
Abstract
Objective:
To review the efficacy and safety of the high-dose inactivated influenza vaccine quadrivalent (HD-IIV4) in the prevention of influenza in older adults.
Data Sources:
A literature search was performed using PubMed and Google Scholar with the search terms high-dose, influenza vaccine, and quadrivalent. Other resources included the Centers for Disease Control and Prevention (CDC), the prescribing information, and the manufacturer’s website.
Study Selection and Data Extraction:
All relevant English-language articles of studies assessing the efficacy and safety of HD-IIV4 were included.
Data Synthesis:
HD-IIV4 is licensed by the Food and Drug Administration for the prevention of influenza in adults aged 65 years and older. The safety and immunogenicity of HD-IIV4 was demonstrated in a phase 3 trial, and the efficacy of the trivalent formulation (HD-IIV3) was demonstrated in a phase 3b-4 trial. HD-IIV4 carries a warning regarding the occurrence of Guillain-Barré syndrome. Adverse reactions, including injection-site pain and myalgia, were reported more frequently with HD-IIV4 than with HD-IIV3.
Relevance to Patient Care and Clinical Practice:
Although the CDC recommends any age-appropriate influenza vaccine for adults aged 65 years and older, HD-IIV4 was associated with improved immunogenicity against the added B strain and HD-IIV3 provided better protection against influenza than the standard-dose vaccine. Other influenza vaccines have weaker evidence of efficacy in older adults. Therefore, HDIIV4 should be recommended as the vaccine of choice in adults aged 65 years and older.
Conclusion:
HD-IIV4 has proven immunogenic, safe, and effective in preventing influenza in older adults and should be recommended as the vaccine of choice in this patient population.
Introduction
Influenza is associated with significant morbidity and mortality worldwide. Each year since 2010, an estimated 9 to 45 million influenza illnesses occur in the United States that result in 140 000 to 810 000 hospitalizations and 12 000 to 61 000 deaths. 1 Although influenza seasons vary in severity from year to year, adults aged 65 years and older usually carry the highest burden of severe disease. 2 In recent years, it is estimated that 50% to 70% of influenza-related hospitalizations and 70% to 85% of influenza-related deaths have occurred in older adults. 2 Influenza vaccination is the primary method to prevent influenza and its complications. 3 Each year, the Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices provides recommendations for influenza prevention and control. Influenza vaccination is recommended for all people aged 6 months and older without any contraindications. 3 Vaccination is especially important in people at high risk of complications, such as adults aged 50 years and older, American Indians/Alaska Natives, residents of long-term care facilities, persons with a body mass index (BMI) of 40 kg/m2 and greater, those with altered immune competence, and those with the following comorbid conditions: chronic pulmonary diseases, including asthma and chronic obstructive pulmonary disease; cardiovascular diseases excluding hypertension; and renal, hepatic, neurological, hematological, or metabolic disorders, including diabetes mellitus. 3 Table 1 lists the recommended influenza vaccines for adults aged 65 years and older during the 2019-2020 influenza season. 3 Despite these recommendations, vaccination rates remain below the Healthy People 2020 target of 90% for noninstitutionalized adults aged 65 years and older and for adults residing in long-term care facilities. 4 In the past 10 years, vaccine effectiveness in the general population has ranged from a low of 19% in the 2014-2015 influenza season to a high of 60% in the 2010-2011 influenza season. 5 Vaccine effectiveness is generally lower in adults aged 50 years and older than in those aged 18 to 49 years old because older adults have a reduced ability to mount appropriate cellular and humoral immune responses to vaccines.5,6 This is because of a gradual weakening of the immune system and a progressive decline of adaptive and innate immune responses with aging, a phenomenon known as immunosenescence. 7 Efforts to identify more effective vaccines than the standard-dose inactivated influenza vaccines (IIVs; trivalent [IIV3] or quadrivalent [IIV4]) in older adults have led to the development of the high-dose inactivated influenza vaccine trivalent (HD-IIV3), the adjuvanted influenza vaccine trivalent (aIIV3), and the recombinant influenza vaccine quadrivalent (RIV4).6-10 In 2019, a high-dose inactivated influenza vaccine quadrivalent (HD-IIV4; Fluzone High-Dose Quadrivalent, Sanofi Pasteur) was licensed by the Food and Drug Administration (FDA) to prevent influenza in persons aged 65 years and older. 11 This article reviews the immunogenicity, efficacy, and safety of HD-IIV4 in older adults.
