
Abstract
Objective:
To review the incidence, management, and current understanding of the pathophysiology of β-lactam–induced neutropenia and to critically evaluate the practicality and safety of direct substitution to an alternative β-lactam in the setting of this reaction.
Data Sources:
A literature analysis using the PubMed and Ovid search engines (July 1968 to October 2020) was performed using the search terms neutropenia, leukopenia, β-lactam, nonchemotherapy, agranulocytosis, and G-CSF (granulocyte colony-stimulating factor).
Study Selection and Data Extraction:
The included English-language studies evaluated the incidence, mechanism, and/or management of β-lactam–induced neutropenia in pediatric or adult patients.
Data Synthesis:
Drug-induced neutropenia is a well-documented adverse reaction of β-lactam antibiotics, with an incidence of approximately 10% following at least 2 weeks of intravenous therapy. However, multiple gaps in knowledge remain in the mechanism of pathophysiology and optimal management of this reaction. Both direct toxic and immune-mediated mechanisms have been implicated. Although the cornerstone of management includes cessation of the offending agent, controversy exists on the appropriateness of direct substitution or future use of an alternative β-lactam.
Relevance to Patient Care and Clinical Practice:
Given the frequency of use and superiority of β-lactams over alternative therapy for several infectious disease states, practical recommendations are needed on the management and safe use of β-lactams following β-lactam–induced neutropenia.
Conclusion:
Future use of β-lactams with differing R1 side chains, particularly those from a separate class, should not be deemed contraindicated following β-lactam–induced neutropenia and may be considered when indicated, with close laboratory monitoring.
Introduction
β-Lactam–induced neutropenia is a well-described adverse reaction of this group of antimicrobials and often progresses to agranulocytosis (absolute neutrophil count [ANC] < 0.1 × 103/µL) without intervention. The reaction is most often described in the setting of intravenous β-lactam courses lasting greater than 2 weeks, with an incidence rate commonly reported at approximately 10% for patients meeting these criteria.1-7 Given the frequency of use and preference of β-lactams over alternative agents for several infectious disease states, a practical understanding of the incidence and management of β-lactam–induced neutropenia is invaluable for clinicians in all treatment settings. Although drug-induced neutropenia has been described with virtually all β-lactams in clinical practice, there appears to be a higher incidence with particular agents such as penicillin G, nafcillin, oxacillin, piperacillin-tazobactam, ceftriaxone, and ceftaroline.1,2,5,6,8,9 Neutropenia in the setting of orally administered, short β-lactam treatment courses (<10 days) is exceedingly rare. 3
Leading theories on the mechanism of β-lactam–induced neutropenia involve a direct toxic effect, an immunologic reaction that involves hypersensitivity or antibody destruction, or a combination of the two. Cumulative β-lactam dose appears to be an important factor, suggesting that the reaction may be triggered by accumulation of toxic metabolites.3,4,10-20
Primary management of β-lactam–induced neutropenia involves discontinuation of the offending agent. To expedite resolution of neutropenia, the use of granulocyte-colony stimulating factor (G-CSF) has been advocated, particularly for those with poor prognosis.6,21-24
Despite the abundance of research on β-lactam–induced neutropenia, gaps in knowledge continue to persist in the mechanism of pathophysiology and optimal management. When additional antimicrobial therapy is indicated, controversy exists over the safety of a direct substitution to an alternative β-lactam in the setting of this reaction. Although several early reports indicate success with this strategy,10,12,25-28 it has been discouraged in other cases describing relapse of neutropenia following rechallenge.7,29-31 The present report reviews the incidence, management, and current understanding of the mechanism of β-lactam–induced neutropenia and discusses the practicality and evidence for a direct switch to an alternative β-lactam class with low cross-reactivity.
Data Sources
A literature search was performed using the PubMed and Ovid search engines for the MEDLINE database. Search terms included neutropenia, leukopenia, β-lactam, nonchemotherapy, agranulocytosis, and G-CSF. The search included only studies in English, and the years of publication ranged from 1968 to 2020. Publications were assessed for relevance prior to inclusion. Studies evaluating the safety and/or efficacy of β-lactams for the indication of febrile neutropenia were excluded.
