
Abstract
Background:
The 2019 community-acquired pneumonia guidelines recommend using recent respiratory cultures and locally validated epidemiology plus risk factor assessment to determine empirical coverage of methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa.
Objective:
To develop a methodology for evaluating local epidemiology and validating local risk factors for P aeruginosa and MRSA.
Methods:
This multicenter, retrospective cohort evaluated adult patients admitted for pneumonia. Risk factors for MRSA and P aeruginosa were evaluated using multivariable logistic regression and reported as adjusted odds ratios (aORs).
Results:
There were 10 723 cases evaluated. Lung abscess/empyema had the highest odds associated with MRSA (aOR = 4.24; P < 0.0001), followed by influenza (aOR = 2.34; P = 0.01), end-stage renal disease (ESRD; aOR = 2.09; P = 0.006), illicit substance use (aOR = 1.7; P = 0.007), and chronic obstructive pulmonary disease (COPD; aOR = 1.26; P = 0.04). For P aeruginosa, the highest odds were in bronchiectasis (aOR = 6.13; P < 0.0001), lung abscess/empyema (aOR = 3.36; P = 0.005), and COPD (aOR = 1.84; P < 0.0001). Isolated COPD without other risk factors did not pose an increased risk of either organism.
Conclusion and Relevance:
Influenza, ESRD, lung abscess/empyema, and illicit substance use were local risk factors for MRSA. Bronchiectasis and lung abscess/empyema were risk factors for Pseudomonas. COPD was associated with MRSA and Pseudomonas. However, isolated COPD had similar rates of MRSA and Pseudomonas pneumonia compared with the total population. This study established a feasible methodology for evaluating local risk factors.
Introduction
In October of 2019, the American Thoracic Society and Infectious Diseases Society of America updated the community acquired pneumonia (CAP) guidelines, replacing the previous version of these guidelines published in 2007.1,2 One of the more notable updates included the recommendation to abandon the health care–associated pneumonia (HCAP) categorization. 1 Released in 2005, the HCAP designation was created to identify patients who present from the community but were at a higher risk for multidrug-resistant (MDR) organisms, including Pseudomonas aeruginosa and methicillin-resistant Staphylococcus aureus (MRSA). 3
An unintended consequence of this distinction was the overuse and overprescribing of broad-spectrum and anti-MRSA antibiotics. Furthermore, a systematic review and meta-analysis demonstrated significant bias in the studies linking HCAP to MDR pathogens. Discriminatory ability of HCAP to predict resistant pathogens was low, and after adjusting for age and comorbidities, HCAP was not associated with increased mortality. 4 Grenier et al 5 evaluated the impact of guideline-directed therapy on mortality rates in CAP and HCAP. Whereas CAP demonstrated lower mortality rates when empirically treated in accordance with the guidelines, HCAP mortality rates were similar regardless of whether or not empirical treatment was concordant with the guidelines. 5 Rothberg et al 6 also evaluated the impact of guideline-directed therapy on patient outcomes in HCAP. After adjusting for demographics, comorbidities, and disease severity, broad-spectrum treatment, including an antipseudomonal agent and an anti-MRSA agent, were associated with an increase in mortality, length of stay, and cost. 6
Based on the concerns for overtreatment and the lack of evidence supporting broad-spectrum antibiotics, the newest CAP guidelines recommend abandoning the HCAP designation. The decision to initially add antipseudomonal or anti-MRSA therapy should be based on (1) previous isolation of either organism and (2) evaluating local epidemiology and validated risk factors to determine the need for coverage of MRSA and P aeruginosa. 1 Additionally, in November of 2019, shortly after the release of the CAP guidelines, the Centers for Disease Control and Prevention (CDC) released their updated version of the Core Elements of Hospital Antibiotic Stewardship Programs. This initiative highlights 3 disease states for hospital antibiotic stewardship programs to focus on, with CAP being one of them. The specific recommendation is to reduce or avoid empirical use of antipseudomonal β-lactams and MRSA agents unless clinically indicated. 7
The current CAP guidelines identify isolation of MRSA or P aeruginosa from a respiratory culture within the past year as an indication to initiate empirical coverage directed against the previous pathogen. For patients with severe pneumonia without prior respiratory isolation of MRSA or P aeruginosa, the recommendation is to add coverage based on recent hospitalization, exposure to parenteral antibiotics, and locally validated risk factors. The guidelines propose that clinicians obtain local prevalence data but acknowledge that many centers may not necessarily have access to this. Therefore, the purpose of this study is to develop a methodology to evaluate local epidemiology and to validate local risk factors for P aeruginosa and MRSA, as recommended by the newest CAP guidelines and the CDC.
Methods
After approval by the institutional review board at East Tennessee State University, this retrospective cohort evaluated all hospitalized patients admitted with a diagnosis of pneumonia present on admission (POA) across a 2-year period from January 1, 2017, through December 31, 2018. There were 8 hospitals included in the catchment area; all are located in Northeast Tennessee and Southwest Virginia, which service the Appalachian region. These hospitals range from the largest being a 445-bed regional-referral hospital and level-1 trauma center to the smallest being a critical access hospital. All hospitals included share the same electronic medical record; thus, the medical record number for each patient was the same, regardless of the hospital.
