
Abstract
Background:
Persistent wound drainage and venous thromboembolism (VTE) are potential complications of total joint arthroplasty, and these risks can be challenging to balance in clinical practice. Anecdotal observation has suggested that following joint arthroplasty, persistent wound drainage occurs more frequently with higher body weight and higher doses of tinzaparin when compared with lower body weight and lower doses of tinzaparin.
Objective:
The overall purpose of this study was to describe the impact of a tinzaparin weight-band dosing table for VTE prophylaxis on wound healing, thrombosis, and bleeding outcomes in patients undergoing total joint arthroplasty.
Methods:
This retrospective chart review included patients who underwent total hip or knee arthroplasty and received tinzaparin for thromboprophylaxis per their weight-banding category. The primary outcome was the incidence of persistent wound drainage. Secondary outcomes include the occurrence of VTE and clinically important bleeding during hospital admission.
Results:
A total of 231 patients were included in the analysis. There was no significant difference in persistent wound drainage between the 3 weight categories, and there were no differences in rates of VTE or clinically important bleeding. Concurrent use of low-dose acetylsalicylic acid was associated with a 3-fold increased risk of persistent wound drainage (risk ratio = 3.35; 95% CI = 2.14-5.24; P = 0.00003).
Conclusion and Relevance:
In joint arthroplasty patients, we observed no significant difference in rates of persistent wound drainage between various weight categories receiving different weight-banded doses of tinzaparin. Our results do not suggest that the current weight-band dosing table for tinzaparin needs to be adjusted to optimize patient outcomes.
Introduction
Osteoarthritis leads to significant pain and impairments in function, mobility, and quality of life. Total joint arthroplasty remains an important treatment modality for these patients. In Canada, nearly 130 000 joint replacement surgeries are performed annually. 1
There are several potential complications of total joint arthroplasty, including impairment of wound healing. Wound drainage is defined as “a noninfectious disturbance in wound healing of short duration that occurs during the first days after total joint arthroplasty.” 2 (p176) Persistent wound drainage following total joint arthroplasty is clinically significant because it is a predictor of prosthetic joint infections and can delay discharge from the hospital.3-7
Another potential complication of total joint arthroplasty is the development of thromboembolism. Among surgical patients, those undergoing hip or knee arthroplasty are in the highest risk category for developing venous thromboembolism (VTE), with deep vein thrombosis occurring in 40% to 60% of patients without appropriate thromboprophylaxis.8,9 Tinzaparin is a low-molecular-weight heparin (LMWH) indicated for the prevention of postoperative VTE in patients undergoing orthopaedic surgery. 10 As an antithrombotic agent, bleeding is a potential adverse reaction of tinzaparin, which ranges from minor local hematoma (approximately 5% or less) to major hemorrhage (approximately 2.8%). 10 The recommended postoperative dose for patients undergoing either hip or knee surgery is 75 anti-Xa U/kg subcutaneously (SC) once daily.10,11
Beginning in late 2018, in consultation with clinicians and key stakeholders, Alberta Health Services (AHS) moved to streamline the LMWHs available on the AHS Provincial Drug Formulary by limiting choices to enoxaparin and tinzaparin and providing a weight-banded dosing table for simplicity of dosing of these medications by patient weight. Weight-banded dosing rounds LMWH doses to be filled with the closest commercially manufactured prefilled safety syringe and eases patient transition to the community while also supporting medication management and accreditation standards. The recommended doses in the weight-banded dosing table were calculated to provide a dose that was ±10% of the patient’s body weight. There are no clinical trials data specifically using this methodology, but ample Canadian, North American, and international experience with weight-band dosing practice has shown improved safety and reduced errors in dosing. As a result of this streamlining initiative, tinzaparin was selected to be the preferential LMWH for VTE prevention and treatment within acute care, with the intention of increasing product familiarity, enhancing patient safety, and reducing costs associated with LMWH use. 11 According to the AHS developed weight-band dosing table that guides prescribers to a standardized dose of tinzaparin based on patient weight categories, patients weighing 40 to 100 kg should receive 4500 units SC once daily for VTE prophylaxis, and patients weighing 100.1 to 120 kg should receive 8000 units SC once daily (see supplemental information for document). 12 The difference in absolute dose between these 2 weight bands appears substantial, and it creates a high degree of variability in per kilogram dosing (U/kg). The hypothesis is that this variability in per kilogram dosing may lead to variability in clinical outcomes and end points.
