
Abstract
Objective
To evaluate the current literature for tisagenlecleucel in the treatment of relapsed/refractory (r/r) B-cell acute lymphoblastic leukemia (ALL).
Data Sources
A literature search of PubMed (inception to June 18, 2020) and ClinicalTrials.gov was conducted using the following search terms: CTL019, chimeric antigen receptor, CAR-T, and tisagenlecleucel.
Study Selection and Data Extraction
All trials evaluating the use of tisagenlecleucel in B-cell ALL were reviewed and considered for inclusion.
Data Synthesis
Tisagenlecleucel displayed overall remission rates ranging from 69% to 93% in patients who historically respond extremely poorly to salvage therapy. Remissions were durable, with 12-month relapse-free survival (RFS) rates of 55% to 59%. These promising results are tempered by the unique adverse effect profile of chimeric antigen receptor (CAR) T-cell therapy. Potentially life-threatening cytokine release syndrome (CRS) occurred in 77% to 100% of patients, and immune effector cell–associated neurotoxicity syndrome (ICANS) developed in 31% to 45% of patients receiving tisagenlecleucel.
Relevance to Patient Care and Clinical Practice
The successful utilization of tisagenlecleucel therapy requires meticulous planning, prudent patient selection, multidisciplinary collaboration, and expert training to ensure optimal patient care. The complex interplay of patient- and treatment-related factors creates problematic barriers that must be expertly navigated by the health care team and authorized treatment center.
Conclusions
As the first US Food and Drug Administration–approved gene therapy, tisagenlecleucel heralds an immunotherapeutic breakthrough for treating pediatric and young adult patients with r/r B-cell ALL. Many questions surrounding patient-specific gene and cellular therapies remain, but their transformative potential in cancer care remains promising.
Keywords
Introduction
Acute lymphoblastic leukemia (ALL) is an aggressive hematological malignancy characterized by the rapid proliferation and infiltration of blastic B or T cells into the bone marrow, peripheral blood, and other organs. 1 Among children, ALL remains the most commonly diagnosed malignancy, comprising approximately 25% of all malignancies in those less than 15 years of age.2-6 Fortunately, 5-year overall survival (OS) in children and adolescents with ALL now exceeds 90%, though approximately 20% of ALL patients experience relapsed/refractory (r/r) disease following initial therapy.4,5 Adults with ALL have a significantly worse overall prognosis compared with pediatric patients, with 5-year OS rates of only 20% to 40%.7,8 Despite recent advances in treatment, overall prognosis for patients with r/r ALL remains poor.5,6 Children and adolescents with r/r disease have an estimated 5-year OS of 20% to 30%, decreasing with each subsequent relapse.2-5 Overall, r/r ALL represents a leading cause of childhood cancer-related mortality and continues to be a significant therapeutic challenge.2,6
There is currently no standard of care for pediatric and adult patients with r/r ALL. Most approaches have historically included high-dose multidrug chemotherapy.5,9 Unfortunately, these options do not typically provide long-term disease-free remission, making allogeneic stem cell transplant (SCT) preferred in qualifying patients.10,11 Monoclonal antibodies such as blinatumomab and inotuzumab ozogamicin are US Food and Drug Administration (FDA)-approved for r/r ALL but fail to provide durable responses in most patients.12-14 Blinatumomab, an anti-CD19 bispecific T-cell engager, achieved an overall response in 39% of pediatric patients and 43% of adult patients with r/r ALL.13,14 Furthermore, the median relapse-free survival (RFS) for those who experienced a complete remission (CR) was 4.4 months (95% CI = 2.3-7.6 months) and 5.9 months (95% CI = 4.8-8.3 months) in pediatric and adult patients, respectively.13,14 Inotuzumab ozogamicin is a humanized anti-CD22 antibody-drug conjugate that delivers calicheamicin, a cytotoxic antibiotic agent, directly to CD22-positive B cells. The phase 3 INO-VATE ALL trial showed a CR rate of 80.7% (95% CI = 72.1%-87.7%) and a duration of remission of 4.6 months (95% CI = 3.9-5.4 months) in adult patients with r/r ALL. 12 Clofarabine and vincristine sulfate liposomal injection are also FDA approved as single-agent options in this population, but both displayed low overall response rates of 30% and 20%, respectively, with poor durability and disease control.15,16
Immunotherapy provides a novel approach to directly targeting leukemic cells using autologous T cells that bypass chemoresistance and provide sustained antitumor surveillance, making them a promising option in chemotherapy-resistant malignancies. 2 Chimeric antigen receptor (CAR) T cells uniquely recognize surface antigens independent of the major histocompatibility complex (MHC), thereby eliminating the need for antigen presentation. Since the early 2000s, research has focused on using CD19 as a molecular target for CAR T-cell therapy because of its relative abundance in various cancer types. 17 University of Pennsylvania School of Medicine and the Children’s Hospital of Philadelphia (CHOP) in conjunction with Novartis Pharmaceuticals developed the CAR T-cell–based therapy known as CTL019. Figure 1 shows a timeline of key events leading to the creation and approval of tisagenlecleucel on August 30, 2017, as the first FDA-approved gene therapy. Tisagenlecleucel is indicated for patients up to 25 years of age with r/r B-cell precursor ALL. 18
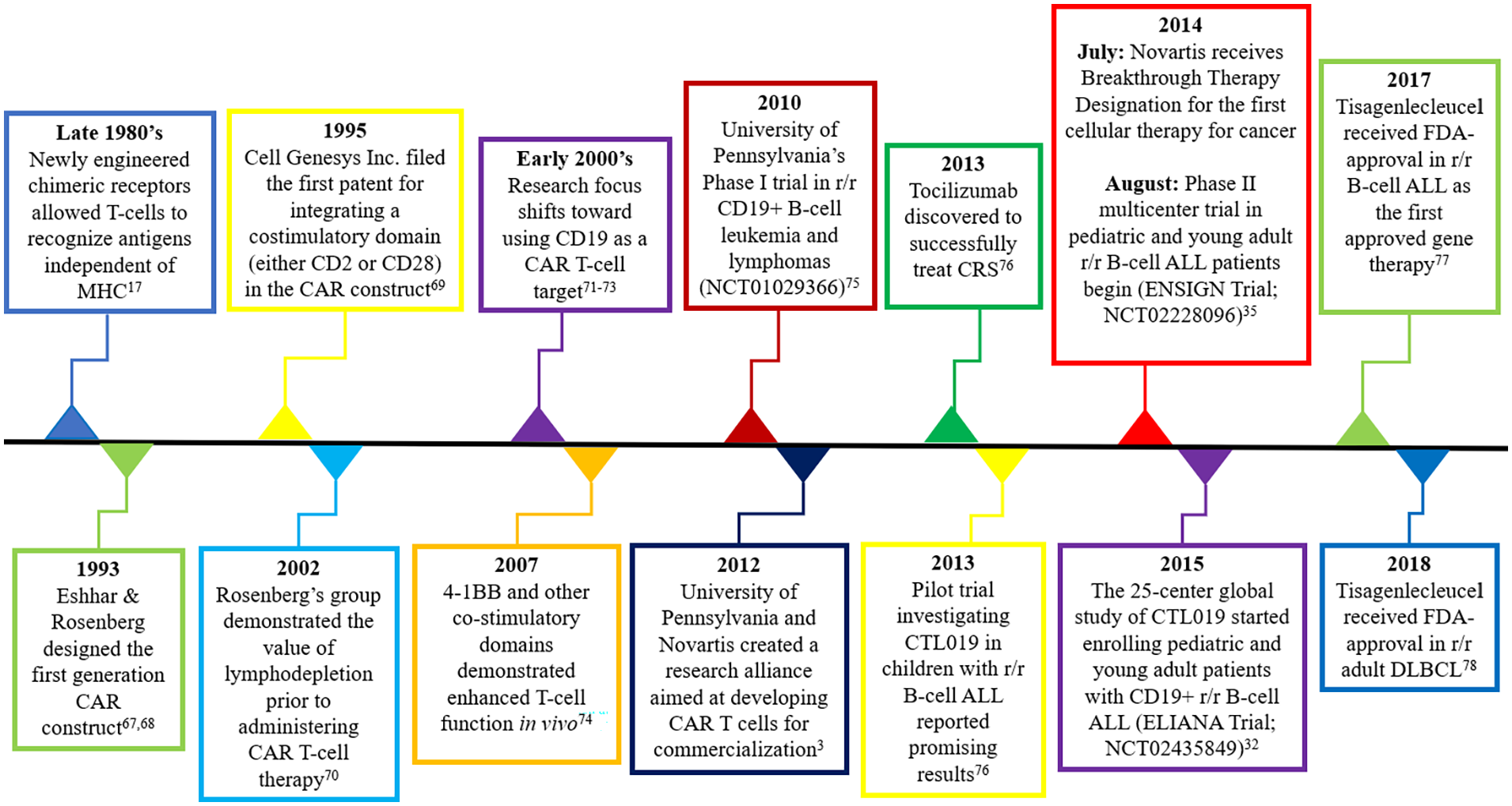
Timeline of key events leading to the creation and approval of tisagenlecleucel.