Patients
Patients were identified using International Statistical Classification of Diseases, Tenth Revision (ICD-10) coded billing data through QualityAdvisor (Premier Incorporated, Charlotte, NC). QualityAdvisor is a third-party clinical benchmarking product that captures resource utilization, ICD-10 coding, and patient-related outcomes. Patients with pneumonia were included if they had any of the following ICD-10 codes: J13 (pneumonia caused by Streptococcus pneumoniae), J14 (pneumonia caused by Hemophilus influenzae), J15 (pneumonia, not elsewhere classified), J18 (pneumonia, unspecified organism), J69.0 (pneumonitis caused by solids and liquids), A48.1 (Legionnaires disease). Note that J16 (pneumonia caused by other infectious organisms, not elsewhere classified) and J17 (pneumonia in diseases classified elsewhere) are additional pneumonia codes not utilized by our organization and were not included. Additionally, patients must have had one of these diagnoses POA to be included and to eliminate hospital-acquired pneumonia or ventilator-associated pneumonia. Patients were excluded for age less than 18 years, if they had had a previous respiratory culture positive for MRSA or P aeruginosa in the past year, or if they had been transferred from another facility. Additionally, only the first admission during the study period was evaluated for each patient. Baseline demographics included age, gender, and race. Age greater than 90 years was reported as 90 because of internal coding within QualityAdvisor. Length of stay, all-cause mortality prior to discharge, and all-cause 30-day readmission rates were also recorded. Risk factors were identified using the epidemiological conditions and/or risk factors related to specific pathogens in the 2007 CAP guidelines. 2 Epidemiological conditions were included in the analysis if they were recognized by the previous CAP guidelines to be associated with S aureus or P aeruginosa as a commonly encountered pathogen and are listed with corresponding ICD-10 codes in Table 1. Additional risk factors were evaluated at the discretion of the investigator.
Risk Factors Evaluated for the Development of Pseudomonas aeruginosa or Methicillin-Resistant Staphylococcus aureus Pneumonia.
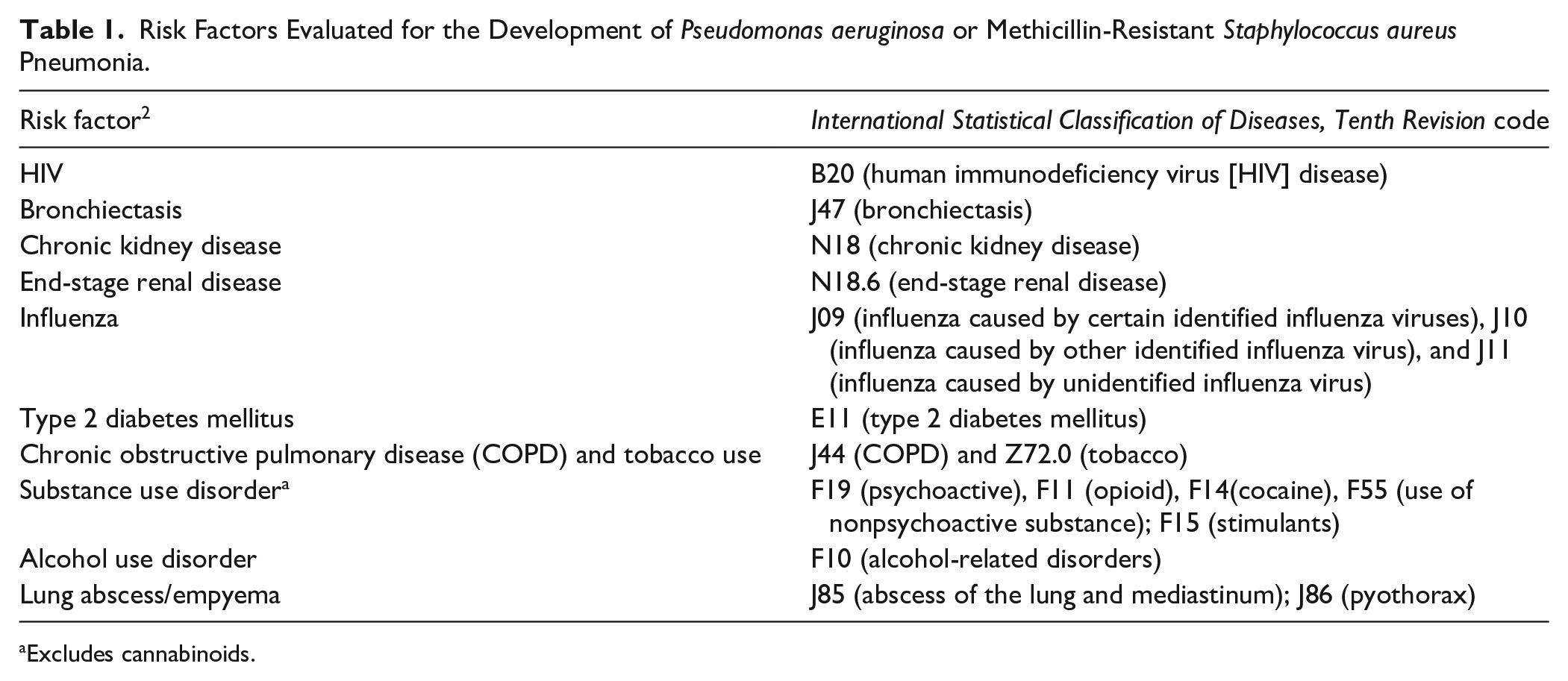
Excludes cannabinoids.
