
Abstract
Background
Optimal dosing of unfractionated heparin (UFH) for thromboprophylaxis in the obese patient population is uncertain because of their high-risk, prothrombotic state and a complexity of pharmacokinetic considerations. Literature on the appropriateness of the use of a higher dose UFH regimen remains unclear and inconsistent.
Objective
To evaluate the safety of the use of 7500 units every 8 hours (high-dose) of subcutaneous UFH compared with the use of 5000 units every 8 hours (standard-dose) of subcutaneous UFH for thromboprophylaxis in obese patients (defined as BMI ≥30 kg/m2).
Methods
In a retrospective cohort study, 326 adult patients were included, with a BMI ≥30 kg/m2, who were admitted to a large, urban academic medical center between September 1, 2015, and September 1, 2018. Patients received either high-dose or standard-dose UFH for at least 48 hours. The primary end point was the incidence rate of bleeding events, defined as a ≥2-g/dL fall in hemoglobin level or receipt of transfusion of 2 or more units of packed red blood cells (pRBCs) from the start of the UFH order.
Results
The incidence rate of bleeding was significantly higher in those who received high-dose UFH (43%) compared with those who received standard-dose UFH (29%; P = 0.008). No significant difference was found between venous thromboembolism event rates.
Conclusion and Relevance
High-dose UFH was associated with an increased bleeding event rate compared with standard-dose UFH in patients with a BMI ≥30 kg/m2. This raises safety concerns about the appropriateness of utilizing this regimen in this population.
Background
Venous thromboembolism (VTE), including deep-vein thrombosis and pulmonary embolism, is a major cause of morbidity and mortality, occurring in as many as 900 000 people and resulting in about 100 000 deaths in the United States annually. 1 This amounts to a tremendous clinical and economic impact in both inpatient and outpatient settings, and prophylaxis is paramount.2-4 Major risk factors include, but are not limited to, surgery, trauma, immobility, previous VTE, increasing age, pregnancy, acute medical illness, and obesity.2,5,6
According to the Centers for Disease Control and Prevention, the current prevalence of obesity in the United States is 42.4%. 3 Obesity puts patients in a prothrombotic state because of enhanced platelet reactivity, impaired fibrinolysis, and activation of endothelial cells and has been demonstrated to be an independent risk factor for the development of VTE in hospitalized patients. 4 Recent studies show that the incidence of VTE increases by 2- to 3-fold as body mass index (BMI) increases to 30 kg/m2 or greater, placing obese patients at a much higher risk of VTE.5,6 Potential altered pharmacokinetic parameters, such as a higher volume of distribution and higher clearance, complicate chemoprophylaxis dosing recommendations.7,8
Unfractionated heparin (UFH) is one of the most common injectable anticoagulant agents used for VTE prophylaxis in hospitalized patients. UFH’s pharmacokinetic profile is complicated by its affinity to bind to multiple plasma proteins (other than antithrombin) and receptors on endothelial cells and macrophages, which leads to a rapid saturable mechanism of clearance via depolymerization. Its clearance is further complicated by a second, slower first-order mechanism that is renally dependent. Pharmacokinetic studies have demonstrated that with increasing UFH doses, its clearance through the rapid saturable mechanism is nonlinear, leading to a disproportionate rise in drug accumulation and increased half-life. These factors lead to an unpredictable anticoagulant response.7,9 When UFH’s nonlinear pharmacokinetic profile is combined with the added complexity of altered pharmacokinetic parameters in obese patients, an optimal dosing strategy to ensure safety and efficacy in this patient population is difficult to determine.
It has come into question whether standard UFH doses used for VTE prophylaxis adequately protect the obese population or if higher doses, such as 7500 units every 8 hours, are warranted given UFH’s unique pharmacokinetic considerations and higher VTE risk of this patient population. 8 Literature evaluating the safety and efficacy of a higher UFH dosing strategy has mainly been assessed in the bariatric surgery population. These studies suggest efficacy of higher UFH doses for reducing the risk of VTE.10,11 However, studies addressing the safety and efficacy of higher doses in the general hospitalized obese patient population are limited, and their findings are inconsistent with interpretation complicated by notable limitations, such as unmeasured confounding.12-14 In addition, the findings from a recent retrospective cohort study conducted by Patanwala et al 15 suggests that standard UFH dosing with 5000 units every 8 hours may provide adequate protection against VTE in the obese hospitalized patient population, adding to the uncertainty of the appropriateness of a higher dose regimen in this patient population. In the setting of unclear and inconsistent evidence, clinicians are challenged with extrapolating data for UFH use for chemoprophylaxis in the obese patient population. This should be done with caution until the balance between the risks and benefits are elucidated.
