
Abstract
Background
Earlier trials on the efficacy of poly (ADP-ribose) polymerase (PARP) inhibitors in platinum-sensitive relapsed ovarian cancer used the hazard ratio (HR) as an efficacy parameter.
Objective
The present meta-analysis was focused on improving the robustness and clinical interpretability of the efficacy evaluation of PARP inhibitors using the restricted mean survival time (RMST).
Methods
A search for relevant studies published up to July 31, 2020, was performed in electronic databases to identify eligible trials comparing PARP inhibitors with placebo. The difference in RMST was used as a PARP inhibitor efficacy parameter. Combined differences in RMST with 95% CIs across studies were calculated using a random-effects model.
Results
Four trials (6 articles) were assessed, including 1079 patients treated with PARP inhibitors and 598 with placebo. The combined RMST differences for up to 360 days (PARP inhibitors minus placebo: point estimate and 95% CI) among all patients and the patients of subgroups with BRCA mutations, homologous recombination-deficient (HRD) carcinoma, and BRCA wild-type carcinoma were 87 days (95% CI = 71, 102), 112 days (95% CI = 96, 129), 99 days (95% CI = 80, 119), and 69 days (95% CI = 47, 92), respectively. The combined RMST differences for up to 660 and 720 days were also larger among patients with BRCA mutations than among those with HRD carcinoma.
Conclusion and Relevance
Based on using the RMST difference as an alternative measure to the HR, this meta-analysis suggests that PARP inhibitors are the most effective for patients with BRCA mutations, followed by patients with HRD carcinoma.
Introduction
Ovarian cancer, which is frequently not diagnosed until it reaches an advanced stage, is associated with the highest fatality rate among gynecological cancers.1,2 Ovarian cancer treatment has traditionally been a combination of chemotherapy and surgery, primarily including hysterectomy and bilateral salpingo-oophorectomy, staging, cytoreduction, and subsequent chemotherapy. 1 However, most patients developed recurrence, with a median progression-free survival (PFS) time of 18 months after standard primary treatment in a 2012 study. 3 Although there is an urgent need for effective treatments to improve the prognosis in ovarian cancer, 4 poly (ADP-ribose) polymerase (PARP) inhibitors developed in 2014 offer some hope for an improvement in PFS.
PARP inhibitors are relatively new medications for ovarian cancer that target the ability of a cell to repair DNA. 5 PARP1 and PARP2 function in base-excision repair triggered by DNA single-strand breaks occurring in normal cells. Blocking these proteins by PARP inhibitors leads to the accumulation of single-strand breaks, causing DNA double-strand breaks and cytotoxicity. 5 BRCA1/2 are 2 key tumor suppressors involved in the repair of DNA double-strand breaks via homologous recombination, one of the DNA repair mechanisms. 4 Homologous recombination deficiency (HRD) is the state that has an abnormality in homologous recombination and is caused by various factors. A germline mutation in these genes is the most common clinical cause of HRD, and PARP inhibitors can induce synthetic lethality in BRCA mutant tumor cells.4,5 Olaparib is the world’s first PARP inhibitor, and it received initial approval in 2014 as maintenance treatment of BRCA1/2-mutated ovarian cancer, based on the results from Study 19.6-8 This study, which was conducted in patients with platinum-sensitive relapsed, high-grade serous ovarian cancer, demonstrated that PFS is significantly longer with olaparib than with placebo (median 8.4 months vs 4.8 months from randomization on completion of chemotherapy; hazard ratio [HR] for progression or death = 0.35 [95% CI = 0.25, 0.49]). 8 After the initial assessment, the approval was expanded to all platinum-sensitive patients, regardless of BRCA1/2 status, and the utility of PARP inhibitors is expected to expand further in the years ahead.7,9 The efficacy of niraparib and rucaparib for ovarian cancer was also confirmed in NOVA and ARIEL3, respectively.10,11
In earlier trials conducted in patients with platinum-sensitive relapsed ovarian cancer on PARP inhibitors, the HR was used as a measure to evaluate the efficacy of PARP inhibitors. The HR is a common model-based measure of the difference between groups for a time-to-event outcome. However, it is not easy to assess the efficacy based on the estimated HR owing to several limitations, such as the lack of a reference value for the hazard from a placebo group to evaluate the difference between groups and the difficulty in interpreting the estimated HR if the proportional hazards assumption, which assumes that the HR is constant over time, is violated.12-15 The restricted mean survival time (RMST) has been recently proposed as an alternative measure for a time-to-event outcome because of its robustness and clinical interpretability.16-19 The RMST represents the expected time spent event-free for a future patient followed for a specified period (τ). The difference in RMST has characteristics not associated with the HR, such as the existence of a reference value for the RMST from a reference group to assess the difference in RMST between groups and independence from any model assumption. We may gain new insights and a better understanding of the efficacy of PARP inhibitors in patients with ovarian cancer if RMST is utilized as an alternative measure to the HR for evaluating their efficacy as maintenance therapy in platinum-sensitive recurrent ovarian cancer.
