
Abstract
Background:
Response-guided hepatitis C therapy was standard with interferon-based regimens but is not used for direct-acting antivirals (DAAs). Week 4 viral kinetics may predict sustained virological response (SVR) with DAAs, but it is unclear whether extending therapy in slow responders affects outcomes.
Objectives:
The primary objective was to compare SVR rates between traditional and extended duration groups. Secondary objectives were to compare SVR rates among subgroups and to determine factors associated with SVR.
Methods:
This institutional review board–approved, retrospective, single-center study identified patients with chronic hepatitis C virus (HCV) infection with detectable week 4 HCV RNA who were treated with DAAs. Patients were excluded for early discontinuation, treatment regimen not recommended first-line, or missing HCV RNA labs. Patients were stratified into traditional and extended duration groups. The primary end point was SVR. Secondary end points included factors associated with SVR and rationale for extension of therapy duration.
Results:
A total of 363 patients were included; 58 (16%) received extended therapy. Patients were primarily genotype 1a (70%) and treatment naïve (80%). More than half had advanced fibrosis or cirrhosis. SVR12 rates were 100% in the extended duration group and 96.7% in the traditional duration group (P = 0.37). There were no associations with SVR and prespecified patient-specific factors. Sample size was limited.
Conclusion and Relevance:
Based on these findings, a recommendation for extension of therapy cannot be made for patients with detectable HCV RNA at week 4 of treatment at this time. Cost analyses may help guide recommendations to re-treat rare failures versus extend therapy in all slow responders.
Hepatitis C virus (HCV) is the most common blood-borne pathogen in the United States.1,2 HCV is associated with more deaths in the United States than 60 other infections combined. 3 Its incidence continues to increase despite curative therapies and preventive measures.4,5 The infection disproportionately affects veterans, making the US Department of Veterans Affairs (VA) the largest HCV care provider in the nation. 6 The VA has been aggressive in efforts to identify and treat HCV. 7 Cure is associated with reductions in all-cause and liver-related mortality, hepatocellular carcinoma (HCC), and liver transplantation.8-10
Response-guided therapy (RGT), using on-treatment viral kinetics to determine treatment duration, was used with interferon-based regimens. Patients with slow virological response warranted therapy extension.11-14
Sofosbuvir was the first direct-acting antiviral (DAA) to be studied with a fixed duration of 12 weeks for all patients. Registration studies showed <1% of patients with detectable HCV RNA at week 4 of treatment.14,15 Similarly, <1% of patients in the ledipasvir/sofosbuvir registration trials had detectable HCV RNA at week 4 of treatment.16-18 High cure rates with fixed treatment duration challenged the utility of RGT for potent DAAs. Use of RGT declined as a result of improved safety and efficacy of DAAs, shortened treatment duration, and conflicting data on the correlation between viral kinetics and SVR in registration trials.13,14
However, real-world, postapproval studies of sofosbuvir-containing regimens have demonstrated a larger proportion of patients with detectable HCV RNA at week 4, reporting up to 30% of patients.19,20 Additional evidence has suggested that viral response at week 4 is still predictive of SVR12 with interferon-free DAA regimens, particularly in more difficult-to-treat populations such as genotype 3 patients with cirrhosis.21-23 A study of 21,095 veterans on interferon-free regimens showed a significant association between detectable week 4 HCV RNA and lower SVR rates, which decreased with increasing baseline viral load. 24
The American Association for the Study of Liver Diseases and Infectious Diseases Society of America (AASLD-IDSA) hepatitis C guidance recommends measuring HCV RNA at week 4 of treatment for all patients on DAA therapy. If week 4 HCV RNA is detectable, the recommendation is to recheck HCV RNA at week 6. However, because of insufficient evidence, the guidance states that no recommendation can be made at this time based on the results of these tests to either stop treatment or extend therapy duration. 25
Given the limited outcomes data for extension of therapy, the purpose of this study was to determine whether extending therapy duration in patients with detectable HCV RNA at week 4 of treatment improves rate of SVR.
Methods
This institutional review board–approved, retrospective, cohort study was conducted within a single VA health care system. Patients were identified using the local pharmacy DAA treatment database. All patients within the database were screened for inclusion. Patients were eligible for inclusion if they had a diagnosis of chronic HCV infection and initiated DAA therapy between January 2014 and July 2018. Included patients had to be slow virological responders, defined as those with detectable HCV RNA at or after week 4 of therapy (either detected but below the lower limit of quantification [LLOQ] or above the LLOQ). Week 4 was chosen as the cutoff for this study because it has been the most studied in relation to decreased rates of SVR and is the focus of the AASLD-IDSA guidance.