Results
Incidence and Characteristics
First reported more than 50 years ago, β-lactam–induced neutropenia is a well-documented adverse reaction associated with this family of antimicrobials. This reaction most often presents after approximately 2 to 3 weeks of parenteral therapy and with an associated incidence ranging widely from 2.2% to 34% with courses lasting greater than 10 to 14 days. Laboratory thresholds for neutropenia in published reports are inconsistent, varying in ANC from <0.5 to <2.0 × 103/µL and occasionally unreported.1-7 Often with β-lactam–induced neutropenia, additional associated laboratory abnormalities are present—namely, eosinophilia and/or thrombocytopenia. 1 Symptomatic manifestations such as febrile episodes and rash are also present in approximately a quarter to half of cases.1,3,4 Agranulocytosis generally presents more seriously and may result in severe sepsis or even septic shock, with risk of mortality.21,22
A summary of characteristics of β-lactam–induced neutropenia for several commonly used parenteral agents from the penicillins, cephems, and penem classes is represented in Table 1. The literature supporting these findings is highly heterogeneous, comprising case reports, case series, retrospective observational studies, systematic reviews, and controlled trials. Limitations in the data include variations in laboratory definitions, populations studied, dosing strategies, durations of therapy, and publication bias. Therefore, the authors urge caution with direct comparisons of drug-induced neutropenia characteristics between agents. Orally administered β-lactams were excluded from this review because drug-induced neutropenia associated with these agents is remarkably rare.
Summary of Reports on β-Lactam–Induced Neutropenia for Select Agents.
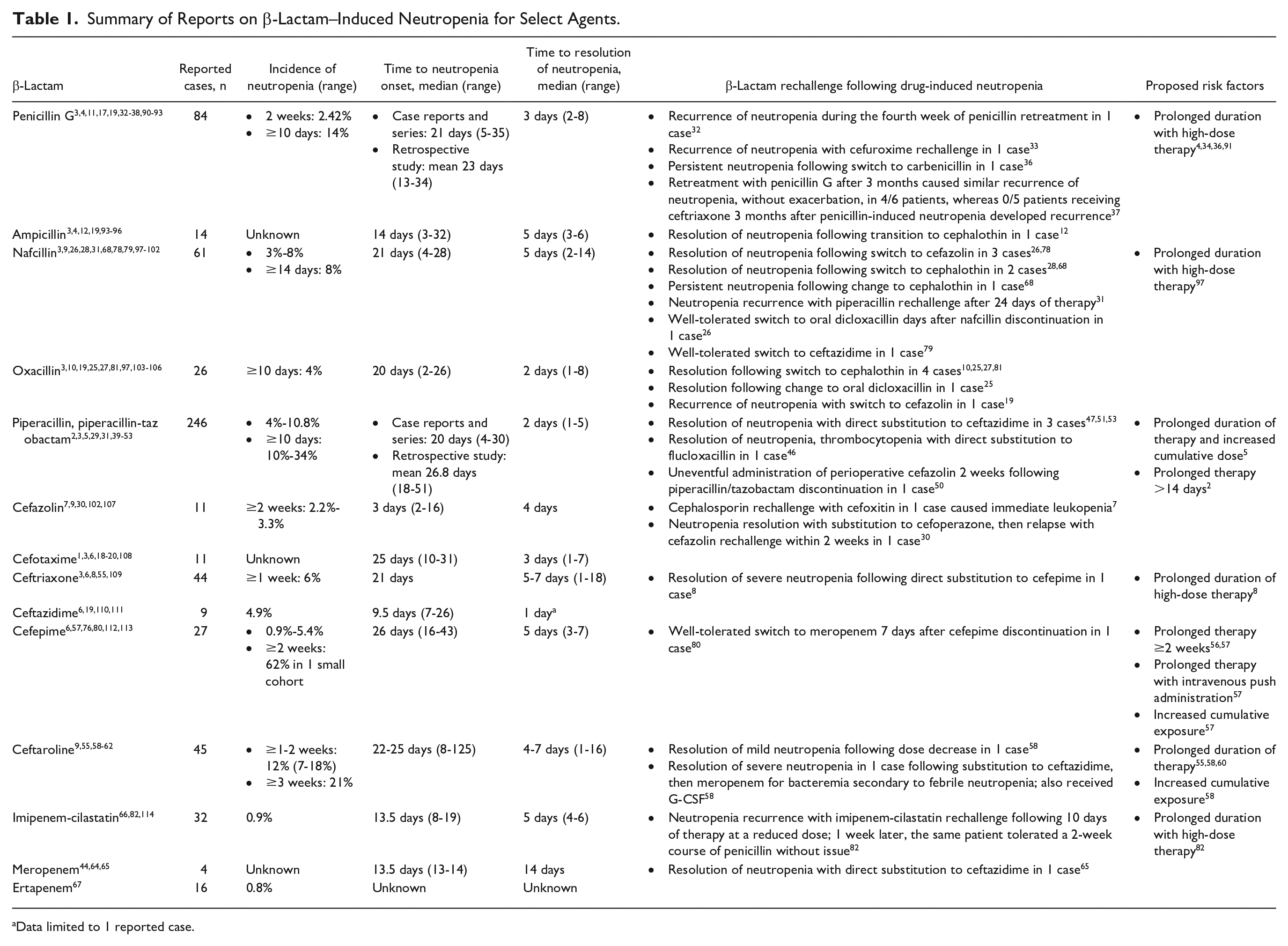
Data limited to 1 reported case.