Hence, the aims of this study were to examine the efficacy of PARP inhibitors in patients with platinum-sensitive relapsed ovarian cancer and determine the length of the extended progression-free period, compared with a reference treatment, when using the difference in RMST. This study also reconfirmed the previously reported results based on HR by using the difference in RMST as an alternative approach to the HR for measuring the efficacy.
Methods
This meta-analysis included all randomized controlled trials in patients with platinum-sensitive relapsed ovarian cancer, comparing the efficacy of PARP inhibitors as maintenance therapy with placebo. Trials were excluded if they did not report the results of PFS or used combinations of PARP inhibitors with chemotherapy. The duration of PFS is generally defined as the time from treatment randomization to the earliest date of disease progression or death from any cause. The main objective of this meta-analysis was to assess the efficacy of PARP inhibitors as maintenance therapy in patients with platinum-sensitive recurrent ovarian cancer using the difference in RMST as a measure for the time-to-event outcome. It is still rare that studies report the RMST estimates, requiring individual-level time-to-event data for calculating RMST values and their standard error. However, it was difficult and impractical to obtain original individual participant data from each clinical trial. Therefore, individual-level time-to-event data for each outcome in every trial was reconstructed using an algorithm developed by Guyot et al 20 to estimate the RMST. The information required for this algorithm includes the observed Kaplan-Meier curves, number of patients at risk at several time points, and observed number of events. Therefore, the trials that had sufficient information for the reconstruction of individual-level data were included, as described above. The necessary information for the reconstruction was obtained from the main articles in the included trials and related publications if necessary. The adequacy of the reconstructed data was assessed by checking whether the Kaplan-Meier curves drawn from the reconstructed data were visually identical to the originally published curves.
A literature search for articles published up to July 31, 2020, was performed in MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials. The search terms were ovarian cancer, ovarian carcinoma, relapsed, recurrent, platinum sensitive, maintenance therapy, and maintenance treatment. No review protocol was published. The Cochrane risk of bias assessment tool was used to assess the risk of methodological quality within the included studies. 21
The RMSTs with 95% CIs were estimated for PARP inhibitors and placebo regarding the PFS of study population subgroups, such as the BRCA mutational status, up to the maximum study follow-up time reported with the corresponding information of the number of patients at risk. Inferences were made about the RMST differences between PARP inhibitors and placebo with 95% CIs for each study. To estimate the combined value in the meta-analysis, among the studies assessed in the meta-analysis, the shortest study follow-up time that was reported with the corresponding information of the number of patients at risk was used as the common time point for calculating the RMSTs with 95% CIs for PARP inhibitors and placebo, and their difference. To assess the effect of using a common time point on the results, another meta-analysis, using a different time point as the reference, was conducted. To account for heterogeneity among the studies, a random-effects model was used to calculate the combined difference in RMST with 95% CIs across studies for each outcome. Statistical heterogeneity was assessed using the I2 statistic, 22 considering I2 <25% as low and I2 >75% as high heterogeneity. Publication bias was visually assessed by the funnel plot.