Patients were excluded if they were on a treatment regimen no longer recommended as first-line in the AASLD-IDSA guidance current at the time of study approval (November 2018). Patients were also excluded if they discontinued therapy early, were initially prescribed a 24-week duration of therapy, had not completed therapy by October 2018, or lacked HCV RNA labs at 4 ± 2 weeks and at least 12 weeks after end of treatment.
Within the health care system, chronic HCV is treated by a multidisciplinary hepatology team, including physicians, nurse practitioners, nurses, and a pharmacist. Baseline labs that include HCV RNA, genotype, complete blood count, comprehensive metabolic panel, and international normalized ratio are required. Resistance testing may be performed at provider discretion, when clinically appropriate for requested regimen. Electronic prior authorization drug requests (PADRs) are submitted for review and approval by the hepatology clinical pharmacy specialist. The initial PADR requires the provider to specify regimen (DAA, duration, with or without ribavirin) and pertinent information such as genotype, fibrosis severity, and prior treatment experience. Regimens are selected in accordance with AASLD-IDSA guidance and Food and Drug Administration prescribing information based on patient-specific factors. The initial PADR approval note documents the anticipated therapy duration (up to 24 weeks) but only provides the initial 8-week supply of medication. A continuation PADR is required prior to 8 weeks of therapy to assess for adherence and safety; this is also used as a mechanism for the pharmacist to recommend or provider to request extended duration of therapy. The continuation PADR approval covers the remaining supply of medication.
The standard practice within the health care system is to measure HCV RNA every 2 weeks after treatment initiation until it becomes undetectable, at the end of treatment, and 12 weeks after the end of treatment. HCV RNA measurement was captured using the Roche COBAS AmpliPrep/COBAS TaqMan HCV v2.0 (quantitative) assay. The LLOQ is 15 IU/mL.
Included patients were categorized into traditional duration or extended duration of therapy for data analysis. Traditional duration was defined as receipt of initially prescribed duration of therapy. Extended duration was defined as receipt of therapy duration longer than initially prescribed. With no current guideline recommendations about extending therapy duration, the choice to extend and duration of extension was provider and patient specific. If therapy duration was extended, rationale was consistently documented in the continuation PADR approval note.
The primary end point was sustained virological response, defined as HCV RNA SVR12 were assessed in prespecified subgroups, including HCV genotype, prior treatment experience, fibrosis severity (advanced fibrosis or cirrhosis), DAA regimen, and week of therapy HCV RNA became undetectable. Advanced fibrosis or cirrhosis was determined by F3/F4 on biopsy when available, FibroScan >9.5 kPa, FIB4 >3.25, or imaging indicative of cirrhosis. Additional analyses include factors associated with SVR12 and provider rationale for extension of therapy duration. Factors evaluated for association with SVR12 included gender, race, HCV genotype, treatment experience, presence of advanced fibrosis or cirrhosis, treatment regimen, ribavirin use, HIV coinfection, and HCC. Because there is no current guidance on extension of therapy duration, provider rationale was collected in an attempt to characterize the rationale. Categories for extension of therapy included the following: excessive delay to undetectable HCV RNA, presence of advanced fibrosis or cirrhosis, high initial HCV RNA, prior treatment experience, HCV genotype, resistance, ribavirin intolerance, and other. All data except rationale for extending duration were obtained from the HCV treatment database. Rationale for extending duration was collected by manual chart review of continuation PADR approval notes.
Descriptive data are reported for baseline characteristics as mean ± SD or frequency (%). Descriptive statistics are also reported for subgroup analyses as frequency (%) achieving SVR12 and for provider rationale for extension of therapy duration. Contingency tables and the Fisher exact test were used to analyze associations between SVR12 and gender, race, genotype, treatment experience, fibrosis severity, treatment regimen, HCC, and HIV coinfection. A P value ≤0.05 was considered statistically significant. Analyses were performed using SAS Version 9.4 (SAS Institute, Cary, NC).