Recommended Influenza Vaccines for Adults Aged ≥65 years in the 2019-2020 Influenza Season. 3
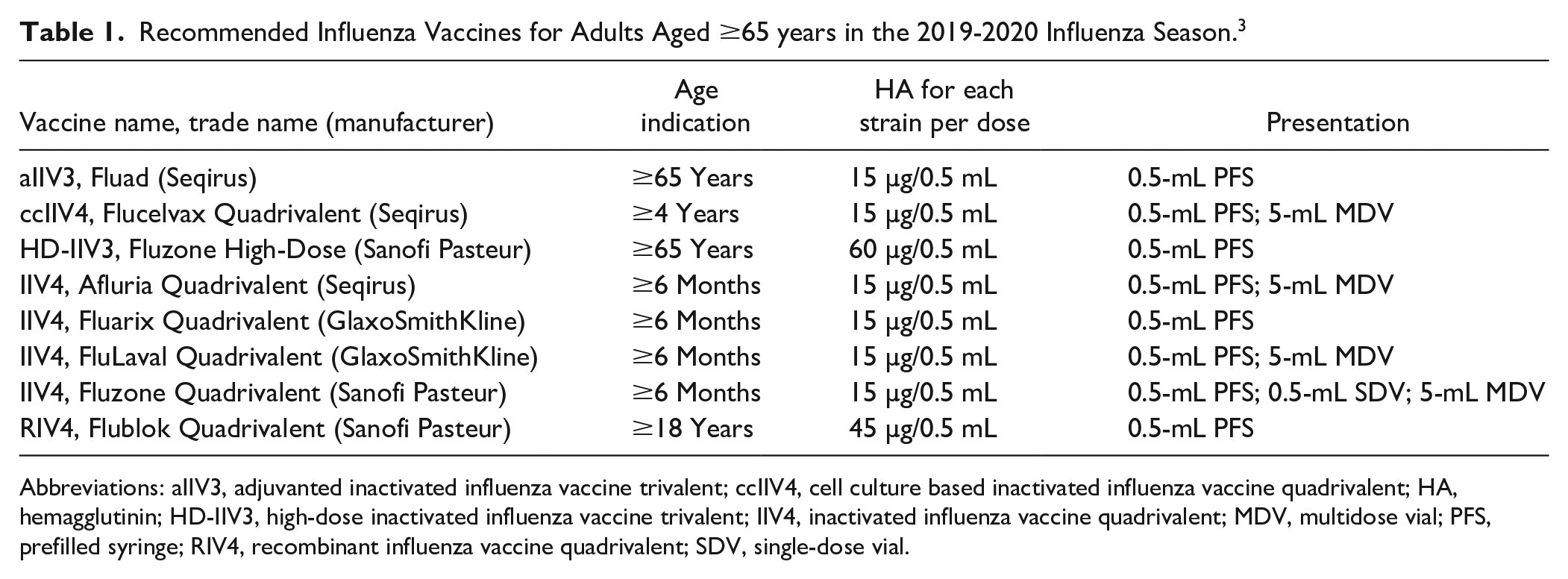
Abbreviations: aIIV3, adjuvanted inactivated influenza vaccine trivalent; ccIIV4, cell culture based inactivated influenza vaccine quadrivalent; HA, hemagglutinin; HD-IIV3, high-dose inactivated influenza vaccine trivalent; IIV4, inactivated influenza vaccine quadrivalent; MDV, multidose vial; PFS, prefilled syringe; RIV4, recombinant influenza vaccine quadrivalent; SDV, single-dose vial.
Data Sources
A literature search was conducted using PubMed (2010 to April 2020) and Google Scholar (2010 to April 2020) with the search terms high-dose, influenza vaccine, and quadrivalent. Other sources included the CDC, the prescribing information, and the manufacturer’s website. References were reviewed for additional data sources. All relevant English-language articles of studies assessing the efficacy and safety of HD-IIV4 were included.
