
Abstract
Background:
Zoledronic acid every 4 weeks (Q4wk) reduces the incidence of skeletal-related events (SREs) in patients with metastatic lung cancer. Lung cancer patients were excluded from extended-interval dosing trials (every 12 weeks [Q12wk]) that demonstrated noninferiority of the 2 dosing schemes. To date, the optimal dosing of zoledronic acid in metastatic lung cancer remains unknown.
Objective:
To determine whether zoledronic acid dosed Q12wk is similar to Q4wk dosing for prevention of SRE in patients with metastatic lung cancer.
Methods:
A retrospective analysis was performed in patients with non–small-cell lung cancer and small-cell lung cancer with bone metastases who received Q12wk and Q4wk zoledronic acid. The primary outcome was incidence of SRE at 1 year. Secondary analyses included time to first SRE, overall survival (OS), incidence of osteonecrosis of the jaw (ONJ), kidney dysfunction, and hypocalcemia.
Results:
A total of 34 patients received Q12wk and 46 patients received Q4wk zoledronic acid. Incidence of SRE at 1 year (Q12wk, 23.5%, vs Q4wk, 23.9%; 95% CI = −0.184 to 0.192; P = 0.968) and median time to SRE (not reached for either cohort; P = 0.530) did not differ. The Q12wk cohort had longer median OS (24.00 vs 8.97 months; P = 0.022). There were no differences in incidence of ONJ, kidney dysfunction, and hypocalcemia.
Conclusion and Relevance:
This is the first report examining extended-interval dosing of zoledronic acid in metastatic lung cancer. Incidence and time to SRE at 1 year were similar. This extended-interval dosing may be safe and reasonable for patients with lung cancer with bone metastases.
Keywords
Introduction
Bone involvement in the setting of metastatic lung cancer is a common clinical problem affecting up to 40% of lung cancer patients. 1 Cumulative survival after bone metastasis diagnosis is poor.2-4 Presence of a skeletal-related event (SRE) reduces survival in lung cancer patients by approximately 50%.2,5-7 Common clinical features of bone metastases are SREs, such as pathological fractures, hypercalcemia, and severe pain.3,4
Zoledronic acid is FDA approved for the management of metastatic bone disease in multiple myeloma and various solid tumors, including lung cancer, because of inclusion of patients with these malignancies in phase III zoledronic acid trials.8,9 These trials demonstrated that zoledronic acid administered intravenously every 3 to 4 weeks reduces incidence of SRE, time to SRE, and pain.8,10,11 Additionally, zoledronic acid in patients with multiple myeloma has shown an improvement in overall survival (OS). 12 Historically, the importance of zoledronic acid in metastatic lung cancer has been overlooked because of poor median survival of 12 months. 3 To date, zoledronic acid has not shown an OS benefit in lung cancer. However, with recent development of targeted therapy, immunotherapy, and chemoimmunotherapeutic options, average survival time in patients with lung cancer has dramatically increased along with renewed interest in skeletal metastasis in this patient population.13,14
Despite the positive effect on patient outcomes, zoledronic acid is associated with toxic adverse effects, including osteonecrosis of the jaw (ONJ), nephrotoxicity, and hypocalcemia. Incidence of ONJ increases with cumulative zoledronic acid exposure, from 1.5% for patients treated for 4 to 12 months to 7.7% for patients treated for 37 to 38 months. 15 The FDA-approved dosing interval of every 3 to 4 weeks based on early clinical trials was arbitrary and not based on comparative studies or compelling pharmacodynamic data.16,17 The CALGB 70604 trial demonstrated that zoledronic acid every 12 weeks (Q12wk) compared with every 4 weeks (Q4wk) did not result in an increased risk of SRE over 2 years in patients with breast cancer, prostate cancer, and multiple myeloma. 18 Interestingly, safety outcomes were similar despite lower cumulative exposure of zoledronic acid in the Q12wk group. Extended-interval dosing allows for improved patient adherence to treatment plans, reduced health care provider workload, and lower treatment costs.
