
Abstract
Background:
Few studies describe the use of dolutegravir (DTG)-based dual therapies under routine clinical practice.
Objectives:
To report real-life data on the use of DTG-based dual therapies in treatment-experienced patients.
Methods:
This was an observational, retrospective study. It included all treatment-experienced HIV patients starting a DTG-based dual therapy from 2014 to 2018. The primary end point was to identify the incidence and reasons for the switch. The secondary end points were to assess the effectiveness, safety, adherence, and costs after 48 weeks of treatment (W48).
Results:
The incidence of the switch to a DTG-based dual therapy increased from 1.6 patients per 1000 patient-years in 2014 to 38.6 in 2018. A total of 241 patients initiated this therapy: 113 (46.9%) patients started DTG plus rilpivirine (RPV), 72 (29.9%), DTG plus lamivudine (3TC), and 68 (28.2%), DTG plus boosted-darunavir (b-DRV). A total of 170 patients completed W48 of follow-up. By intention-to-treat analysis, 89.3% of virologically suppressed (VS) patients (94.3% with DTG plus b-DRV, 91.3% with DTG plus 3TC, and 87.2% with DTG plus RPV) and 56.7% of non-VS patients (71.4% with DTG plus RPV and 52.2% with DTG plus b-DRV) achieved a viral load <50 copies/mL at W48. The protocol-defined virological failure was 6.5%. Overall, 8.8% of patients had early discontinuation. The annual cost increased by €800 per patient ($916).
Conclusions and Relevance:
The use of DTG-based dual therapies has increased in real life, showing a favorable effectiveness and safety profile. Treatment costs increased, except for the switch to DTG plus 3TC.
Introduction
The introduction of combined antiretroviral therapy (ART) has led people living with HIV (PLWH) to live almost as long as those without HIV infection. 1 However, because of the chronic inflammatory status, different events such as renal, bone, cardiovascular, or liver disease, cognitive decline, and metabolic disorders could occur 15 to 20 years earlier than normal. 2 Besides, concerns exist regarding the toxicities accruing from cumulative exposure to drugs that need to be taken for life. 3
Reducing the number of ART agents that PLWH require may have the potential to reduce cumulative toxicities as well as the economic burden associated with long-term treatment. 4 Although not all simplified regimens studied have demonstrated positive results, dual regimens with dolutegravir (DTG) plus rilpivirine (RPV), lamivudine (3TC), or boosted darunavir (b-DRV) have recently been shown to maintain viral suppression in ART-experienced patients.5-11
However, few studies describe patient characteristics and virological outcomes after the use of the DTG-based dual therapies in routine clinical practice.12-15 Besides, their value on improving treatment adherence and reducing ART costs is not well described.
In this study, we report real-life data on the incidence and reasons for the switch to DTG-based dual therapies in a large Spanish cohort of ART-experienced PLWH and the effectiveness and safety of each regimen. Adherence to these combinations and their impact on ART costs were also evaluated.
Methods
This was an observational, retrospective study, which was conducted at Gregorio Marañón University General Hospital, a tertiary care institution serving a population of 350 000 inhabitants in Madrid (Spain). This hospital is a national reference center for HIV/AIDS that provides the most advanced patient care to 2700 PLWH every year.
The study sample comprised all treatment-experienced PLWH starting a DTG-based dual therapy from February 12, 2014 (approval date of DTG), to December 31, 2018.
Assessments
The primary end point of the study was to identify the incidence and reasons for the switch to a DTG-based dual therapy in the study population. The secondary end points were to assess the effectiveness, safety, and adherence to each combination after 48 weeks of treatment (W48). Only patients who had completed the W48 at the study end point were included in this second analyses. The economic impact of the switch (estimated as the difference of the annual per-patient ART costs between the DTG-based dual therapy and the previous ART) was also evaluated.
The effectiveness was defined as the proportion of patients who achieved virological suppression (viral load [VL] < 50 copies/mL) at W48. Treatment was considered to have failed when any of the following events occurred: virological failure (VF), defined as plasma HIV-1 RNA >50 copies/mL at W48 in previously nonsuppressed patients, or 2 consecutive HIV-1 RNA measurements >50 copies/mL or a single measurement of >50 copies/mL if treatment was changed afterward in previously suppressed patients; change of treatment regimen for non-VF reasons; treatment interruption by the patient; and incomplete data. VL was evaluated 2 or 3 times during the 48-week period of the study to ascertain virological control, according to the routine clinical protocol in the hospital.
VL was determined using the SIEMENS VERSANT HIV-1/kPCR system (limit of quantification: 37 HIV-1 RNA copies/mL). Reverse-transcriptase, protease, and integrase sequencing were performed prior to the change following the manufacturer’s indications if the patient was virologically nonsuppressed or after the change in those patients whose therapy had failed. Drug resistance mutations, as well as genotypic resistance (resistance or possible resistance), were defined according to the Stanford HIV Drug Resistance Database algorithm.
The safety was evaluated with the incidence of adverse events (AEs) leading to discontinuation of the DTG-based dual therapy and its effect on laboratory values. Laboratory data at baseline were those obtained up to 4 weeks before starting the dual therapy. Laboratory data at W48 were those obtained between W44 and W52.
