 12%. They were randomized in a 2:2:2:1 ratio to HP/TAZ lotion, HP lotion, TAZ lotion, and vehicle lotion groups. The topicals were applied once daily for 8 weeks, with clinical assessment performed at 2, 4, 6, and 8 weeks and 4 weeks after treatment completion (week 12). 15 Treatment success was defined as an improvement of IGA score by at least 2 grades and IGA score of clear or almost clear. Overall, by week 8, the HP/TAZ, HP alone, TAZ alone, and vehicle groups all had at least 1-grade improvement in IGA (74%, 33.3%, 16.9%, and 12.9% of patients, respectively), but the highest percentage of patients with improvement was in the HP/TAZ cohort. Furthermore, at the end of week 8, 52.5% of HP/TAZ patients reached treatment success compared with 33.3% in the HP group (P = 0.030), 18.6% in the TAZ group (P < 0.001), and 9.7% in the vehicle group (P < 0.001). 15 Four weeks after concluding the treatment period (week 12), 67.7% of the HP/TAZ-treated participants who achieved treatment success maintained their improvement based on IGA score compared with 61.9% of those in the HP group and 54.5% in the TAZ group. 15 Overall, of all groups, the TAZ group had lowest adherence, defined as the percentage of patients who applied 80% to 120% of the total expected doses over the course of the treatment period. TAZ patients had a 79.7% adherence compared with 94.9% in the HP/TAZ group. 15 Side effects, such as application site pain, erythema, and pruritus occurred most often in the TAZ group (22.4%) compared with 10.6% in the HP/TAZ cohort. The HP and vehicle groups did not report side effects. As such, the TAZ treatment group had the highest proportion of treatment discontinuation resulting from adverse effects (AEs). In the other groups, side effects reported were skin atrophy in 3 patients in the HP/TAZ cohort, compared with 1 patient applying HP. Telangiectasias were reported in 6 patients treated with HP/TAZ, and folliculitis was documented in patients in all 3 treatment groups. 15
HP/TAZ decreased IGA score compared with vehicle (P = 0.047) and TAZ lotion (P = 0.029) as early as week 2. 16 Additionally, by week 2, 47.5% of HP/TAZ-treated patients were classified as “mild,” “almost clear,” or “clear.” In comparison, 33.3% of HP-, 16.9% of TAZ-, and 12.9% of vehicle-treated patients achieved the same levels of improvement. Subjective symptoms were also assessed at this interval. Of the patients in the HP/TAZ group, 45.6% had improvement in baseline itch, 42.2% in dryness, and 55.9% in burning/stinging. These values were similar to those treated with HP alone but were relatively large improvements over the TAZ-alone group (30.8%, 35.4%, and 13.3%, respectively). 16
Another multicenter, randomized, double-blinded, parallel-group phase II clinical trial (NCT02785172) compared 0.01% HP/0.045% TAZ lotion and HP 0.05% cream with vehicle in 154 individuals with moderate to severe psoriasis. Comparison of HP/TAZ with the 0.05% HP cream was made to assess if a lower concentration of HP in the combinational treatment (0.01%) would be as effective while promoting a better safety profile. Adult patients were randomized into treatments group in a 2:2:1 (HP/TAZ:HP:vehicle) ratio. The primary efficacy end point was defined as the percentage of patients with at least a 2-grade improvement from baseline IGA score and IGA score of clear or almost clear at week 2. Also assessed were clinical symptoms and changes in BSA involvement. 17 Overall, treatment success was achieved in 32.8%, 34.0%, and 3.3% of patients using HP/TAZ lotion, HP cream, and vehicle, respectively. Compared with vehicle, HP/TAZ lotion and 0.05% HP cream were more successful than vehicle in reducing erythema (34.4% and 43.5%, respectively), plaque elevation (54.1% and 50.8%, respectively), and scaling (60.7% and 50.8%, respectively). During this 2-week period, AEs were reported; the most common was application site pain. 17