Analysis
Patients were also coded for MRSA pneumonia, identified using ICD-10 code of J15.212 and Pseudomonas pneumonia, identified with ICD-10 code of J15.1. Organism-specific ICD-10 codes were also matched to respiratory cultures provided by Theradoc (Premier Incorporated, Charlotte, NC). Risk factors were linked by medical record number and recorded in binary with “1” for present and “0” for absent. Diagnoses of MRSA pneumonia or Pseudomonas pneumonia were also recorded in binary fashion. A further analysis was performed within the chronic obstructive pulmonary disease (COPD) cohort because of its large sample size and potential impact on antimicrobial stewardship. Rates of MRSA and Pseudomonas in a cohort of patients with isolated COPD and no other risk factors were compared with the rates in the total population.
To assess the accuracy of coding, 50 patients with multiple comorbidities were randomly selected for profile review. End points for internal verification included overall percentage of data agreement (total data points in agreement divided by total possible data points), percentage of patients without a coding discrepancy, percentage of patients with more than 1 coding discrepancy, and percentage agreement for each risk factor.
Statistics
Continuous variables were reported using means and SDs. Categorical variables were reported as counts and frequencies. When needed, categorical variables were compared using χ2 test with Yate’s correction. Adjusted odds ratios (aORs) of MRSA pneumonia and Pseudomonas pneumonia were calculated for each risk factor. Separate analyses were performed for MRSA pneumonia and Pseudomonas pneumonia as the outcome variable and risk factors as the predictor variables using a multivariable logistic regression analysis. An additional analysis was performed to determine which risk factors were associated with increased odds of mortality. Results were provided using aORs and 95% CIs. P values <0.05 were considered statistically significant for the purposes of the study.
Results
Population