The aim of this review is to summarize the safety and efficacy data for tisagenlecleucel in r/r B-cell precursor ALL and to provide a practical discussion on the clinical considerations involved with CAR T-cell therapy.
Data Sources
A systematic English-based literature search was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 19 A literature search was conducted using PubMed from inception through June 18, 2020, in human subjects only. Search terms included CTL019, chimeric antigen receptor, CAR-T, and tisagenlecleucel. In addition, we included these search terms on ClinicalTrials.gov for completed trials not published in PubMed. Relevant articles and abstracts found within identified citations were also evaluated for consideration. Only trials evaluating the safety and efficacy of CTL019/tisagenlecleucel in B-cell ALL were considered for inclusion and analysis. The literature search was verified by 2 separate investigators.
Pharmacology
T cells are an important component of the adaptive immune response and act as orchestrator and protagonist of cellular immunity. In 1909, Paul Ehrlich proposed that both innate and adaptive immunity play key roles in preventing carcinogenesis. 20 Ehrlich’s hypothesis, which is now well established, states that the immune system plays a pivotal role in preventing cancer development and halting its progression. One mechanism that helps prevent cancer progression involves the presentation of tumor antigens to both CD8+ and CD4+ T cells by antigen-presenting cells. In addition to this important role, antigen-presenting cells also stimulate the differentiation and proliferation of lymphocytes by providing a costimulatory signal such as B7 that interacts with CD28 and activates clonal expansion of the T cell. Given enough time and activity, cytotoxic T cells will then actively target and destroy cancer cells. Additionally, T cells activate memory B cells, which are capable of providing sustained immunosurveillance. 21 A high density of memory lymphocyte markers within tumor cells showed positive prognostic value in cancer patients, providing strong evidence for the immunosurveillance hypothesis. 22
Overview of CAR T-cell Design and Function
CAR T-cell therapy offers a unique immunological approach to managing patients with r/r B-cell ALL. Genetic engineering is used to create autologous, adoptive cellular treatment options with high immune specificity, effectively turning ordinary T cells into “hunter cells” with enhanced anticancer predilections. 23 One key benefit of CAR T-cell therapy over other immunotherapies is their ability to act as “living drugs” that undergo rapid expansion with persistent anticancer activity for months to years following initial treatment. 24 Tisagenlecleucel, formerly known as CTL019, is a CAR T-cell immunotherapy requiring autologous T cells that undergo ex vivo genetic modification to express a CD19-specific CAR. Following genetic manipulation, CAR T-cell activation occurs in an MHC-independent manner. 24 Tisagenlecleucel contains a CD19-specific murine single-chain variable fragment (scFv) antibody fused to the intracellular signaling domains of 4-1BB (CD137) and CD3ξ.3,24 After binding to CD19 antigens on the cell surface, the CAR transmits a signal that allows T-cell activation, proliferation, and a robust antitumor response.
Both the intracellular receptor signaling domain and the costimulatory domain are required to optimally initiate T-cell activation and enhance the expansion and perseverance of the antitumor drug. First-generation CAR T-cell therapies did not include costimulatory domains and were generally disappointing in preclinical evaluation. 17 Therefore, second-generation CAR T-cell products, such as tisagenlecleucel, were designed with costimulatory domains to augment antitumor activity and prolong drug persistence. One important difference between CAR products is the specific costimulatory domain selected (Figure 2). Various costimulatory domains are now under investigation, including 4-1BB, CD28, CD2, CD27, TLR2, and OX40.3,25 Whereas tisagenlecleucel incorporates the 4-1BB domain, axicabtagene ciloleucel (Yescarta; Kite Pharma, Inc), an FDA-approved CAR T-cell agent for r/r large B-cell lymphoma, utilizes CD28. 