A post hoc analysis of the first-discussed phase II clinical trial (NCT02045277) used a disease severity composite tool (IGA×BSA) to evaluate improvement in the group treated with HP/TAZ. The IGA×BSA tool is an alternative measurement correlating well with the commonly used Psoriasis Area and Severity Index. With this measurement, patients in the HP/TAZ lotion group had a 63.5% reduction in mean IGA×BSA composite score by week 8 (P < 0.001 compared with both TAZ and vehicle). This improvement was maintained at week 12 compared with the TAZ (P < 0.001), HP (P = 0.003), and vehicle (P < 0.001) groups. 18 On average, 25% IGA×BSA improvement was achieved at 1.9 weeks, whereas 50% IGA×BSA improvement was obtained by 4.6 weeks; 47.5% of the patients treated with HP/TAZ reached 75% IGA×BSA by week 8. 18
Another post hoc analysis of phase II clinical trial data (NCT02045277) assessed synergy of the HP/TAZ formulation. Synergy was defined as HP/TAZ success rate greater than the sum of the HP group and TAZ group success rates, such that the HP/TAZ success rate divided by the sum of HP group and TAZ group success rates was >1.0. At week 8 and relative to improvement in vehicle-treated patients, 42.8% of patients treated with HP/TAZ lotion had treatment success (defined as IGA score equaling “clear” or “almost clear”) compared with 32.5% for HP plus TAZ (ratio of 1.3). Furthermore, the percentage change in baseline IGA×BSA score was 51.6% for the HP/TAZ group compared with 40.6% for the HP plus TAZ group (ratio 1.3). At week 12, 31.3% of patients treated with HP/TAZ maintained treatment success compared with 20.0% of HP plus TAZ patients relative to vehicle (ratio 1.6). Furthermore, the percentage changes in baseline IGA×BSA score relative to vehicle were 47.3% and 34.2% (ratio 1.4), respectively. 19
Additionally, an ongoing phase II clinical trial (NCT02785159) is comparing the efficacy and safety of HP/TAZ lotion, TAZ cream, vehicle lotion, and vehicle cream.
Phase III Clinical Trials
Two multicenter, randomized, double-blind phase III clinical trials (study 1: NCT02462070; study 2: NCT02462122) were conducted comparing HP/TAZ with vehicle.20,21 In these studies, 418 adults with moderate to severe plaque psoriasis with baseline IGA scores of 3 or 4 and 3% to 12% BSA were randomized (2:1 ratio) to receive HP/TAZ lotion or vehicle lotion once daily for 8 weeks with a subsequent 4-week follow-up. In both studies, the primary end point evaluated was an at least 2-grade improvement in IGA score and “clear” or “almost clear.” At the end of the treatment period (week 8), 35.8% of HP/TAZ-treated patients in study 1 (NCT02462070) and 45.3% of such patients in study 2 (NCT02462122; pooled mean of 40.6%) were considered treatment successes compared with merely 7.0% and 12.5% of vehicle-treated patients (pooled mean of 9.9%; P < 0.001).20,21 At the 4-week follow-up (week 12), 33.3% of patients in study 1 (NCT02462070) and 33.4% of patients in study 2 (NCT02462122) maintained treatment success compared with 8.5% and 8.8% of vehicle-treated patients in both studies, respectively (P < 0.001).20,21 The most commonly reported treatment-related AEs in both studies were contact dermatitis (6.3%), application site pain (2.6%), and pruritus (2.2%).20,21
A post hoc analysis of the 2 phase III clinical trials using IGA×BSA to assess efficacy of HP/TAZ was carried out. 22 A ≥75% reduction in IGA×BSA score from baseline (IGA×BSA-75) was considered a clinically significant outcome. The mean percentage change in IGA×BSA from baseline by week 8 was 51.9% in the HP/TAZ group compared with 9.21% in the vehicle group (P < 0.001). At week 8, 41.7% of patients in the HP/TAZ group achieved IGA×BSA-75 compared with 9.9% treated with vehicle (P < 0.001). 22