There were 121 278 evaluable records identifying 14 045 cases of pneumonia POA. After excluding 3322 cases, there were 10 723 cases included for analysis. Reasons for exclusion were the following: 338 were <18 years old; 1666 were transferred from another facility; 1314 had a previous admission; and 4 had previously positive respiratory cultures for MRSA or P aeruginosa. The population was almost exclusively white, with a slight predominance of female, and the majority were older than 65 years. The frequencies of MRSA pneumonia and Pseudomonas pneumonia were 3.32% (356/10 723) and 2.33% (250/10 723), respectively. Average length of stay was 5.5 days. Overall all-cause mortality and 30-day readmission rates were 8.46% (907/10 723) and 14.93% (1466/9816), respectively. The most commonly encountered comorbidities were COPD, diabetes mellitus type 2, and chronic kidney disease (CKD). Population characteristics are given in Table 2.
Patient Characteristics. a
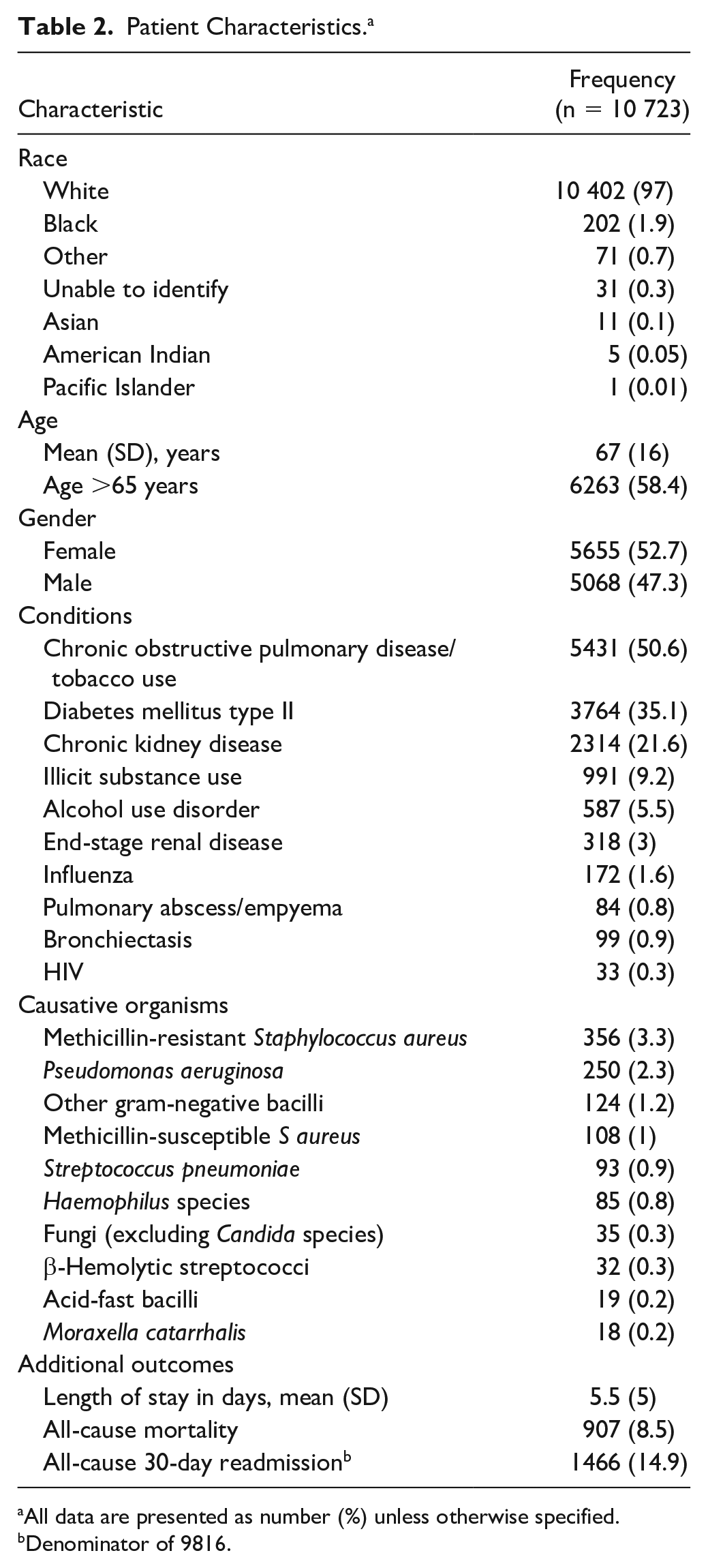
All data are presented as number (%) unless otherwise specified.
Denominator of 9816.
Pseudomonas and MRSA Risk Factors
Multivariable logistic regression analysis of risk factors for MRSA pneumonia are presented in Table 3. Lung abscess/empyema had the highest associated odds of developing MRSA (aOR = 4.24; 95% CI = 2.21-8.14; P < 0.0001), followed by influenza (aOR = 2.34; 95% CI = 1.18-4.67; P = 0.01), end-stage renal disease (ESRD; aOR = 2.09; 95% CI = 1.23-3.56; P = 0.006), illicit substance use (aOR = 1.7; 95% CI = 1.25-2.3; P = 0.0007), and COPD (aOR = 1.26; 95% CI = 1.01-1.55; P = 0.04). Multivariable logistic regression of risk factors for Pseudomonas pneumonia are presented in Table 4. The highest risk was seen in bronchiectasis (aOR = 6.14; 95% CI = 3.35-11.23; P < 0.0001), followed by lung abscess/empyema (aOR = 3.36; 95% CI = 1.43-7.87; P = 0.005), and COPD (aOR = 1.84; 95% CI = 1.41-2.39; P < 0.0001). There were no cases of P aeruginosa in patients with HIV. Therefore, this risk factor was omitted from analysis.
Logistic Regression Evaluation for Methicillin-Resistant Staphylococcus aureus in Community-Acquired Pneumonia.