Pharmacology
Influenza is a single-stranded RNA virus that belongs to the family of Orthomyxoviridae. 12 Types A and B are responsible for epidemic human disease, whereas type C is rarely reported to cause human disease and type D does not cause human disease. 12 Influenza A viruses are further categorized into subtypes based on surface antigens hemagglutinin (HA) and neuraminidase (NA), whereas influenza B viruses do not exhibit the same type of antigenic and genetic variation in the HA and NA and are not further categorized into subtypes.12,13 Influenza A(H1N1), influenza A(H3N2), influenza B-Victoria lineage, and influenza B-Yamagata lineage have been in global circulation for decades. 13 All commercially available US influenza vaccines are either trivalent, containing influenza A(H1N1), A(H3N2), and B-Victoria lineage, or quadrivalent, containing an additional influenza B-Yamagata lineage. 3 Antigenic variants are determined annually based on predictions of the viruses likely to circulate. 3
Each dose of HD-IIV4 contains a total of 240 µg HA (60 µg per strain) corresponding to the 4 influenza strains recommended by the FDA’s Vaccines and Related Biological Products Advisory Committee and standardized according to the US Public Health Service requirements.11,14 Recommendations for the 2019-2020 influenza season were A/Brisbane/02/2018 (H1N1)pdm09–like virus, A/Kansas/14/2017 (H3N2)–like virus, B/Colorado/06/2017–like virus (Victoria lineage), and B/Phuket/3073/2013–like virus (Yamagata lineage). 3 The immune response to IIV is best characterized by a humoral response that can be measured by increases in serum HA inhibition (HAI) antibodies that peak 2 to 4 weeks after vaccination but fall quickly to reach near baseline levels before the next influenza season. 13 Cellular response involving CD4+ T-cells and CD8+ T-cells is also noted after vaccination. 13 Many studies have shown that increasing the dose of HA in influenza vaccines can increase serum antibody responses.15,16 In a placebo-controlled trial among healthy persons aged 65 years and older, increasing the dose of HA resulted in increasingly higher levels of serum HAI antibody titers. 15 Mean serum antibody titers 1 month after vaccination increased 2- to 3-fold with a 9-fold increase in dose; the frequencies of 4-fold or greater rises in titer likewise increased. 15 In an active-controlled trial among persons aged 65 years and older, HD-IIV3 resulted in a statistically significant increase in mean HAI antibody titers and seroconversion rates at day 28 after vaccination for all strains compared with IIV3. 16 Seroconversion is usually defined as either an increase in HAI titer from <1:10 to ≥1:40 after vaccination or a 4-fold increase in HAI titer after vaccination from a prevaccination titer ≥1:10. 16
Clinical Trials
Table 2 summarizes the results of immunogenicity trials of HD-IIV4 and the efficacy trial of HD-IIV3.8,17,18 There are no published efficacy trials using HD-IIV4, but data can be extrapolated from HD-IIV3 because both vaccines are manufactured using the same process. 11
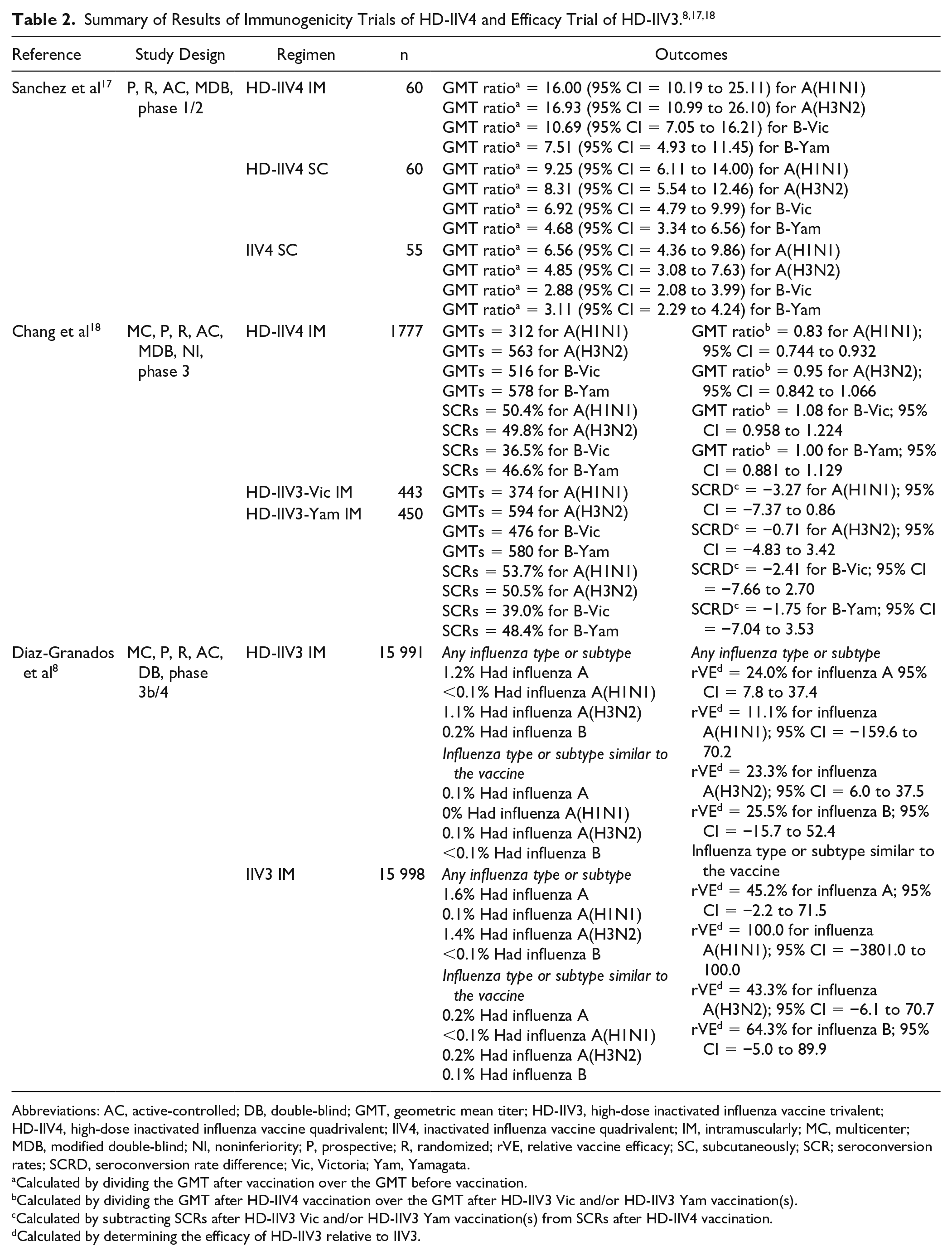
Abbreviations: AC, active-controlled; DB, double-blind; GMT, geometric mean titer; HD-IIV3, high-dose inactivated influenza vaccine trivalent; HD-IIV4, high-dose inactivated influenza vaccine quadrivalent; IIV4, inactivated influenza vaccine quadrivalent; IM, intramuscularly; MC, multicenter; MDB, modified double-blind; NI, noninferiority; P, prospective; R, randomized; rVE, relative vaccine efficacy; SC, subcutaneously; SCR; seroconversion rates; SCRD, seroconversion rate difference; Vic, Victoria; Yam, Yamagata.