The following variables were recorded: baseline demographics, comorbidities, HIV-related data (including VL, CD4+ T-cell count, presence of resistance mutations, and previous ART), and laboratory values, including the fasting lipid profile, liver enzymes, total bilirubin, creatinine, and glomerular filtration rate (GFR). The GFR was estimated by applying the Modification of Diet in Renal Disease (MDRD) equation, which is the standard measure used in Spain. Other variables such as the reason for the discontinuation of the DTG-based dual therapy, the development of resistance mutations in those patients whose dual therapy failed, pill burden, adherence to ART, and the annual per-patient ART costs were also recorded. Patient and treatment data were obtained retrospectively from the HCIS electronic medical record and Farhos Computerized Physician Order Entry software.
Adherence was assessed using the method of medication possession ratio. This is reported automatically by the electronic dispensing software of the pharmacy department by dividing the sum of a day’s supply by the number of days in a period multiplied by 100. Adherence was compared 48 weeks before and after the switch or until its interruption. Pill burden was calculated as the total number of pills the patient took on a daily basis.
ART costs were calculated based on the actual dose administered and the drug acquisition costs for each year. The prices of ART may differ from officially established ones. Costs are presented in euros (€) and US dollars ($), using 1.145 as the conversion rate dollar-euro, published by European Central Bank on December 31, 2018 (date of the end of the study).
Statistical Analysis
Continuous variables were described by the median and interquartile range (IQR) and categorical variables by frequencies and percentages. The Wilcoxon signed-rank test was used for comparisons between 2 continuous variables. The χ2 test or Fisher exact test was used to compare 2 categorical variables. A P value <0.05 was considered statistically significant.
The effectiveness was analyzed using intention to treat (ITT), missing equals failure, and on-treatment (OT) analyses, in which all patients whose treatment was interrupted for nonvirological reasons were excluded.
Computer support used for the statistical analysis was Stata Statistical Software: Release 14 (College Station, TX: StataCorp LP).
Ethical Aspects
The study protocol was approved by the local Ethics Committee with code FAR.DUAL.2019.1, in accordance with the principles of the Declaration of Helsinki, 2008.
Results
Incidence of the Switch to a DTG-Based Dual Therapy
The incidence of the switch to a DTG-based dual therapy was progressively increased from 1.6 patients per 1000 patient-years in 2014 to 38.6 in 2018 (Figure 1). From 2014 to 2017, the most frequent DTG-based dual therapy initiated was DTG plus RPV, compared to 2018, when it was DTG plus 3TC. The use of DTG plus b-DRV remained stable and close to 5 to 10 patients per 1000 patient-years.
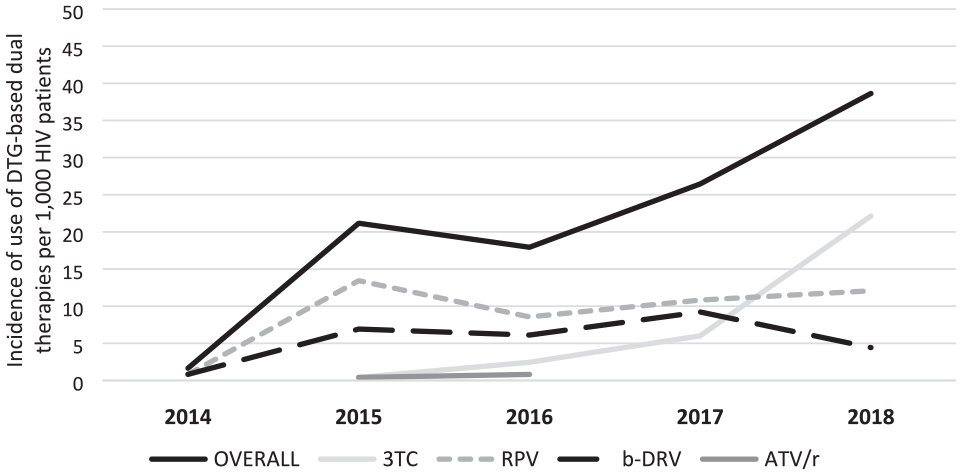
Incidence of use of dolutegravir-based dual therapies.
Overall, 241 patients initiated a DTG-based dual therapy throughout the study period, which represents 8.9% of the ART-experienced PLWH population. Of these, 113 (46.9%) patients started DTG plus RPV, 72 (29.9%), DTG plus 3TC, and 68 (28.2%), DTG plus b-DRV. Only 3 patients received DTG plus atazanavir/ritonavir and 1 patient, DTG plus etravirine. In all, 16 patients received more than 1 DTG-based dual therapy during the study period. All patients received the dual regimen in separate pills because no single-tablet formulations were available.