The present meta-analysis was reported following the PRISMA checklist. 23 Analyses were performed on an intention-to-treat basis. A P <0.05 (2-sided) was considered statistically significant. All analyses were performed using R software, version 3.4.0. 24
Results
The trial flow is summarized in Figure 1, identifying 6 articles (4 trials) available for inclusion in this meta-analysis.8-11,25,26 The summary of the 4 trials—Study 19,8,9 SOLO2, 25 NOVA,10,26 and ARIEL3 11 —included in this meta-analysis is displayed in Table 1. The analysis included 1079 patients treated with PARP inhibitors and 598 patients treated with placebo. The risk of bias in the included studies was low (Appendix A, available online), and statistical heterogeneity was not observed based on the I2 value (Figure 2; Appendices B and C, available online). The funnel plot suggested no major publication bias (data not shown).
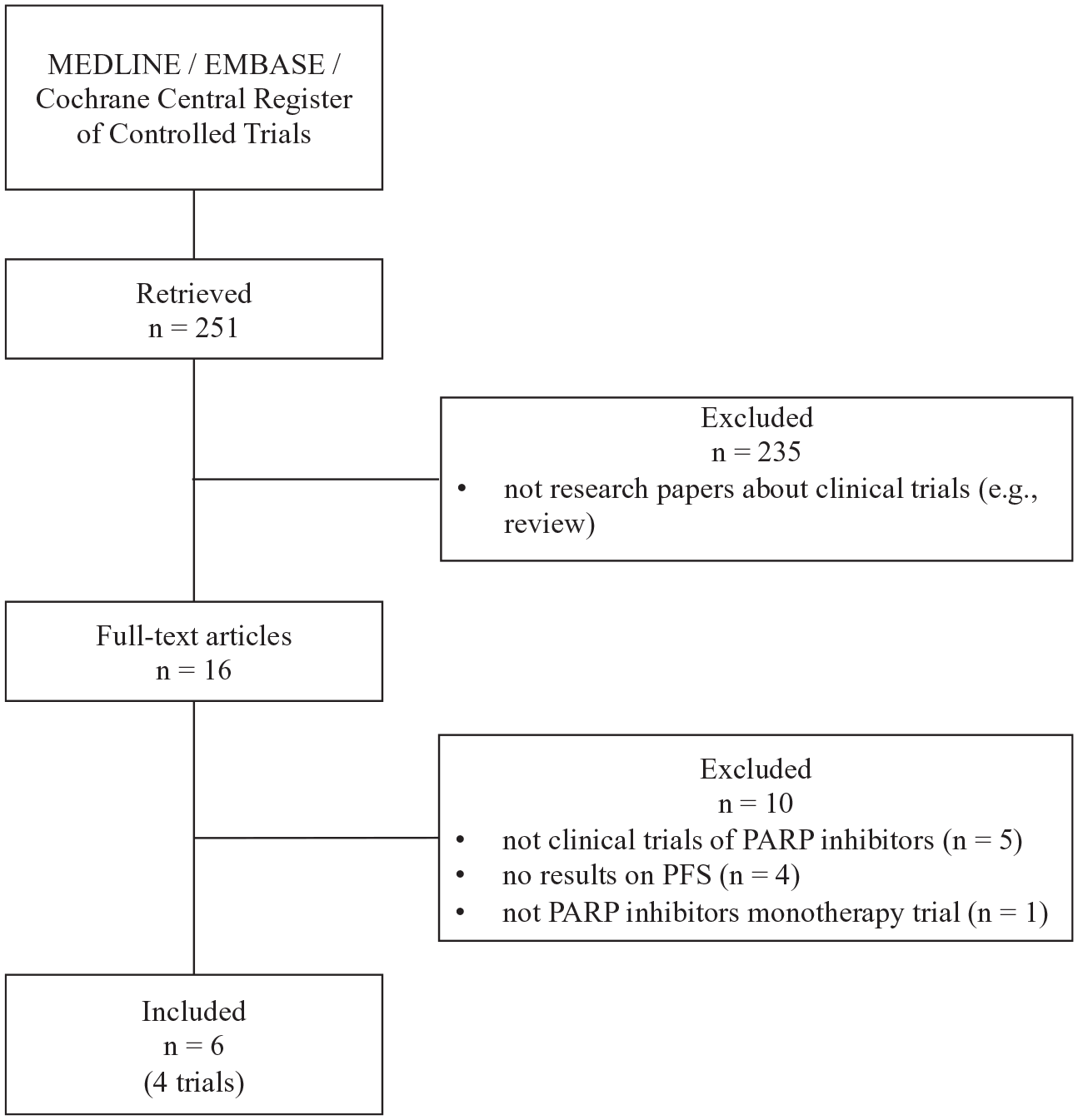
Flow diagram of study selection.