A long-term, open-label phase III study (NCT02462083) evaluated safety and tolerability of HP/TAZ lotion. 23 A total of 555 adult patients aged 19 to 87 years were treated with HP/TAZ and followed for up to 1 year with particular focus on safety and tolerability. Participants were treated with once-daily HP/TAZ for 8 weeks and as needed thereafter. Clinical evaluation was performed at baseline, week 2, week 4, and every 4 weeks thereafter. Treatment success was defined as an IGA score of either 0 (clear) or 1 (almost clear). 23 In addition to the primary outcome measure of the percentage of patients with local skin reaction, efficacy was also evaluated. At 12 weeks, patients were evaluated for response. In all, 26 patients (4.6%) discontinued treatment because of lack of efficacy (defined as ≥1-grade improvement in IGA). Those not achieving treatment success (defined as IGA score of 0 or 1—ie, clear or almost clear) were continued on treatment for 4 more weeks. Patients who did not have treatment success by week 24 were discontinued from the study. Overall, 20.9% of patients were discontinued from treatment at 24 weeks for lack of treatment success. The most common AEs were dermatitis (5.1% > 12-24 weeks; 2.5% > 24-36 weeks; 0.9% > 36 weeks), pruritus (1.5% > 12-24 weeks; 1.7% > 24-36 weeks; 0.9% > 36 weeks), and pain (0.5% > 12-24 weeks; 0.4% > 24-36 weeks; 0.5% > 36 weeks); 7.5% of patients discontinued therapy secondary to adverse events. 23 The higher rate of AEs earlier on in the treatment period may be a result of initial sensitization or adverse response that is appreciable during the initial treatment period. This finding falls in line with those of the pivotal studies that document a peak in AE incidence by 60 days, remaining stable thereafter throughout the study periods. 23
Discussion
Mechanism of Action
HP/TAZ is approved as a once-daily 0.01%/0.045% combination lotion. HP is a topical corticosteroid (6-α-fluoroclobetasol 17-propionate). 24 It induces phospholipase A2 inhibitory proteins, which decrease inflammatory cytokines. 25 TAZ is a retinoid that undergoes esterase hydrolysis into its active form, tazarotenic acid. Tazarotenic acid binds to retinoic acid receptors (RARs), specifically RAR-γ and RAR-β, and promotes keratinocyte differentiation while also inhibiting proliferation and inflammation through expression induction of TAZ-induced genes.14,26 Although HP and TAZ have similar anti-inflammatory and antiproliferative effects, they elicit these responses via different mechanisms, possibly leading to a synergistic response when used in combination. This is the premise under which the HP/TAZ combination product was created.
Combination Therapy in Psoriasis Treatment
Combination therapies are often prescribed for patients with psoriasis. Most often, such regimens include a topical corticosteroid and one of the following: calcipotriene, calcitriol, TAZ, or ultraviolet B phototherapy. Sometimes patients are encouraged to use even more treatments, such as keratolytics, along with these treatments. When multiple different treatments are needed for different areas (solutions for the scalp, low-potency topicals for the face and genitals, high-potency ointments for elbows and knees), the complexity of the treatment regimen can be overwhelming. Simplifying treatment routines to 1 topical application per day encourages adherence.8,9 Therefore, formulations containing 2 active medications are promising alternatives that may encourage adherence, which may subsequently lead to increased efficacy, tolerability, and rapid responses. Examples of these 2-in-1 formulations are the already established calcipotriol/betamethasone combination products and the more recently approved HP/TAZ therapy.