Population Characteristics and Reasons for the Switch to a DTG-Based Dual Therapy
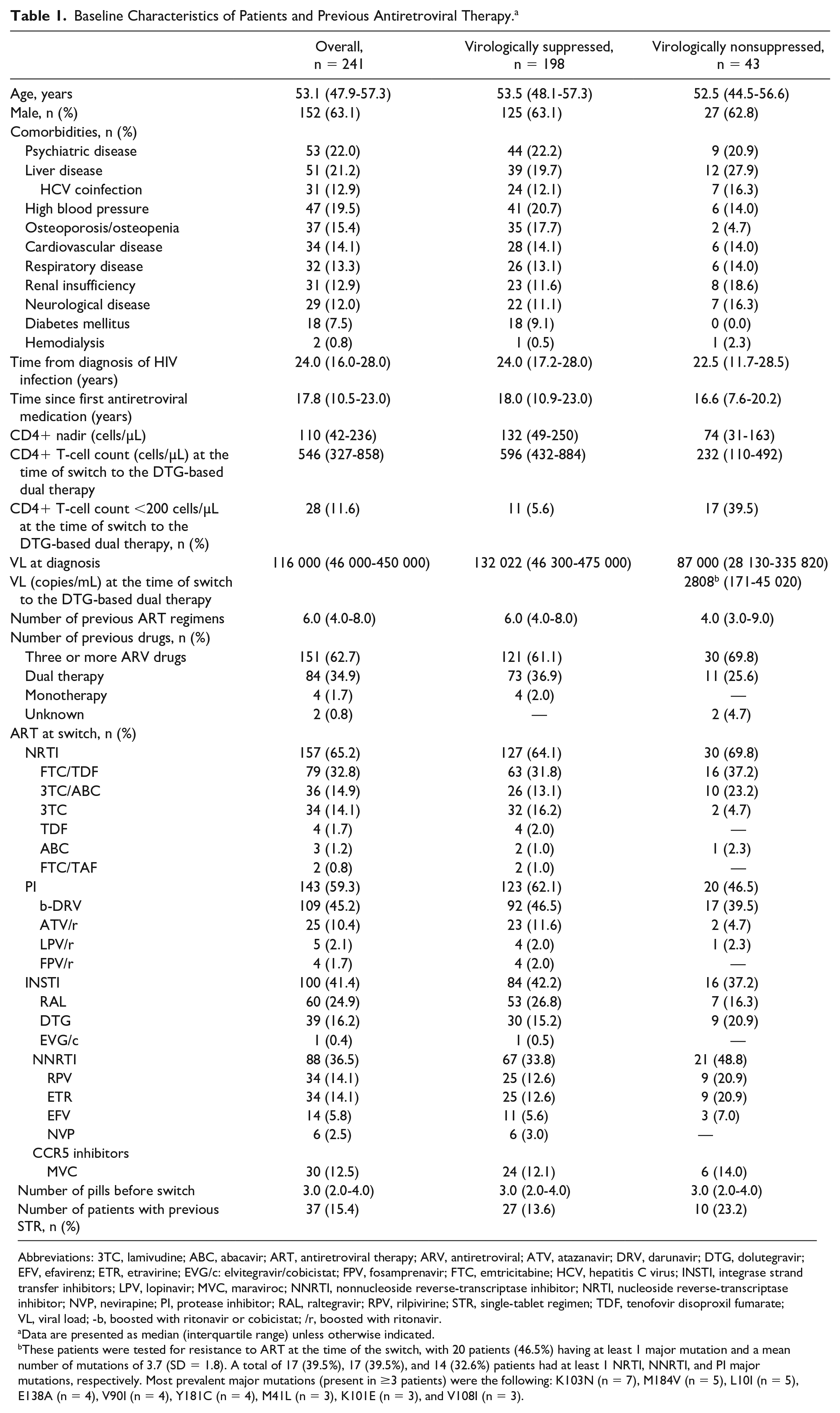
Overall, 241 ART-experienced PLWH initiated a DTG-based dual therapy from February 12, 2014, to December 31, 2018. Baseline characteristics of these patients are summarized in Table 1. Their median age was 53 years (IQR = 48-57), and 63% were male. Overall, 82.2% of patients were virologically suppressed (VS), and the median time since first ART medication was 17.8 (IQR = 10.5-23.0) years. At least 1 comorbidity was present in 64.7% of all patients, with a mean number of comorbidities per patient of 1.82 (SD = 0.95). The most frequent comorbidities were psychiatric disease (22.0%), liver disease (21.2%), high blood pressure (19.5%), and osteoporosis/osteopenia (15.4%).
Baseline Characteristics of Patients and Previous Antiretroviral Therapy. a
Abbreviations: 3TC, lamivudine; ABC, abacavir; ART, antiretroviral therapy; ARV, antiretroviral; ATV, atazanavir; DRV, darunavir; DTG, dolutegravir; EFV, efavirenz; ETR, etravirine; EVG/c: elvitegravir/cobicistat; FPV, fosamprenavir; FTC, emtricitabine; HCV, hepatitis C virus; INSTI, integrase strand transfer inhibitors; LPV, lopinavir; MVC, maraviroc; NNRTI, nonnucleoside reverse-transcriptase inhibitor; NRTI, nucleoside reverse-transcriptase inhibitor; NVP, nevirapine; PI, protease inhibitor; RAL, raltegravir; RPV, rilpivirine; STR, single-tablet regimen; TDF, tenofovir disoproxil fumarate; VL, viral load; -b, boosted with ritonavir or cobicistat; /r, boosted with ritonavir.
Data are presented as median (interquartile range) unless otherwise indicated.
These patients were tested for resistance to ART at the time of the switch, with 20 patients (46.5%) having at least 1 major mutation and a mean number of mutations of 3.7 (SD = 1.8). A total of 17 (39.5%), 17 (39.5%), and 14 (32.6%) patients had at least 1 NRTI, NNRTI, and PI major mutations, respectively. Most prevalent major mutations (present in ≥3 patients) were the following: K103N (n = 7), M184V (n = 5), L10I (n = 5), E138A (n = 4), V90I (n = 4), Y181C (n = 4), M41L (n = 3), K101E (n = 3), and V108I (n = 3).
The prevalence of comorbidities was more frequent in patients who started DTG plus RPV (72.1%), compared to b-DRV (62.7%) and 3TC (56.7%), showing statistically significant differences when comparing DTG plus RPV with DTG plus 3TC (P = 0.036).