Obesity has been cited as a risk factor for VTE.13-15 However, obesity has also been shown to be a risk factor for prolonged wound drainage following total joint arthroplasty.3,16-20 For these reasons, the balance between VTE risk and prolonged wound drainage may be particularly challenging in obese patients.
Anecdotal observation has suggested that following total joint arthroplasty, persistent wound drainage occurs more frequently in patients who weigh 100.1 to 120 kg and have received 8000 units SC daily of tinzaparin than lower-weight patients who received 4500 units SC daily. The overall purpose of this study was to evaluate the impact of the existing tinzaparin weight-band dosing table for VTE prophylaxis on wound healing, thrombosis, and bleeding outcomes in patients undergoing total joint arthroplasty.
Methods
The study protocol was reviewed and approved by the Health Research Ethics Board at the University of Alberta. The ethics review board waived the requirement for informed consent.
Study Setting and Population
This retrospective chart review was performed at Foothills Medical Centre in Calgary, Alberta, Canada, with adult patients (>18 years of age) who underwent elective primary unilateral total hip or knee arthroplasty between October 1, 2018, and December 31, 2019. Patients were included if they weighed 56 to 67 kg or 80 to 120 kg and received at least 1 dose of prophylactic tinzaparin per their weight-banding category (40-100 kg received 4500 units SC daily, and 100.1 to 120 kg received 8000 units SC daily). The reasoning behind the selection of these weight categories and a detailed description of the categorical breakdown is described in the subsequent section “Study Groups.” Patients were excluded if they underwent revision, resurfacing, or reconstruction surgery, bilateral joint replacement surgery, surgery to repair a traumatic injury or fracture, or unicompartmental knee or single-component hip surgery. Patients were also excluded if they received a therapeutic dose of tinzaparin (175 U/kg), a prophylactic or therapeutic dose of another anticoagulant or antiplatelet agent other than tinzaparin in the hospital, or used any anticoagulant or antiplatelet therapy at home prior to surgery, except for the use of low-dose (less than 100 mg/d) acetylsalicylic acid (ASA). Patients were included, however, if they were changed from prophylactic tinzaparin to a treatment dose of an anticoagulant for the purpose of treating a new-onset VTE postoperatively. If patients underwent multiple surgeries within the study time frame, only the data from the most recent surgery were included. All patients received antibiotic prophylaxis preoperatively and postoperatively, per local guidelines. All patients received tinzaparin for VTE prophylaxis beginning the next morning following joint replacement surgery. However, some patients received an additional low dose of tinzaparin (2500 units) in the evening of the day of the surgery, according to physician preference.
Study Groups
The eligible study participants were separated into 3 groups. The heaviest-weight group (termed group 3) included patients who weighed 100.1 to 120 kg and received 8000 units SC daily of tinzaparin. This group represents use of a higher weight-based dose of tinzaparin (~67-80 U/kg/d). The middle-weight group (termed group 2) included patients who weighed 80 to 100 kg and received 4500 units SC daily of tinzaparin, representing a lower weight-based dose of tinzaparin (~45-56 U/kg/d). The lowest-weight group (termed group 1) included patients who weighed 56 to 67 kg and received 4500 units SC daily of tinzaparin. This group represents a higher dose of tinzaparin (~67-80 U/kg/d) in lower-weight individuals and served as a group to match the equivalent unit-per-kilogram dosing between groups 1 and 3, in an attempt to control for the confounding factor of absolute body weight, in the risk of developing persistent wound drainage.