A plethora of clinical experience exists with drug-induced neutropenia associated with the penicillins class of β-lactams, which includes penicillin G and other subclasses, including aminopenicillins, ureidopenicillins, carboxypenicillins, and the penicillinase-stable penicillins. The incidence of drug-induced neutropenia with penicillin G has been reported to be as high as 14% with durations of therapy exceeding 10 days. 4 The dosing strategies used in these studies is highly variable, with daily doses generally ranging from 8 to 32 million units and up to 100 million units in 1 case series.3,4,11,17,19,32-38 An association between an increased daily dose and the development of drug-induced neutropenia does appear to be evident for penicillin G in particular. In a prospective study of patients treated with β-lactam antibiotics for the indication of endocarditis, neutropenia was significantly more likely in patients receiving high-dose penicillin G (35%) as compared with a low-dose treatment strategy (8%), with no patient developing neutropenia prior to day 17 of parenteral β-lactam therapy. The mean daily dose of penicillin G in the high-dose cohort was 28.2 million units compared with 19.3 million units in the low-dose group. 4 These data support the findings from a compilation of early cases, which observed an association between penicillin-induced neutropenia and daily doses in excess of 150 mg/kg (250 050 U/kg, or 17.5 million units of penicillin G for a 70-kg patient), which is easily achievable when using the full licensed doses of parenteral penicillins for most nonobese patients.1,3
Piperacillin, a member of the ureidopenicillin subclass, has been implicated in β-lactam–induced neutropenia more often than any other agent, with 246 cases.2,3,5,29,31,39-53 Cases involving piperacillin or piperacillin-tazobactam were included in this count. Notably, a systematic review of piperacillin or piperacillin-tazobactam–induced neutropenia identified 183 cases using the Food and Drug Administration Adverse Event Reporting System. 40 Studies assessing piperacillin-tazobactam and other β-lactams for the indication of febrile neutropenia were excluded from the literature review, given the clear presence of confounders.
The incidence of piperacillin-induced neutropenia varies from 10% to 34% in studies assessing a minimum duration of 10 days of therapy.5,39 However, the exceptionally high incidence of 34% is limited by the retrospective nature of the corresponding study, which included a small cohort of patients treated for osteomyelitis and used a conservative threshold of <2.0 × 103/µL for neutropenia. 5 Piperacillin-induced neutropenia in adults treated with shorter courses is rare. A pooled safety analysis of 22 clinical trials, including 1585 patients treated with piperacillin-tazobactam, uncovered no cases of bone marrow toxicity in patients treated for less than 10 days.43,54 Direct comparisons with other β-lactams are sparse, with 1 exception being a retrospective study of pediatric patients demonstrating a 10.8% incidence of drug-induced neutropenia with piperacillin-tazobactam compared with 2.6% with ticarcillin-clavulanate despite median treatment durations of approximately 6 days in each group. 2 The most common adult daily dose of piperacillin-tazobactam reported in the cases of drug-induced neutropenia was 13.5 g, and at this time, there is no clear evidence of a dose-dependent effect.40,41,43,46,49-51