Summary of 4 Clinical Trials Included in the Present Meta-analysis.

Abbreviations: ECOG, Eastern Cooperative Oncology Group; HRD, homologous recombination-deficient; ITT, intention-to-treat.
ITT population.
Patients with BRCA mutation and those with BRCA wild-type carcinoma were evaluated in preplanned retrospective analysis of data from Study 19.
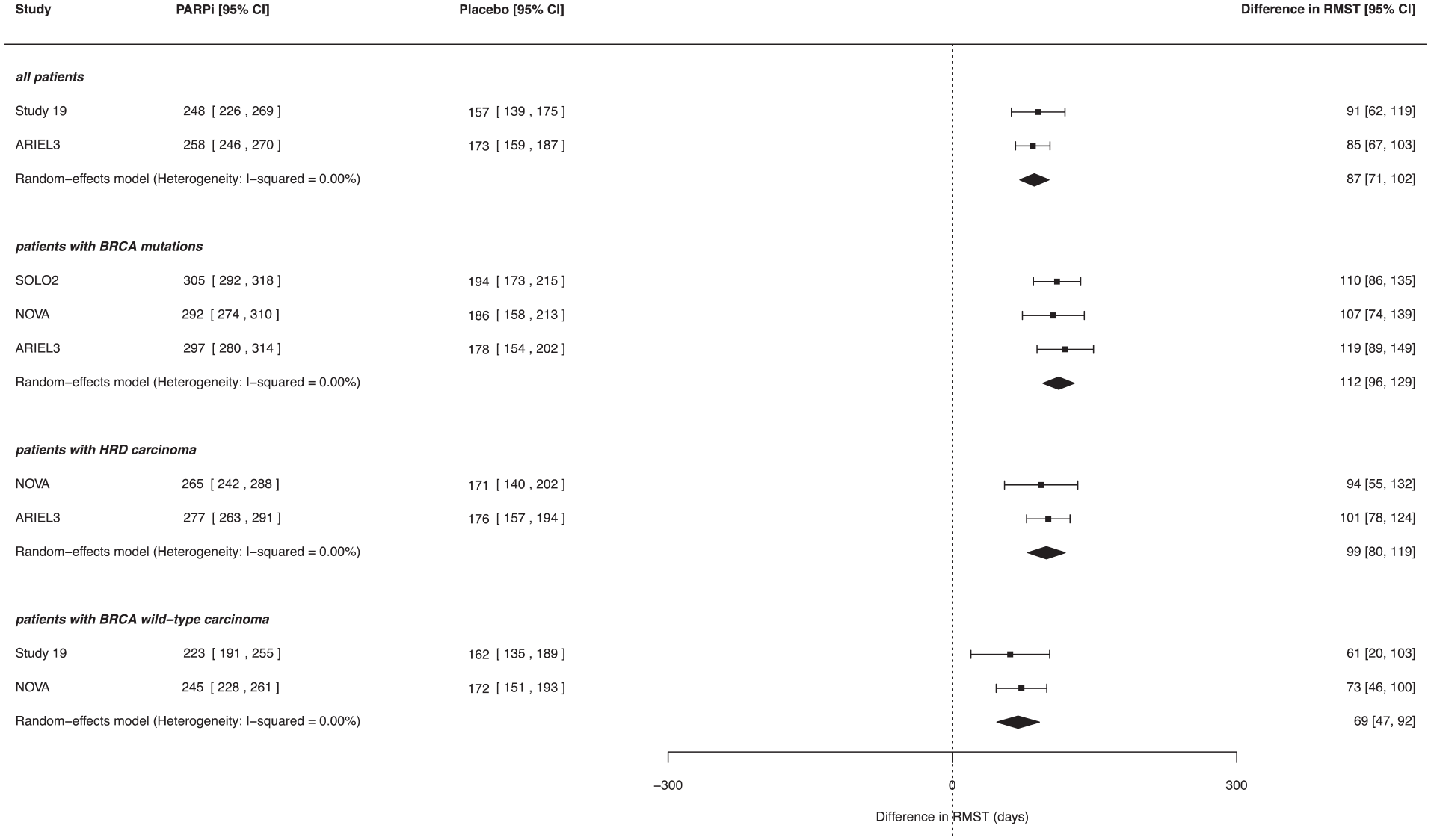
Forest plot of the difference in RMST for progression-free survival by the subgroup of the study population (τ = 360 days).