Outcomes
The primary outcome of this study was the incidence of persistent wound drainage in each of the 3 weight categories. This was reported as the total number of patients with persistent wound drainage and the number of patients with persistent wound drainage that led to an increased length of hospital admission. For the purposes of this study, persistent wound drainage is defined as a noninfectious disturbance in wound healing that persists at least 72 hours postoperatively, as documented by nursing staff. This definition was adapted from the definition provided by the International Consensus Meeting on Prosthetic Joint Infection to allow the feasibility of retrospective application of the criteria. 2 An internal quality improvement tracking form that documents the reason for prolonged admissions (length of stay longer than 3 days postoperatively) was used to identify patients with persistent wound drainage, along with nursing notes in the patient’s chart regarding wound description and dressing changes. Severity of wound drainage was not evaluated given the difficulty in collecting this information retrospectively. The secondary outcomes of this study included the incidence of VTE, encompassing deep-vein thrombosis and pulmonary embolism, and the incidence of clinically important bleeding that occurred during hospital admission post-joint arthroplasty. The occurrence of VTE and clinically important bleeding were defined using ICD-10-CA Codes (International Classification of Diseases, 10th Revision, with Canadian Enhancements).
Sample Size
Because it may be less common for patients who undergo hip or knee arthroplasty to be in the lowest body weight category, data were collected beginning from the most recent data time point and working backward in time until a sufficient sample size was obtained in each group. We estimated that 140 patients were needed in each group (total n = 420) to detect a difference of 10% in the primary outcome, with a power of 80% and α =0.05. It was felt that a 10% difference in rates of wound drainage between groups would be clinically significant.
Statistical Analysis
Descriptive statistics were used to summarize and report demographic characteristics and primary and secondary outcomes. Statistical comparisons were conducted using χ2 or Fisher Exact tests. Association of variables is presented as a risk ratio with 95% CIs. Statistical significance was set at α =0.05.
Results
A total of 231 patients who underwent total joint arthroplasty were included in the study, which did not meet our target sample size. This is attributed to having to exclude more patients than expected because they did not receive the appropriate tinzaparin dose based on their weight category and because of limitations in the time frame of data available given the change in practice when tinzaparin became the preferential LMWH at our site (~September 2018).
The demographic characteristics of the groups are outlined in Table 1. Overall, the groups were well balanced with respect to age and length of hospital stay. The groups were appropriately differentiated by their weight and tinzaparin dose (U/kg), with group 1 and group 3 successfully matched based on tinzaparin dose. There was a higher proportion of female patients and patients who underwent hip surgery in group 1 compared with the other groups.
Baseline Demographic Characteristics.

Abbreviation: ASA, acetylsalicylic acid.
Persistent Wound Drainage
The observed frequencies of persistent wound drainage in each group are summarized in Table 2. In total, 17.0% (8/47) of patients in group 1, 23.6% (33/140) of patients in group 2, and 27.3% (12/44) of patients in group 3 developed wound drainage. There were no significant differences in wound drainage (P = 0.489) or wound drainage leading to an increased length of stay (P = 0.464) between groups.
Persistent Wound Drainage in Each Weight Category.
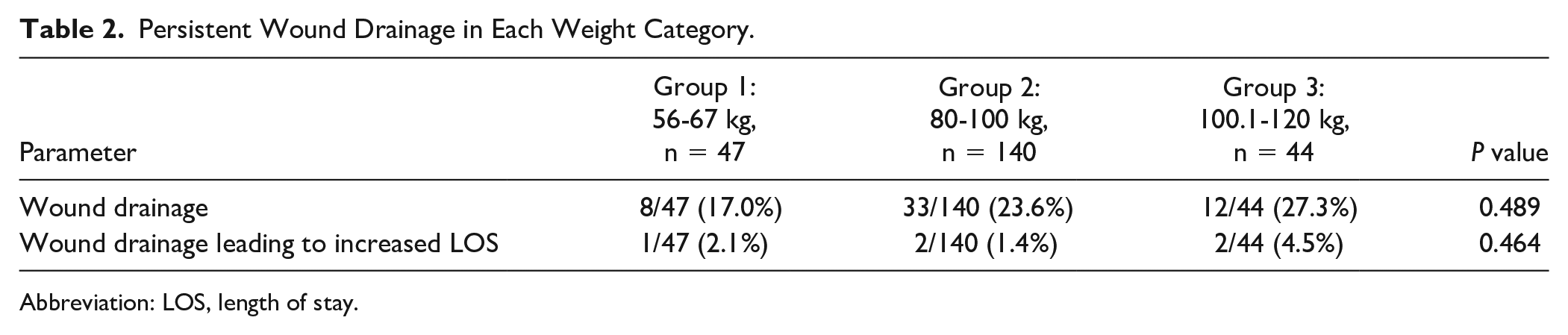
Abbreviation: LOS, length of stay.