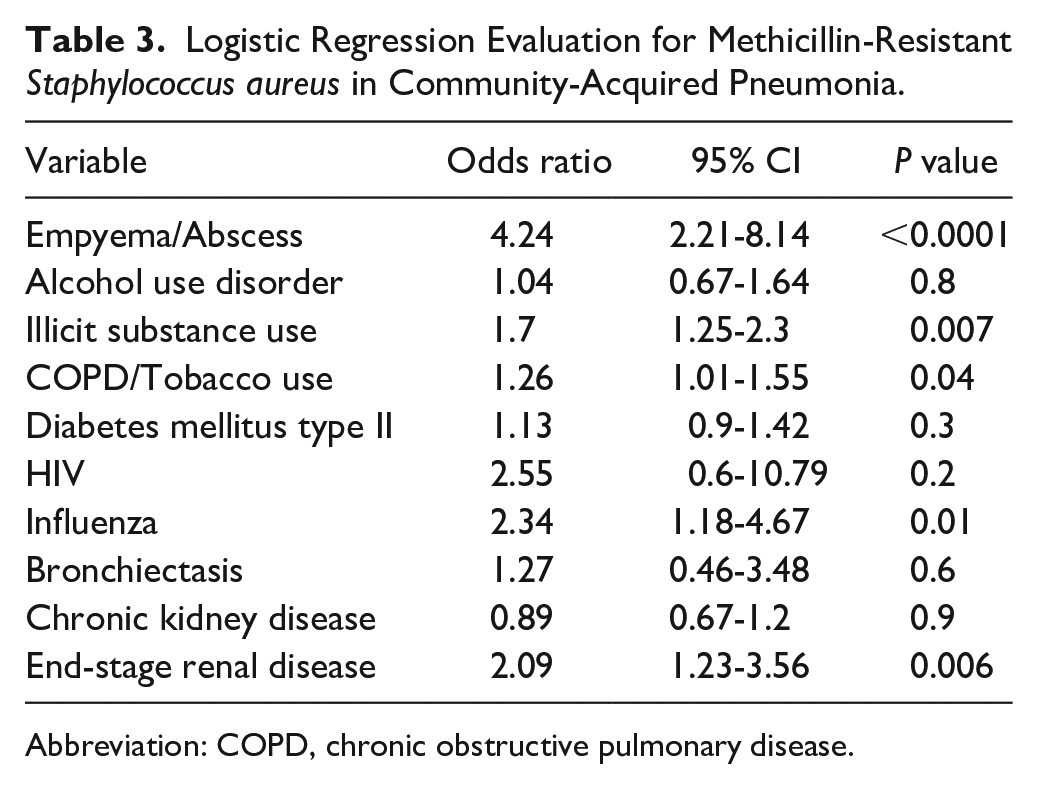
Abbreviation: COPD, chronic obstructive pulmonary disease.
Logistic Regression Evaluation for Pseudomonas aeruginosa in Community-Acquired Pneumonia.
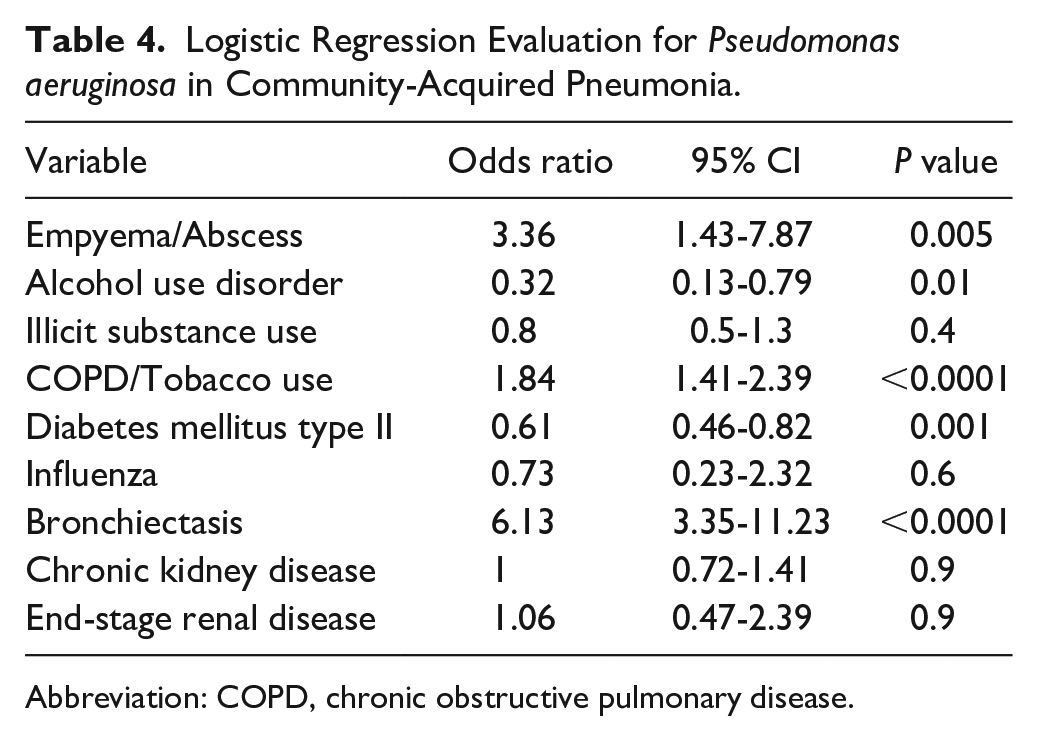
Abbreviation: COPD, chronic obstructive pulmonary disease.
Mortality Risk Factors
The average rate of mortality was 8.5% and highest in those with ESRD (13.5%), confirmed MRSA pneumonia (12%), alcohol use (11.8%), CKD (11.8%), lung abscess/empyema (9.5 %), diabetes mellitus type II (9.1%), and Pseudomonas pneumonia (8.7%). Mortality was lower than the average in patients with bronchiectasis (3%), illicit substance use (5.9%), HIV (6.1%), influenza (7%), and COPD (7.7%). aORs are listed in Table 5.
Logistic Regression Evaluation for Mortality in Community-Acquired Pneumonia.