In relation to previous ART therapies, 97.5% of patients had received a nucleoside reverse transcriptase inhibitor (NRTI), 88.0% a nonnucleoside reverse transcriptase inhibitor (NNRTI), 83.4% a protease inhibitor (PI), and 51.9% an INSTI. At the point of switch, 62.7% of patients were receiving ≥3 antiretrovirals (ARVs), whereas 34.9% were already taking another dual therapy not based on DTG. The ARVs before the switch are detailed in Table 1. The most common backbone was emtricitabine/tenofovir disoproxil fumarate (32.8%), and the anchor drugs were b-DRV (45.2%) and raltegravir (24.9%). A total of 39 (16.2%) patients were already receiving DTG as part of a triple therapy. Also, 38.5% of patients switched to DTG plus RPV, 35.8% to DTG plus 3TC, 23.1% to DTG plus b-DRV, and 2.6% to DTG plus ATV. Of the 72 patients who switched to DTG plus 3TC, 4 (5.6%) were receiving the single-tablet regimen (STR) regimen DTG/ABC/3TC.
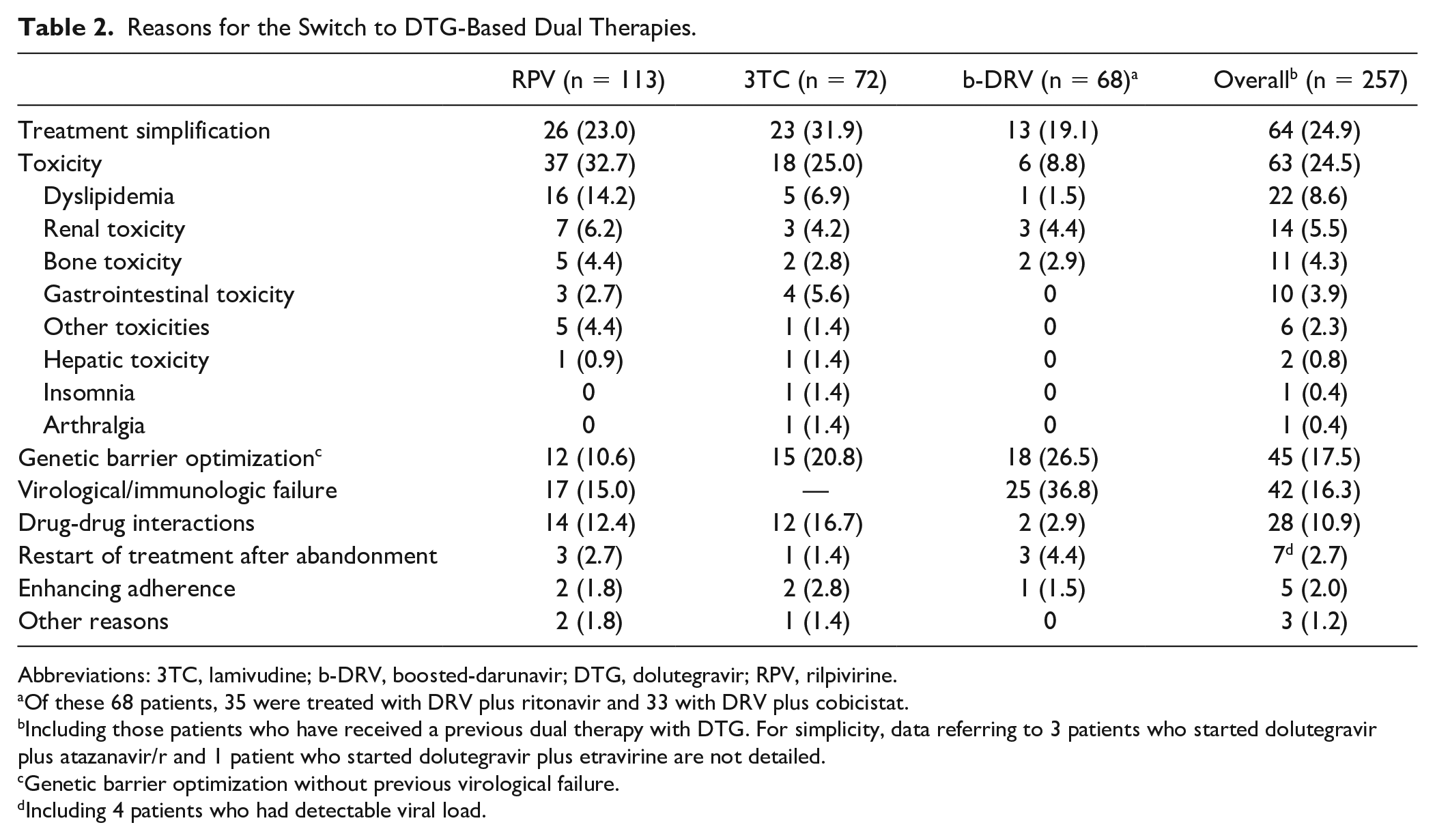
The most common reasons for initiating a DTG-based dual therapy were treatment simplification (24.9%) and toxicity reasons (24.5%), although this proportion varied considerably between the different therapies (Table 2). DTG plus 3TC was mainly used as a simplification strategy (mostly previously treated with emtricitabine/tenofovir disoproxil fumarate, 60.9%), whereas the combination with RPV and b-DRV was used to improve tolerability and effectiveness, respectively. The most common toxicities reported with previous ARTs were dyslipidemia (22 cases, mostly PI treated, n = 20), renal toxicity (14 cases, mostly tenofovir disoproxil fumarate [TDF] treated, n = 12), and bone toxicity (11 cases, mostly TDF treated, n = 10). For the 14 patients with renal toxicity, 10 had a reduced GFR, 2 had glucosuria, 1 experienced a renal tubulopathy, and 1 experienced phosphaturia. Of these 14 patients, 7 (50.0%) showed proteinuria at the time of the switch. In relation to the bone toxicity (n = 11), all of them had reduced bone mineral density, 7 with osteoporosis (63.6%) and 4 with osteopenia (36.4%). Overall, 42 patients (16.3%) initiated the regimen as salvage therapy when showing VF, receiving mostly DTG plus b-DRV (25/42). None of these non-VS patients started DTG plus 3TC. In all, 28 patients (10.9%) switched to a DTG-based dual therapy because of drug-drug interactions, including 9 patients who were treated with DAA for the HCV infection.