Drug-induced neutropenia is well reported with the cephalosporins, a subclass of the cephems class of β-lactams. The incidence of ceftriaxone-induced neutropenia in 1 retrospective cohort study was 6%, with durations of therapy equaling or exceeding 7 days. 55 A recent literature summary of ceftriaxone-induced neutropenia demonstrated a mean time to neutropenia of 23 days, a mean time to recovery of 6.5 days, and a mean ANC nadir of 0.1 × 103/µL. 8 The vast majority of cases of ceftriaxone-induced neutropenia have reported a daily dose of 2 g.3,8,55
Regarding cefepime, 1 study identified a 62% incidence (8/13) of cefepime-induced neutropenia, with extended courses using a dose of 2 g every 12 hours, with an average neutropenia onset of 25 days. However, this was a low-volume cohort limited exclusively to patients with osteomyelitis. 56 Interestingly, 1 recent study found that patients experiencing cefepime-induced neutropenia were 3 times as likely to have received cefepime by intravenous push as opposed to standard infusion. 57
Ceftaroline, despite having arguably less clinical experience relative to other agents in this review, has amassed a considerable amount of attention for its propensity to cause neutropenia with extended courses of therapy.9,55,58-62 The reported incidence of ceftaroline-induced neutropenia following 1 to 2 weeks of therapy varies from 7% to 18% and increases to 21% with 3 weeks of therapy.9,55,58,60,62 In 1 large cohort study evaluating characteristics of drug-induced neutropenia following 2 weeks of therapy, the incidence of neutropenia with ceftaroline was found to be 17%, compared with only 2% for cefazolin. The study, which included ceftaroline, cefazolin, and nafcillin, did not find any evidence of a dose-dependent effect on the development of neutropenia. 9 The most common dosing strategy utilized in reported cases of ceftaroline-induced neutropenia was 600 mg every 12 hours, followed by the off-label dose of 600 mg every 8 hours.55,58-62
Reports of neutropenia are sparse with the carbapenems, a subclass of the penems class of β-lactams, possibly owing to their reserved indication for use, lack of prolonged use, and/or low immunogenicity.6,63-65 A pooled safety analysis of 3470 patients treated with imipenem-cilastatin in clinical trials demonstrated a 0.9% incidence of neutropenia, which dropped to 0.3% when limited to cases that were probably or definitely drug induced. 66 Similarly, a pooled safety analysis of patients treated with ertapenem in phase II/III controlled trials demonstrated a 0.8% incidence of drug-related neutropenia, with no patient requiring treatment discontinuation. 67 However, a minority of patients in these studies received a duration of therapy exceeding 14 days. The median duration of ertapenem therapy was 4 days and 6 days in studies comparing ertapenem with ceftriaxone and piperacillin-tazobactam, respectively. 67
Pathogenesis