Calculated by dividing the GMT after vaccination over the GMT before vaccination.
Calculated by dividing the GMT after HD-IIV4 vaccination over the GMT after HD-IIV3 Vic and/or HD-IIV3 Yam vaccination(s).
Calculated by subtracting SCRs after HD-IIV3 Vic and/or HD-IIV3 Yam vaccination(s) from SCRs after HD-IIV4 vaccination.
Calculated by determining the efficacy of HD-IIV3 relative to IIV3.
Immunogenicity Trials
A 2-center trial was conducted in healthy, community-dwelling adults aged 65 years and older in Japan. The exclusion criterion was altered immunocompetence. 17 A small number of participants (cohort 1) were randomized to receive either a single intramuscular (IM) injection of HD-IIV4 or a subcutaneous (SC) injection of HD-IIV4. After review of the adverse events occurring within 7 days after vaccination, more participants were recruited (cohort 2). Participants were randomized to receive either a single IM injection of HD-IIV4, a SC injection of HD-IIV4, or a SC injection of IIV4. The primary immunogenicity end points were HAI geometric mean titers (GMTs) and seroconversion rates at day 28 in the per-protocol analysis. This analysis was conducted in cohort 2 participants who received the trial vaccine, had a postvaccination blood sample HAI result, and did not have a major protocol deviation. All participants were vaccinated as randomized and completed the study according to protocol, although 1 participant who received IIV4 was excluded from the immunogenicity analysis set because of taking a prohibited medication. In the HD-IIV4 IM arm, the mean age of participants was 70.2 years, 15.0% were ≥75 years old, 53.3% were male, 100.0% were Asian, the mean BMI was 23.43 kg/m2, and 16.7% had received an influenza vaccine in the previous season. In the HD-IIV4 SC arm, the mean age of participants was 70.6 years, 16.7% were ≥75 years old, 55.5% were male, 100% were Asian, the mean BMI was 24.09 kg/m2, and 31.7% had received an influenza vaccine in the previous season. In the IIV4 SC arm, the mean age of participants was 69.9 years, 16.4% were ≥75 years old, 54.5% were male, 100% were Asian, the mean BMI was 23.51 kg/m2, and 30.9% had received an influenza vaccine in the previous season. Postvaccination/prevaccination GMT ratios in the HD-IIV4 IM arm were numerically higher than those in the HD-IIV4 SC arm, and ratios in the HD-IIV4 SC arm were numerically higher than those in the IIV4 SC arm. Seroconversion rates were provided only in a figure format; rates in the HD-IIV4 IM arm were numerically higher than those in the HD-IIV4 SC arm, and rates in the HD-IIV4 SC arm were numerically higher than those in the IIV4 SC arm. This trial showed that HD-IIV4 is highly immunogenic in healthy adults aged 65 years and older in Japan. Immune responses were higher with HD-IIV4 than IIV4, and the IM route was associated with higher immune response than the SC route. Limitations include the exclusion of frail and institutionalized older adults, the small percentage of participants who received an influenza vaccine in the previous season, the lack of statistical comparisons given the small sample size, and the fact that protection against influenza was not directly measured.