Reasons for the Switch to DTG-Based Dual Therapies.
Abbreviations: 3TC, lamivudine; b-DRV, boosted-darunavir; DTG, dolutegravir; RPV, rilpivirine.
Of these 68 patients, 35 were treated with DRV plus ritonavir and 33 with DRV plus cobicistat.
Including those patients who have received a previous dual therapy with DTG. For simplicity, data referring to 3 patients who started dolutegravir plus atazanavir/r and 1 patient who started dolutegravir plus etravirine are not detailed.
Genetic barrier optimization without previous virological failure.
Including 4 patients who had detectable viral load.
Effectiveness
A total of 170 patients (140 VS and 30 non-VS at baseline) completed 48 weeks of follow-up and then were included in the effectiveness analysis. These results are shown in Figure 2.
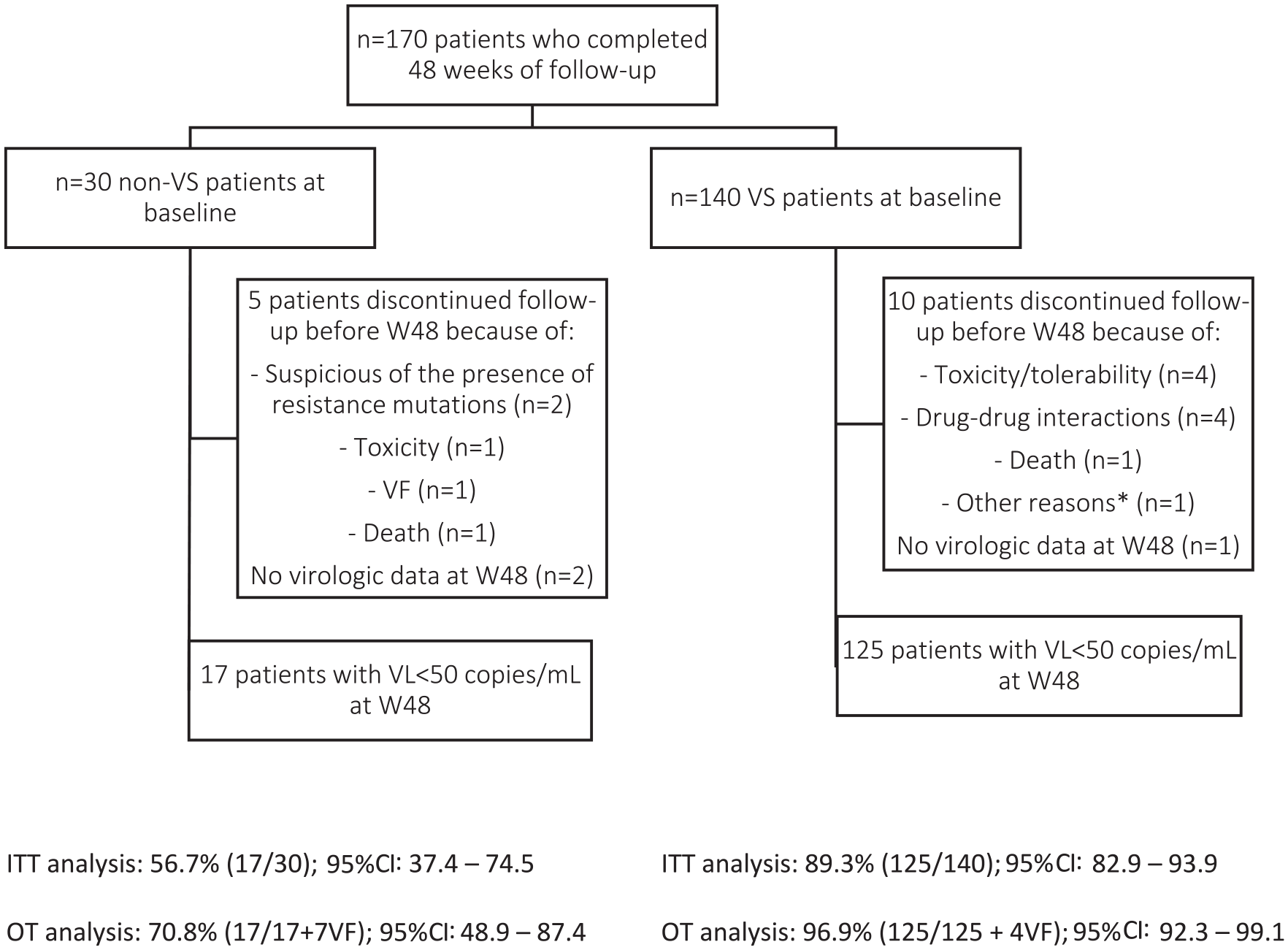
Effectiveness results.