The RMST results for each arm of the trials and the RMST differences (PARP inhibitors minus placebo) for PFS are shown in Table 2. The τ value of each study population was based on the maximum study follow-up time reported with the corresponding information of the number of patients at risk. The olaparib analysis revealed the following. In Study 19, the RMSTs for all patients regardless of BRCA status were 223 days (95% CI = 207, 240) in the olaparib group and 150 days (95% CI = 135, 166) in the placebo group, resulting in an RMST difference of 73 days (95% CI = 50, 95). This RMST difference and 95% CI indicated that, on average, future patients treated with olaparib for 300 days are expected to have 73 more days free of events of disease progression or death than the patients receiving placebo. The RMST differences among patients with mutated BRCA were 100 days (95% CI = 72, 129; 243 days [95% CI = 223, 264] with olaparib vs 143 days [95% CI = 123, 163] with placebo; τ = 300 days) in Study 19 and 267 days (95% CI = 204, 331; 534 days [95% CI = 494, 573] with olaparib vs 266 days [95% CI = 217, 316] with placebo; τ = 810 days) in SOLO2. The efficacy of olaparib was also confirmed in patients without mutated BRCA (Table 2). The assessment of the effect of niraparib in NOVA revealed that the RMST difference among patients with a germline BRCA mutation was 216 days (95% CI = 148, 284; 446 days [95% CI = 405, 487] with niraparib vs 230 days [95% CI = 176, 284] with placebo; τ = 660 days). An analysis for patients without a germline BRCA mutation in whom tumors were not found to be HRD also revealed a difference in RMST of 136 days (95% CI = 86, 187) in favor of niraparib (342 days [95% CI = 307, 376] with niraparib vs 205 days [95% CI = 169, 242] with placebo; τ = 660 days). The efficacy of niraparib was also confirmed in patients without a germline BRCA mutation in whom tumors were found to be HRD (Table 2). The analysis for rucaparib in ARIEL3 showed that using this PARP inhibitor in patients with a BRCA mutation was associated with an RMST difference of 262 days (95% CI = 200, 324; 469 days [95% CI = 425, 514] with rucaparib vs 207 days [95% CI = 164, 250] with placebo; τ = 720 days). An analysis for patients with HRD carcinoma determined a rucaparib-associated RMST difference of 223 days (95% CI = 178, 269), in favor of rucaparib (425 days [95% CI = 391, 459] with rucaparib vs 202 days [95% CI = 171, 232] with placebo; τ = 720 days). The efficacy of rucaparib was also confirmed in an ITT population (Table 2).
Results of 4 Clinical Trials Using the Difference in RMST for Progression-Free Survival.

Abbreviations: CR, complete response; HRD, homologous recombination-deficient; ITT, intention-to-treat; LOH, loss of heterozygosity; PARPi, poly (ADP-ribose) polymerase inhibitors; PR, partial response; RMST, restricted mean survival time.
Each τ is the maximum study follow-up time reported with the corresponding information of the number of patients at risk.
Each RMST was estimated up to each corresponding time point, τ.
Among the studies assessed in this meta-analysis, the shortest study follow-up time that was reported with the corresponding information of the number of patients at risk was used as the common time point (τ) in the meta-analysis. The meta-analysis results based on τ =360 days, which was chosen from the assessed trials as the common time point, are shown in Figure 2. The efficacy of PARP inhibitors compared with placebo was confirmed among all patients or those in the subgroups with BRCA mutations, HRD carcinoma, or BRCA wild-type carcinoma. The combined RMST difference was the largest among patients with BRCA mutations, followed by patients with HRD carcinoma (112 days [95% CI = 96, 129] and 99 days [95% CI = 80, 119], respectively). To assess the effect of using a common time point on the results, meta-analyses using different time points (τ = 660, 720 days) were conducted as the reference. The combined RMST difference was also larger in patients with BRCA mutations than in those with HRD carcinoma when τ =660 days was used (228 days [95% CI = 195, 261] and 196 days [95% CI = 159, 233], respectively; Appendix B), and this tendency was still detectable when τ = 720 days was selected (250 days [95% CI = 209, 292] and 213 days [95% CI = 173, 253], respectively; Appendix C).