Currently, there is a paucity of literature addressing the optimal regimen of zoledronic acid for reducing SRE in patients with non–small-cell lung cancer (NSCLC) or small-cell lung cancer (SCLC) and metastatic bone disease. Historically at our institution, zoledronic acid every 3 to 4 weeks starting at the time of osseous metastasis diagnosis was utilized. However, clinicians at our institution extrapolated dosing zoledronic acid Q12wk to metastatic lung cancer patients as a new standard, despite their exclusion from the CALGB 70604 trial. The objective of this study is to determine whether the rate of SRE at 1 year in lung cancer patients with bone metastases receiving zoledronic acid Q12wk is similar to Q4wk dosing. Comparative incidence of adverse drug events will also be reported.
Methods and Materials
Study Design and Patient Population
This single-center, retrospective cohort analysis was conducted at Michigan Medicine in Ann Arbor, MI. Ethics approval was obtained from the International Review Board (IRB), and the study was carried out in accordance with the principles of the Declaration of Helsinki. The IRB waived written informed consent given the nature of the study.
Eligible patients included adults 18 years and older with a diagnosis of metastatic NSCLC or SCLC with at least 1 bone metastasis who received zoledronic acid for the prevention of SREs between January 1, 2012, and December 31, 2018. Bone metastases were defined as bone involvement by malignancy documented by plain radiograph, computed tomographic (CT) scan, positron emission tomographic (PET) scan, combination CT and PET scan, magnetic resonance imaging, bone scan, or skeletal survey. Patients were assigned to 1 of 2 cohorts based on receipt of zoledronic acid Q12wk or Q4wk. Patients who received at least 2 doses of zoledronic acid were eligible. Patients for whom key efficacy and safety end points were not evaluable because of incomplete medical records or who received prior IV bisphosphonates or denosumab were excluded.
Study data were collected using the electronic medical record (EMR) and managed using the Research Electronic Data Capture (REDCap) tools hosted at Michigan Medicine. Baseline demographics and disease-specific characteristics collected included age, sex, race, diagnosis, lung cancer histological subtype, molecular markers, programmed death-ligand 1 (PD-L1) testing, Numeric Pain Rating Scale (NPRS) scores, oral bisphosphonate use history, concomitant vitamin D, calcium and corticosteroid use, line of therapies received for lung cancer, concomitant chemotherapy, immunotherapy and/or targeted therapy, and serum creatinine and serum calcium levels. Baseline was defined as the time point when a patient initiated zoledronic acid treatment. The zoledronic acid dose was obtained following each administration.
Study End Points
The primary outcome was the incidence of SRE (the proportion of patients with at least 1 SRE) within 1 year of zoledronic acid initiation. SRE was defined as clinical fracture, spinal cord compression, radiation to bone, or surgery involving bone. Clinical fractures were defined as fractures identified during clinic visits and confirmed by written report of radiographic testing. Spinal cord compression was defined as neurological impairment with or without back pain and confirmed with radiographic testing. Radiation to bone was defined as using radiation to treat painful bone lesions or prevent fractures. Surgery involving bone was defined as surgical procedures meant to prevent fractures or treat clinical fractures or spinal cord compression. Secondary outcomes included time to first SRE, OS, and pain scores. Time to first SRE was defined as time in months from zoledronic acid initiation to first SRE, death, or 1 year, whichever came first. OS was defined as time in months from zoledronic acid initiation to death or last follow-up. Pain scores were based on NPRS scores reported at each zoledronic acid infusion and were not specific to bone pain. Safety outcomes included incidence of ONJ, kidney dysfunction, and hypocalcemia. ONJ was defined as a diagnosis made by a dental specialist. Grade of kidney dysfunction and hypocalcemia was based on the common terminology criteria for adverse events (CTCAEv5.0).
Statistical Analysis
All data were analyzed using SPSS software, version 26.0 (SPSS Inc, Chicago, IL). Descriptive statistics were used for baseline data to describe demographics and disease characteristics. Categorical variables were analyzed using the Pearson χ2 test or Fisher exact test. Continuous variables were analyzed using the Student t test and Mann-Whitney U where appropriate. The primary efficacy outcome was analyzed using a 2-proportion Z-test. Time to first SRE within 1 year and OS were analyzed using the Kaplan-Meier method and compared using the log-rank test. OS was determined only for patients with NSCLC because patients with SCLC represented a small percentage of patients in this analysis and demonstrate remarkably different long-term outcomes and survival. A Cox proportional-hazards regression model was used to analyze the effect of targeted therapy or immunotherapy and zoledronic acid dosing interval on OS. An α level of 0.05 was considered statistically significant. Results are reported as mean (SD) or median (range), unless otherwise specified.