The virological suppression at W48 was observed in 125 of 140 VS patients (89.3% [95% CI: 82.9%-93.9%]) and in 17 of 30 non-VS patients (56.7% [95% CI: 37.4%-74.5%]) by ITT analysis. When patients who had discontinued therapy for nonvirological reasons were excluded, the proportion of patients who achieved virological suppression increased to 96.9% (95% CI: 92.3%-99.1%) in the subgroup of VS patients and 70.8% (95% CI: 48.9%-87.4%) in non-VS patients.
The virological suppression rate was comparable across the different DTG-based dual therapies by OT analysis. By ITT analysis, the virological suppression rate was slightly lower for DTG plus RPV (87.2%) in VS patients (Figure 3). In this subgroup, 6 (7.7%) patients discontinued the therapy for nonvirological reasons. In contrast, in the small subpopulation of non-VS patients, the virological suppression rate was lower with DTG plus b-DRV (52.2%). Four patients (17.4%) had stopped this combination because of ART optimization (n = 2), death (n = 1), and toxicity (n = 1).
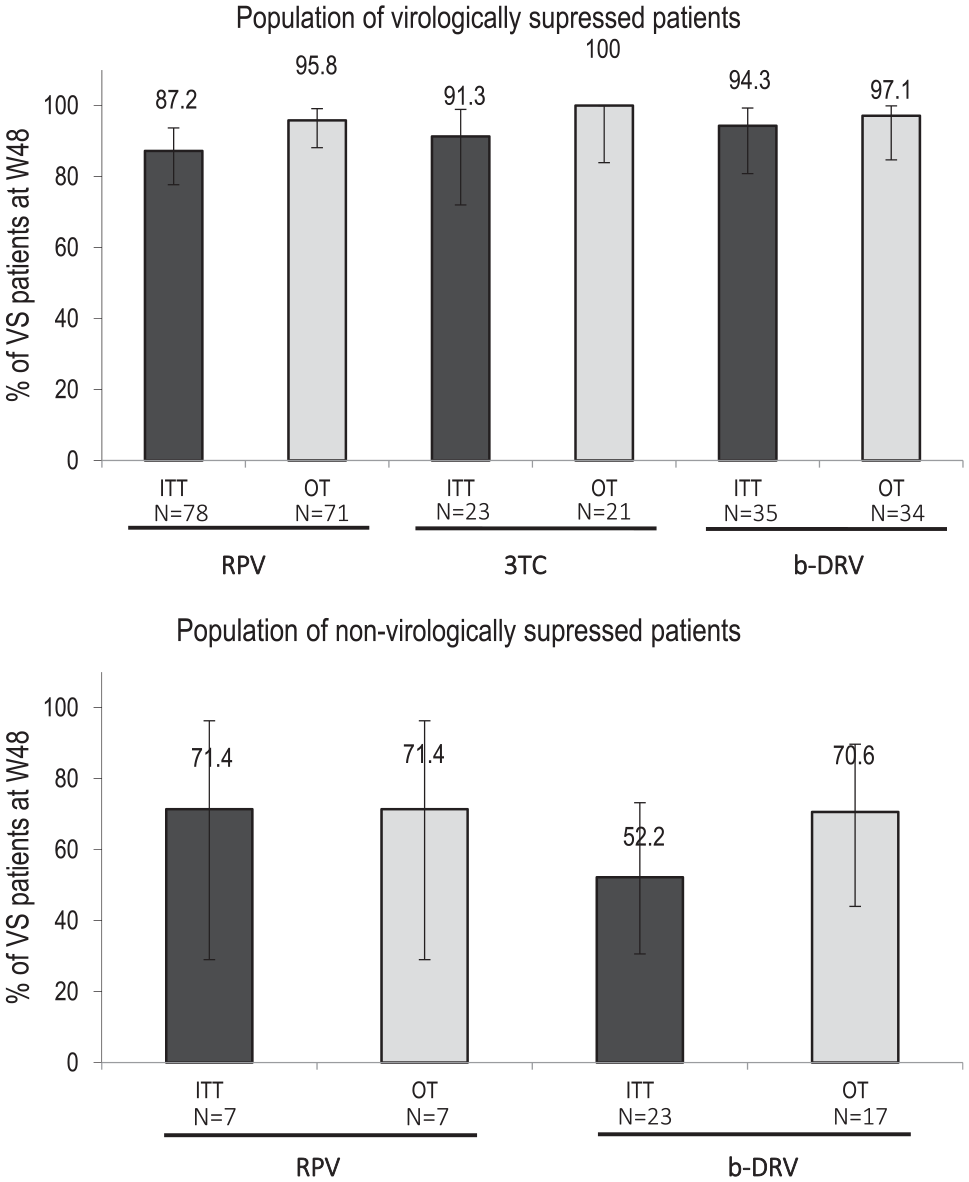
Effectiveness of dolutegravir-based dual therapies.