26 The costimulatory variations selected for specific CAR designs may play an important role in their cellular kinetics, cytotoxic function, and safety profile. For instance, CAR T cells incorporating the 4-1BB domain may persist for years following treatment, whereas those with the CD28 domain generally persist for several months.26,27 Third-generation CARs utilizing more than 1 costimulating domain (eg, CD28 and TLR2) are now being investigated. 28 The ideal domain pairing and optimal CAR design remains to be determined and is likely dependent on tumor microenvironment and specific clinical indication. Most CAR T-cell therapies are currently directed at CD19, a B cell and B-cell precursor surface antigen commonly expressed on most B-cell malignancies, including chronic lymphocytic leukemia (CLL), B-cell non-Hodgkin lymphoma, and B-cell ALL.29,30 Research is currently underway assessing CAR T-cell therapy with alternative antigen targets in both hematological and solid malignancies. 25
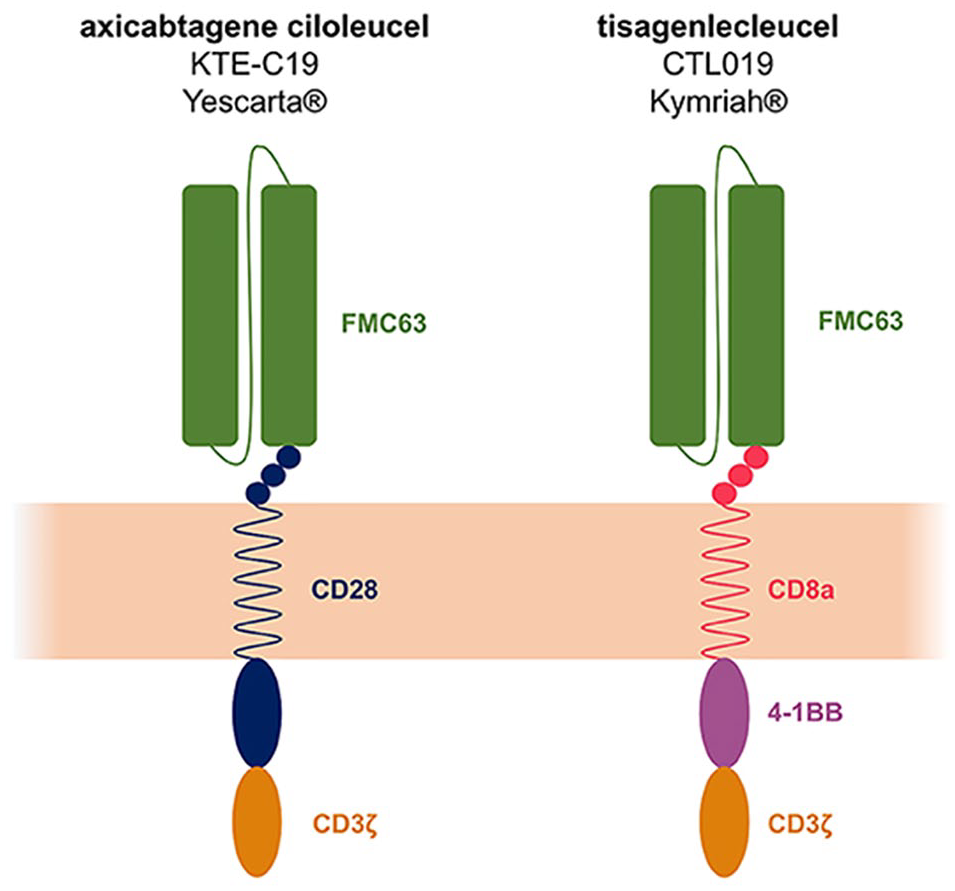
Chimeric antigen receptor (CAR) structure and design. Second-generation CAR T-cell products, axicabtagene ciloleucel (KTE-C19) and tisagenlecleucel (CTL019), share similar CAR constructs with identical CD19-specific murine single-chain variable fragment (FMC63-scFv) and intracellular signaling domain (CD3ξ). The costimulatory domain for axicabtagene ciloleucel (CD28) is different from that for tisagenlecleucel (4-1BB).a
CAR T-cell Manufacturing and Administration
Overall, the manufacturing and delivery of CAR T cells remain complex, with several key steps (Figure 3). Initially, cellular harvest via leukapheresis is required to obtain donor T cells that will then be sent to the manufacturing facility. Pediatric and adult patients have variable leukapheresis protocols to reduce perfusion-related adverse drug reactions such as hypovolemia, hypothermia, and hypocalcemia. Prior to leukapheresis, methotrexate and other immunomodulator therapies should be discontinued. 3 Once the manufacturer receives sufficient donor CD3+ cells, activation is initiated using antibody-coated beads (anti-CD3/anti-CD28) serving as artificial dendritic cells. Following activation, the T cells must undergo transduction and reprogramming using lentiviral-mediated infection to encode the desired CAR. These engineered T cells undergo rapid ex vivo expansion over 8 to 12 days before being shipped back to the treatment facility in a single bag, ready for intravenous infusion. Tisagenlecleucel is manufactured in the United States with a target turnaround time of 22 days. 27
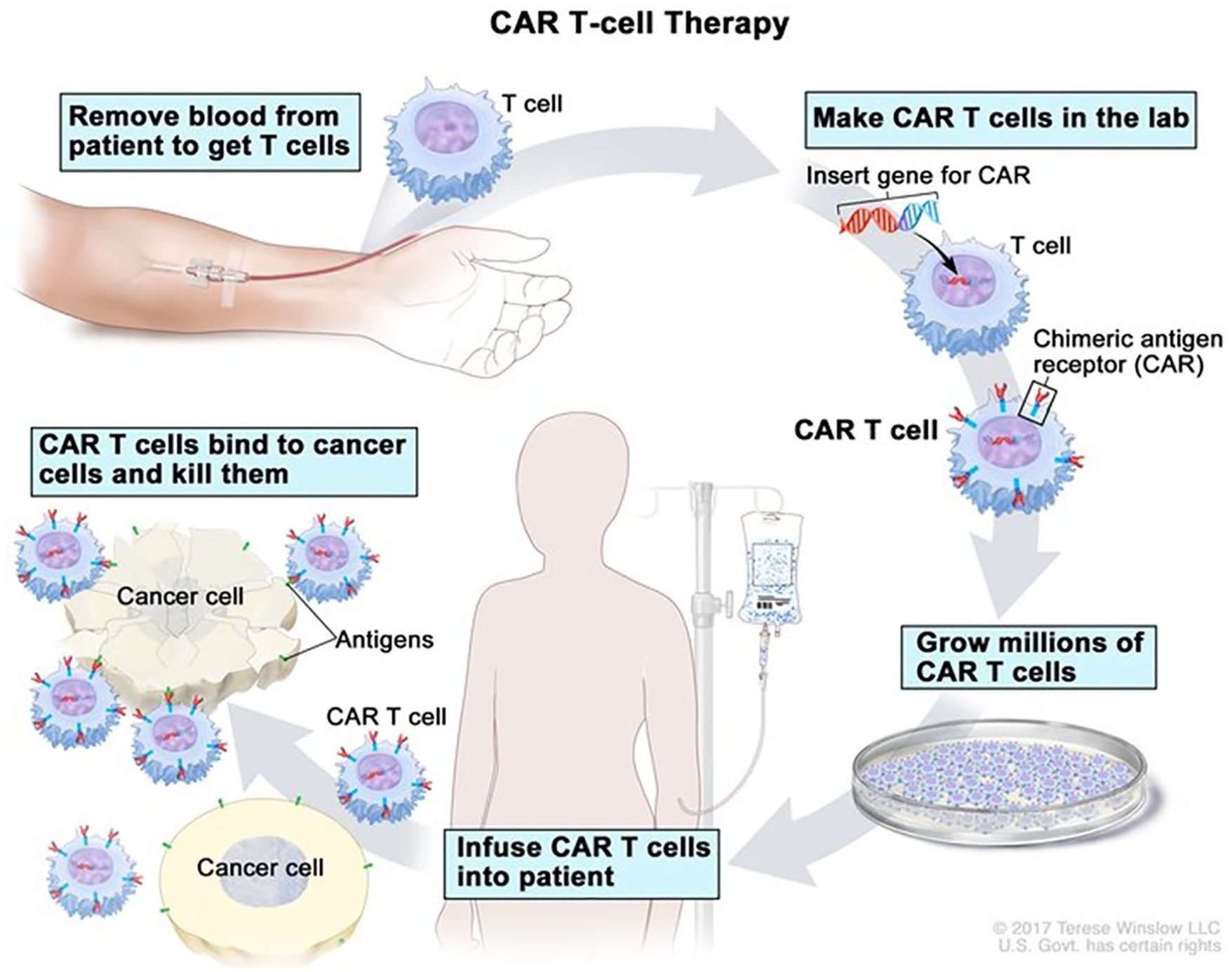
Chimeric antigen receptor (CAR) T-cell treatment process.a
Following leukapheresis and prior to tisagenlecleucel administration, patients typically receive lymphodepleting chemotherapy using a highly myelosuppressive fludarabine-based regimen to provide disease control while awaiting CAR T-cell therapy and to allow for clonal expansion following tisagenlecleucel infusion. 27 The recommended lymphodepleting regimen consists of fludarabine (30 mg/m2) for 4 days and cyclophosphamide (500 mg/m2) for 2 days followed by a single dose of tisagenlecleucel containing 0.2 to 0.5 × 106 CAR-positive T cells/kg for patients weighing ≤50 kg or 0.1 to 2.5 × 108 CAR-positive T cells/kg for patients weighing >50 kg. Cellular kinetics show initial exponential growth with a maximal concentration occurring 10 days after infusion, followed by a biexponential decline. 27 Some patients receiving tisagenlecleucel displayed persistent and measurable CAR T-cell levels up to 780 days after initial therapy.31,32
Data Synthesis
Clinical Evidence in Pediatric and Young Adults With r/r ALL
In 2014, Maude et al 33 published the results of the first single-institution phase I/IIa trial evaluating the use of CTL019 cells in patients with r/r ALL (Table 1). Researchers at the; CHOP and the University of Pennsylvania School of Medicine included 25 patients aged 5 to 22 years and 5 patients aged 26 to 60 years to test the efficacy of CTL019 cells in r/r B-cell ALL. Doses of 0.76 × 106 to 20.6 × 106 cells/kg were administered after lymphodepleting therapy with fludarabine and cyclophosphamide. CTL019 cells produced a CR in 90% (27/30 patients) of patients, with 73% of patients achieving minimal residual disease (MRD)-negative status. After a median follow-up of 7 months, 19 patients remained in remission following treatment with CTL019 cells. At 6 months, the rates of event-free survival (EFS) and OS were 67% and 78%, respectively.