In addition to possibly increasing adherence, combination therapy may enhance efficacy through synergy of the drugs combined. When 2 drugs are used together, the 2 active ingredients can have additive or synergistic effects. In 2 post hoc analyses of phase II clinical trial data, the HP/TAZ combination was calculated to be more effective than the sum of separate HP and TAZ products.18,19 Additionally, at least 1 trial compared HP 0.01%/TAZ 0.045% with HP 0.05% (Ultravate) and with vehicle. 17 The goal is to compare a drug with a better safety profile (less corticosteroid) with the higher-concentration corticosteroid and show that it was more effective even with a lower dose in order to offer a combinational regimen with an equivalent or better safety profile, such as by using less corticosteroid. In fact, HP/TAZ lotion minimized TAZ’s irritation and reduced the local AEs secondary to halobetasol. 15
Pharmacokinetics and Pharmacodynamics
An open-label, randomized trial was conducted in 22 adults with moderate to severe psoriasis (20% or more BSA) to assess the pharmacokinetics of halobetasol, TAZ, and tazarotenic acid, specifically with respect to detectable blood concentrations. Overall, after once-daily dosing for 28 consecutive days, systemic concentrations of HP (lower limit of quantification of 50 pg/mL) was detectable in 13 of 22 patients, whereas systemic concentrations of TAZ were similarly detectable (5 pg/mL) in 18 of 22 patients. 27
Vasoconstrictor assays of the HP/TAZ combination resulted in its classification as a high- to super-high-range corticosteroid. 27 Additionally, 20 patients were assessed for HPA axis suppression after 4 weeks of daily HP/TAZ application. A serum cortisol level of 18 mg/dL or less after stimulation with cosyntropin was considered as HPA axis suppression. Overall, 3 of 20 patients (15%) had HPA axis suppression at week 4, whereas zero patients had suppression at week 8. 27 A review of 15 clinical trials and 20 case reports of topical corticosteroids noted no pathological adrenal suppression within the limits of current US Food and Drug Administration use. 28 As such, HP/TAZ is unlikely to cause clinically significant HPA axis suppression if used as prescribed.
Treatment Onset and Duration
HP/TAZ lotion has a more rapid onset of action, showing more significant improvement earlier in the treatment process, compared with its individual drugs independently or vehicle.15,16 Two weeks into treatment, clinical signs of plaque elevation and scaling were improved compared with its monads or vehicle, and erythema was improved compared with TAZ. 16 In patients with psoriasis, this is important because one of the treatment goals rated by patients as most important is timely improvement. 29 Overall, HP/TAZ treatment was associated with a significant reduction in signs and symptoms of psoriasis, improvement in quality of life, and substantial reductions in affected BSA. However, patients with >12% BSA affected were excluded in most trials of HP/TAZ lotion, so its efficacy and safety in patients with more extensive disease are not well characterized.
Additionally, HP/TAZ was associated with improvement in disease severity even after cessation of treatment. 30 TAZ may induce longer remissions than do topical corticosteroids. TAZ use in the combination may help reduce rebound worsening of psoriasis, which can occur with topical corticosteroids alone. 31 However, most of the clinical trials described above only extended to 4 weeks after treatment cessation, so longer-term effects have not been studied yet.
Adverse Events
The most commonly reported adverse events caused by HP/TAZ include contact dermatitis, application site pain, and skin atrophy.15,17,20,21 Some patients stopped treatment because of AEs (4.0% in the HP/TAZ group compared with 2.8% in the vehicle group). 20 In the HP/TAZ group, 35.9% of patients reported AEs compared with 21.4% of patients treated with vehicle; 85.6% of these adverse events were mild or moderate. The most common adverse events themselves were contact dermatitis (6.3%), pruritus (2.2%), and application site pain (2.6%). Three patients in the HP/TAZ groups (1.1%) reported severe adverse events, but none were considered treatment related (cellulitis, staphylococcal pneumonia, and anemia). 20
Overall, skin atrophy and telangiectasias in the HP/TAZ treatment group occurred with a frequency similar to those in the HP treatment group. When used as part of the HP/TAZ combination, TAZ irritant AEs were reduced, resulting in an increase in adherence in the combination treatment group. In longer-term studies, however, HP/TAZ discontinuation rates resulting from adverse events were similar to those of retinoid-only treatment groups.12,23 Additional side effects of the HP/TAZ combination include increased risk of photosensitivity, subcapsular cataracts, and glaucoma, reflecting previously established side effects of corticosteroids and retinoids. 27
Contraindications
HP/TAZ contains a vitamin A derivative from the TAZ component and is contraindicated in pregnant patients and women of reproductive age not on adequate birth control. No reports of birth defects have been reported with topical TAZ use. 13 A pregnancy test is recommended 2 weeks prior to beginning this treatment. If the patient becomes pregnant, treatment should promptly be discontinued. 27 HP/TAZ is not approved for the pediatric population. However, ongoing studies are assessing its safety and efficacy in children (NCT03988439).