VTE and Bleeding
In group 2, 1/140 participants (0.7%) developed a VTE while in hospital. No patients in group 1 or group 3 developed a VTE. Similarly, 2/140 participants (1.4%) in group 2 experienced a clinically important bleed while on tinzaparin prophylaxis during their hospital admission. No patient in the other groups experienced a bleed.
Subgroup Analyses
Because the baseline characteristics of sex and type of surgery were not matched between groups, we conducted a bivariate analysis to determine if there was a relationship observed between these parameters and wound drainage. There were no statistically significant differences in persistent wound drainage between hip and knee surgeries (21.1% vs 24.4%; P = 0.558), or between male and female sex (20.2% vs 25.9%; P = 0.301).
As concurrent ASA therapy and timing of tinzaparin initiation were based on physician preference at our site, we conducted an analysis to determine the impact of these parameters on wound drainage. The use of concurrent ASA was associated with a significant increase in wound drainage compared with no ASA use (66.7% vs 19.9%; RR = 3.35; 95% CI = 2.14-5.24; P = 0.00003). There was no difference observed in the incidence of wound drainage in patients who received an additional low dose of tinzaparin (2500 units) postoperatively on the day of surgery and then received the full dose of tinzaparin on subsequent days compared with patients who received tinzaparin only at the full dose starting the day after surgery (28.9% vs 19.6%; P = 0.106). No statistically significant differences were found for risk factors associated with wound drainage that prolonged hospital admission for any of the subgroup analyses. The results of these subgroup analyses are presented in Table 3.
Subgroup Analyses for Persistent Wound Drainage.
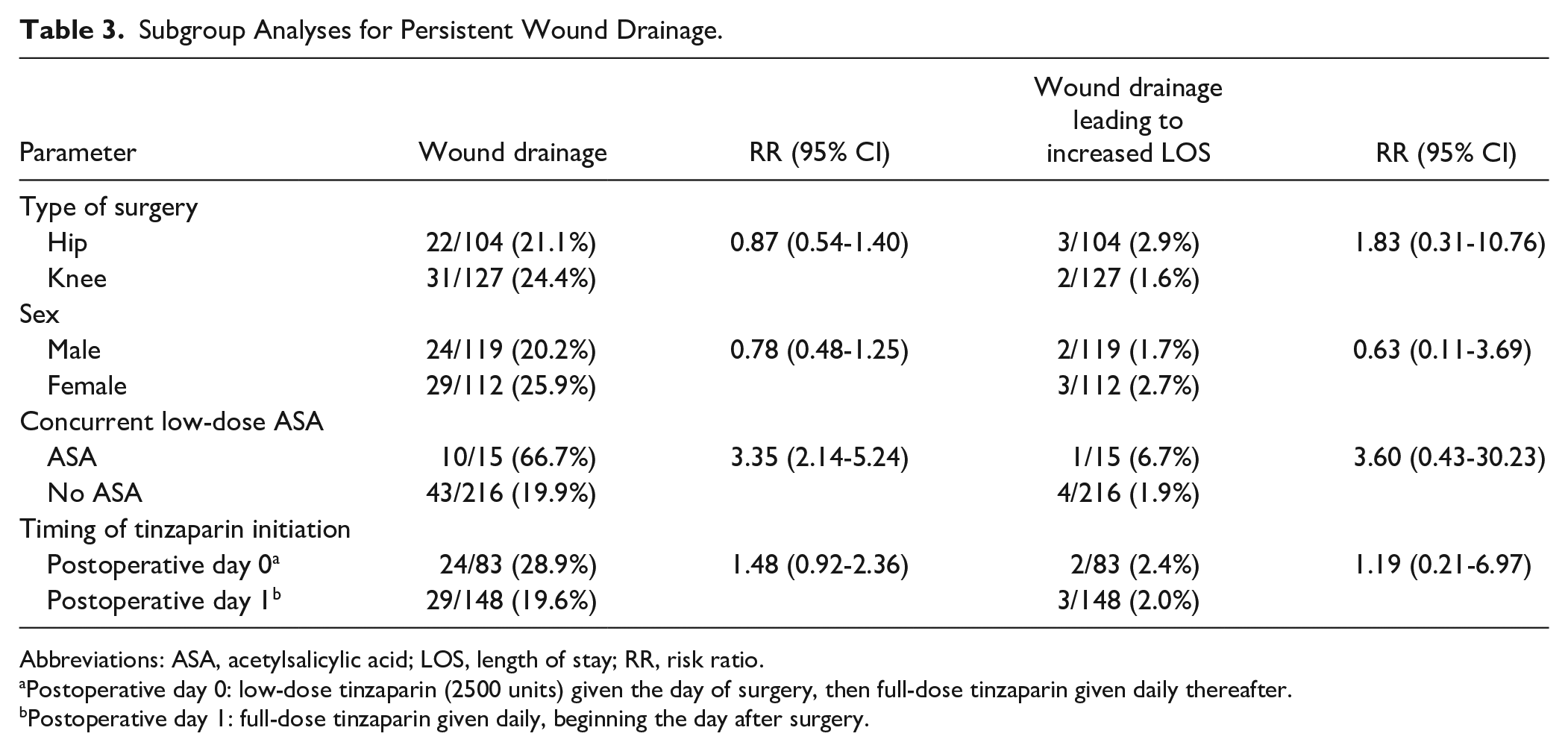
Abbreviations: ASA, acetylsalicylic acid; LOS, length of stay; RR, risk ratio.
Postoperative day 0: low-dose tinzaparin (2500 units) given the day of surgery, then full-dose tinzaparin given daily thereafter.
Postoperative day 1: full-dose tinzaparin given daily, beginning the day after surgery.