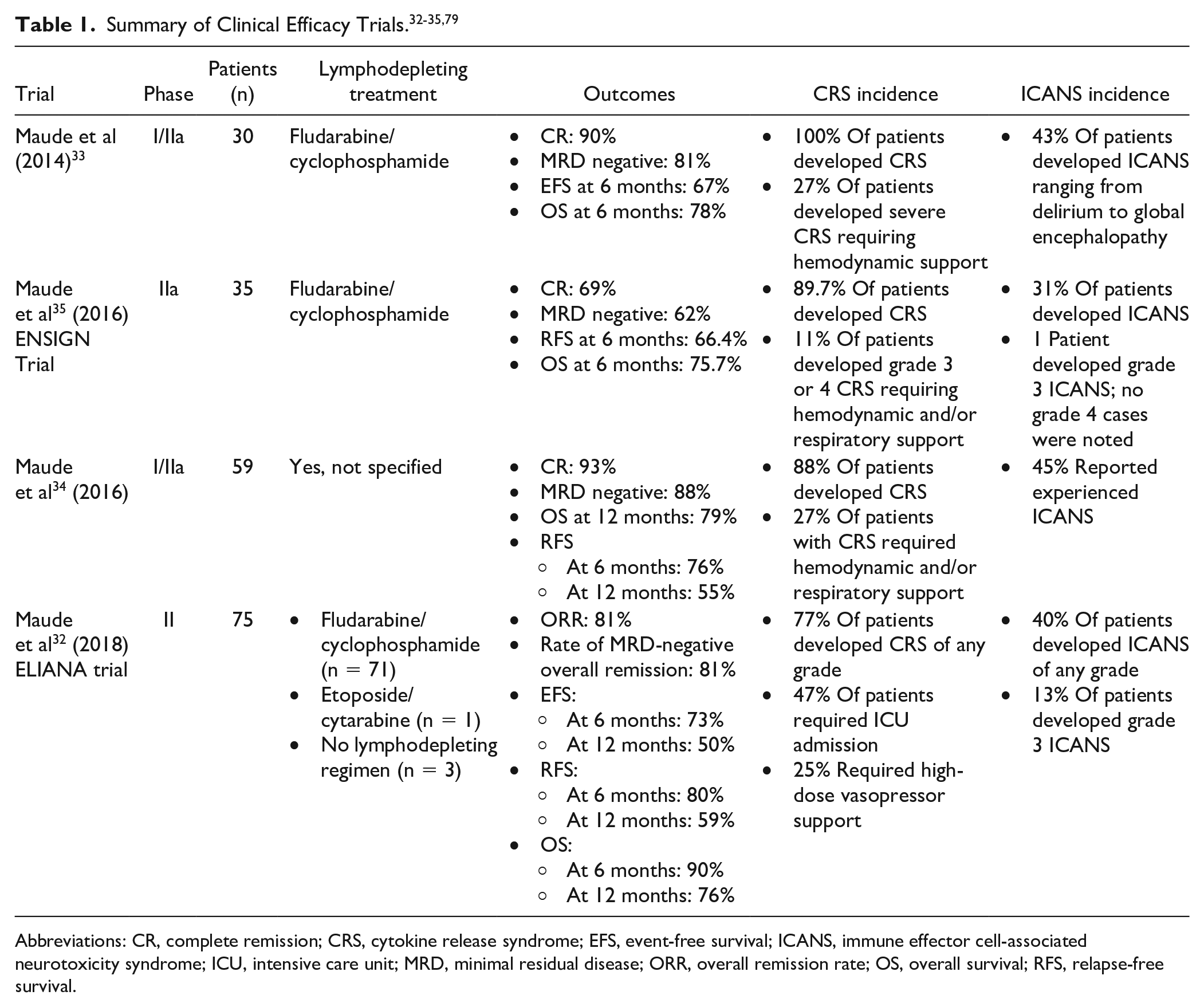
Abbreviations: CR, complete remission; CRS, cytokine release syndrome; EFS, event-free survival; ICANS, immune effector cell-associated neurotoxicity syndrome; ICU, intensive care unit; MRD, minimal residual disease; ORR, overall remission rate; OS, overall survival; RFS, relapse-free survival.
A follow-up study to the original CHOP trial was published in 2016. 34 This analysis evaluated 59 patients aged 20 months to 24 years with r/r ALL. One month after infusion of CTL019 at a dose of 107 to 108 cells/kg, the rate of CR was 93% (55/59 patients), with 88% of patients achieving MRD-negative status. With a median follow-up of 12 months, 58% (34/59 patients) remained in remission. The rate of RFS was 76% at 6 months and 55% at 12 months. OS was 79% at 12 months. These nascent CHOP reports provided the first key evidence showing the benefit of CTL019 cells in patients with r/r ALL, but this experience was limited to a single institution.
The ENSIGN 35 trial was conducted to broaden the evidence for CTL019 cells in r/r ALL. Across the United States, 9 institutions participated in this single-arm trial. After lymphodepletion with fludarabine and cyclophosphamide, 29 patients received CTL019 cells at a target dose of 2.0 to 5.0 × 106 cells/kg for those weighing ≤50 kg or 1.0 to 2.5 × 108 cells/kg for those weighing >50 kg. The primary efficacy outcome was the overall remission rate (ORR), which includes patients who achieved CR with incomplete blood count recovery. Investigators reported an ORR of 69% (22/29 patients). At 6 months, the rates of RFS and OS were 66.4% and 75.7%, respectively. Over a median follow-up time of 6.4 months, 12 patients remained in remission. The ENSIGN 35 and original CHOP trials33,34 paved the way for the pivotal ELIANA 32 trial that would assess the feasibility of providing CAR T cells to patients worldwide.