The objective of this study is to evaluate the safety of the use of 7500 units every 8 hours (high-dose) of subcutaneous UFH for thromboprophylaxis in obese patients in order to offer guidance on the appropriate use of UFH in this patient population.
Methods
Study Design and Participant Selection
This was a retrospective cohort study of patients admitted to a large urban academic medical center in New York City. The inclusion criteria were adult patients (18 years or older) admitted to the medical center between September 1, 2015, and September 1, 2018, who weighed >100 kg on admission. Patients with a BMI <30 kg/m2 and those with incomplete documentation (ie, any missing data points) were excluded. Patients were categorized based on UFH dosing received for at least 48 hours. The study group was defined as patients who received 7500 units of subcutaneous UFH every 8 hours (high-dose group). The control group was defined as patients who received 5000 units of subcutaneous UFH every 8 hours (standard-dose group). Patient reports were generated using a data mining tool, Clinical Looking Glass (Emerging Health Information Technology, Yonkers, NY). The study protocol was approved by the institutional review board, with a waiver of informed consent.
Outcomes
The primary outcome was the incidence of bleeding during hospitalization. Bleeding was defined as a ≥2-g/dL fall in hemoglobin level or receipt of transfusion of 2 or more units of packed red blood cells (pRBCs) within the admission period starting from the initiation of the UFH order. The secondary outcomes included incidence of a ≥2-g/dL fall in hemoglobin level, receipt of transfusion of 2 or more units of pRBCs, and incidence of VTE (as defined by ICD-10 codes) that occurred within the admission period starting from the initiation of the UFH order.
Statistical Analysis
A sample of 200 patients in each study group was needed to provide at least 80% power to detect a 5% difference in bleeding at a 2-sided α level of 0.05. This power analysis is based on an expected incidence rate of 38% for the high-dose group and an incidence rate of 25% for the standard-dose group, based on a previous study conducted on this subject. 5 Categorical variables were analyzed using the χ2 test or Fisher exact test. Logistic regression was conducted to adjust the primary end point for the most likely confounders and covariates. Investigator expertise was used to identify potential confounders, defined as variables that are likely to influence both therapy selection and outcome of interest. Given our access to the electronic medical record data, we chose not to use any automatic confounder identification methods (eg, P value cutoffs) because of a lack of evidence for their superiority over expert knowledge alone. 16 The a priori identified confounding variables included intensive care unit admission, malignancy, surgery, Charlson Comorbidity Index with age, BMI, concomitant aspirin use, length of stay, and the All Patient-Refined Diagnosis-Related Groups severity-of-illness categories. 17 A 2-tailed test of statistical significance set at P <0.05 was used for the statistical analyses.
Results
A total of 343 patients were screened for inclusion in the study. Of these patients, 7 were excluded because of incomplete documentation, and 10 were excluded for a BMI <30 kg/m2. All excluded patients were from the standard-dose UFH group, except 1 high-dose patient with incomplete documentation. A total of 162 patients in the high-dose group and 164 patients in the standard-dose group were included in the study analysis (Figure 1). Patient demographics and baseline characteristics are described in Table 1. Significantly more patients in the high-dose UFH group were female and had a lower baseline hemoglobin, longer length of stay, higher severity of illness, and a higher BMI at baseline, with a majority belonging to obese class III. It should be noted that there was no baseline difference in concomitant aspirin use or surgery type, including bariatric surgery (Table 1).