Results
A total of 1358 patients treated within the health care system were evaluated for eligibility. Overall, 34.7% (472/1358) of patients treated with DAA therapy for chronic HCV within the health care system experienced slow virological response. Of the 1358 patients evaluated, 995 were excluded (Figure 1).
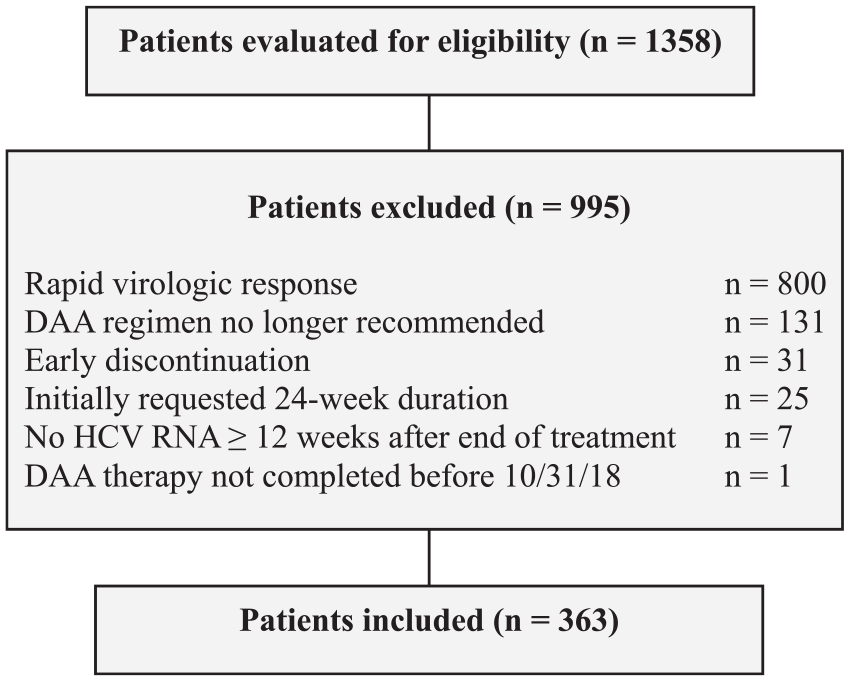
Flow of patients for inclusion and exclusion.
A total of 363 patients were included and were categorized as either traditional duration of therapy (n = 305) or extended duration of therapy (n = 58). Baseline characteristics were similar between groups, with the exception of a numerically greater proportion of genotype 1b in the traditional duration group and advanced fibrosis or cirrhosis in the extended duration group (Table 1). Patients were a mean age of 61 years, approximately 95% male, 70% African American, 70% with genotype 1a, and 80% treatment naïve. More than half the patients had advanced fibrosis or cirrhosis. There were no patients with hepatitis B coinfection and only a few patients with HIV coinfection, HCC, or history of liver transplant. The most commonly prescribed regimens were ledipasvir/sofosbuvir and paritaprevir/ritonavir/ombitasvir + dasabuvir. Most patients were initially approved for a 12-week duration of therapy. Only 1 ledipasvir/sofosbuvir patient and 5 glecaprevir/pibrentasvir patients were initially approved for an 8-week duration of therapy. Length of duration extension was variable, at provider discretion, and ranged from 4 to 12 weeks of additional therapy. Most patients achieved undetectable HCV RNA at week 6 in the traditional duration group and at week 8 in the extended duration group. HCV RNA became undetectable at or after week 8 of treatment in only 20.6% (63/305) of patients in the traditional duration group compared with 67.2% (39/58) in the extended duration group (Table 2).
Baseline Characteristics (n = 363).