Discussion
In this meta-analysis, the efficacy of PARP inhibitors in patients with platinum-sensitive relapsed ovarian cancer was evaluated using the difference in RMST as an efficacy measure that represents an alternative approach to the HR used in earlier meta-analyses. Among all patients or those of the subgroups associated with BRCA mutations, HRD carcinoma, or BRCA wild-type carcinoma, the efficacy of PARP inhibitors olaparib, niraparib, and rucaparib was confirmed based on the evaluation up to the chosen time point considering the study follow-up time of each study. The results of this meta-analysis suggested that PARP inhibitors were the most effective in patients with BRCA mutations, followed by patients with HRD carcinoma, all patients, and patients with BRCA wild-type carcinoma.
The systematic review identified 4 trials—Study 198,9 and SOLO2 25 for olaparib, NOVA10,26 for niraparib, and ARIEL3 11 for rucaparib—which were used in this meta-analysis. The efficacy of the PARP inhibitors administered in each trial, which was originally assessed based on HR, was reevaluated using the difference in RMST. Study 19 was a randomized, double-blind, placebo-controlled, phase 2 study to evaluate maintenance treatment with olaparib in platinum-sensitive, relapsed, high-grade serous ovarian cancer. 8 A preplanned retrospective analysis of the outcomes in Study 19 based on the BRCA status showed the efficacy of olaparib compared with placebo in patients with a BRCA mutation (HR = 0.18 [95% CI = 0.10, 0.31]) and with wild-type BRCA (HR = 0.54 [95% CI = 0.34, 0.85]). 9 However, it is not easy to assess treatment efficacy based on the estimated HR because it is not possible to know the hazard of a placebo group as reference value for evaluating the difference between groups. On the contrary, the difference in RMST applied in this study utilizes the reference value from a placebo group to evaluate the difference. This study showed that future patients treated with olaparib for 300 days are expected to be free of events of disease progression or death for a longer period than those receiving placebo. Specifically, treatment with olaparib for 300 days extended the event-free period by an additional 100 and 52 days on average, compared with that of the placebo treatment, based on the reference RMST values of the placebo group of 143 and 155 days, in patients with and without BRCA mutation, respectively. For SOLO2, conducted in patients with BRCA mutation, 25 the results of this study also showed that, on average, future patients treated with olaparib for 810 days are expected to be free of events of disease progression or death for 267 more days than placebo-treated patients, based on an RMST reference value of 266 days for the placebo group. These results will improve our understanding of the efficacy of olaparib in patients with and without a BRCA mutation. According to NOVA using the HR results for PFS, the efficacy of niraparib was confirmed compared with placebo in patients with and without germline BRCA mutations.10,26 The results of the present study, based on the RMST difference, confirmed these observations. The ARIEL3 report indicated the efficacy of rucaparib compared with placebo among patients with mutated BRCA or HRD carcinoma, 11 and these results were also confirmed in this study. The extended event-free period identified by the difference in RMST for the PARP inhibitor group based on a reference value in the placebo group is expected to be used as new clinically meaningful information on the effects of PARP inhibitors.
The combined differences in RMST derived from this meta-analysis showed that the efficacy of PARP inhibitors, compared with placebo, was confirmed among all patients or those with BRCA mutations, HRD carcinoma, or BRCA wild-type carcinoma when τ =360 days was used as the common time point for the included trials. The efficacy of PARP inhibitors has also been shown in an earlier meta-analysis using the HR as an efficacy parameter, independent of the BRCA mutational status. 27 The analysis based on the difference in RMST and the HR detected the same tendency for both parameters. Thus, the evidence for the efficacy of PARP inhibitors in each study population subgroup is relatively strong. The clinical trial design has to account for various factors that can potentially affect the trial result, and the study follow-up time is one of the most important factors. This approach, using reconstructed individual-level time-to-event data in the meta-analysis, allowed the adjustment of the study follow-up time variations among the assessed clinical trials by setting a certain follow-up time for the meta-analysis. Using the time-to-event data represented an advantage for the present work compared with earlier meta-analysis studies. This meta-analysis was performed for 3 different time points (τ = 360, 660, 720 days). The results showed that, up to each chosen time point, the efficacy of PARP inhibitors was consistently higher for patients with a BRCA mutation than for those with HRD carcinoma. The efficacy of PARP inhibitors was reconfirmed in this meta-analysis using a different statistical measure. Therefore, I believe that the results of this study improve the evidence for the effectiveness of PARP inhibitors.