Overall, the global rate of protocol-defined VF at W48 was 6.5%, being significantly higher in the non-VS population (23% vs 2.8%, P < 0.001). No VF was observed in the DTG plus 3TC population, being 5.9% and 10.3% for DTG plus RPV and DTG plus b-DRV, respectively. In these patients, the median VL at W48 was 105.0 copies/µL (IQR = 86.0-31 985.0). Three of 11 patients underwent resistance testing at the time of the VF, in whom no major resistance mutations to DTG or the second drug were detected. The median adherence in these 3 patients was 95.0%.
The median increase in the CD4+ T-cell count was 26 cells/µL (IQR = −52.0 to 135.0), and the CD4+/CD8+ ratio was 0.03 (IQR = −0.03 to 0.09; P = 0.013 and P < 0.001, respectively). In the subgroup of patients with a CD4+ T-cell count at baseline of less than 200 cells/µL, the median increase was 61.5 cells/µL (IQR = 35.0-106.5; P = 0.002). According to the DTG-based dual therapy, the median increases in CD4+ T-cell count were 27.0, 72.5, and 8.0 cells/µL for DTG plus RPV, DTG plus 3TC, and DTG plus b-DRV, respectively (P = 0.075, 0.029, and 0.686).
Safety and Tolerability
Overall, 8.8% of patients stopped the DTG-based dual therapy before W48, with the appearance of AEs (2.9%) being the most frequent reason. This proportion was 8.7% (2/23) in the subgroup of patients treated with DTG plus 3TC, 2.4% (2/85) in those treated with DTG plus RPV, and 1.7% (1/58) in those treated with DTG plus b-DRV. These toxicity reasons included dizziness and anxiety for DTG plus 3TC, nausea and headache for DTG plus RPV, and myalgia for DTG plus b-DRV; none of them required hospitalization. In 3 patients (60.0%), the AEs resolved after ART discontinuation. In addition, pharmacological interactions were the cause for discontinuation in 4 patients (2.4%): RPV with omeprazole and clomipramine, ATV/r with methadone, and DRV/r with hydrocortisone.
The impact of the regimens in the laboratory values at W48 is shown in Table 3. No significant changes were found in the lipid parameters in the overall population. However, statistically significant reductions were found for triglycerides (TG) and total cholesterol (TC) in the subgroup of patients previously treated with PIs (−20.0 and −2.5 mg/dL, respectively; P = 0.008 and 0.044) but not for low-density lipoprotein cholesterol (LDL; +6 mg/dL, P = 0.539). Conversely, there were no significant increases in the lipid parameters in the subgroup of patients previously treated with TDF. In the subgroup of patients who switched to DTG plus b-DRV, the median increases in LDL and TC were 6.0 (P = 0.163) and 8.5 (P = 0.062) mg/dL, respectively.
Laboratory Values at Baseline and W48 After the Switch to Dolutegravir-Based Dual Therapy.
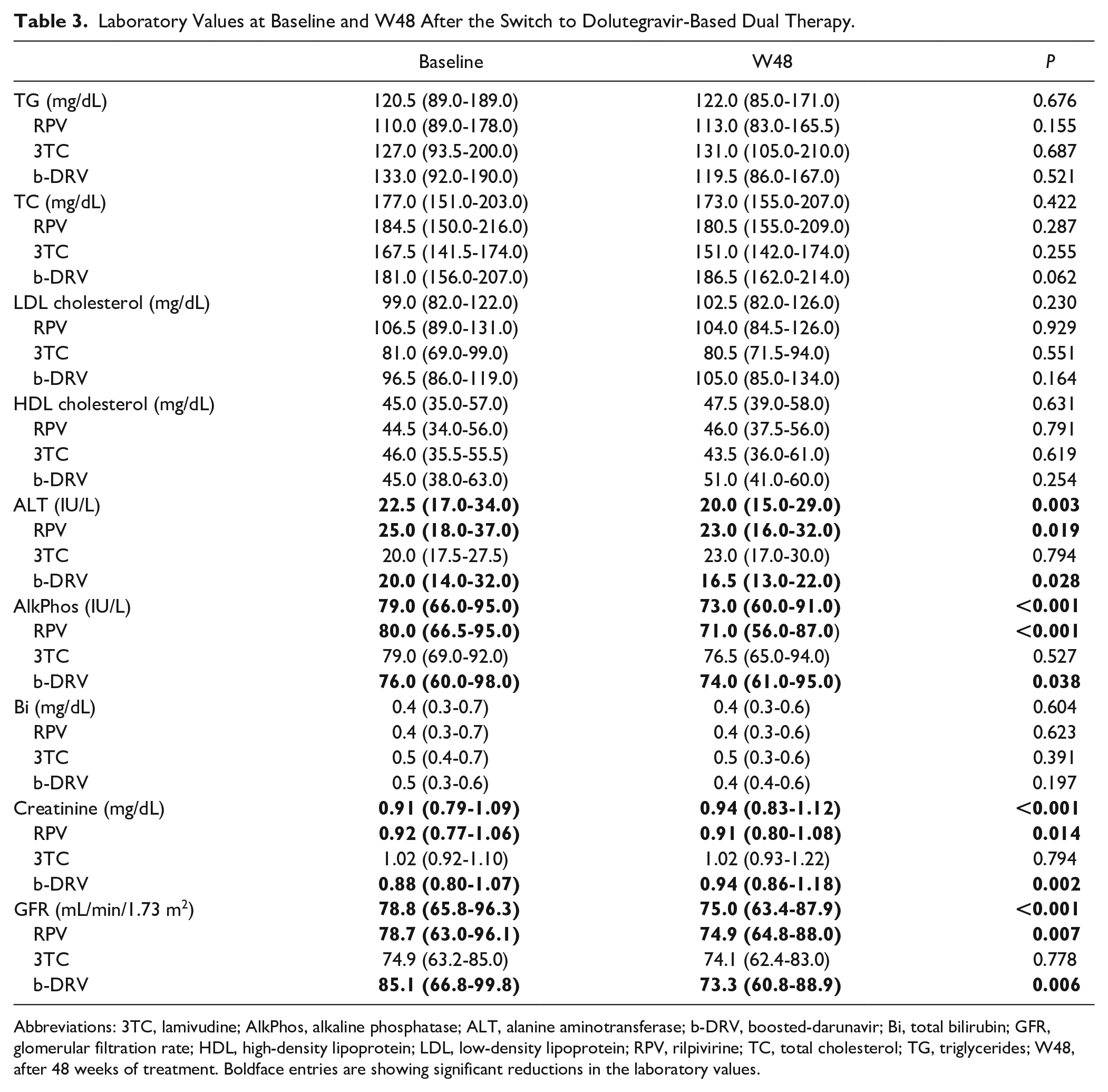
Abbreviations: 3TC, lamivudine; AlkPhos, alkaline phosphatase; ALT, alanine aminotransferase; b-DRV, boosted-darunavir; Bi, total bilirubin; GFR, glomerular filtration rate; HDL, high-density lipoprotein; LDL, low-density lipoprotein; RPV, rilpivirine; TC, total cholesterol; TG, triglycerides; W48, after 48 weeks of treatment. Boldface entries are showing significant reductions in the laboratory values.