Another trial was conducted in healthy, community-dwelling adults aged 65 years and older in the United States. 18 Exclusion criteria were altered immunocompetence and history of Guillain-Barré syndrome. Participants were randomized to receive either a single IM injection of HD-IIV4, the licensed HD-IIV3 containing B-Victoria referred to as HD-IIV3-Victoria, or an HD-IIV3 containing the alternate Yamagata-lineage B strain referred to as HD-IIV-3-Yamagata. The primary immunogenicity end points were HAI GMTs and seroconversion rates at day 28 in the per protocol analysis. This analysis was conducted in participants who received the trial vaccine, had a postvaccination blood sample HAI result, and did not have a major protocol deviation. The predefined noninferiority criterion for the GMT ratio was that the lower limit of the 95% CI of the GMT ratio (HD-IIV4/HD-IIV3) should be greater than 0.667. The predefined noninferiority criterion for seroconversion rates was that the lower limit of the 2-sided 95% CI of the difference in rates (HD-IIV4 − HD-IIV3) should be greater than −10%. Of the 2670 enrolled participants, 2654 (99.4%) completed the active study period, and 2533 (94.9%) completed the active study period according to the protocol and were included in the per protocol analysis. In the HD-IIV4 arm, the mean age of participants was 72.9 years, 35.4% were ≥75 years old, 41.8% were male, 91.2% were white, 21.1% had a normal BMI, 47.0% had ongoing chronic medical conditions, 75.7% were taking concomitant medications, and 75.4% had received an influenza vaccine in the previous season. In the HD-IIV3-Victoria arm, the mean age of participants was 72.8 years, 33.3% were ≥75 years old, 40.7% were male, 89.8% were white, 21.5% had a normal BMI, 50.8% had ongoing chronic medical conditions, 74.9% were taking concomitant medications, and 69.5% had received an influenza vaccine in the previous season. In the HD-IIV3-Yamagata arm, the mean age of participants was 73.2 years, 38.1% were ≥75 years old, 44.4% were male, 89.5% were white, 19.1% had a normal BMI, 41.1% had ongoing chronic medical conditions, 74.0% were taking concomitant medications, and 74.0% had received an influenza vaccine in the previous season. All GMT ratios and seroconversion rate differences met the criteria for noninferiority. This trial demonstrated that, despite the higher dose of antigen, adding a second influenza B strain to HD-IIV3 did not compromise the immunogenicity induced by the other 3 strains or limit the immune response to the added B-lineage strain in adults aged 65 years and older in the United States. Limitations include the exclusion of frail and institutionalized older adults and the fact that protection against influenza was not directly measured.
Efficacy Trial
A trial was conducted in adults aged 65 years and older in the United States and Canada. 8 Exclusion criteria were moderate or severe acute illness and history of Guillain-Barré syndrome. Participants were randomized to receive either an IM injection of HD-IIV3 or IIV3 for 2 influenza seasons. Participants enrolled in the first year were able to reenroll and were rerandomized in the second year. The primary end point was the occurrence, at least 14 days after vaccination, of laboratory-confirmed influenza, defined as positive culture or polymerase chain reaction caused by any influenza viral types or subtypes, in association with a protocol-defined influenza-like illness, defined as the occurrence of at least 1 of the following respiratory symptoms, that is, sore throat, cough, sputum production, wheezing, or difficulty breathing, in conjunction with at least 1 of the following systemic signs or symptoms: temperature >99.0 °F, chills, tiredness, headaches, or myalgia. Participants were monitored for the occurrence of a respiratory illness, starting 2 weeks after vaccination for approximately 7 months. The primary end point was assessed in both the intention-to-treat and per protocol analyses. The predefined superiority criterion was that the lower limit of the 95% CI for relative vaccine efficacy (rVE) should be greater than 9.1%. A key secondary end point was the occurrence of culture-confirmed influenza caused by viral types or subtypes antigenically similar to those contained in the respective annual vaccine formulations in association with a modified CDC-defined influenza-like illness, defined as the occurrence of a temperature >99.0 °F with cough or sore throat. Of the participants who underwent randomization, 31 983 (>99.9%) received the study vaccine and were included in the intention-to-treat analysis, and 31 803 (99.4%) did not have major protocol violation and were included in the per protocol analysis. In the HD-IIV3 arm, the mean age of participants was 73.3 years, 42.9% were male, 94.4% were white, 67.2% had at least 1 chronic medical condition, 33.7% had at least 2 chronic medical conditions, and 73.5% had received an influenza vaccine in the previous season. In the IIV3 arm, the mean age of participants was 73.3 years, 44.0% were male, 94.8% were white, 67.2% had at least 1 chronic medical condition, 33.8% had at least 2 chronic medical conditions, and 73.6% had received an influenza vaccine in the previous season. A total of 228 participants (1.4%) had laboratory-confirmed influenza caused by any viral type or subtype in the HD-IIV3 arm, and 301 participants (1.9%) had the same in the IIV3 arm resulting in an rVE of 24.2% (95% CI = 9.7-36.5), which met the superiority criterion. This indicates that about one quarter of all breakthrough influenza cases could be prevented if HD-IIV3 were used instead of IIV3. A total of 22 participants (0.1%) had culture-confirmed influenza caused by virus type or subtype similar to the vaccine component in the HD-IIV3 arm, and 45 participants (0.3%) had the same in the IIV3 arm, resulting in an rVE of 51.1% (95% CI = 16.8-72.0). This indicates that about half of all breakthrough influenza cases caused by strains similar to the vaccine component could be prevented if HD-IIV3 were used instead of IIV3. This trial demonstrated that HD-IIV3 provided better protection than IIV3 against laboratory-confirmed influenza illness caused by any viral type or subtype in adults aged 65 years and older in the United States and Canada. Limitations include the small number of confirmed influenza cases and the very small number of confirmed influenza cases caused by strains similar to the vaccine, which may result in insufficient precision in determining vaccine efficacy.