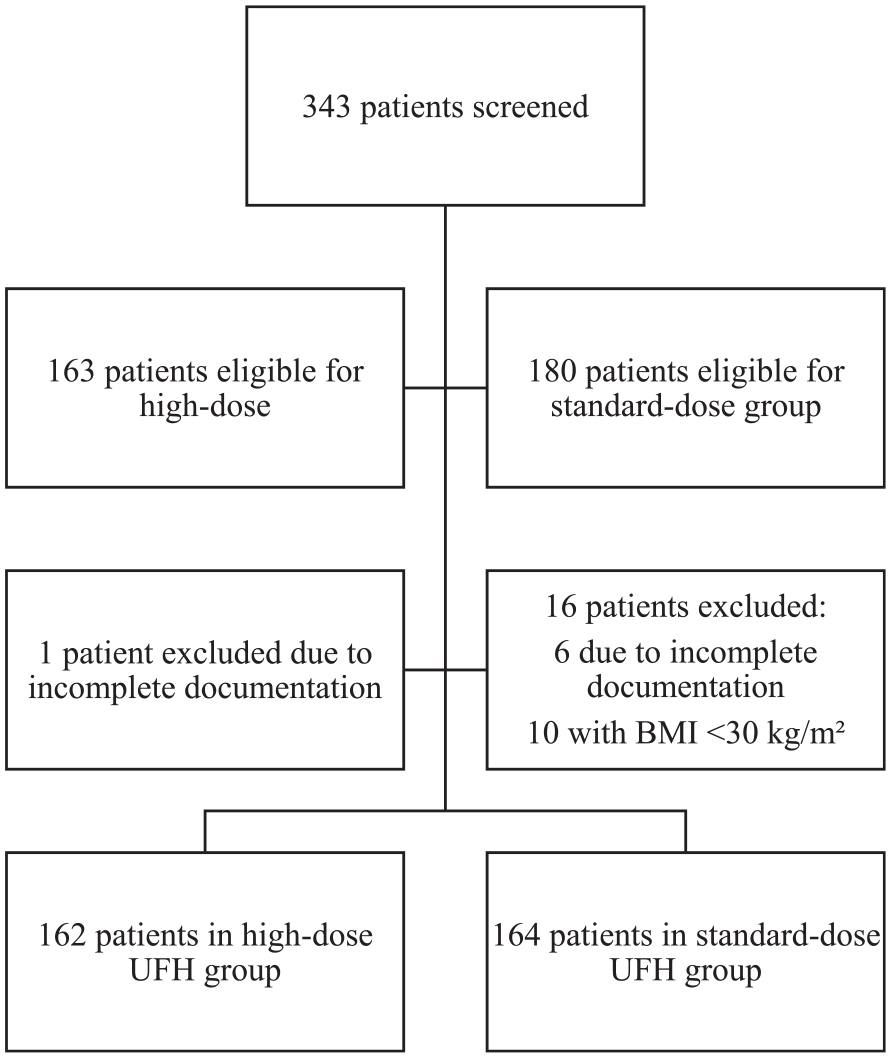
Participant selection.
Baseline Characteristics. a
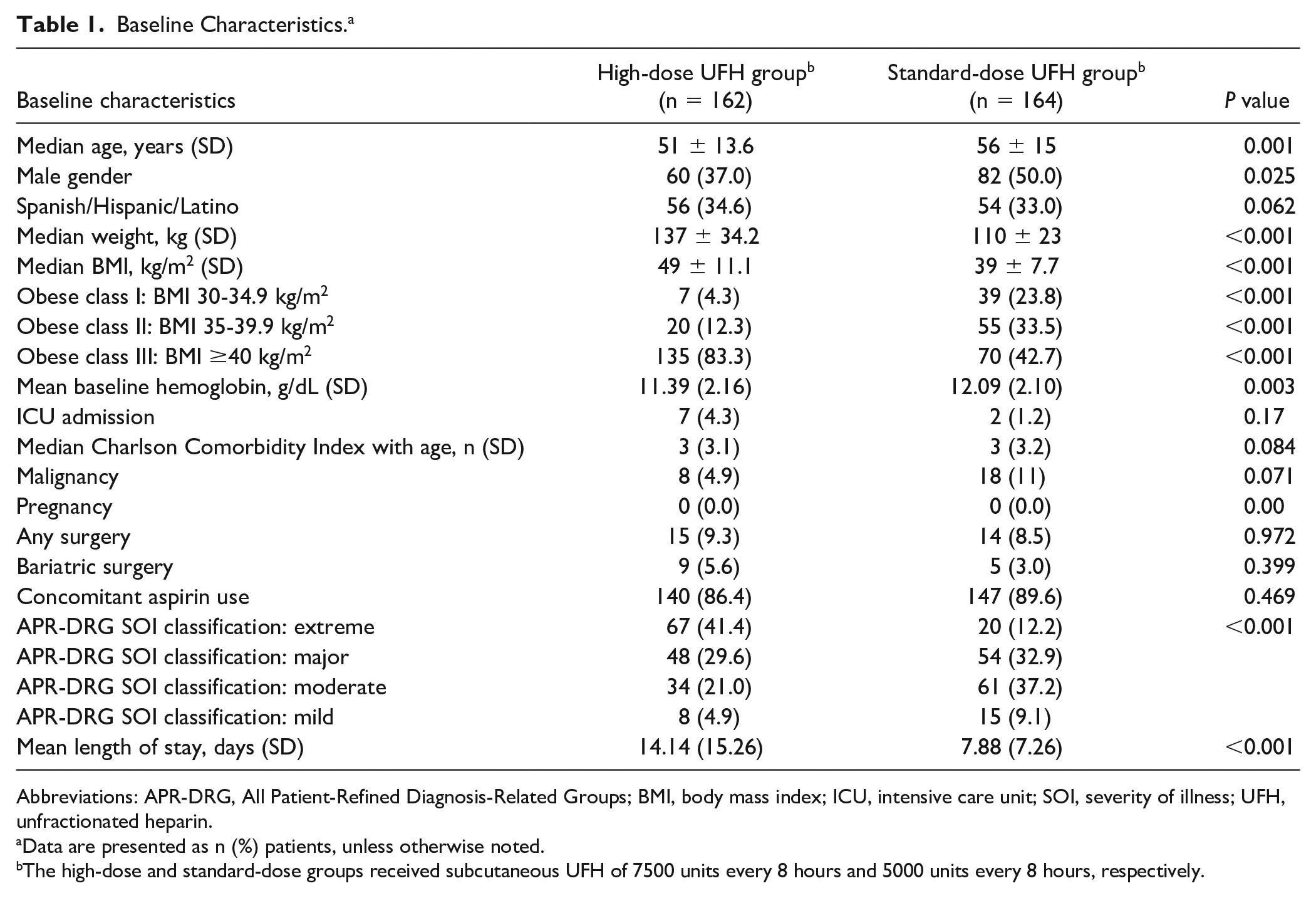
Abbreviations: APR-DRG, All Patient-Refined Diagnosis-Related Groups; BMI, body mass index; ICU, intensive care unit; SOI, severity of illness; UFH, unfractionated heparin.
Data are presented as n (%) patients, unless otherwise noted.
The high-dose and standard-dose groups received subcutaneous UFH of 7500 units every 8 hours and 5000 units every 8 hours, respectively.
For the primary end point, the high-dose and standard-dose groups received subcutaneous UFH 7500 units every 8 hours and 5000 units every 8 hours, respectively. The incidence of bleeding was significantly higher in the high-dose UFH group at 43% compared with the standard-dose UFH group at 29% (risk ratio = 1.49, 95% CI = 1.1-2.0, P = 0.008; Table 2). After adjusting for potential confounders, this difference remained significant (adjusted odds ratio = 1.89, 95% CI = 1.01-3.61; Table 3). Obese class III was noted to have a significantly protective effect against bleed risk (odds ratio = 0.32, 95% CI = 0.14-0.70; Table 3). However, when the primary end point was subcategorized by obesity class, high-dose UFH was found to have the strongest association with bleeding risk in obesity class III (odds ratio = 3.58; 95% CI = 1.78-7.74) as compared with the other 2 classes (Table 4).