Results
Patient Characteristics
The study population consisted of 80 patients, 34 in the Q12wk cohort and 46 in the Q4wk cohort (Figure 1). Baseline and disease characteristics were similar between the 2 groups, except for EGFR mutation status and treatment history (Table 1). Overall, NSCLC comprised most of the study population (n = 77, 96.3%). There were no differences in median number of bone metastases at baseline (P = 0.944), history of SRE (P = 0.555), history of oral bisphosphonate (P = 0.388), or concomitant calcium (P = 0.159), vitamin D (P = 0.921), or oral corticosteroid use (P = 0.402). Median line of systemic therapy at the time of zoledronic acid initiation was not different (median 1, range 1-4; P = 0.154). Most patients started zoledronic at the time of first systemic therapy (Q12wk, 64.7%, vs Q4wk, 78.3%; P = 0.180). A total of 14 (41%) patients in the Q12wk cohort were EGFR positive compared with 5 (10.9%) patients in the Q4wk cohort (P = 0.002). Although not significantly different, a higher percentage of patients in the Q12wk cohort harbored ALK fusions (5.9% vs 2.2%; P = 0.572), ROS1 fusions (2.9% vs 0%; P = 0.425), and PD-L1 expression ≥50% (11.8% vs 4.3%; P = 0.393). Consequently, more patients in the Q12wk cohort were treated with an EGFR inhibitor (38.2% vs 17.4%; P = 0.036), whereas the Q4wk cohort were more likely to have received traditional chemotherapy (50% vs 80.4%; P = 0.004) and bevacizumab (0% vs 15.2%; P = 0.019). Percentage of patients treated with immunotherapy were similar (Q12wk, 26.5%, vs Q4wk, 26.1%; P = 0.969). Baseline renal function and median pain scores were also similar (Table 1).
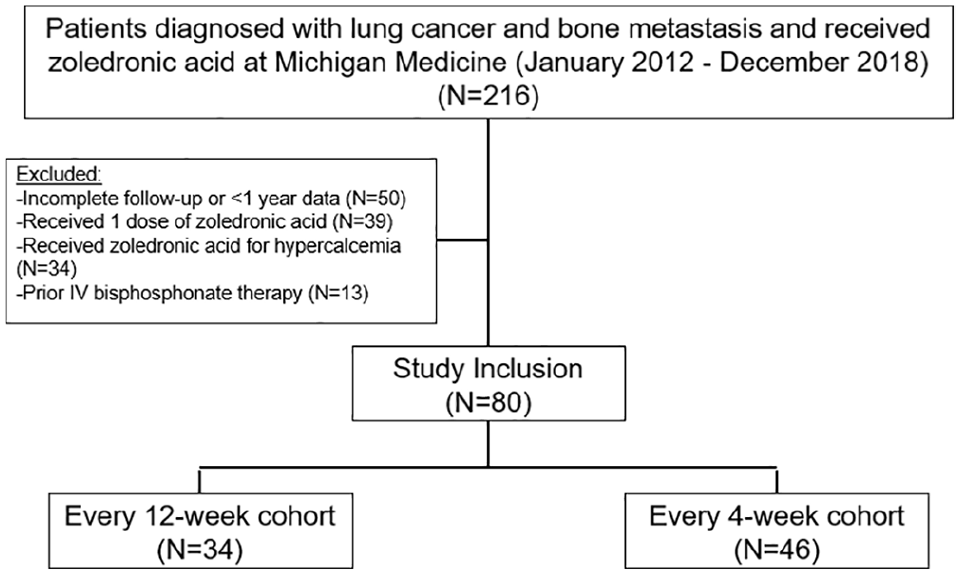
Patient enrollment and exclusion.
Demographic, Baseline Disease, and Clinical Characteristics.