A limitation of the present study is that reconstructed individual-level time-to-event data were used and not original patient-level data. Thus, caution should be exercised in the interpretation of the results. Specifically, to reconstruct individual-level time-to-event data using an algorithm developed by Guyot et al, 20 it was necessary to manually extract the coordinate data from the provided Kaplan-Meier curves. Therefore, the effect of measurement errors resulting from the implementation of this step was unavoidable. Furthermore, the information available for this study was limited to the publicly available results, which contained sufficient information for the individual-level data reconstruction. Although patients with BRCA mutation and HRD carcinoma provide critical information regarding the potential treatment benefit, these biomarkers are not precise enough to predict individual patients who will or will not benefit from PARP inhibitor treatment, even among those with platinum-sensitive relapsed tumors.4,5,7 Therefore, caution should be exercised when interpreting each result and the comparison of the results between the trials.
PARP inhibitors are being tested not only in ovarian cancer, but also in other cancer types, such as metastatic castration-resistant prostate cancer.28-30 The application of PARP inhibitors is expected to expand further and become a useful therapeutic option for various cancer types. Further basic research and clinical trials on PARP inhibitors will improve the overall assessment of the efficacy of PARP inhibitors. In general, there is no one single and most appropriate parameter for evaluating time-to-event data; thus, it is critical to evaluate the results of clinical trials comprehensively using various comparative parameters.
Conclusion and Relevance
The use of the RMST difference as an efficacy parameter for olaparib, niraparib, and rucaparib indicated that the efficacy of these PARP inhibitors, compared with placebo, was reconfirmed among all patients or those in study population subgroups based on the BRCA mutational status and the presence of HRD carcinoma. The meta-analysis results suggested that PARP inhibitors were the most effective in patients with BRCA mutations, followed by patients with HRD carcinoma. The results of this study concerning the extended event-free period identified by the RMST differences between PARP inhibitors and placebo improve the evidence for the effectiveness of PARP inhibitors.
Supplemental Material
sj-docx-1-aop-10.1177_10600280211013489 – Supplemental material for Effect of PARP Inhibitors as Maintenance Treatment on Restricted Mean Survival Time in Platinum-Sensitive Recurrent Ovarian Cancer: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-aop-10.1177_10600280211013489 for Effect of PARP Inhibitors as Maintenance Treatment on Restricted Mean Survival Time in Platinum-Sensitive Recurrent Ovarian Cancer: A Systematic Review and Meta-analysis by Masayuki Kaneko in Annals of Pharmacotherapy
Supplemental Material
sj-docx-2-aop-10.1177_10600280211013489 – Supplemental material for Effect of PARP Inhibitors as Maintenance Treatment on Restricted Mean Survival Time in Platinum-Sensitive Recurrent Ovarian Cancer: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-2-aop-10.1177_10600280211013489 for Effect of PARP Inhibitors as Maintenance Treatment on Restricted Mean Survival Time in Platinum-Sensitive Recurrent Ovarian Cancer: A Systematic Review and Meta-analysis by Masayuki Kaneko in Annals of Pharmacotherapy
Supplemental Material
sj-pdf-1-aop-10.1177_10600280211013489 – Supplemental material for Effect of PARP Inhibitors as Maintenance Treatment on Restricted Mean Survival Time in Platinum-Sensitive Recurrent Ovarian Cancer: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-aop-10.1177_10600280211013489 for Effect of PARP Inhibitors as Maintenance Treatment on Restricted Mean Survival Time in Platinum-Sensitive Recurrent Ovarian Cancer: A Systematic Review and Meta-analysis by Masayuki Kaneko in Annals of Pharmacotherapy
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI Grant Number JP18K18416.
Supplemental Material
Supplemental material for this article is available online.