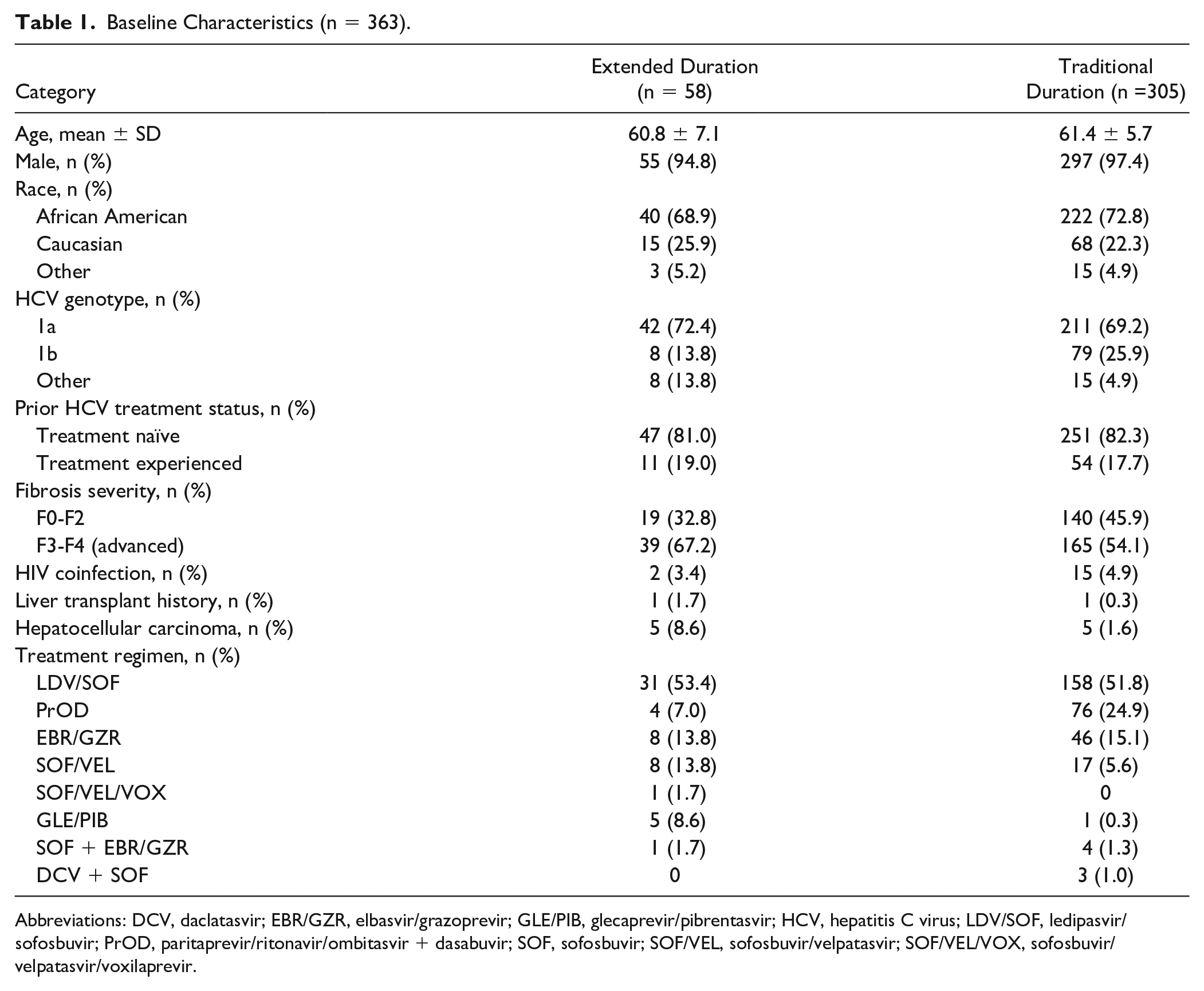
Abbreviations: DCV, daclatasvir; EBR/GZR, elbasvir/grazoprevir; GLE/PIB, glecaprevir/pibrentasvir; HCV, hepatitis C virus; LDV/SOF, ledipasvir/sofosbuvir; PrOD, paritaprevir/ritonavir/ombitasvir + dasabuvir; SOF, sofosbuvir; SOF/VEL, sofosbuvir/velpatasvir; SOF/VEL/VOX, sofosbuvir/velpatasvir/voxilaprevir.
SVR12 by Duration and Among Subgroups (n = 363).