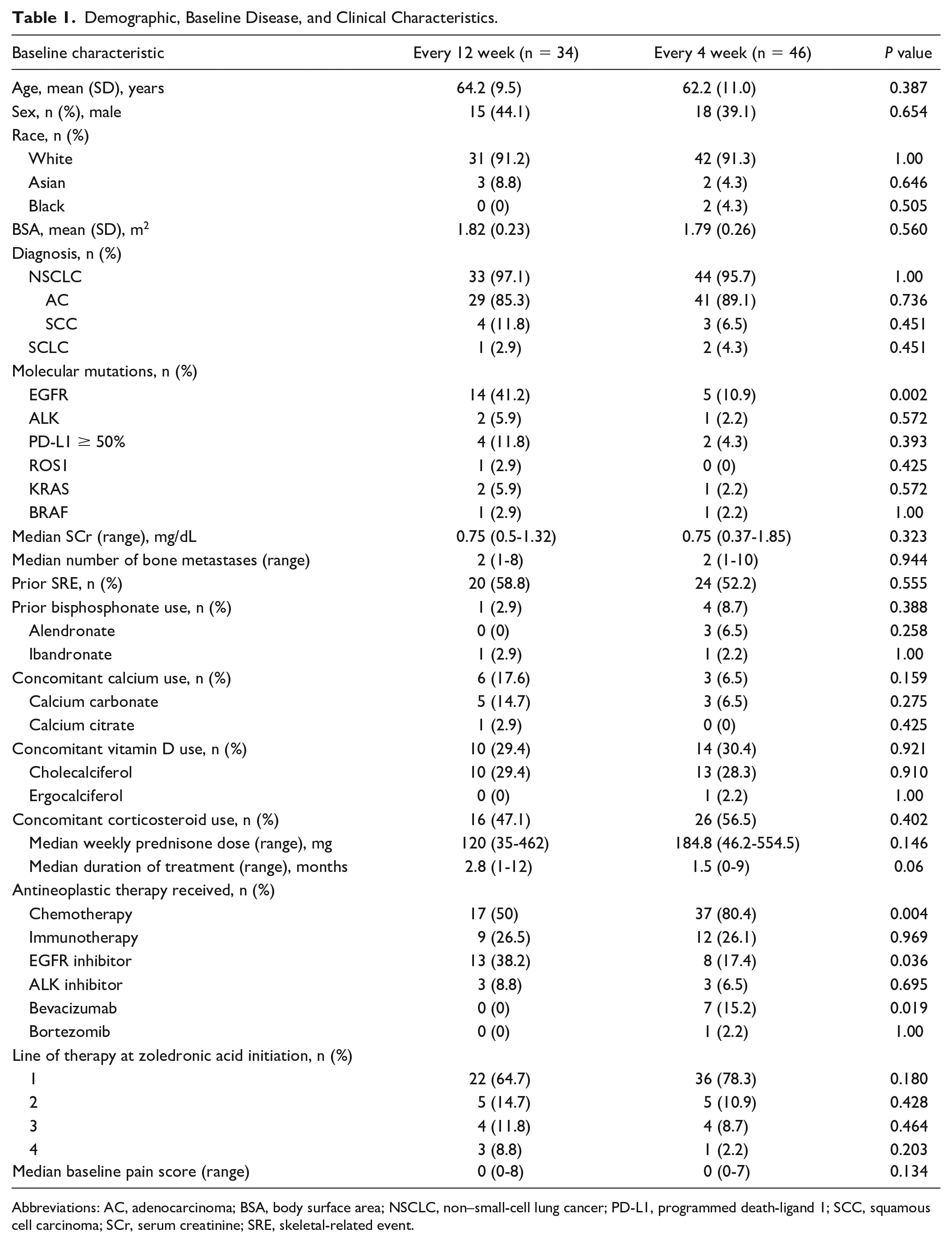
Abbreviations: AC, adenocarcinoma; BSA, body surface area; NSCLC, non–small-cell lung cancer; PD-L1, programmed death-ligand 1; SCC, squamous cell carcinoma; SCr, serum creatinine; SRE, skeletal-related event.
Efficacy Outcomes
The proportion of patients who experienced an SRE within 1 year were similar (Q12wk, 23.5%, vs Q4wk, 23.9%; 95% CI = −0.184 to 0.192; P = 0.968; Table 2). Median time to first SRE was not reached in either group (P = 0.530; Figure 2A). Average time to first SRE did not differ (Q12wk, 10.6 months, vs Q4wk, 9.9 months). The proportion of patients who experienced a second SRE was not significantly different (P = 0.572; Table 2).