Overall Incidence of Outcomes. a
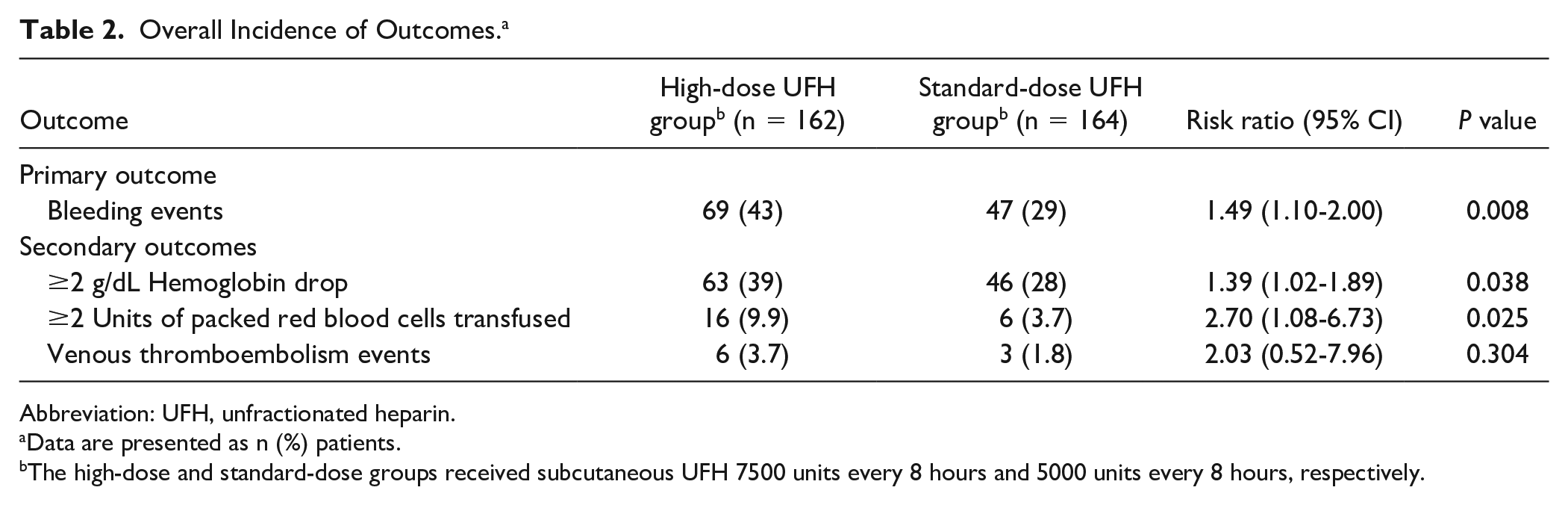
Abbreviation: UFH, unfractionated heparin.
Data are presented as n (%) patients.
The high-dose and standard-dose groups received subcutaneous UFH 7500 units every 8 hours and 5000 units every 8 hours, respectively.
Results of the Multivariable Regression Analysis.
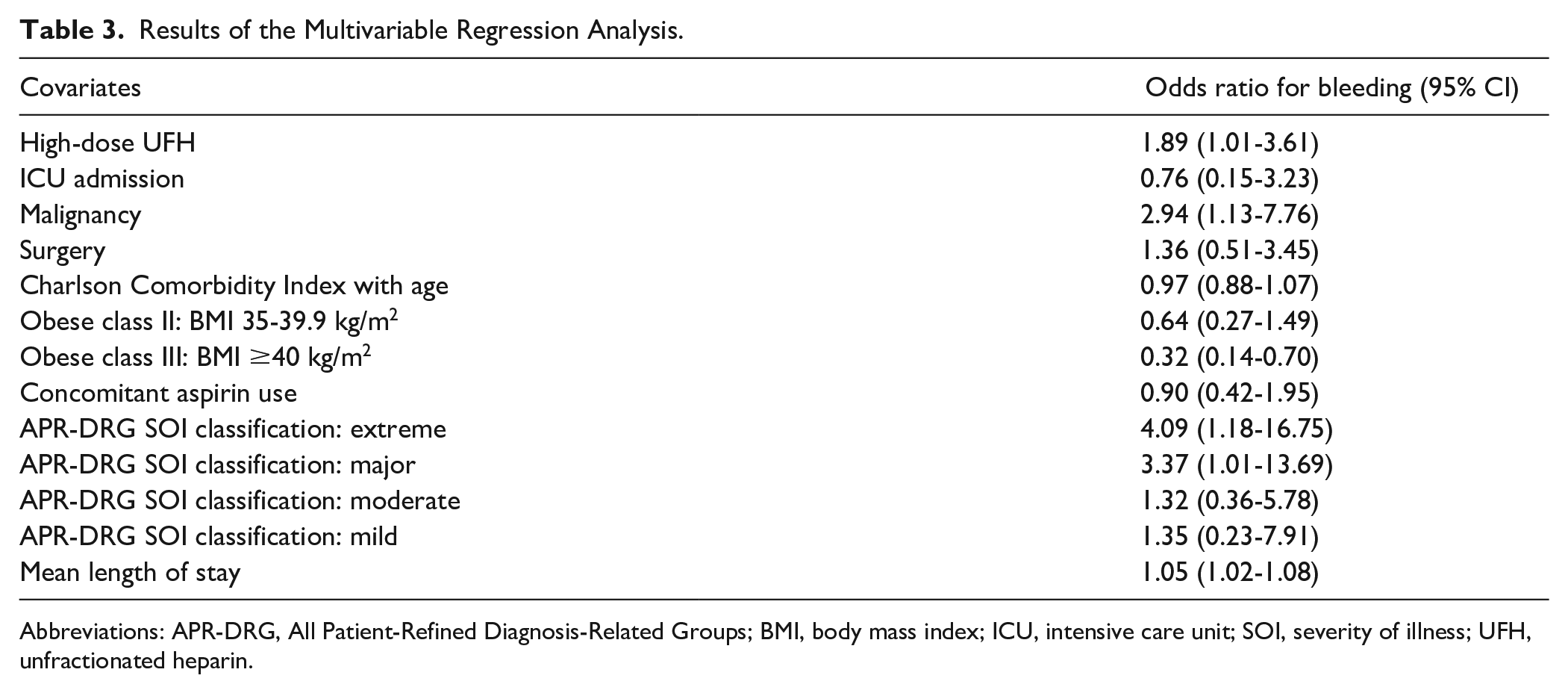
Abbreviations: APR-DRG, All Patient-Refined Diagnosis-Related Groups; BMI, body mass index; ICU, intensive care unit; SOI, severity of illness; UFH, unfractionated heparin.