Effectiveness Studies
There are no published studies on the relative vaccine effectiveness (rVE) of HD-IIV4 compared with other vaccines in adults aged 65 years and older in real-life, but data can be extrapolated from HD-IIV3.19-23 In an analysis of data collected from 6.1 million Medicare beneficiaries over 2 influenza seasons, HD-IIV3 was shown to be more effective than IIVs in preventing postinfluenza deaths (rVE = 24.0%; 95% CI = 0.6-42). 19 In an analysis of data collected from a cohort of 73 773 veterans over 1 influenza season, HD-IIV3 was shown to be more effective than IIVs in preventing influenza- or pneumonia-associated hospitalization (rVE = 25%; 95% CI = 2-43) and all-cause outpatient visits (rVE = 5%; 95% CI = 2-8). 20 In an analysis of data collected from a cohort of 47 424 patients in the Portland metropolitan area over 1 influenza season, HD-IIV3 was shown to be more effective than IIVs in preventing influenza-related hospitalization (rVE = 30.7%; 95% CI = 8-48). 21 In an analysis of data collected from 1.7 million veterans over 5 influenza seasons, HD-IIV3 was shown to be more effective than IIVs in preventing influenza- or pneumonia-associated hospitalizations (rVE = 14%; 95% CI = 6-22), cardiorespiratory hospitalizations (rVE = 18%; 95% CI = 15-21), and all-cause hospitalization (rVE = 10%; 95% CI = 8-12). 22 Finally, in an analysis of data collected from 2.1 million members of a managed care company over 2 influenza seasons, HD-IIV3 was shown to be more effective than aIIV3 in preventing respiratory-related hospitalizations (rVE = 12%; 95% CI = 3.3-20). 23
Safety and Tolerability
According to the manufacturer, HD-IIV4 is contraindicated in persons with severe allergic reaction to egg protein because the vaccine is prepared from influenza viruses propagated in embryonated chicken eggs. 11 However, the CDC recommends that persons with a history of allergy to eggs may receive any recommended influenza vaccine appropriate for their age and health status, and those with severe reactions such as angioedema or respiratory distress should be vaccinated under the supervision of a health care professional who is able to recognize and manage severe allergic reactions. 3 Like all influenza vaccines, HD-IIV4 carries precautions regarding use in patients with moderate or severe acute illness with or without a fever and in those with a history of Guillain-Barré syndrome occurring within 6 weeks following any previous influenza vaccine.3,11 In the latter case, the decision to vaccinate should be based on careful consideration of the potential benefits and risks. 3 Like all inactivated influenza vaccines, HD-IIV4 cannot cause influenza but may result in a lower immune response when administered to patients with altered immunocompetence.3,11 HD-IIV4 is not licensed to be used in persons younger than 65 years old, and safety and effectiveness have not been established in pregnancy, lactation, and pediatrics. 11