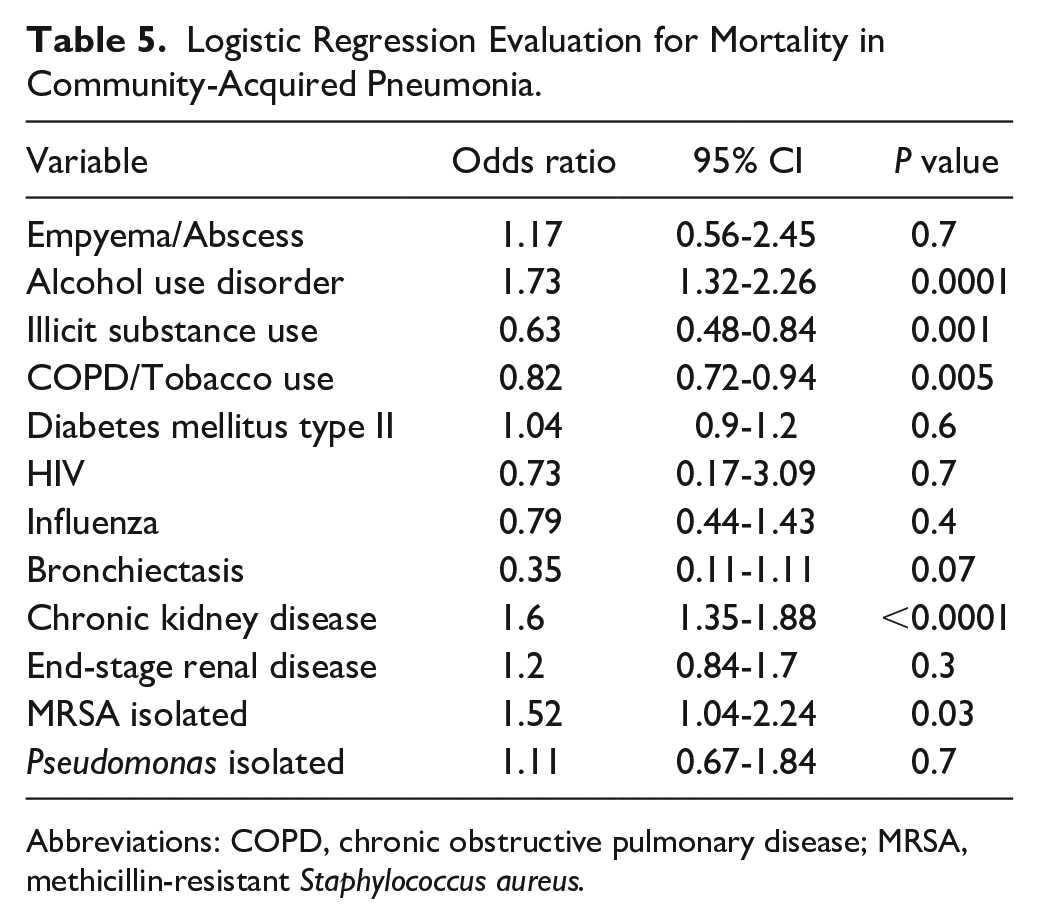
Abbreviations: COPD, chronic obstructive pulmonary disease; MRSA, methicillin-resistant Staphylococcus aureus.
COPD Cohort
Given that COPD was present in more than 50% of patients and was associated with an increased risk of both MRSA and Pseudomonas pneumonia, a separate evaluation was performed. When evaluating the risk of MRSA within the COPD cohort, 13.48% (732/5431) of patients had at least 1 additional risk factor for MRSA. Rates of MRSA pneumonia in patients with isolated COPD without any additional risk factors were similar to the overall rates of MRSA pneumonia in the total population (3.58% vs 3.32%, respectively; P = 0.6). When evaluating the risk of Pseudomonas within the COPD cohort, 1.64% (89/5431) of patients had at least 1 additional risk factor for Pseudomonas. Rates of Pseudomonas pneumonia in patients with isolated COPD without any additional risk factors were similar to the overall rates of Pseudomonas pneumonia in the total population (2.83% vs 2.33%, respectively; P = 0.07).
Internal Coding Assessment
A total of 12 data points from 50 patients were included for evaluation (10 risk factors and culture results for MRSA and P aeruginosa). There were 11 coding discrepancies and 589 agreements (98.2% agreement). There were 10 patients with at least 1 discrepancy and only 1 patient with 2 discrepancies, resulting in 80% of patients with complete agreement. The most common risk factors associated with coding discrepancies were alcohol use disorder (n = 4) and illicit substance use disorder (n = 3). Most of these were related to discrepancies between active use and history of use. Of the remaining discrepancies, 1 patient grew MRSA from a pleural effusion that was most likely lung abscess/empyema but not coded as such, another patient was coded with tobacco dependence but was not mentioned in the medical record, a third patient was coded with CKD that appeared to be acute kidney injury that recovered, and the last patient had steroid-induced hyperglycemia listed in the medical record but was coded as diabetes mellitus. Excluding the social history discrepancies, 92% of patients showed complete coding assessment agreement.