Mechanisms on the pathophysiology of β-lactam–induced neutropenia have been proposed and like other causes of drug-induced neutropenia involve both a direct toxic effect inhibiting granulopoiesis and an immunologic reaction involving drug-induced or drug-dependent antibodies.3,4,8,10-19,68,69 Genetic variation causing predisposition to drug-induced neutropenia has been described and may play a role by increasing risk of a reaction to a specific agent.70,71
A recent review of drug-induced agranulocytosis concluded that the available evidence supports an immune-mediated mechanism as the primary pathogenesis. 71 Specific findings from case series involving β-lactams include drug-dependent antineutrophil antibodies and leukocyte agglutination, possibly induced by accumulation of reactive metabolites over several days of therapy.4,14-16,18,19,69 IgG and/or IgM antibodies have been theorized to be involved in this reaction.4,18,69 Findings from other studies demonstrate evidence of marrow toxicity, suggesting a heterogeneous nature of this reaction.3,13,20 A literature review that summarizes the proposed mechanisms of β-lactam–induced neutropenia is shown in Table 2.
Literature Review of β-Lactam–Induced Neutropenia and Agranulocytosis With Regard to Proposed Mechanism.
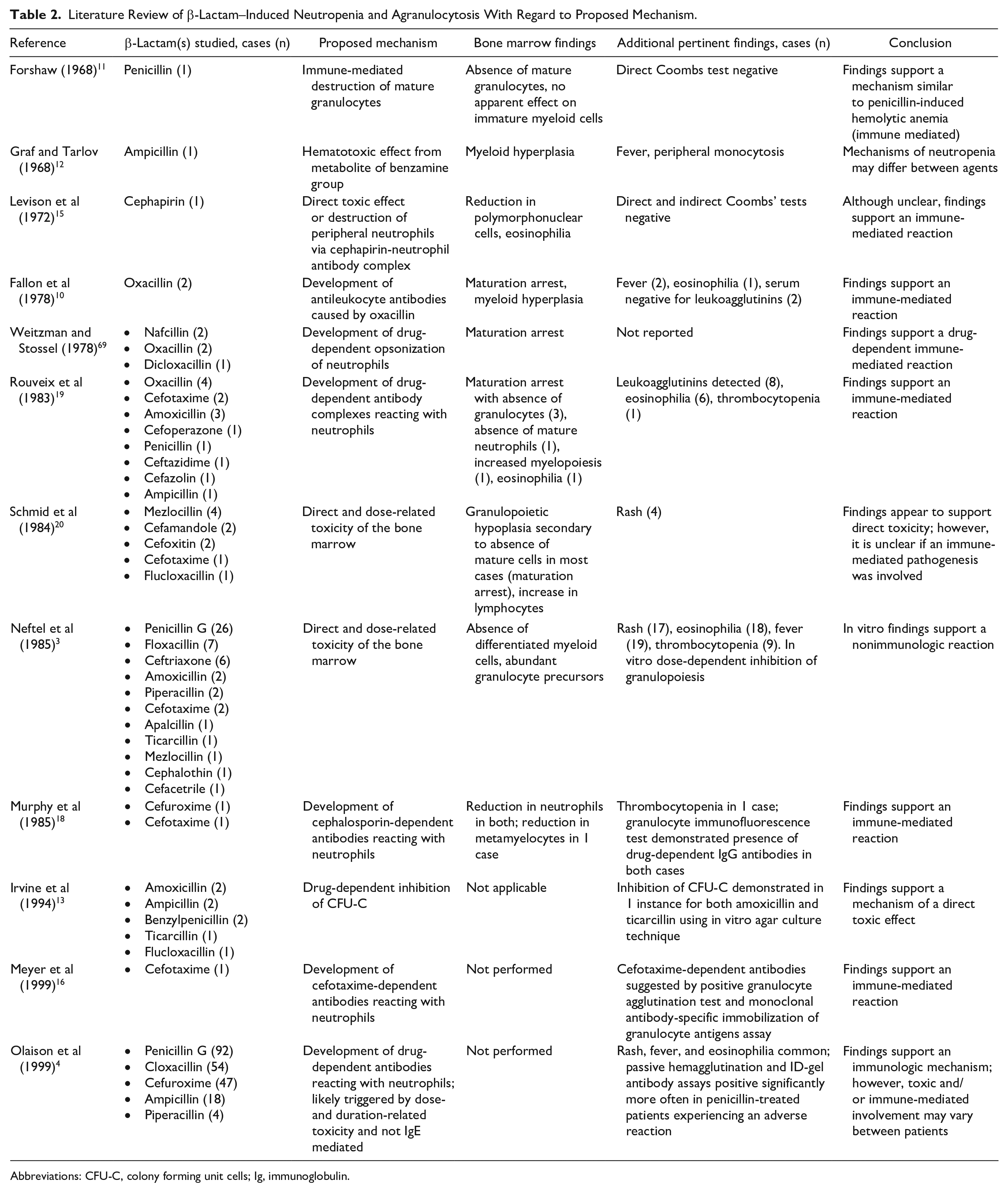
Abbreviations: CFU-C, colony forming unit cells; Ig, immunoglobulin.
Bone marrow studies generally reveal granulopoietic hypoplasia, secondary to the presence of immature granulocyte precursors, and apparent myeloid maturation arrest, presumably as a result of antibody-mediated destruction of mature myeloid cells.1,8,10,12,20,68 Drug-induced neutropenia with a more rapid onset and resolution (<2 days) suggests peripheral neutrophil destruction by antineutrophil antibodies, whereas delayed resolution (2-7 days or longer) may indicate the presence of marrow toxicity and maturation arrest. Protracted recovery (14 days) may represent depletion of myeloid precursors. 72 However, the differences between these reactions are not completely understood and often not distinct. The median time to neutropenia recovery following treatment discontinuation for the β-lactams presented in this report fell within the 2- to 7-day range. Unfortunately, no validated tools exist to predict time to recovery.
The proposed mechanism of β-lactam–induced neutropenia appears to be distinct from other types of drug-induced agranulocytosis. In the case of thionamide antithyroid drugs, antineutrophil cytoplasmic antibodies against antigens on the surface of neutrophils have been found, and T-cell responses to oxidative metabolites may also play a role.70,71,73 Class I HLA alleles such as HLA-B*27:05 in European populations and HLA-B*38:02 in Asian populations have also been associated with thionamide agranulocytosis.70,71,73 HLA associations have also been described with agranulocytosis associated with other drugs such as HLA-B*27:05 and levamisole as well as HLA-B38, DR4, and DQw3 with clozapine-induced agranulocytosis in Ashkenazi Jewish populations.74,75
At this time, a detailed and thorough understanding of the mechanisms underlying β-lactam–induced neutropenia remains elusive, and no relevant HLA class I or II associations have been defined.