Primary and Secondary Efficacy Outcomes and Safety Outcomes.
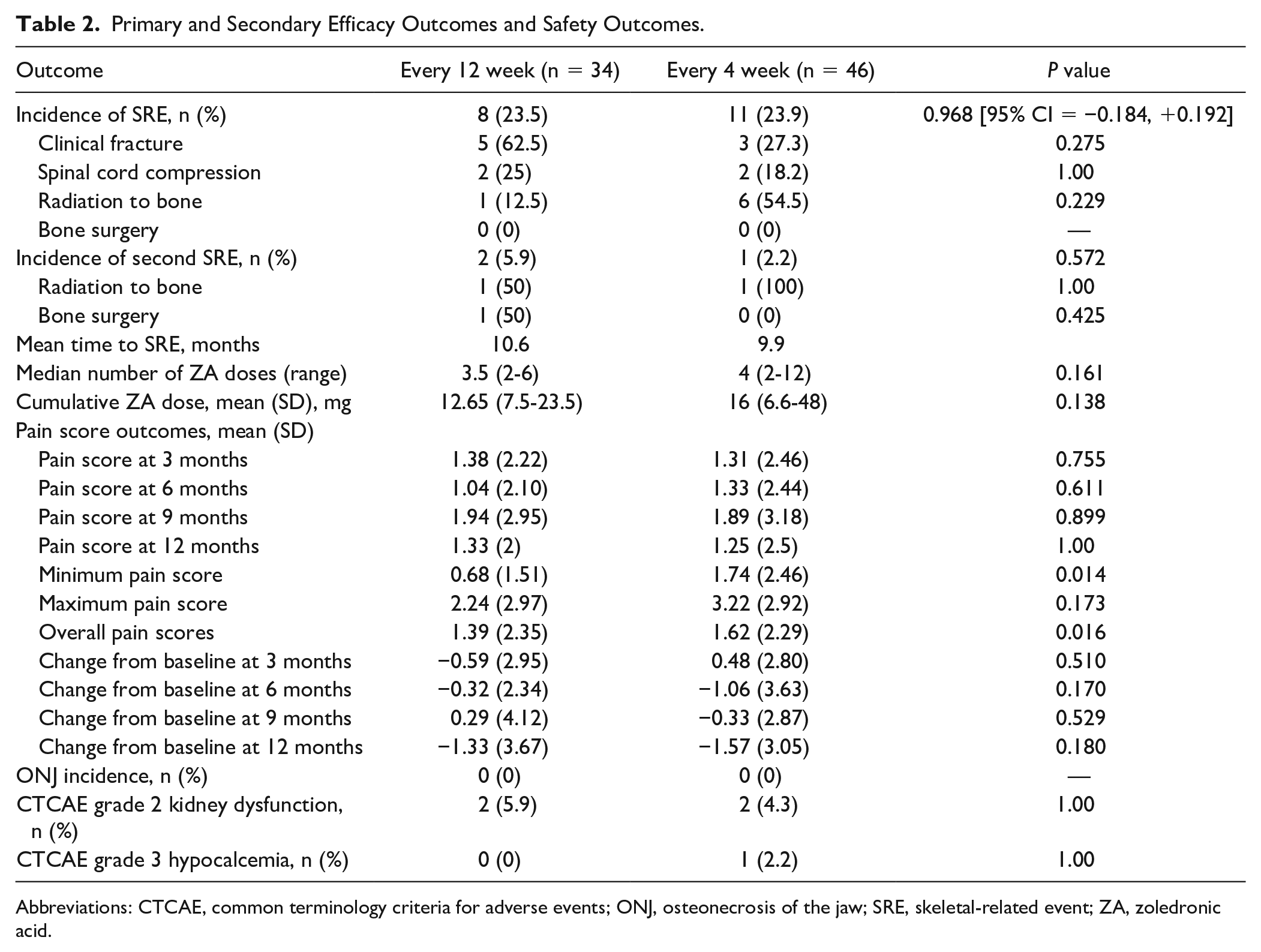
Abbreviations: CTCAE, common terminology criteria for adverse events; ONJ, osteonecrosis of the jaw; SRE, skeletal-related event; ZA, zoledronic acid.