Bleeding Events Subcategorized by BMI.

Abbreviation: BMI, body mass index.
For the safety secondary end points, the incidence of a ≥2-g/dL fall in hemoglobin level and receipt of transfusion of 2 or more units of pRBCs were higher in the high-dose UFH group compared with the standard-dose UFH group (39% and 9.9% vs 28% and 3.7%, respectively). For the efficacy secondary end point, no significant difference was found for VTE during the admission in the high-dose group compared with the standard-dose group (3.7% and 1.8%, respectively; Table 2).
Discussion
As the incidence of obesity continues to grow in society, the challenge of making ambiguous anticoagulant dosing decisions will continue, unless more, well-defined research is conducted. This study aims to provide more defined guidance on the most appropriate UFH dosing for VTE prophylaxis in obese patients. The findings of this study demonstrate that prophylactic subcutaneous UFH dosed 7500 units every 8 hours in patients with a BMI of 30 kg/m2 or greater led to a significantly higher incidence of bleeding compared with subcutaneous UFH dosed 5000 units every 8 hours (risk ratio = 1.49; 95% CI = 1.1-2.0; P = 0.008), with a risk difference of 13.9% (95% CI = 3.6-24.2) and number needed to harm to cause 1 bleeding event of 7.
Our study provides more clarity on the safety of higher-dose UFH regimens in light of inconsistent and unclear findings in previous studies. Wang et al 13 published a retrospective cohort study that analyzed the incidence of bleeding in 3928 morbidly obese medical and surgical inpatients (weight > 100 kg; BMI ≥ 40 kg/m2) who received high-dose thromboprophylaxis with UFH (7500 units 3 times daily) or enoxaparin (40 mg twice daily) compared with standard dosing. The incidence of bleeding in the high-dose thromboprophylaxis group did not significantly differ from that in the standard-dose thromboprophylaxis group (7.18% vs 8.44%; P = 0.15). 13 Although the study provided valuable insight into high-dose thromboprophylaxis strategies in obese patients, the lack of separate analysis of UFH and enoxaparin groups makes it unclear whether the findings are applicable to individual therapies. Furthermore, bleeding events were identified only by ICD-9 codes, which have been demonstrated to have questionable sensitivity and specificity rates without a confirmation via chart review. 18 Additionally, ICD-9 codes are recorded for the entire admission event without temporal relation to initiation of UFH therapy, making it difficult to attribute bleeding events to choice of thromboprophylaxis. 18
Another retrospective cohort study conducted by Samuel et al 14 assessed the occurrence of major bleeding in 398 neurocritical patients weighing >100 kg, who received either 7500 units every 8 hours or 5000 units every 8 hours of UFH subcutaneously. No significant difference in major hemorrhage was observed between groups. However, the study population was limited to neurocritical obese patients, which limits the generalizability of their findings, and incidence rates were compared with historical controls. 14 Furthermore, a follow-up study from the same institution by Joy et al 12 that included 1335 overweight or obese inpatients demonstrated an increased incidence of bleeding in patients who received the UFH regimen of 7500 units every 8 hours. This inconsistency in findings within the same institution raises concerns as to whether the increased bleeding rate may be a result of type I error in secondary findings or unmeasured confounding. The study showed a higher use of antiplatelet and aspirin use in the obese class III group who received the high-dose UFH regimen, which the findings were not adjusted for. 12
Our study aimed to replicate the design and outcomes of the Joy et al 12 study while adjusting for any clinically meaningful covariates that meet the definition of potential confounders. The consistency of our findings with those of Joy et al suggest that the higher bleeding rates found in obese patients on the high-dose UFH regimen likely represents a true signal and requires further exploration. Furthermore, we sought to improve on limitations of previous studies to strengthen our findings. We used minimal exclusion criteria to make our findings more generalizable to obese inpatients; we focused on transfusion and hemoglobin drop-defined bleeding to overcome the inaccuracies of diagnostic coding; and we used logistic regression analyses to ensure that our findings are not driven by some of the most common confounders, such as aspirin use.