Cross-reactivity of β-Lactams Following Drug-Induced Neutropenia
The substitution to an alternative β-lactam following drug-induced neutropenia has been debated and remains controversial. Several early reports of penicillin-induced neutropenia, and even agranulocytosis, have demonstrated success with resolution of neutropenia with direct substitution to an alternative β-lactam and have advocated for this practice. Detailed investigation reveals that the overwhelming majority of these cases involved regimen modification to an agent in a different β-lactam class—namely, the cephems, which includes the cephalosporins subclass. Several instances of penicillin-, nafcillin-, and oxacillin-induced neutropenia have been successfully managed with substitution to cephalosporin therapy, often cefazolin or cephalothin.10,12,25-28,68
More recently, the strategy of substitution to an alternative β-lactam, within the same class or otherwise, in the setting of this reaction has come under scrutiny. 7 The incidence of neutropenia recurrence following β-lactam reexposure has been noted to be 15% to 30%, but this statistic includes the rechallenge of the same β-lactam in several instances and is also dependent on the dose and duration of therapy used during rechallenge of an alternative β-lactam.3,19,30,76 In 1 retrospective study of patients treated with 10 to 14 days of penicillin G for neurosyphilis, 4 of 6 patients rechallenged with penicillin G 3 months after the initial episode of drug-induced neutropenia developed a recurrence of neutropenia with similar pattern of onset and severity. 37 In addition, many reports describing relapse of neutropenia following substitution of an alternative β-lactam involved agents with structural similarities and relatively higher risk of cross-reactivity. Published regimen changes resulting in neutropenia relapse include substitution to β-lactam agents within the same class but with differing R1 groups such as cefazolin to cefoxitin, 7 nafcillin to piperacillin, 31 methicillin to ampicillin, 77 and mezlocillin to piperacillin. 29 Relapse in neutropenia following change to an alternative β-lactam class is unusual but was demonstrated with penicillin G to cefuroxime in 1 case 33 and from oxacillin to cefazolin or cephalothin in others.19,68
A recent descriptive study using patient information from the French Pharmacovigilance Database provides evidence for the relative safety and practicality of switching to an alternative β-lactam with low cross-reactivity risk in the setting of drug-induced neutropenia. 6 In this study, only 2 of 21 (9.5%) patients experienced neutropenia recurrence following rechallenge of an alternative β-lactam. Interestingly, 5 of these patients who did not experience neutropenia recurrence were rechallenged with agents from the same class. The authors did not comment on the implicated agents for the 2 patients experiencing recurrence. 6 Furthermore, it is unclear what the time period was, if any, between β-lactam re-exposures. These findings are in agreement with the pooled data from case reports and case series presented in this report. Following β-lactam–induced neutropenia, only 3 of 27 (11%) patients experienced persistence or recurrence of neutropenia following substitution to or future rechallenge with a β-lactam from a separate class.10,12,19,25-28,33,37,47,50,51,53,58,65,68,78-82