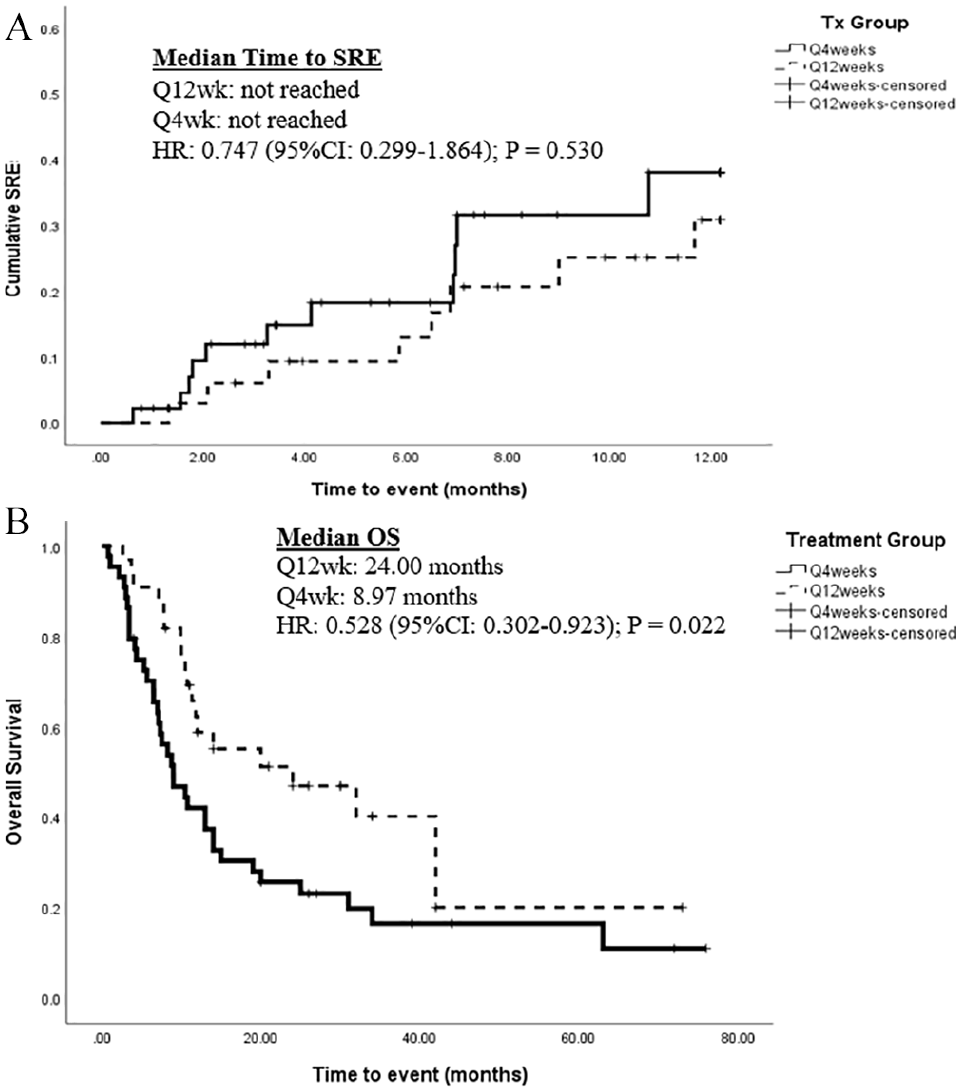
A. Time to skeletal-related event (SRE). B. Overall survival (OS).
OS analysis was performed for patients with NSCLC. Median OS was significantly longer in the Q12wk group (24.00 vs 8.97 months, P = 0.022; Figure 2B). A Cox proportional-hazards model demonstrated that only zoledronic acid dosing interval was associated with longer OS (hazard ratio [HR] = 0.528, 95% CI = 0.300-0.928, P = 0.026; Figure 2B). Receipt of targeted therapy (HR = 0.851; 95% CI = 0.487-1.486; P = 0.570) and immunotherapy (HR = 1.032; 95% CI = 0.526-2.027; P = 0.926) did not have a significant impact on survival.