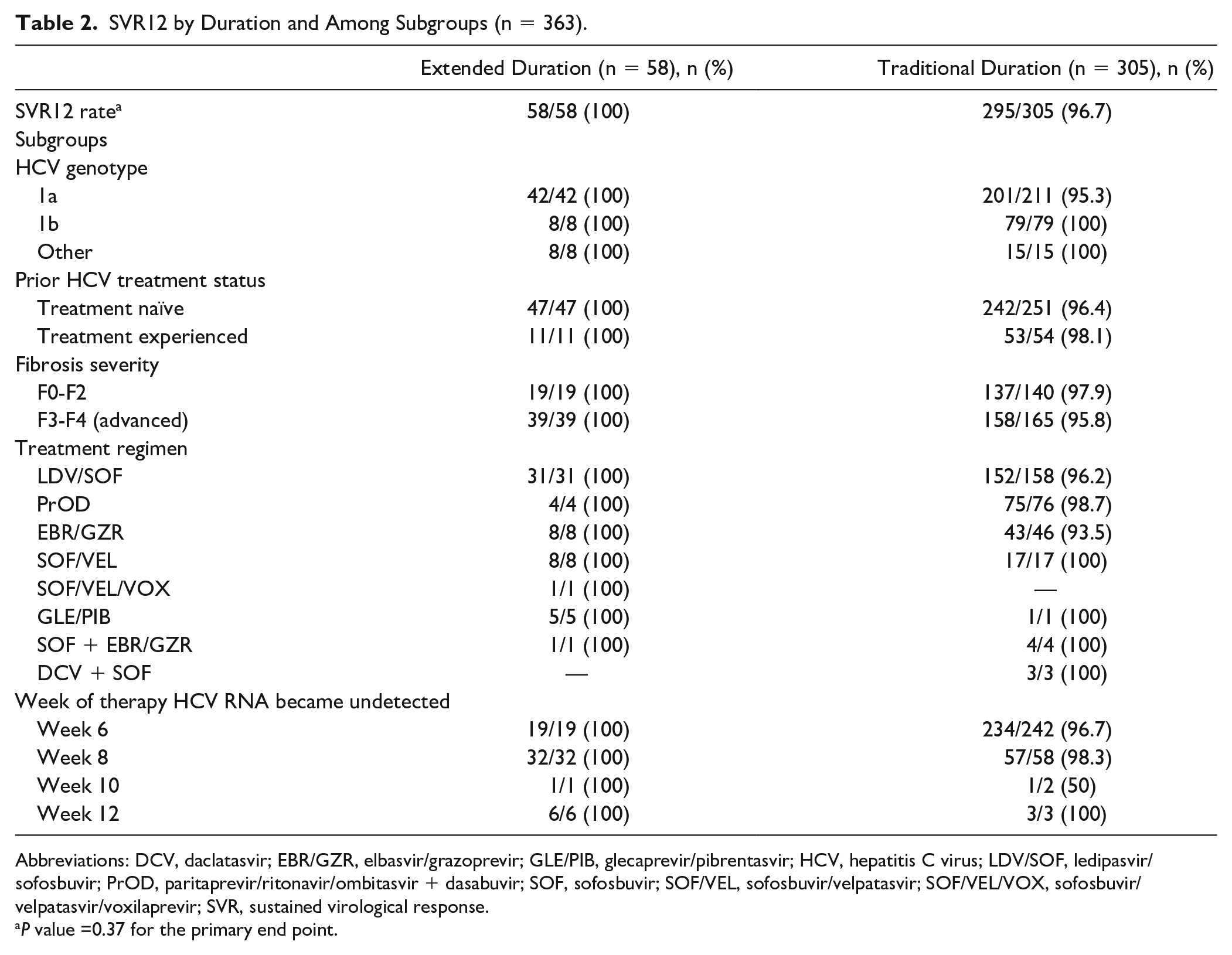
Abbreviations: DCV, daclatasvir; EBR/GZR, elbasvir/grazoprevir; GLE/PIB, glecaprevir/pibrentasvir; HCV, hepatitis C virus; LDV/SOF, ledipasvir/sofosbuvir; PrOD, paritaprevir/ritonavir/ombitasvir + dasabuvir; SOF, sofosbuvir; SOF/VEL, sofosbuvir/velpatasvir; SOF/VEL/VOX, sofosbuvir/velpatasvir/voxilaprevir; SVR, sustained virological response.
P value =0.37 for the primary end point.
Overall, rate of SVR12 was high at 97.2%. A total of 10 patients did not achieve SVR12, all of which occurred in the traditional duration group. There was no statistically significant difference in SVR12 between extended duration and traditional duration groups (100% vs 96.7%; P = 0.37). Descriptive statistics for rate of SVR12 among subgroups of HCV genotype, fibrosis severity, DAA regimen, or prior treatment experience may be found in Table 2. Among the 10 patients with treatment failure, 100% were genotype 1a, 70% had advanced fibrosis/cirrhosis, 60% were treated with ledipasvir/sofosbuvir, and 90% were treatment naïve. There were no factors independently associated with SVR12 in this population (Table 3).