The ELIANA 32 trial was an international, multicenter, phase II clinical trial published in 2018. A total of 107 patients across 11 countries were screened; 92 patients were enrolled, and 75 patients received tisagenlecleucel at 25 different study sites. The patients included were 3 to 21 years of age with a diagnosis of r/r B-cell ALL. Prior to infusion of the study drug, 96% of patients received lymphodepleting therapy, predominantly with fludarabine and cyclophosphamide. The median dose of tisagenlecleucel infused was 3.1 × 106 cells/kg. An ORR of 81% was achieved, with 77% of all eligible patients attaining MRD-negative status. The rates of RFS and EFS were 80% and 73% at 6 months and 59% and 50% at 12 months, respectively. A median duration of response had not been reached. In addition, OS at 6 and 12 months was 90% and 76%, respectively. Tisagenlecleucel produced lasting remissions in this multiply relapsed and historically difficult-to-treat patient population. Based on the results of this study, the FDA approved tisagenlecleucel (Kymriah; Novartis) for the treatment of r/r B-cell ALL in patients up to 25 years of age. 27 An updated analysis on the ELIANA 32 trial was presented at the 2018 American Society of Hematology Annual Meeting. 36 Investigators reported stable outcomes with an 18-month OS probability of 70% and tisagenlecleucel blood concentrations persisting for 30 months or longer in responding patients, corroborating the impressive early findings originally reported.
Safety
CAR T-cell therapy displays unique toxicities requiring thorough planning and hypervigilant monitoring. Conventional chemotherapy may result in nonspecific complications, such as myelosuppression, multiorgan system damage, and secondary cancers. CAR T-cell toxicities, on the other hand, are on-target effects with a limited duration. 37 Three common and potentially life-threatening toxicities include cytokine release syndrome (CRS), immune effector cell-associated neurotoxicity syndrome (ICANS), and B-cell aplasia. 37 Based on the international ELIANA 32 trial, 89% of patients experienced “any adverse event of special interest,” including CRS, ICANS, infection, neutropenic fever, tumor lysis syndrome, and unresolved cytopenias by day 28. Furthermore, 73% of patients experienced a grade 3 or 4 adverse event suspected to be related to tisagenlecleucel. The most common adverse events occurring in at least 20% of patients included the following: acute kidney injury, bleeding episodes, cough, CRS, decreased appetite, delirium, diarrhea, edema, encephalopathy, fatigue, headache, hypogammaglobulinemia, hypotension, hypoxia, infection, nausea, pyrexia, tachycardia, and vomiting. 27
Although CAR T-cell therapy has the potential to revolutionize the treatment of B-cell malignancies, and possibly other cancers, practitioners are required to have a firm understanding of the unique toxicity profile associated with this novel therapeutic option. The National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) grading system is routinely used for grading most adverse events related to cancer therapy. 38 This approach, however, was created before the emergence of cellular-based therapies and did not adequately cover toxicities such as CRS and ICANS. Initially, various grading criteria across clinical trials and institutions were created to fill this gap. Trials evaluating CTL019, for instance, utilized the Penn Grading System for CRS, whereas axicabtagene ciloleucel research incorporated the modified Lee criteria.26,27,39 The lack of uniform grading across trials and CAR T-cell products complicates and prevents reliable comparisons of the incidence and severity of CAR T-cell–associated toxicities. To harmonize definitions and grading criteria, The American Society of Transplant and Cellular Therapy (ASTCT; formerly American Society for Blood and Marrow Transplantation) published the ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with ICANS guidelines in 2019 (Table 2). 40 The ASTCT consensus score is readily calculated at the patient’s bedside and appears to be gaining traction as the preferred scoring system in clinical practice.
ASTCT Toxicity Grading Scales. 40
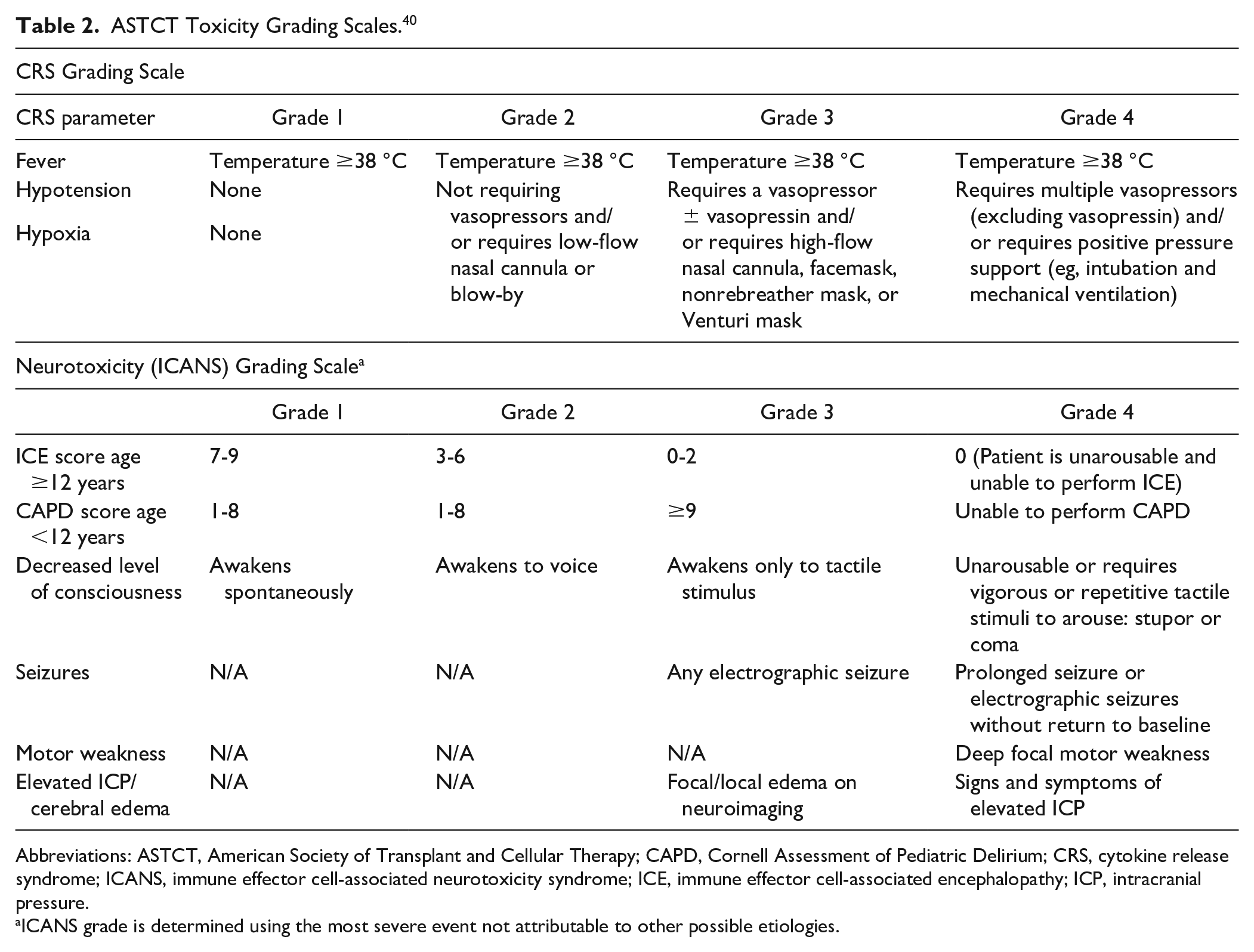
Abbreviations: ASTCT, American Society of Transplant and Cellular Therapy; CAPD, Cornell Assessment of Pediatric Delirium; CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome; ICE, immune effector cell-associated encephalopathy; ICP, intracranial pressure.