Mean pain scores at months 3, 6, 9, and 12 were similar (Table 2). Mean minimum pain score over 1 year was lower for the Q12wk group (0.68 vs 1.74; P = 0.014), whereas mean maximum pain score was similar. Mean overall pain score was lower in the Q12wk cohort (1.39 vs 1.62; P = 0.016). The average change from baseline pain score at months 3, 6, 9, and 12 were similar between the 2 groups.
Safety Outcomes
There was no difference in median number of zoledronic acid doses received (Q12wk, 3.5 doses, vs Q4wk, 4 doses; P = 0.161) or total cumulative zoledronic acid dose received (Q12wk, 12.65 mg, vs Q4wk, 16 mg; P = 0.138) among cohorts (Table 2). Two patients experienced grade 2 kidney dysfunction in each cohort (Q12wk, 5.9%, vs Q4wk, 4.3%; P = 1.00; Table 2). No patient experienced grade 3 or 4 kidney dysfunction. Grade 3 hypocalcemia occurred in 1 patient in the Q4wk group. There were no instances of ONJ in either cohort.
Discussion
Bone metastases are a common complication of lung cancer despite remarkable advances in treatment. SRE secondary to bone metastases decreases median OS for this patient population. 4 Bisphosphonates remain standard of care for the prevention of SRE in these patients. Although optimal dosing for zoledronic acid is unknown, literature from various solid and hematological malignancies has demonstrated noninferiority of Q12wk to Q4wk dosing of zoledronic acid for the prevention of SRE and improved adherence.18-20 Unfortunately, patients with lung cancer were excluded from these trials because of historically poor median OS. To our knowledge, these are the first published data to demonstrate similar incidence of SRE at 1 year in lung cancer patients with bone metastases who received zoledronic acid Q12wk versus Q4wk.
The proportion of patients experiencing an SRE within 1 year (Q12wk, 23.5%, vs Q4wk, 23.9%; P = 0.968) and median time to first SRE (NR vs NR; P = 0.530) were similar between the 2 groups. Overall rate of SRE in this analysis is similar to results in previous studies—ranging from 30% to 40%—of patients with lung cancer receiving zoledronic acid. 9 Numerical differences between incidence of SRE reported in this analysis and in the published literature may be a result of drastic improvements in treatment of lung cancer demonstrated in the past decade.13,14
Median OS was significantly longer in the Q12wk cohort (24.00 vs 8.97 months; P = 0.022). This OS difference may be driven by imbalances in actionable biomarkers and lung cancer therapies between cohorts. Patients receiving Q12wk zoledronic acid were more likely to harbor actionable mutations (EGFR, ALK, and ROS1), have PD-L1 expression (PD-L1 ≥ 50%), and receive targeted agents and less likely to receive cytotoxic chemotherapy. In patients with actionable biomarkers or higher PD-L1 expression, oral targeted agents and immunotherapy drastically improve survival compared with traditional chemotherapy, which may have enhanced OS in the Q12wk group independent of zoledronic acid. Therefore, a Cox proportional-hazard model was performed, and neither receipt of targeted therapy nor immunotherapy had an independent impact on survival, whereas zoledronic acid dosing interval remained significant. Additionally, most patients were on first-line systemic therapy at the time of zoledronic acid initiation, demonstrating that patients started zoledronic acid early during their treatment for lung cancer.
Emerging data suggest decreased response of bone metastases to immunotherapy. It is theorized that the bone marrow is crucial for regulating and activating the immune system. In addition, osseous disease may exhibit decreased PD-L1 expression compared with disease found in other areas. 21 An analysis of 1588 patients with NSCLC demonstrated that presence of bone metastases was associated with lower response rates to nivolumab. 22 Furthermore, in patients with bone metastases treated with immune checkpoint inhibitors, bone involvement remains an adverse prognostic factor, and use of bone-modifying agents, including zoledronic acid, may not diminish this risk. 23 These data suggest that the type of cancer-directed therapy patients receive may affect response of disease in bone and efficacy of bone-modifying agents. Although the cohorts in this analysis were equally likely to receive immunotherapy, the growing role of immunotherapy in treating lung cancer should be considered when interpreting SRE and survival outcomes.