Table 3 lists the most frequently solicited adverse reactions in participants receiving HD-IIV4 in the phase 1/2 trial conducted in Japan and the phase 3 trial conducted in the United States.17,18 In both trials, the most frequently solicited injection-site reactions occurring within 3 days of vaccination were pain, erythema, swelling, and induration, whereas the most frequently solicited systemic reactions were myalgia, headache, malaise, and shivering.17,18
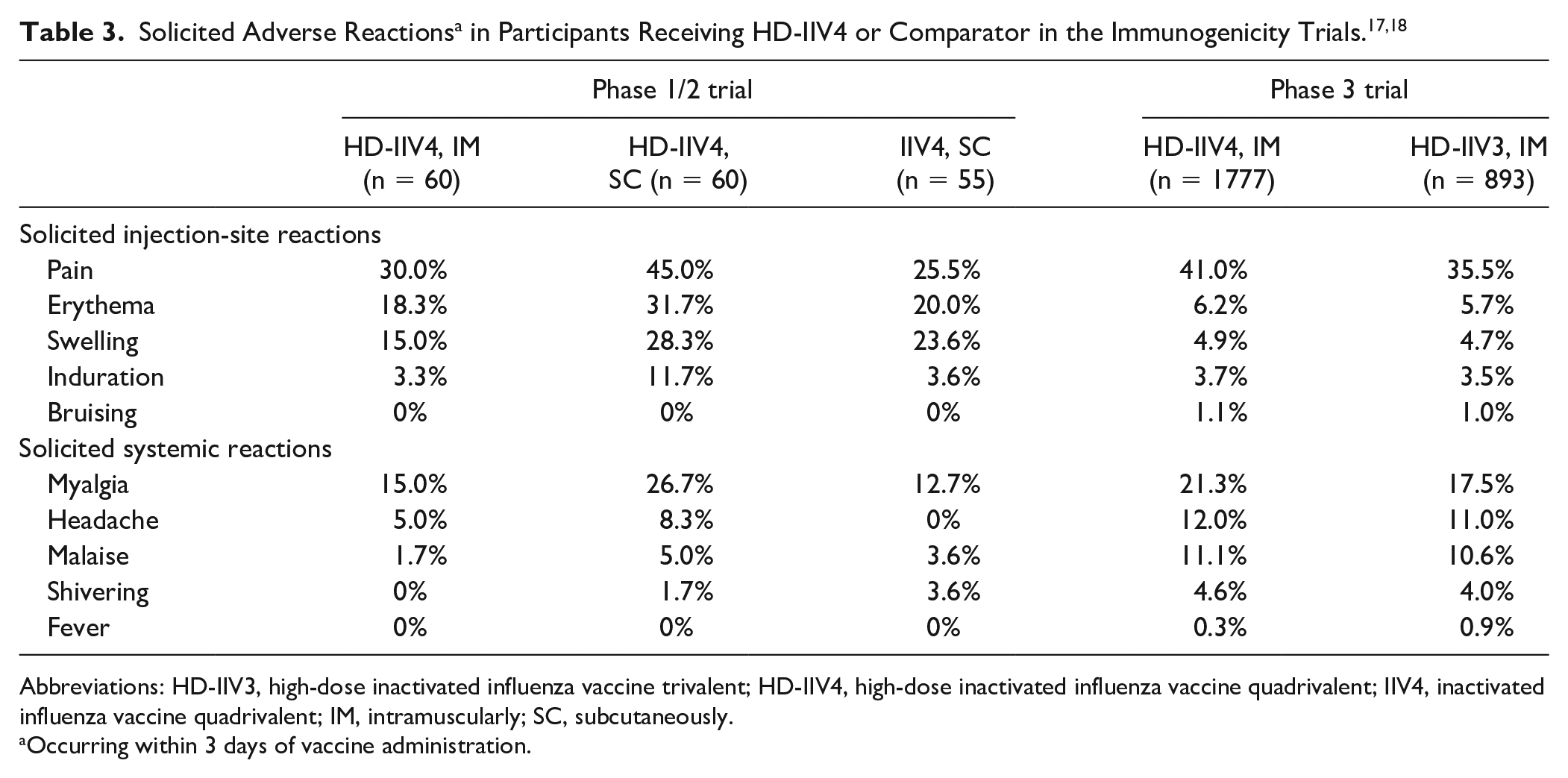
Abbreviations: HD-IIV3, high-dose inactivated influenza vaccine trivalent; HD-IIV4, high-dose inactivated influenza vaccine quadrivalent; IIV4, inactivated influenza vaccine quadrivalent; IM, intramuscularly; SC, subcutaneously.
Occurring within 3 days of vaccine administration.
In the phase 1/2 trial, solicited reactions were more common in the HD-IIV4 SC arm. 17 Most solicited reactions were of mild to moderate intensity, started within the first 3 days after vaccination, and resolved within 7 days of onset. The proportions of any unsolicited adverse events were the same in the HD-IIV4 IM and HD-IIV4 SC arms (6.7%) and were higher in the IIV4 SC arm (14.5%). Treatment-related unsolicited adverse events, mostly injection-site pruritus, were reported more often in participants vaccinated SC than IM (1.7% vs 5.0% vs 7.3%). No immediate unsolicited adverse events, adverse events leading to study discontinuation, deaths, or adverse events of special interest were reported. A single serious adverse event of sudden hearing loss 3 days after vaccination was reported in the IIV4 SC arm. The event was not considered related to the vaccination.
In the phase 3 trial, solicited reactions were more common in the HD-IIV4 arm than in the HD-IIV3 arm; however, <1% of individuals reported their reactions as severe, and most reactions began within 3 days of vaccination and resolved within 3 days of onset. 18 The proportions of any unsolicited adverse events (16.4% vs 16.5%), immediate adverse events (0.3% vs 0.2%), adverse events leading to study discontinuation (<0.1% vs 0.2%), serious adverse events within 28 days (1.1% vs 1.3%), serious adverse events up to 6 months (4.5% vs 5.4%), serious adverse events related to study drug (<0.1% vs 0%), deaths (0.2% in both arms), and adverse events of special interest (<0.1% vs 0.2%) were similar between the HD-IIV4 and the HD-IIV3 arms. A serious adverse event of special interest related to HD-IIV4 was reported for 1 participant. The event was a moderate small-fiber neuropathy involving both sensory and autonomic fibers diagnosed 42 days after vaccination.