ICANS grade is determined using the most severe event not attributable to other possible etiologies.
Cytokine Release Syndrome
The most frequent and life-threatening acute complication of CAR T-cell therapy is CRS, with a median time to onset of 3 days (range, 1-51) following tisagenlecleucel administration. 27 CRS is a global inflammatory response generated as a direct result of CAR T-cell expansion, immune system activation, and antitumor effects, culminating in constitutional symptoms of severe flu-like illness and progressing to multiorgan dysfunction in severe cases. 39 This supraphysiological response results from immune cell activation, which triggers the production of multiple cytokines and inflammatory markers. C-reactive protein, ferritin, interferon (IFN)-γ, interleukins (IL-1, IL-2, IL-4, IL-6, IL-8, and IL-10), tumor necrosis factor (TNF)-α, and granulocyte-macrophage colony-stimulating factor (GM-CSF) are some of the cytokines and inflammatory markers implicated in the pathogenesis of CRS. 41 IL-6, in particular, appears to play a central pathophysiological role, as evidenced by the rapid symptom resolution following anti–IL-6 therapy.32,42 Excessive cytokine production contributes to the constellation of CRS manifestations, including arthralgias, fever, headaches, hypotension, malaise, myalgias, respiratory changes, and rigors. The cardinal features of CRS are fever, hypotension, and hypoxia. 39 Fortunately, the deleterious effects of this on-target toxicity are typically reversible when promptly identified and appropriately treated. In the ELIANA 32 trial, CRS was extremely common, with 77% of patients experiencing any grade of CRS and 47% experiencing grade ≥3 CRS. Furthermore, 47% of all patients required intensive care unit (ICU) admission for CRS management, 37% received tocilizumab therapy, and 25% were given high-dose vasopressors. The median duration of ICU admission following a CRS episode was 7 days (range, 1-34). 32 Tocilizumab (Actemra; Genentech), a humanized anti–IL-6 monoclonal antibody indicated for the treatment of rheumatoid arthritis, gained FDA approval in 2017 for the management of CAR T-cell–induced severe or life-threatening CRS.27,43,44 Tocilizumab is dosed at 8 mg/kg in patients weighing ≥30 kg (maximum dose of 800 mg) and 12 mg/kg in patients weighing <30 kg. In patients with persistent CRS, dosing may be repeated every 8 hours for up to 4 total doses.
All patients need to be carefully identified and managed for CRS. Grade 3 and 4 CRS are considered to be severe, along with certain high-risk grade 2 cases. 27 Risk factors for the development of severe CRS include high disease burden, preexisting comorbidities, and early symptom onset. 41 Grade 1 CRS can typically be managed with supportive care measures alone, including intravenous fluids, antipyretics, and an appropriate workup for infectious etiologies (Table 3).27,43 Grade 2 CRS requires appropriate supportive care along with tocilizumab. Grades 3 and 4 CRS require ICU admission for close monitoring and aggressive supportive care measures, including supplemental oxygenation via facemask or ventilation, vasopressors, tocilizumab, and possibly methylprednisolone, dexamethasone, or hydrocortisone.27,43,45 Corticosteroids are used with caution in patients receiving CAR T-cell therapy with suspected CRS because of their inherent ability to diminish or eradicate activated CAR T cells. The potential abrogation of CAR T cells by concomitant corticosteroids, though theoretical and unsubstantiated, is worth careful consideration. Currently, corticosteroids may be appropriate to utilize in cases of life-threatening emergencies. Finally, while awaiting results from the infectious disease workup, broad-spectrum antibiotics appropriate for patients with suspected neutropenic fever are required to manage CRS.27,32,43
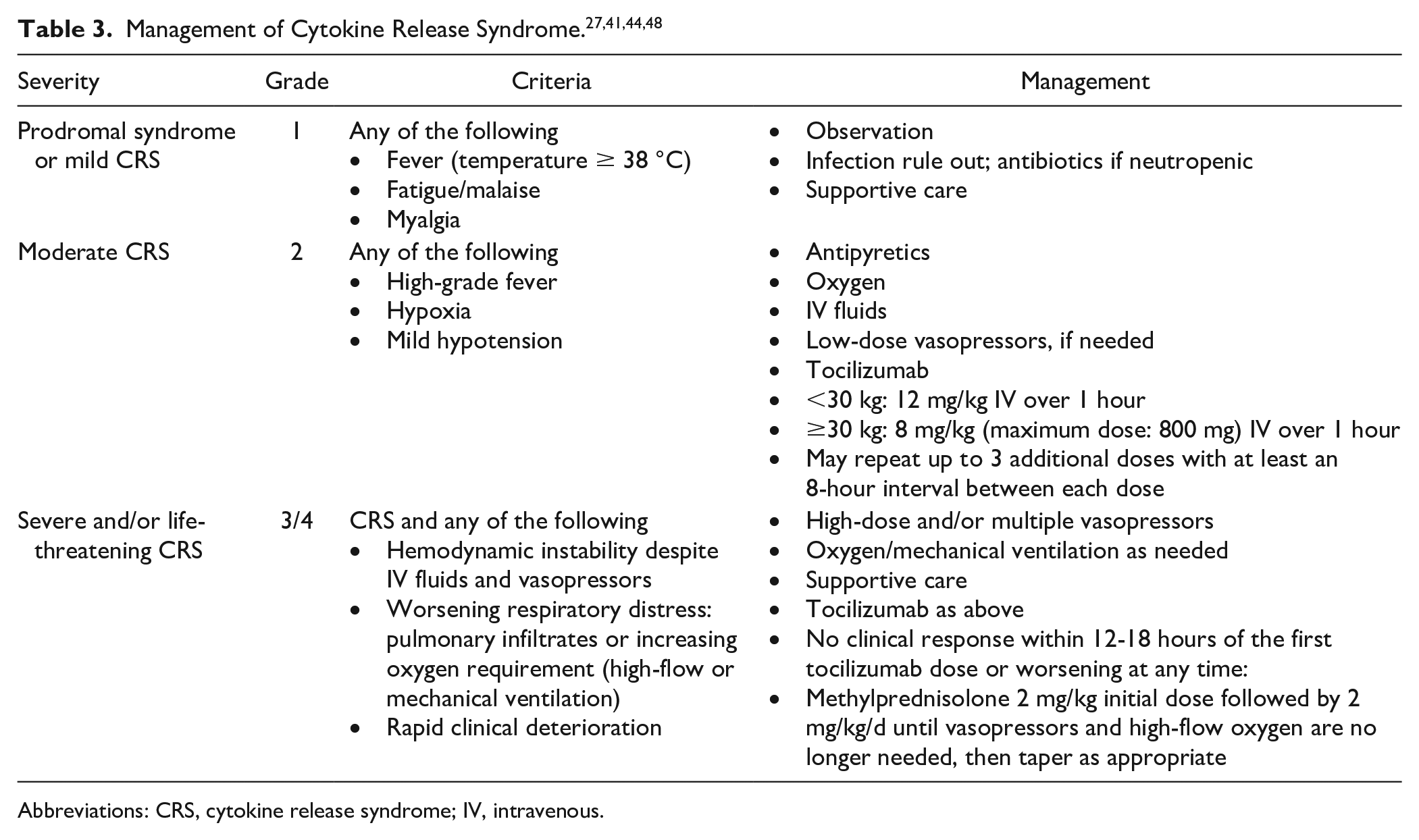
Abbreviations: CRS, cytokine release syndrome; IV, intravenous.