Conclusion and Relevance
Persistent wound drainage and VTE are 2 potential complications of total joint arthroplasty, and it can be challenging to balance the risks of both in clinical practice. The purpose of this study was to evaluate the impact of weight-band dosing of tinzaparin on persistent wound drainage in patients undergoing hip or knee arthroplasty. In joint arthroplasty patients, we observed no significant difference in rates of persistent wound drainage between various weight categories receiving different weight-banded doses of tinzaparin.
Although our primary findings were nonsignificant, the study was underpowered to detect a true difference between groups. There was no clear relationship between weight-banded dose of tinzaparin and persistent wound drainage, but rather, we observed a relationship between increased weight and increased wound drainage. This is consistent with findings in previously published literature that describe obesity as a risk factor for developing persistent wound drainage.3,16,17,21
Although our site has developed a weight-band dosing table to standardize dosing of tinzaparin, there were 25 patients who were excluded from this study who were in the highest weight category, but yet they did not receive the appropriate dose of tinzaparin based on their weight—that is to say, they received a dose which was in the weight band for the lower weight category. We conducted an analysis comparing this group (group 4) with group 3, which has the same body weight category but where patients received a different dose of tinzaparin (see Table 4). There appeared to be a numerically higher rate of wound drainage (27.3% vs 16.0%) and potentially more severe wound drainage, leading to prolonged hospital admission (4.5% vs 0%) in group 3, which received a higher dose of tinzaparin (~67-80 U/kg) compared with group 4, which received a lower dose of tinzaparin (~39-45 U/kg), although the differences between these groups were nonsignificant.
Post Hoc Data Comparing Patients in the Highest Weight Group With Differing Tinzaparin Dose.