Cross-reactivity between β-lactams can occur through either the β-lactam ring itself, the class-specific ring, or side chains. The R1 side chain comes off the β-lactam ring, and penicillins only have the 1 side chain. The R2 group defining other β-lactams, including agents from the cephalosporin and carbapenem subclasses, comes off the class-specific ring. An illustration of β-lactam structures indicating the presence and location of R group side chains is depicted in Figure 1. In certain instances, the R1 side chain is shared between agents from separate β-lactam classes. Amoxicillin shares an R1 side chain with cefadroxil and cefprozil, whereas ampicillin shares an R1 side chain with cephalexin and cefaclor. Within the cephalosporin subclass, cephalexin and cefaclor share an R1 side chain. In addition, an R1 side chain is shared between ceftriaxone, cefotaxime, cefpodoxime, and cefepime. Cefazolin has no shared R1 side chains with other penicillins or cephalosporins. Important to note is the shared R1 side chain between ceftazidime and the monobactam aztreonam. 63
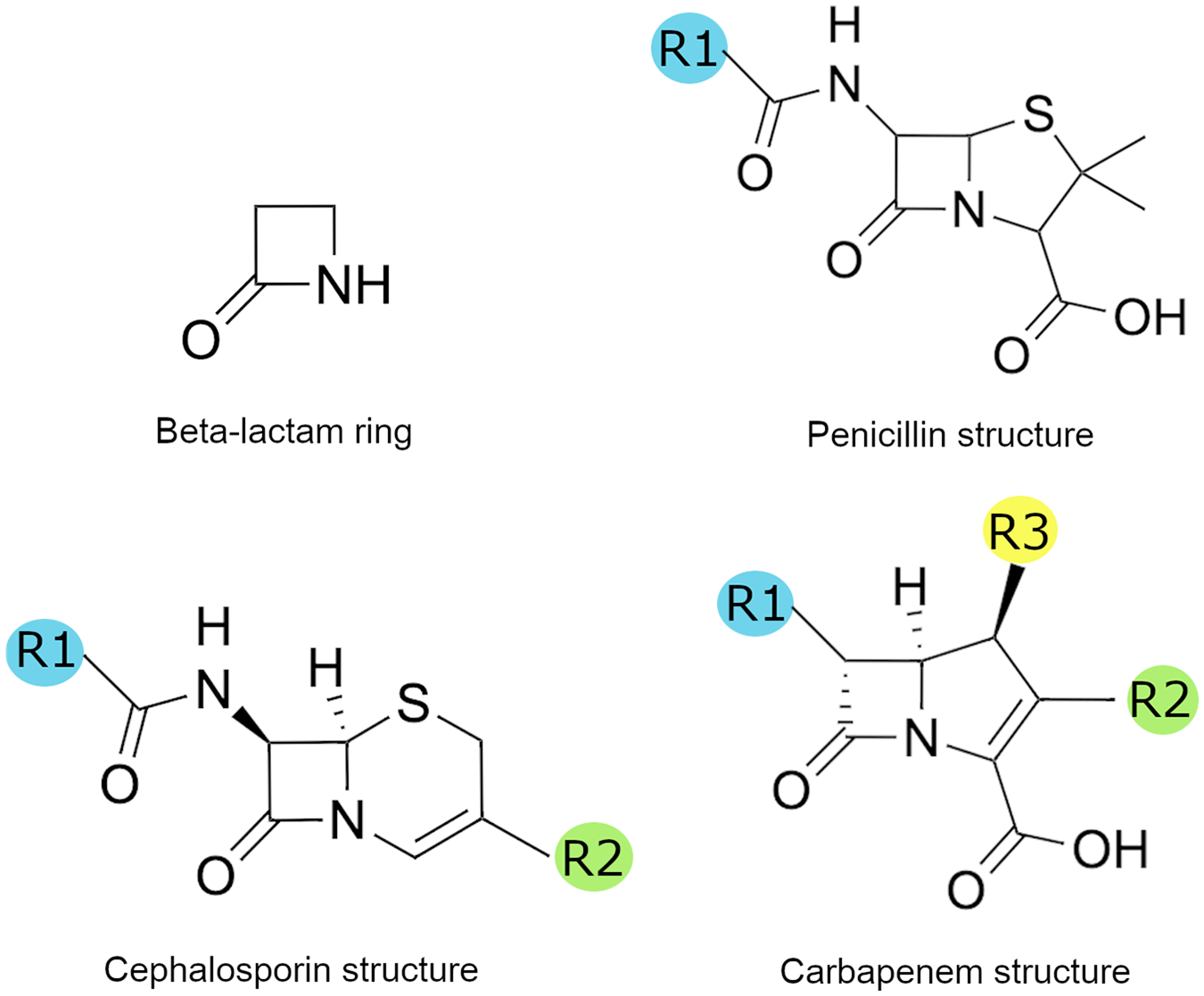
β-Lactam structures indicating the presence and location of R-group side chains.
Current literature on cross-reactivity rates between β-lactam classes suggests a <1% risk of cross-reactivity between carbapenems and both cephalosporins and penicillins, lower than the rate for cross-reactivity between penicillins and cephalosporins at <2%. 63 Although allergic reactions to β-lactams are believed to be mediated largely by side chains, the induction of β-lactam–induced neutropenia by antineutrophil antibodies or a T-cell response to unique side chains remains unproven, however plausible based on what is known on cross-reactivity with other β-lactam hypersensitivity reactions. Thus, it is unclear whether the cross-reactivity rates between β-lactams cited in the literature are applicable in the setting of drug-induced neutropenia. One recent patient case demonstrating resolution of ceftriaxone-induced neutropenia following direct substitution to cefepime implicated the reactive triazinedione group of the ceftriaxone R2 side chain, given the shared R1 side chain and core between ceftriaxone and cefepime. 8
Management of β-Lactam–Induced Neutropenia
The cornerstone of management for β-lactam–induced neutropenia is prompt withdrawal of the offending agent and close monitoring of blood counts to assess for resolution. Diagnosis can be challenging, particularly in the presence of confounding clinical scenarios with bone marrow–suppressive potential such as malignancy, sepsis, or the receipt of cytotoxic medications. β-Lactam discontinuation should be strongly considered once the ANC is <1.0 × 103/µL. 68 Drug-induced agranulocytosis, a drop in neutrophils <0.1 × 103/µL, is a medical emergency and is occasionally fatal. Prognosis has improved in recent years with earlier detection and improved management for those presenting with suspected sepsis or septic shock.6,21-23,83 Outpatients should be instructed to immediately seek medical attention in the setting of febrile neutropenia.
Monitoring for the development of β-lactam–induced neutropenia is particularly important in the setting of outpatient parenteral antimicrobial therapy (OPAT), given the frequency of prolonged treatment courses and decentralization of patient care in the outpatient setting. National guidelines recommend routine laboratory monitoring for patients receiving OPAT, including but not limited to a weekly complete blood count with differential for patients receiving β-lactam therapy. 84 However, insufficient data are available to inform the optimal frequency of laboratory monitoring for specific laboratory tests. Thus, patients at higher risk, such as those with low baseline or downtrending counts, may require more frequent monitoring.