Clinical response to tocilizumab therapy is rapid and marked, with most patients experiencing symptom relief (ie, defervescence) within hours and resolution of catecholamine-dependent shock within a median of 4 days. 42 Prophylactic and early-intervention strategies utilizing tocilizumab therapy for the prevention of CRS require further analysis. No reports to date have evaluated the use of prophylactic tocilizumab before the onset of CRS symptoms, and questions surrounding the role of IL-6 in stimulating initial CAR T-cell expansion remain. Investigators at the University of Pennsylvania and the CHOP are currently evaluating tocilizumab timing optimization following tisagenlecleucel in high-risk pediatric ALL patients (NCT02906371). Siltuximab (Sylvant, Janssen Biotech, Inc) and sarilumab (Kevzara, Sanofi) are potential alternatives to tocilizumab for the treatment of CAR T-cell–induced CRS. Siltuximab is an anti–IL-6 monoclonal antibody indicated for multicentric Castleman’s disease. 46 Siltuximab has a high affinity for IL-6 itself, rather than the IL-6 receptor, thereby reducing circulating IL-6 and theoretically minimizing ICANS. Additional research is needed to further evaluate the clinical implications of direct IL-6 inhibition. Siltuximab is currently recommended for use in tocilizumab-refractory CRS. Sarilumab is another FDA-approved monoclonal antibody for rheumatoid arthritis that has a high affinity for the IL-6 receptor. 47 Currently, there are no published reports on the safety or efficacy of sarilumab for the treatment of CRS.
Immune Effector Cell–Associated Neurotoxicity Syndrome
Neurotoxicity, also known as CAR-related encephalopathy syndrome or ICANS, is the second most common acute toxicity following CAR T-cell infusion. 48 It most frequently presents as agitation, anomia, confusion, delirium, disorientation, encephalopathy, somnolence, and tremors, possibly progressing to seizures, aphasia, cerebral edema, and coma.2,3,27,48,49 The underlying mechanism leading to ICANS remains elusive. Some researchers hypothesize that it is a direct consequence of CRS, with endothelial activation and enhanced blood-brain barrier permeability allowing inflammatory cytokines to penetrate and damage the central nervous system.49,50 Despite high CAR T-cell penetration into the cerebral spinal fluid, severe ICANS is still uncommon, and CAR T cells are present in the cerebral spinal fluid without the presence of central nervous system disease. 48 Similar to CRS, host and tumor factors may play a role in the development of ICANS. For instance, high tumor burden, active infection, and elevated baseline inflammatory markers, such as C-reactive protein, ferritin, IFN-γ, and TNF-α, may correlate with disease severity. 50
Most cases of ICANS occur within the first 8 weeks postinfusion, with a median time of onset of 6 to 7 days and median duration lasting another 6 to 7 days, though some cases have been reported 3 to 4 weeks postinfusion.3,27 ICANS more commonly appears in conjunction with or shortly following CRS; however, it may develop with, after, or in the absence of CRS.2,3,27,48-50 ELIANA 32 reported neurological events in 40% of patients within 8 weeks of tisagenlecleucel infusion. The most common neurological events were encephalopathy (11%), confusion/delirium (9%), tremor (8%), agitation (7%), and somnolence (7%). Grade 3 neurological events occurred in 13% of patients, with 1 patient experiencing a seizure. Management of ICANS consists of supportive care measures, with tocilizumab playing no role in mitigating neurotoxicity because of its inability to cross the blood-brain barrier.2,3,27,48-50 In addition, tocilizumab administration in the absence of CRS may be detrimental, potentially resulting in elevated IL-6 concentrations in the cerebral spinal fluid and further potentiating the risk for ICANS.51-53 Instead, corticosteroids, typically dexamethasone or high-dose methylprednisolone, are the preferred treatment in moderate to severe cases.3,48,49,54 Seizure prophylaxis with levetiracetam (750 mg orally every 12 hours), starting on the day of CAR T-cell infusion or at the first sign of ICANS, may be considered to help minimize neurological sequelae. 25 Recent evidence suggests that IL-1 and GM-CSF are important players in the pathophysiology of both CRS and ICANS.55-57 Anakinra, an IL-1 receptor antagonist used in rheumatoid arthritis, may provide theoretical benefit in patients with both CRS and ICANS; however, no prospective clinical trial exists for this indication, and further research is required. 56 Lenzilumab, an investigational GM-CSF neutralizing monoclonal antibody, may reduce neuroinflammation and improve ICANS in CAR T-cell patients, based on preclinical models. 57 Additional research is underway to further evaluate lenzilumab in patients receiving axicabtagene ciloleucel (NCT04314843). Fortunately, ICANS generally appears to be transient and self-limiting.2,25,48 The majority of cases resolve completely, with minimal long-term deficits. 49
B-cell Aplasia
B-cell aplasia and subsequent hypogammaglobinemia are expected on-target off-tumor effects of anti-CD19 CAR T-cell therapies resulting from a robust CAR T-cell response that depletes normal B cells expressing CD19.3,48,49 These cytopenias increase patient susceptibility to infections, warranting antibiotic prophylaxis and intravenous immunoglobulin (IVIG) supplementation.2,27,48 Immunoglobulin levels need to be monitored postinfusion and IVIG supplementation continued until B-cell recovery.2,3,27,48 Cytopenias and hypogammaglobulinemia blunt the body’s response to vaccines, so live vaccines should not be given within 6 weeks of CAR T-cell infusions or until the immune system has recovered postinfusion.3,27 There have been reports of B-cell aplasia lasting up to 2 years, but long-term effects have yet to be determined because of lack of follow-up data.2,49 Fortunately, it can be easily managed with IVIG without significantly compromising quality of life. 54 The ELIANA 32 trial showed that 83% of patients had B-cell aplasia at 6 months and was present in 100% of patients who responded to tisagenlecleucel therapy.
Overall mortality resulting from tisagenlecleucel therapy in the ELIANA 32 trial was low. A total of 19 patients died following tisagenlecleucel administration. Of these patients, 2 died within 30 days of infusion. The first patient died from fatal cerebral hemorrhage with concomitant coagulopathy and CRS 15 days after tisagenlecleucel. The second death resulted from progressive B-cell ALL. The remaining 17 patients experienced the following causes of death: B-cell ALL relapse or progression (12 patients), pneumonia or hepatobiliary disease following new therapies for ALL (2 patients), viral encephalitis with prolonged neutropenia/lymphopenia (1 patient), systemic mycosis with prolonged neutropenia (1 patient), and unknown causes (1 patient).