Variables for Association With SVR12 in the Overall Population (n = 363).
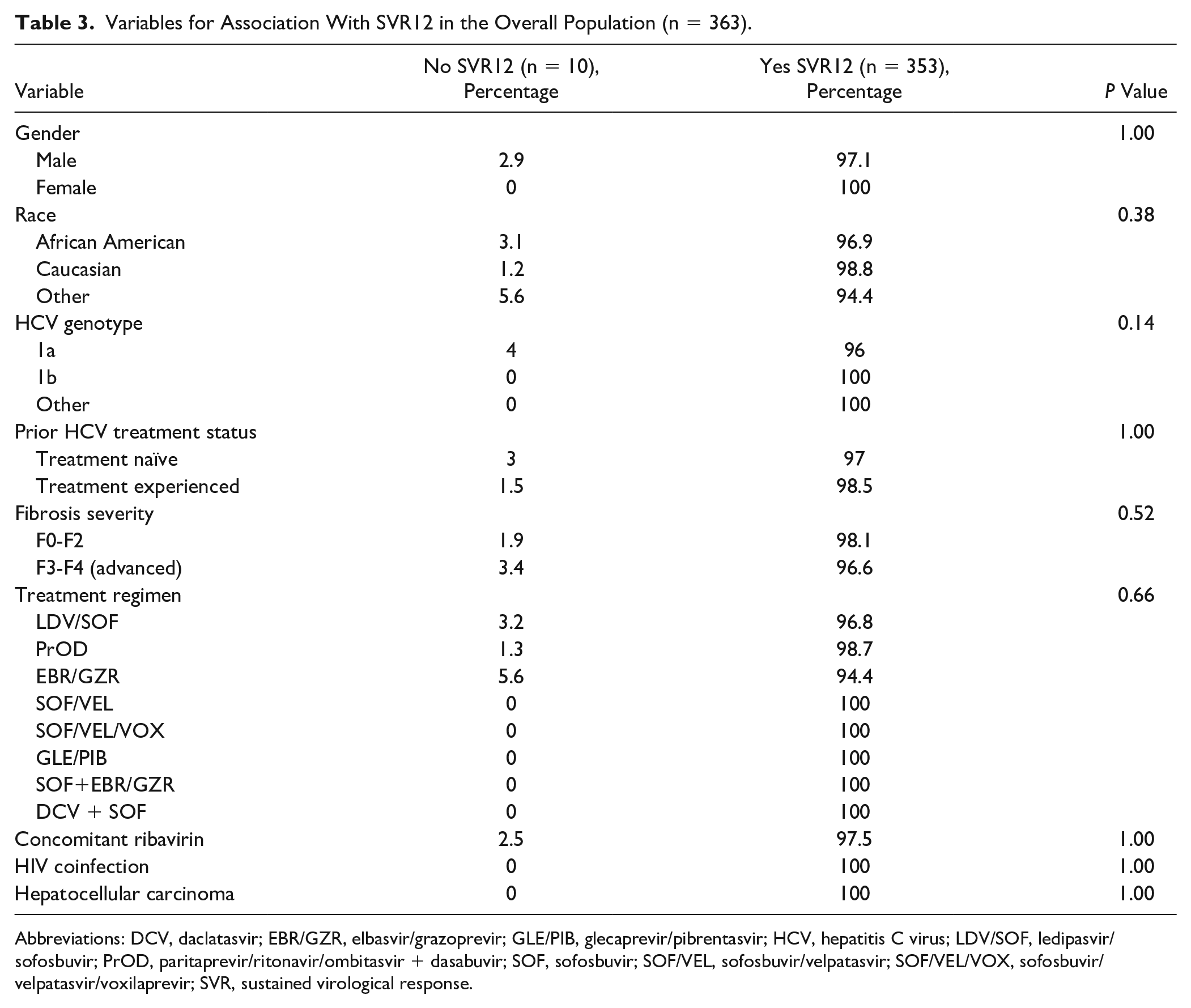
Abbreviations: DCV, daclatasvir; EBR/GZR, elbasvir/grazoprevir; GLE/PIB, glecaprevir/pibrentasvir; HCV, hepatitis C virus; LDV/SOF, ledipasvir/sofosbuvir; PrOD, paritaprevir/ritonavir/ombitasvir + dasabuvir; SOF, sofosbuvir; SOF/VEL, sofosbuvir/velpatasvir; SOF/VEL/VOX, sofosbuvir/velpatasvir/voxilaprevir; SVR, sustained virological response.