Discussion
This study demonstrated that pneumonia associated with lung abscess/empyema, influenza, illicit substance use, ESRD, and COPD were risk factors for MRSA and that lung abscess/empyema, bronchiectasis, and COPD were risk factors for P aeruginosa. Perhaps more important, this study also demonstrated that ICD-10 billing data could be used to evaluate local risk factors and epidemiology for the development of MRSA and P aeruginosa pneumonia. Moreover, this approach will allow other institutions to follow the newest CAP guideline recommendations by validating their local risk factors and then utilizing these to create order sets or treatment pathways tailored to their findings. Based on CDC guidance, reducing unnecessary coverage of MRSA and P aeruginosa has been identified as a top priority for hospital antibiotic stewardship programs. 7
The risk factors associated with MRSA and P aeruginosa pneumonia in this study are consistent with other reports. The 2007 CAP guidelines highlight lung abscess, influenza, bronchiectasis, injection drug use, and endobronchial obstruction as conditions associated with S aureus. 2 COPD and/or smoking, HIV infection (late), and bronchiectasis are highlighted as conditions for which P aeruginosa is commonly encountered. 2 There were 44 cases of HIV, 2 of which resulted in MRSA and no cases of Pseudomonas. Endobronchial obstruction did not have an ICD-10 code applicable to evaluate. Therefore, no conclusions can be drawn from these conditions.
ESRD had the highest incidence of mortality (13.5%) and was identified as a risk factor for MRSA in this study with an aOR of 1.94 (95% CI = 1.05-3.58). Visitation to a hemodialysis clinic was listed as a criterion used to identify patients at risk for MDR pathogens according to the proposed definition of HCAP. 3 Additionally, Wang and Wang 8 reported a frequency of 10.4% (5/48) of MRSA pneumonia in patients with ESRD. Whereas CKD represented 21.6% of the population, only 3% were ESRD. Given the high mortality and low incidence of ESRD, it is reasonable to include ESRD as a risk factor for MRSA.
Lung abscess/empyema had the next highest mortality rate (9.5%). Common pathogens include staphylococci, streptococci, gram-negative organisms, including Pseudomonas, anaerobes, and mycobacteria. 9 In this study, lung abscess/empyema was associated with the highest risk of MRSA and the second odds of P aeruginosa, with aORs of 5.33 (95% CI = 2.7-10.55) and 4.27 (95% CI = 1.81-10.05), respectively. In addition to coverage of MRSA and P aeruginosa, the most recent CAP guidelines highlight lung abscess or empyema as the only conditions warranting additional anaerobic coverage. 1 Based on these findings, piperacillin-tazobactam plus vancomycin (or linezolid) is a reasonable regimen for lung abscess/empyema. Alternative regimens without expanded anaerobic coverage would warrant the addition of clindamycin or metronidazole to the regimen.
COPD accounted for more than 50% of the study population, had a mortality of 7.7%, and was associated with increased odds of P aeruginosa (aOR = 1.84; 95% CI = 1.41-2.39) and MRSA (aOR = 1.26; 95% CI = 1.01-1.55). Historically, COPD has been recognized as a risk factor for P aeruginosa and MRSA.10-12 The 2007 CAP guidelines discuss the association between COPD and P aeruginosa in greater detail, highlighting that risk is associated with severe COPD, which is often accompanied by frequent antibiotic and steroid use. The updated 2019 CAP guidelines take a softer stance in patients with COPD, acknowledging that broader coverage is needed for multiple comorbidities (such as COPD). However, coverage of P aeruginosa in COPD is not specifically indicated. It would stand to reason that many of these patients would have previous admissions with prior respiratory cultures available to assist with guiding empirical treatment. Although COPD was associated with increased rates of both MRSA and Pseudomonas in this study, these rates were small, and statistical significance was found as a function of the large sample size, which does not imply clinical significance. Isolated COPD without other risk factors had rates of MRSA and Pseudomonas similar to that of the total cohort. The decision to empirically cover both organisms would result in an overwhelming number of patients for whom broad spectrum coverage is not warranted. The decision to cover either organism in COPD should not be based on the presence of COPD alone.
Pneumonia associated with influenza had a mortality of 7% (12/172) and was associated with increased odds of MRSA (aOR = 2.34; 95% CI = 1.18-4.67). Coinfection with MRSA and influenza is well established, and the increased frequency observed in this study supports previous findings.13-16 Mortality rates were slightly less than that in a previous report, of 10%. 15 When further evaluating the data, 2 of the 9 (22.2%) culture-positive patients died. This is also consistent with the previously reported rate of 30% following the 2009 H1N1 outbreak. 16 Given the high mortality rates in MRSA-positive patients, empirical coverage of MRSA in pneumonia associated with influenza is warranted.