If further antimicrobial therapy is required following β-lactam–induced neutropenia, an alternative antimicrobial with low or absent risk of cross-reactivity should be selected. Based on the collection of data in the present literature review, this may include substitution to a β-lactam from a separate class. Specific care should be taken to evaluate the patient’s current medication list for alternative potential causes of neutropenia. Other medications implicated in drug-induced neutropenia include clozapine, methimazole, propylthiouracil, procainamide, hydroxyurea, and several others.69,71,85 Concurrent use of vancomycin poses a particular challenge because vancomycin-induced neutropenia is implicated in 2% to 12% of extended courses. 86 If additional medications confounding the diagnosis of β-lactam–induced neutropenia are present, all such agents may need to be withdrawn depending on the clinical context. Alternatively, if close clinical and laboratory monitoring are feasible and neutropenia is mild in severity, agents may be discontinued sequentially beginning with the most likely culprit in an attempt to minimize medication changes.
The use of G-CSF has been recommended as an adjunct in the setting of β-lactam–induced neutropenia to expedite neutrophil recovery. Limited data have demonstrated an association between G-CSF and a shorter duration of neutropenia, although this effect has not been consistently shown and requires validation in randomized controlled trials.6,21-23,87,88 A review of case reports was able to demonstrate a modest decrease in neutropenia duration caused by nonchemotherapy agents with the use of G-CSF, from a median 9 to 8 days. 22 Despite this, its use should be considered in patients with poor prognosis. Such prognostic factors include ANC <1.0 × 103/µL, age >65 years, presence of bacteremia and/or septic shock, and renal failure.21-23,87 In a systematic review of agranulocytosis caused by nonchemotherapy agents, patients with an ANC nadir <1.0 × 103/µL who were treated with G-CSF had a lower rate of infectious or fatal complications (22%) compared with those who did not receive G-CSF (46%). 22
Relevance to Patient Care and Clinical Practice
Drug-induced neutropenia is a well-reported adverse event associated with β-lactams, with an elevated incidence of approximately 10% in the setting of prolonged parenteral therapy exceeding 10 to 14 days. Untreated, this reaction may progress to agranulocytosis, which is a medical emergency and carries a case-fatality rate of <5% to 10%.21,22
Given the frequency of β-lactam use, practical recommendations on the management of drug-induced neutropenia and safe use of β-lactams following this reaction are critical, particularly in the setting of OPAT, where extended durations of therapy are commonly used. Several clinical and logistical factors must be considered, and knowledge of the general trends in time to onset and resolution of β-lactam–induced neutropenia can serve as a tool to help guide treatment and monitoring decisions, including the use of adjunctive G-CSF to decrease the risk of complications associated with agranulocytosis.6,21-23,87,88
Clinical rationale supporting the continuation of β-lactam therapy includes the preference and superiority of this family of antibiotics for several infectious disease states, with 1 well-documented example being invasive infections caused by methicillin-susceptible Staphylococcus aureus. 89 Furthermore, commonly used β-lactam alternatives such as vancomycin and fluoroquinolones carry the risk of serious and potentially debilitating adverse events, including the not uncommon occurrence of neutropenia in the case of vancomycin. Following β-lactam–induced neutropenia, the risk of sustained or relapsed neutropenia with substitution to a β-lactam from a separate class appears to be low at approximately 10% based on the available case reports.10,12,19,25-28,33,37,47,50,51,53,58,65,68,78-82 Thus, this strategy can serve as a useful and viable option when close laboratory monitoring is feasible and the benefits of continued β-lactam therapy outweigh the risks.
Conclusion
Drug-induced neutropenia is a well-documented reaction associated with β-lactams, with an associated incidence of approximately 10% following 10 to 14 days of parenteral therapy. Although several theories have been proposed, the predominant pathogenesis appears to involve an immune-mediated reaction. Primary management includes cessation of the offending agent(s), and G-CSF may be considered for patients with poorer prognosis. In the setting of penicillin or cephalosporin-induced neutropenia, the available evidence supports the practicality of substitution to a β-lactam with a differing R1 side chain, particularly one from a separate class, when clinical benefits of β-lactam therapy outweigh the low but potential risk of sustained neutropenia. Although rechallenge with the offending agent or a drug that shares an R1 side chain would not be routinely recommended, future use of β-lactams should not be considered contraindicated and may be utilized with caution, particularly with short courses and close laboratory monitoring.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare no competing interests. EJP reports grants from National Institutes of Health (P50GM115305, R01HG010863, R01AI152183, R21AI139021, U01AI154659) and from the National Health and Medical Research Council of Australia. She receives Royalties from Uptodate and consulting fees from Biocryst. She is codirector of IIID Pty Ltd that holds a patent for HLA-B*57:01 testing for abacavir hypersensitivity and holds a patent for Detection of Human Leukocyte Antigen-A*32:01 in connection with Diagnosing Drug Reaction with Eosinophilia and Systemic Symptoms without any financial remuneration and not directly related to the submitted work. Funders played no role in any aspect of this review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.