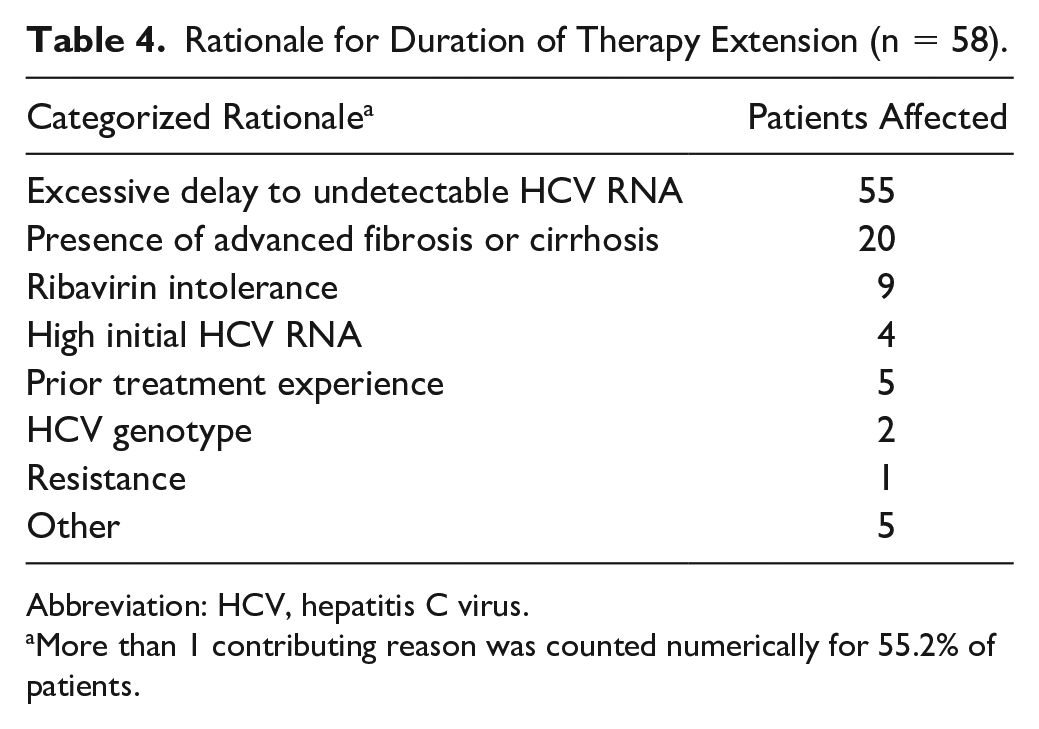
Among 58 patients with an extended therapy duration, there was more than one contributing reason for extension in 55.2% of patients (Table 4). The most common reason for extension of therapy duration was excessive delay to undetectable HCV RNA. The second most common reason was presence of advanced fibrosis or cirrhosis (34.5%). Other contributing reasons included ribavirin intolerance, treatment experience, high baseline HCV RNA, genotype, or resistance testing. Five patients had a rationale not fitting into previously mentioned categories, including concomitant proton-pump inhibitor use, incorrect medication administration, and therapy interruption.
Rationale for Duration of Therapy Extension (n = 58).
Abbreviation: HCV, hepatitis C virus.
More than 1 contributing reason was counted numerically for 55.2% of patients.
Conclusion and Relevance
Limited data regarding duration of treatment exists for patients treated with DAA regimens who have a detectable HCV RNA at week 4. Registration studies reported only 1% of patients with detectable HCV RNA at week 4.14-18 However, real-world studies suggest a higher incidence of slow response. The Project ECHO study indicated that 27.4% of patients had detectable HCV RNA at week 4 of treatment. Detectable week 4 HCV RNA was also found to be an independent predictor of failure to achieve SVR12 (OR = 2.9; P = 0.001). 20 However, the Project ECHO study only included early sofosbuvir-containing regimens, which are no longer recommended as first-line therapy by AASLD-IDSA guidance. Within the national VA registry, Johnson et al 24 found that at week 4 of treatment, 33.6% of patients had HCV RNA detectable below the LLOQ and 13.5% of patients had HCV RNA detectable above the LLOQ. The study by Johnson et al included ledipasvir/sofosbuvir in addition to early sofosbuvir-based regimens and paritaprevir/ritonavir/ombitasvi + dasabuvir with or without ribavirin. 24 The 34.7% slow response rate within our study is consistent with the previously published real-world data, further supporting the conjecture that the incidence of detectable HCV RNA at week 4 is higher than initially thought.