Relevance to Patient Care and Clinical Practice
ALL is the most commonly diagnosed cancer in children, with current survival rates exceeding 90% as a result of improved risk stratification, advanced methods of detecting residual disease, and a better understanding of disease biology. 54 Pediatric and adult patients who relapse after initial ALL treatment have dismal outcomes with traditional high-dose multidrug chemotherapy. 54 Allogeneic SCT remains a viable option for qualifying patients; however, treatment-related morbidity and mortality concerns limit this option, with only 40% of patients experiencing long-term survival.58,59 Current treatment regimens for pediatric and adult patients with multiply r/r ALL are inadequate for this unmet medical need. Salvage options may include clofarabine, blinatumomab, inotuzumab ozogamicin, vincristine sulfate liposomal injection, and various combination chemotherapy regimens. There is no current standard of care for these patients, and enrollment in a clinical trial is recommended whenever possible. Overall, these therapeutic options remain marred by toxicity concerns and poor durability.2,14-16
Across multiple clinical trials, tisagenlecleucel displayed promising response rates, with durable remissions that far exceeded other treatment options for multiply r/r ALL patients.32-35 CAR T-cell therapy heralds a novel approach to cancer treatment but harbors significant toxicities requiring advanced training and expertise. Tisagenlecleucel is only available through a risk evaluation and mitigation strategy (REMS) program known as KYMRIAH REMS. Furthermore, tisagenlecleucel is only available at select treatment centers with prespecified capabilities, including SCT. One component of REMS approval includes the ability to procure and store at least 2 doses of tocilizumab for each patient receiving tisagenlecleucel. All pharmacists, nurses, physicians, and advanced practitioners interacting with patients receiving tisagenlecleucel must receive FDA-mandated training focused on the management of CAR T-cell–related toxicities.
In the ELIANA 32 trial, 76% of patients received CAR T-cell infusion in the inpatient setting. Because most will experience CRS in the first few days following administration, the majority of institutions require an inpatient admission for at least 3 to 7 days. 45 Furthermore, patients are typically required to remain within proximity of the certified treatment center for at least 4 weeks following CAR T-cell infusion. 27 Tisagenlecleucel manufacturing costs and reimbursement rates are also noteworthy concerns for patients, providers, and treatment centers. A single infusion of tisagenlecleucel, as announced by Novartis, is priced in the United States at $475 000. 60 This cost is significantly more than the $290 000 estimated cost for myeloablative allogeneic SCTs. 61 Additionally, the $475 000 price tag does not include ancillary costs required for tisagenlecleucel therapy, including evaluation, leukapheresis, hospital admission, possible ICU care, tocilizumab, and other potential treatment requirements. 60 With the various costs associated with CAR T-cell therapy and current reimbursement rates, hospitals may lose up to $300 000 per patient. 62 Spending on cancer care in the United States is expected to reach $158 billion by 2020. 63 Given the high cost of tisagenlecleucel, cost-effectiveness research is vital for the evaluation and integration of CAR T-cell therapy into general practice. A National Institutes of Health–funded analysis conducted in 2019 concluded that “CAR-T therapy may represent a cost-effective option for pediatric relapsed/refractory B-ALL, although longer follow-up of CAR-T survivors is required to confirm validity of these findings.” 64 Moreover, reimbursement for novel cellular therapies remains highly contentious and an area of national discourse and interest. 62 In 2020, the Centers for Medicare and Medicaid Services (CMS) released its proposed Hospital Inpatient Prospective Payment System rule for 2021. 65 CMS outlined a separate hospital payment category for CAR T-cell therapy called the Medicare Severity Diagnostic Related Group for CAR-T. This CMS proposal, if implemented, would ameliorate some of the barriers to CAR T-cell access by providing a predictable payment rate for treatment centers. Similar obstacles exist for current commercial payer reimbursement structures. 62
Other noteworthy patient- and treatment-specific barriers that require thoughtful navigation include geographic limitations creating restricted access to tisagenlecleucel therapy; medical insurance constraints, including prior authorization difficulties; lymphodepleting regimen and timing; manufacturing complications; and persistent lentiviral vector presence postinfusion.27,32 Collaboration between health care providers, professional societies, regulatory agencies, policy makers, insurance providers, and cooperative treatment groups is imperative for facilitating appropriate access to cellular therapy and providing optimal patient care for those who do have access. The patient referral process, identifying suitable patients, and receiving payor authorization can significantly delay the projected timeline if the treatment center lacks experience in navigating these challenging obstacles. The ELIANA 32 trial reported a median time from study enrollment to infusion of 45 days (range, 30-105). The window between leukapheresis and CAR T-cell infusion is a high-risk period for patients, and reducing the overall time to infusion should be a key goal for manufacturers as we move forward with increased CAR T-cell use.
Future research is underway to determine how early in treatment, and with what specific risk stratifications, tisagenlecleucel can and should be given for pediatric and young adult patients with newly diagnosed ALL (NCT03876769, NCT03123939). The next phase of efficacy studies evaluates tisagenlecleucel in first-line therapy for very-high-risk pediatric ALL patients. The Children’s Oncology Group, in conjunction with Novartis, initiated the AALL1721/Cassiopeia Study (NCT03876769) to evaluate frontline tisagenlecleucel therapy in ALL patients with poor early response to conventional chemotherapy. This phase II clinical trial is an international collaboration that will help determine the viability and utility of incorporating cellular immunotherapy into upfront treatment for certain high-risk ALL subgroups. With an estimated enrollment of 140 participants, AALL1721/Cassiopeia is projected to conclude in 2027. Immunotherapy remains a hotbed of research and clinical interest, with more than 1000 cellular-based therapies and 500 CAR T-cell products in the global pipeline. 66 Ongoing research into CAR T-cell therapy encompasses a wide range of malignancies, including non-Hodgkin lymphoma, multiple myeloma, acute myelogenous leukemia, CLL, and even common solid tumors.
Conclusion
Because of the poor prognosis and overall paucity of suitable chemotherapy-based treatment options for patients with r/r ALL, research has shifted to alternative options, particularly immune- and cellular-based therapies. Tisagenlecleucel, a novel CAR T-cell therapy, represents a powerful tool in the clinician’s armamentarium for the treatment of high-risk pediatric and young adult patients with r/r B-cell ALL. Although still in its infancy, CAR T-cell therapy directed at CD19-positive disease offers notable response and survival rates for these difficult-to-treat patients. This burgeoning therapeutic option presents unique and potentially life-threatening toxicities requiring careful planning and meticulous monitoring by expert practitioners in well-equipped cancer treatment centers. Ultimately, tisagenlecleucel has reshaped the landscape of r/r ALL treatment and, with additional research, could potentially alter upfront therapy for high-risk patients with newly diagnosed ALL. With the growing number of clinical trials and marked interest from industry sponsors, government agencies, and academic centers, CAR T-cell therapy represents the dawning of a new era in contemporary cancer treatment. Tisagenlecleucel, as the vanguard for this novel therapeutic class, is a landmark agent highlighting the unprecedented promise and significant challenges of cellular immunotherapy and genetic engineering in r/r ALL treatment.
Footnotes
Authors’ Note
The authors of this article have the following to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect interest in the subject matter of this article: Zachery Halford, nothing to disclose; Mary Kate Anderson, nothing to disclose; Lunawati L. Bennett, nothing to disclose; Jonathan Moody, nothing to disclose.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.