It could also be hypothesized that providers may opt for traditional chemotherapy with a faster mechanism of action as well as Q4wk zoledronic acid dosing in patients with more severe disease or bone pain at baseline, inherently biasing the study population. However, baseline median number of bone metastases and pain scores were similar. Because of limited sample size of this analysis and baseline differences in the receipt of targeted agents, the impact of zoledronic acid dosing interval on survival cannot definitively be made. It is likely that multiple contributing factors could explain these results, and more robust studies are needed to confirm these findings.
During the study period, overall cumulative zoledronic acid dose and median number of doses received were not different between cohorts. In the Q4wk group, 26 patients (56.5%) discontinued zoledronic acid because of death. Early deaths in the Q4wk group may have contributed to both cohorts receiving similar number of zoledronic acid doses, despite having different dosing intervals. Additionally, patients in the Q4wk group may be less adherent to more frequent administrations, resulting in less zoledronic acid doses received. No patient experienced ONJ or ≥grade 3 kidney dysfunction, and incidence of CTCAE grade 2 kidney dysfunction and CTCAE grade 3 hypocalcemia were similar between the 2 cohorts. These outcomes suggest that extended-interval dosing of zoledronic acid does not change the safety profile. The average minimum pain score and overall pain score were lower in the Q12wk group than in the Q4wk group. However, the differences are small and may not be clinically significant. The unchanged pain scores from this analysis suggest that extended-interval dosing for zoledronic acid may not result in patients experiencing more bone pain.
Cost savings is another consideration for comprehensive evaluation of a new dosing regimen. Wholesale acquisition cost for a single dose of 4 mg of zoledronic acid is approximately $45, according to the RED BOOK Online database. 24 Administering zoledronic acid 4 mg Q12wk compared with Q4wk will reduce drug costs by approximately $360 (66%) per year (Q12wk, $180, vs Q4wk, $540). Notably, this is only the cost of the medication and does not factor decreased health care resource use, via decreased health care exposure and administration costs.
This study has several limitations. First, this was a retrospective study, so we are limited to data available in the EMR and are unable to adjust for selection bias in dosing interval choice. This study is also single center, with a small sample size of 80 patients. These data may not be characteristic of a broad lung cancer patient population. Second, the data regarding SRE and key safety end points is limited to 1 year of follow up. Median time to SRE was not reached for either cohort. Third, similar cumulative zoledronic acid dose between cohorts may mask true efficacy and safety differences between dosing schemes. This analysis represents a real-world cohort of patients who may delay or discontinue zoledronic acid for various reasons. Fourth, primary treatments for lung cancer differed between cohorts, as expected. As clinicians adopted Q12wk dosing for zoledronic acid following publication of CALGB 70604, patients in the Q4wk group may represent a more historical cohort. Improvements in lung cancer treatment have been achieved in both therapy selection based on molecular markers and supportive care. Although targeted therapy did not significantly affect survival, survival differences likely stem from cumulative impact of treatment advances and improved overall care of patients with lung cancer. Fifth, the NPRS system is not specific to bone pain, resulting in a limited ability to assess the effect of extended-interval zoledronic acid on bone-related pain. Sixth, patients were not required to see dental specialists at a defined interval, nor were patients required to see a dental specialist within the health care system; the true incidence of ONJ may be underreported in this analysis. Finally, few patients had SCLC, and their disease pathophysiology and outcomes are extremely different from those with NSCLC. Thus, it is difficult to make similar conclusions regarding patients with SCLC, and they remain an area of focus.
Conclusion and Relevance
This single-center, retrospective cohort analysis demonstrates that the proportion of lung cancer patients with bone metastases experiencing an SRE within 1 year was similar whether zoledronic acid was administered Q12wk or Q4wk. Time to first SRE and adverse effect profiles were also similar. Extended-interval dosing of zoledronic acid has opportunity to save health care resources and expenditure. Although a prospective trial is needed to definitively confirm these results, zoledronic acid dosed Q12wk may be an acceptable treatment option for lung cancer patients with bone metastases that produces similar efficacy and safety. Further studies should address changes in patient quality of life with extended-interval dosing of zoledronic acid.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Angel Qin reports research funding to institution from Merck and Clovis.