Patients or caregivers should be provided with a Vaccine Information Statement per the requirements of the National Childhood Vaccine Injury Act prior to each immunization and should be instructed to report adverse reactions to their provider and/or to the Vaccine Adverse Event Reporting System.24,25
Availability, Dosage, and Administration
The vaccine is supplied as a single-dose prefilled syringe without needle containing 240 µg of HA—60 µg of A(H1N1), 60 µg of A(H3N2), 60 µg of B-Victoria, and 60 µg of B-Yamagata—in a 0.7-mL suspension. 11 The vaccine contains 4 times the amount of antigen of IIV, hence the term high-dose. 3 The syringe is made without natural rubber latex and can be safely given to persons with latex allergy. 11 The vaccine should be stored in the refrigerator between 2 and 8 °C and must be discarded if it was frozen. 11 The recommended dose of HD-IIV4 for adults aged 65 years and older is 0.7 mL administered IM in the deltoid muscle once every year. 11 The CDC recommends that vaccination should be offered by the end of October to provide protection against influenza before the influenza season begins. 3 Health care professionals can begin administering vaccines as soon as supplies are available and throughout the influenza season; however, vaccinating too early (ie, August) is likely to result in suboptimal immunity before the end of the influenza season, particularly among older adults. 3
Relevance to Patient Care and Clinical Practice
The safety and immunogenicity of HD-IIV4 in adults aged 65 years and older was demonstrated in a phase 3 trial, where the added second B strain resulted in improved immunogenicity against the added strain without compromising the immunogenicity of the other strains or the vaccine’s tolerability compared with HD-IIV3; however, HD-IIV4 was associated with more injection-site and systemic adverse reactions than HD-IIV3. 18 The efficacy and safety of HD-IIV3 in adults aged 65 years and older was demonstrated in a phase 3 trial, where HD-IIV3 resulted in significantly higher antibody responses and better protection against influenza than IIV3. 8 HD-IIV4 will be available in the 2020-2021 influenza season. 26 An adjuvanted inactivated influenza vaccine quadrivalent (aIIV4) will also be available in the 2020-2021 influenza season. 27 Other available vaccines with less robust evidence of efficacy and effectiveness in older adults include aIIV3 and RIV4. 28 There are no head-to-head clinical trials comparing the efficacy and safety of HD-IIV4 with that of aIIV3. 3 Although aIIV3 was shown to be immunogenic in adults aged 65 years and older compared with IIV3, it has not been shown to prevent influenza in a randomized clinical trial. 3 In addition, aIIV3 contains a novel adjuvant, which may be an issue if it is administered with other vaccines that contain novel adjuvants, such as the recombinant herpes zoster vaccine and the adjuvanted hepatitis B vaccine, because the safety and efficacy of administration of 2 vaccines containing novel adjuvants, either concomitantly or at other intervals, have not been evaluated.3,29,30 There are also no head-to-head clinical trials comparing the efficacy and safety of HD-IIV4 with that of RIV4. 3 Nonetheless, RIV4 was shown to be effective at preventing influenza in adults aged 50 years and older in one randomized clinical trial. 10 The CDC does not express preference for any licensed age-appropriate vaccine type over another in older adults and states that vaccination should not be delayed if a specific product is not available. 3 However, the CDC acknowledges that HD-IIV3 has been the most extensively studied in older adults, and evidence has accumulated for its superior efficacy and effectiveness compared with IIV3 in this patient population, but in terms of safety, HD-IIV3 is associated with a higher frequency of injection-site and systemic reactions than IIVs. 3 The average wholesale price of 1 dose of HD-IIV4 is expected to be $117.90, which is higher than the average wholesale price of IIV4s. 31 Although the cost of HD-IIV4 relative to other influenza vaccines is an important factor to consider when deciding to add to the formulary, some pharmacoeconomic studies have demonstrated the cost-effectiveness of HD-IIV3 in older adults.32-34
Conclusion
With the approval of HD-IIV4, clinicians now have an additional vaccine to prevent influenza in adults aged 65 years and older. HD-IIV4 has been shown to be safe and immunogenic compared with HD-IIV3, and the latter has been shown to be safe and more effective than IIV3 in preventing influenza in older adults. HD-IIV4 carries warnings regarding the occurrence of Guillain-Barré syndrome within 6 weeks following previous influenza vaccination. HD-IIV4 appears to be associated with more adverse reactions than HD-IIV3 and IIV4. The most common injection-site reaction associated with HD-IIV4 is pain, and the most common systemic reaction is myalgia. Whereas HD-IIV4 is useful in all older adults, it may be particularly useful in those at a further increased risk of complications from influenza such as those with comorbid conditions and those who reside in long-term care facilities.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Chahine serves on the speakers’ bureaus of Merck & Co, Inc, and Paratek Pharmaceuticals, Inc.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.