Nevertheless, our study is subject to important limitations. First, incidence rates of bleeding were higher than expected. The definition of bleeding was based on hemoglobin drop and receipt of transfusion, which did not follow the full criteria for major bleeding set forth by the International Society on Thrombosis and Haemostasis (ISTH). The bleeding events that occurred in this study were mainly driven by hemoglobin drop. This definition may capture more minor bleeding as opposed to clinically relevant, major bleeding. A definition that would offer greater sensitivity for bleeding rather than specificity for major bleeding was chosen because a small sample size was being studied. Information on the specific types of bleeds that patients may have experienced were unable to be collected at the time of data collection, so we could not determine if symptomatic bleeding occurred in a critical site or organ per the ISTH definition. 19
Our study findings are mainly applicable to the medical obese patient population, because the study sample only included a small number of surgical patients. Our study sample also included some significant differences in baseline, which represent the differential selection process for higher-dose UFH therapy. For example, patients with higher BMI categories were much more likely to be initiated on high-dose UFH than those in lower categories. To overcome this limitation in our data, we have adjusted our primary findings for baseline differences, which we identified as most likely confounders (variables that influence therapy selection and bleeding risk). Nevertheless, there is always a possibility of unmeasured confounding that we could not account for in our adjusted analysis, and thus, these findings should be interpreted with the same caution that we would apply to any nonrandomized study.
In addition, the initially proposed sample size to meet power was not reached; therefore, any findings that did not achieve statistical significance should be interpreted with caution. Despite a smaller sample size, a difference between both groups was detected for the primary outcome, which was likely driven by a larger than predicted effect size. This study was also not powered to detect a difference in VTE rates, so no conclusion can be drawn based on our findings regarding the difference in VTE rates between high-dose and standard-dose UFH regimens. Given these limitations, a decision not to use high-dose UFH cannot be made without a larger study assessing this risk versus benefit ratio.
An unexpected finding in our study was the seemingly protective effect of obesity on bleeding risk. Patients with BMI ≥40 kg/m2 demonstrated a significantly lower risk of bleeding than other BMI classes, independent of other risk factors and therapy selection. Furthermore, there appears to be a linear relationship between obesity class and bleeding risk. Interestingly, this relationship has been well described in the surgical literature, where patients in higher obesity classes are at a lower risk of blood loss and require less perioperative transfusions (sometimes deemed the “obesity paradox”).20,21 The proposed explanations include the increased procoagulant factors in obese patients (the same ones responsible for higher VTE risk), larger blood volumes reducing the risk of hemodilution, and adipose tissue providing compression of minor bleeding sites. 22 We believe that these explanations could be extrapolated to our general inpatient population. Conversely, when our primary end point is stratified by obesity class, the odds ratios of bleeding risk appear to be higher with increasing BMI categories, consistent with the findings in the Joy et al 12 study. Given the wide CIs and consistently elevated bleeding risk across all BMI categories, we cannot make much of this finding without a larger study to assess this variation.
Conclusion and Relevance
This study demonstrated that high-dose UFH (7500 units every 8 hours) was associated with an increased bleeding event rate compared with standard-dose UFH (5000 units every 8 hours) in patients with a BMI ≥30 kg/m2. This raises safety concerns about the appropriateness of utilizing high-dose UFH for VTE prophylaxis in the obese patient population. In the absence of strong evidence of benefit from higher-dose UFH regimens, caution should be exercised before utilizing this regimen in clinical practice until further studies clarify the balance between bleeding and thrombosis in this patient population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.