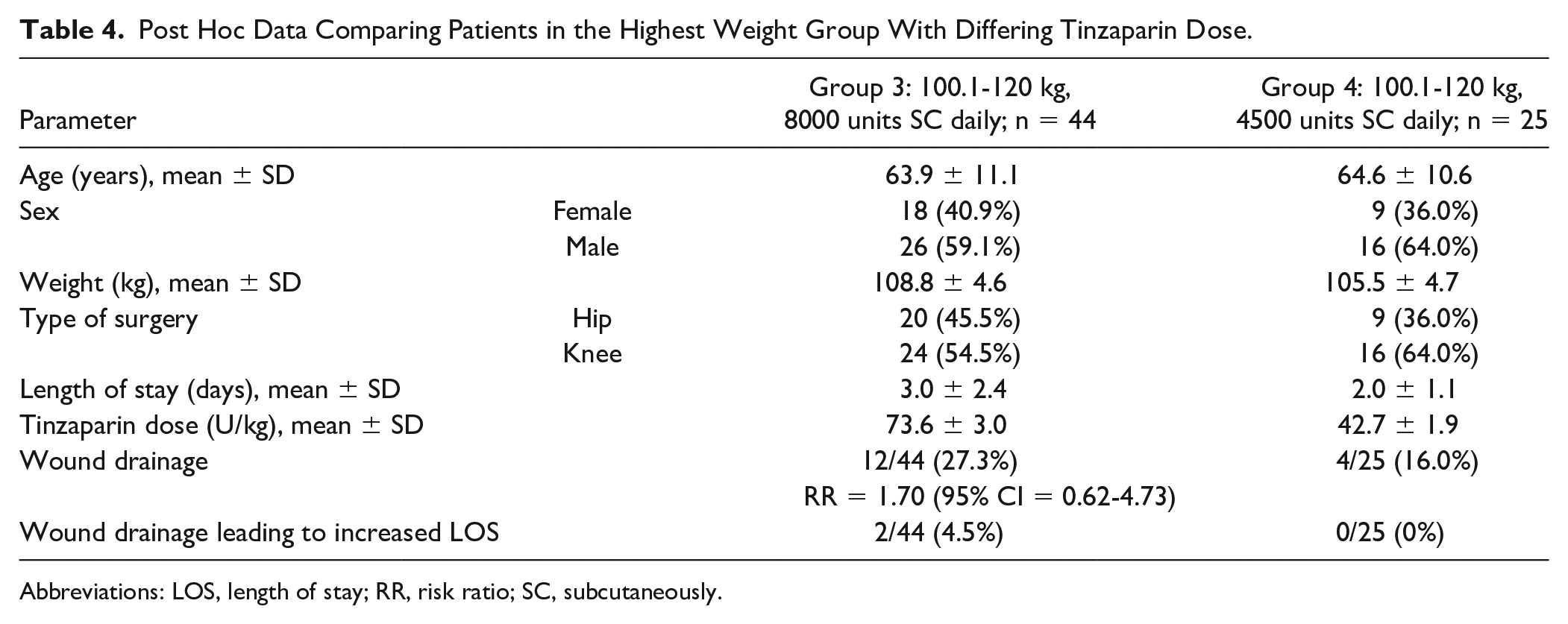
Abbreviations: LOS, length of stay; RR, risk ratio; SC, subcutaneously.
To our knowledge, this is the first study to evaluate the impact of the dose of LMWH on wound drainage. Although we did not achieve our desired sample size and larger studies are needed to further evaluate this relationship, previously published literature suggests that excessive anticoagulation may be associated with prolonged wound drainage.5,22 A review of postoperative persistent wound drainage identified the use of LMWH for VTE prophylaxis as an independent risk factor. 3 It has been demonstrated that a greater proportion of joint arthroplasty patients on prophylactic LMWH have wound drainage and this drainage persists longer than in patients treated with warfarin or ASA.3,23 Additionally, a review of postoperative complications following total joint arthroplasty found a higher risk of bleeding and surgical site infections in patients on prophylactic LMWH compared with warfarin. 22 In patients on thromboprophylaxis for joint replacement surgery, wound leakage was identified as the reason for delayed discharge from the hospital in approximately one-third of patients. 7 As a result, there is an important balance between appropriate anticoagulation to prevent VTE and allowing appropriate conditions for surgical wounds to heal. 22
A unique finding from our data came from the subgroup analysis showing that concurrent use of low-dose ASA with tinzaparin yielded a statistically significant increase in wound drainage compared with use of tinzaparin alone. However, given the small sample of patients who were on ASA in this study, future studies are warranted to describe the relationship between combination therapy and wound drainage in more detail. Although there appears to be an association between ASA use and persistent wound drainage in our study population, it is unclear what an appropriate management strategy to deal with this clinical situation would entail because patients may have concomitant comorbidities for which ASA treatment is appropriate.