Relevance to Patient Care and Clinical Practice
Topical treatments for psoriasis are available to patients with moderate to severe psoriasis. Topical treatments can be used as the sole agent for local disease, but their efficacy is limited by poor adherence. 8 For more severe disease, combination treatment is often used, but this further reduces adherence, especially if both drugs are topical. Combining HP and TAZ may present a more favorable once-daily regimen with 2 drugs in 1 lotion. This is further bolstered by clinical trials noting this combination’s greater efficacy than the efficacy of either of its component products.17,18 Just like the long-available topical calcipotriene-betamethasone combination products, which combine a topical corticosteroid with a vitamin D analog, HP/TAZ adds another combinational topical regimen to the dermatologist’s arsenal. However, longer-duration postsurveillance studies are needed to assess long-term efficacy, especially with real-world use.
Another important consideration in adherence to any treatment is cost, which when prohibitive can negatively affect adherence. Currently, coupon pages such as GoodRx list the cost of halobetasol 0.05% ointment (50 g) as $37 to $68 and the cost of TAZ 0.1% cream (30 g) as $65 to $125. Meanwhile, the cost of Duobrii, with coupon, is $822 to $891. Cost-effectiveness or value-based studies comparing Duobrii to treatment with each of its individual components together or in combination are lacking. Nevertheless, for motivated patients who have insurance plans that do not cover this combinational medication, purchasing the individual components of the treatment to be applied together may be a reasonable option. However, this again leads to a regimen of 2 different topical medications that must be combined, leading to an unfavorable setting for adherence.
Conclusion
HP/TAZ appears to be an effective combination topical medication for the treatment of psoriasis in adults. It is efficacious in short-term trials of 8 to 12 weeks; however, longer-term data are required to render more substantial conclusions. This is especially true because in the poststudy period 4-week follow-ups, improvements regressed.18,19 Nevertheless, its effects appear consistent in trials and are important in justifying its potential use over topical monotherapy in patients who are not improving.18,19 However, HP/TAZ is still a topical medication susceptible to factors affecting intentional nonadherence in the real world of clinical care: dissatisfaction with efficacy and inconvenience, which are more likely to manifest in everyday practice, an environment very different from clinical trials. 10
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Steven Feldman has received research, speaking and/or consulting support from a variety of companies, including Galderma, GSK/Stiefel, Almirall, Leo Pharma, Boehringer Ingelheim, Mylan, Celgene, Pfizer, Valeant, Abbvie, Samsung, Janssen, Lilly, Menlo, Merck, Novartis, Regeneron, Sanofi, Novan, Qurient, National Biological Corporation, Caremark, Advance Medical, Sun Pharma, Suncare Research, Informa, UpToDate, and National Psoriasis Foundation. He is the founder and majority owner of ![]() and founder and part owner of Causa Research, a company dedicated to enhancing patients’ adherence to treatment. Vignesh Ramachandran, Brooke Bertus, and Arjun Bashyam have no conflicts to disclose.
and founder and part owner of Causa Research, a company dedicated to enhancing patients’ adherence to treatment. Vignesh Ramachandran, Brooke Bertus, and Arjun Bashyam have no conflicts to disclose.
Funding
The authors received no financial support for the research and/or authorship of this article.