Illicit substance use was associated with a mortality of 5.9% and an increased odds of MRSA (aOR = 1.67; 95% CI = 1.25-2.3). Because of coding limitations to identify injection drug use, illicit substance use for each class was used instead. Additionally, injection drug use carries significant social stigma, and patients are often reluctant to admit to use or routes of administration. 17 This makes it difficult to distinguish illicit drug use from injection drug use. Pneumonia associated with injection drug use often follows a pathophysiology different from that of the classic bronchopulmonary aspiration route. 18 Frequently, pneumonia results from septic emboli associated with right-sided endocarditis from repeated injections. 18 The link between injection drug use and invasive MRSA infections is well established. 19 It is reasonable to provide empirical coverage of MRSA in injection drug use (or illicit substance use). Although Pseudomonas is recognized as a potential pathogen in the endocarditis guidelines, rates were rare even in injection drug users.18,20 Of note, marijuana use was evaluated separately and not associated with either pathogen and was, therefore, omitted from further analysis.
Structural lung disease (including bronchiectasis and cystic fibrosis) is highlighted as a disease commonly associated with pneumonia. Whereas there were no patients with cystic fibrosis in this study, there were 99 cases of bronchiectasis. Bronchiectasis was associated with the highest odds of Pseudomonas (aOR = 6.14; 95% CI = 3.35-11.23) and a nonsignificant risk of MRSA (aOR = 1.27; 95% CI = 0.46-3.48). The incidence of Pseudomonas in bronchiectasis is widely known. Approximately 25% (range 9%-33%) of bronchiectasis patients are chronically colonized with P aeruginosa.21-23 Although not reaching statistical significance, there were 4 cases of MRSA in the cohort of 99 patients with bronchiectasis, raising an interesting question regarding whether a larger sample size would have led to similar findings. Metersky et al 24 evaluated 830 cases of non–cystic fibrosis patients with bronchiectasis from the Bronchiectasis Research Registry in the United States and reported that 94 cases (11.3%) grew S aureus, with approximately one-third being MRSA. Interestingly, S aureus was not associated with severe disease in this cohort. 24 Another study reported 17 cases of S aureus (6 being MRSA) in 233 cases of bronchiectasis, for rates of 7.3% (2.6% MRSA) in Spain. 25 Our reported rate of MRSA and Pseudomonas in bronchiectasis were 4% and 12.1%, respectively, and mortality was 3%. Given these findings, the question of whether either of these organisms represent a true pathogen or simply colonization remains unanswered. It is reasonable to direct prescribers to cover P aeruginosa but not MRSA until further research can provide insight into the high incidence, yet low mortality.
This study used coded billing data to identify risk factors and diagnoses. This comes with advantages and disadvantages. Advantages include a very large, multicenter sample size, speed of review, and lack of performing a manual chart review in which data could be missed. Limitations include relying on the quality of the documentation and coding to ensure that all diagnoses were captured. Because coding data can take several months to finalize, these types of studies will always be retrospective and missing the most recent months. The facilities included in this study used Cerner Soarian as the electronic medical record, which offers computer-assisted diagnostic coding to prescribers. Additionally, these facilities utilize clinical documentation specialists, which has been shown to improve coding ability. 26 In the sample audited records, agreement was seen in more than 98% of data points. The majority of discrepancies were related to inconsistencies in social history, which can be somewhat subjective. With large sample sizes, clinical judgment is imperative to distinguish clinical significance from statistical significance. There may be low frequency risks with high increases in incidences of MRSA or Pseudomonas that do not reach statistical significance but may be clinically meaningful. Alternatively, there could be high frequency risks with small increases in MRSA or Pseudomonas that reach statistical significance but are not clinically relevant. The latter was true for our institution with regard to COPD.
Another limitation was the lack of a means to control for exposure to parenteral antibiotics in the past 90 days. Only the first admission for pneumonia was included during the study period. However, receipt of antibiotics for indications not related to pneumonia might have been missed. Collinearity was not assessed, which is also a limitation. Risk factors in this study comprised comorbidities as well as presentation factors, such as influenza or lung abscess/empyema. Presentation factors may not always be known at the point of antibiotic selection. QualityAdvisor was used in this study, a service that may not be readily available to many hospital systems. However, most electronic health record systems are capable of generating billing data reports. Replication of the methodology with other electronic health record systems or data mining programs is needed for external validation.
The population in this study was mostly white and included a high frequency of COPD or tobacco use. We had a very small number of patients with HIV and cannot draw conclusions regarding this population. Ultimately, it is up to each individual site to evaluate the local risk factors and hospital epidemiology to create individualized treatment plans.
Conclusion and Relevance
ICD-10 coded data provided via QualityAdvisor is a feasible method for evaluating local risk factors for MRSA and Pseudomonas pneumonia. Influenza, ESRD, lung abscess/empyema, illicit substance use, and bronchiectasis were local risk factors for MRSA in this study. Bronchiectasis and lung abscess/empyema were local risk factors for Pseudomonas pneumonia. COPD was a risk factor for both MRSA and Pseudomonas; however, this risk was small, and consequences of drug overexposure outweigh the risk associated with missed coverage. This study established a feasible methodology for evaluating local risk factors that should be completed by each hospital or catchment area.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.