The secondary end points of VTE and bleeding episodes yielded frequencies that were too small to arrive at meaningful conclusions. However, no obvious signal was observed in this study to suggest that the current standardized doses of tinzaparin used are inadequate for efficacy or safety purposes.
Our study does have some limitations. First, there is potential subjectivity in the documentation by nursing staff in terms of the description of the wound and timing of dressing changes as well as the authors’ interpretation of these chart notes. To mitigate this, a broader definition of wound drainage was used and any form of drainage that was documented greater than 72 hours postoperatively was included. As a result, the incidence of wound drainage reported was slightly higher than has been previously depicted in the literature (up to 21%). 2 Earlier studies have had variable definitions of wound drainage, including describing the surface area of the dressing that was soaked, 2 but this definition was not feasible in a retrospective study design. For these reasons, we also could not evaluate severity of wound drainage. We reported on wound drainage that appeared to be clinically significant as it persisted several days after surgery and, in some cases, led to a prolonged hospital admission. Second, we were unable to capture information on wound drainage that persisted in patients who were discharged home, given the data sources available. However, this was felt to be less clinically relevant because the drainage was not severe enough to warrant continued hospitalization. Data from patients who had an extended hospital admission for other purposes (eg, concerns with mobility) were included. Third, the presence of wound drainage does not necessarily indicate a more complicated wound because it may heal spontaneously with appropriate wound care. 24 However, the data presented in this study remain impactful given the increased costs to the health care system related to persistent wound drainage, such as additional hospitalization days, medication administration, dressing changes, and nursing time. It is beyond the scope of this study to report on prosthetic joint infections or functional outcomes. We also note that from the point of view of the demographics of our study population, there is a tendency for our group 1 patients to be skewed more heavily toward female hip replacement patients, whereas our group 2 and 3 patients tend to be skewed toward male knee replacement patients. It was also noted that groups 2 and 3 were more likely to be taking ASA concurrently and that there were no patients in group 1 that were taking ASA concurrently. Increased wound drainage in groups 2 and 3 is likely at least partially explained by obesity and/or concurrent ASA use, although it is difficult to determine the exact contribution of these 2 confounding factors to the results that we have observed.
At our institution, patients who receive prophylactic dosing of LMWH typically receive active monitoring of hemoglobin/hematocrit and electrolytes. They are also monitored for adverse effects of the LMWH as well as clinical observation for the development of VTE. We do not actively monitor antifactor Xa levels, because this lab value is typically only monitored in patients who are on treatment doses of LMWH in whom there is reason to believe that their risk of a VTE event might be outside of the expected course (eg, obesity, renal insufficiency, pregnancy). It may be that monitoring of antifactor Xa levels would provide an interesting model for monitoring both VTE risk as well as monitoring for persistent wound drainage, but with uncertain target range data in the real world, it would be difficult to determine the appropriate protocol for management with respect to antifactor Xa levels in this patient population. This would be a potential question for future study.
This study has implications for clinical practice. Our results do not suggest that the current weight-band dosing table for tinzaparin needs to be adjusted to optimize patient outcomes. However, we acknowledge that it is difficult to determine the absolute contribution of concurrent ASA and obesity itself as factors that may contribute to increased wound drainage in the elective adult joint arthroplasty population.
Supplemental Material
sj-pdf-1-aop-10.1177_10600280211024294 – Supplemental material for Impact of Weight-Band Dosing of Tinzaparin for Venous Thromboembolism Prophylaxis on Persistent Wound Drainage in Adult Patients Undergoing Hip and Knee Arthroplasty
Supplemental material, sj-pdf-1-aop-10.1177_10600280211024294 for Impact of Weight-Band Dosing of Tinzaparin for Venous Thromboembolism Prophylaxis on Persistent Wound Drainage in Adult Patients Undergoing Hip and Knee Arthroplasty by Cassandra Cooper, Ouida Antle, Jennifer Lowerison, Deonne Dersch-Mills and Ashley Kenny in Annals of Pharmacotherapy
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.