The publication by Johnson et al 24 is the only known study to date that has analyzed whether extending duration in patients with detectable HCV RNA at week 4 of treatment is associated with increased rates of SVR. Specifically, the study evaluated extending treatment duration to 12 weeks among patients who were eligible for 8 weeks of ledipasvir/sofosbuvir. No difference in outcomes was observed, but the study may not have been powered for that end point. 24 Our study included patients on any first-line DAA therapy for chronic HCV and mostly included those eligible for standard durations of therapy rather than only shortened duration. For example, only 1 patient on ledipasvir/sofosbuvir was approved initially for an 8-week duration.
The rates of SVR12 were 96% or higher regardless of therapy duration in this population of patients with slow virological response. Although there was no statistically significant difference in SVR12 between patients treated with extended duration versus traditional duration of therapy, it is promising that no failures occurred in the extended duration group, despite a numerically higher rate of advanced fibrosis or cirrhosis and longer prevalence of on-treatment viremia. This is encouraging, given the expectation for increased risk of treatment failure in patients with advanced fibrosis or cirrhosis.
There were no factors independently associated with achievement of SVR12 in this study. Afdhal et al 16 previously published 2 studies in a genotype 1 rapid virological responder population on ledipasvir/sofosbuvir ± ribavirin. The first study found that longer duration of therapy in treatment-experienced patients with cirrhosis led to increases in SVR (P = 0.007). Lack of cirrhosis was associated with a higher likelihood of achieving SVR (OR = 4.9; 95% CI = 1.386-18.378; P = 0.0124). 16 The second study included only treatment-naïve patients on ledipasvir/sofosbuvir ± ribavirin for 12 or 24 weeks. Compared with the first study, the presence of cirrhosis had no effect on rates of SVR. 18 In our study of a slow responder population, including both treatment-naive and treatment-experienced patients, advanced fibrosis or cirrhosis was not shown to be associated with achievement of SVR.
This study is limited because of the small sample size and is likely underpowered to find a statistically significant benefit of extending therapy duration. However, given the high rates of SVR, an extremely large number of patients would be required to demonstrate statistical significance. It is unlikely that a study of this nature would be feasible in a real-world setting. Additionally, the population was primarily African American patients and included few patients with genotype 2 to 6 infection or coinfection with HIV. This may limit the application of these findings to patients matching these characteristics. However, the SVR12 rates in this study are similar to data with ledipasvir/sofosbuvir, which had a primarily Caucasian population.16-18
Although no statistically significant benefit of therapy extension was seen between groups, all therapy failures occurred in the traditional duration group. A recommendation for extension of therapy cannot be made for patients with detectable HCV RNA at week 4 of treatment at this time based on this study. However, these data do provide further validation of previous data indicating that there are high rates of patients with detectable HCV RNA at week 4 of treatment in comparison to registration trials.
Because the slow responder population could be as large as 30% of treated patients, evidence to inform clinical decision-making becomes increasingly important. However, because of the high efficacy of the current DAA therapies even in the traditional duration group, this issue is relevant for a minority of patients. To address this, large studies would be required. The recent approval of safe and efficacious DAA salvage regimens have also changed the risk scenario related to treatment failure. Cost-effectiveness analyses may help guide decision making on whether investment in further studies are needed or if re-treatment of the few treatment failures is more cost-effective than extending therapies on all patients with slow viral kinetics, of whom only a minority would fail.
Footnotes
Authors’ Note
Background, methods, and objectives were presented at the American Society of Health-System Pharmacists Midyear Clinical Meeting in Anaheim, CA, in December 2018 (resident poster session).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Susanna Naggie, MD, MHS, has served as a speaker, a consultant, or advisory board member for BMS, BioMarin Pharmaceutical, IAS-USA, Vindico, Clinical Care Options, and Platform Q Health Inc.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Susanna Naggie has received research funding from Gilead Sciences, Abbvie, BMS, Tacere, and Janssen.