Concerning liver function tests, the median changes in alanine aminotransferase and alkaline phosphatase were significant (−2.0 and −4.0 IU/L; P = 0.003 and P < 0.001), but not for bilirubin. When comparing results by the second drug, the differences remained significant for RPV (−2.0 and −6.0 IU/L; P = 0.019, P < 0.001) and b-DRV (−3.0 and −3.0 IU/L; P = 0.028, P = 0.038).
The renal function showed a significant decrease in the median of GFR from baseline to W48 (78.8 to 75.0 mL/min/1.73 m2; P < 0.001). This change was significant in the case of switching to DTG plus RPV and DTG plus b-DRV, with a median change of −4.1 and −5.8 mL/min/1.73 m2, with P =0.007 and P =0.006, respectively.
Pill Burden and ART Adherence
The mean pill burden was reduced from 3.13 (SD = 1.55) to 2.16 (SD = 0.39) in the overall population (P < 0.001). The pill burden prior to the switch was higher in the subgroup of patients treated with DTG plus b-DRV (3.83, SD = 1.74) and DTG plus RPV (3.27, SD = 1.58), compared to DTG plus 3TC (2.28, SD = 0.83).
The median adherence in the year prior to the switch was 97.0% (IQR = 89.0-100.0) and 98.0% (IQR = 94.0-100.0) at W48 after the switch (P = 0.006). The adherence rate was similar between the different DTG-based dual therapies. The proportion of patients who had an adherence <90% was reduced after the switch from 29.4% to 14.2% (P < 0.001). These nonadherent patients were mostly switched to DTG plus DRV (56.3%). The subgroup of participants where we found an improvement in the treatment adherence were those who were taking a twice-daily schedule prior to the switch (n = 85; from 32.9% to 12.5%, P = 0.002) or a regimen based on ≥4 pills per day (n = 85; from 29.9% to 15.7%, P = 0.027). No significant changes were found in patients who had received a previous regimen with 3 pills (n = 84) or a STR (n = 36).
Cost Analysis
The median annual per-patient costs before switching were €5694 (IQR = 5078 to 8878; $6520 [IQR = 5814 to 10 165]) and €7693 (IQR = 5421 to 9308; $8808 [IQR = 6657 to 11 639]) after switching to the DTG-based dual therapy. The annual costs of the different dual therapies were €9780 for DTG plus ATV/ritonavir, €9769 for DTG plus DRV/ritonavir, €9308 for DTG plus DRV/cobicistat, €9221 for DTG plus etravirine, €7693 for DTG plus RPV, and €5421 for DTG plus 3TC. Overall, a median increase of €800 ($916) per patient was calculated (IQR = −1100 to 2605; $916 [IQR = −1260 to 2983]). The greatest increase was found in the subgroup of patients that switched to DTG plus DRV/ritonavir (+€1511, IQR = 783 to 4600, P ≤ 0.001; $1730, IQR = 897 to 5267), followed by DTG plus RPV (+€1119, IQR = −1185 to 2605, P = 0.022; $1281, IQR = −1357 to 2983) and DTG plus DRV/cobicistat (+€800, IQR = −461 to 3614, P = 0.020; $916, IQR = −528 to 4138). In contrast, a small cost reduction was found in those who switched to DTG plus 3TC (−€85, IQR = −1938 to 804, P = 0.783; −$97, IQR = −2219 to 921).
Discussion
We reported the real-life experience with different DTG-based dual therapies in a Spanish cohort of ART-experienced PLWH. To our knowledge, this is the first cohort that describes their increasing incidence since DTG approval as well as the real impact of each combination on patient adherence and ARV costs.
We observed a growing trend in the use of DTG-based dual therapies, with DTG plus RPV being the most frequent combination during 2014-2017. Since 2018, there was a significant increase in DTG plus 3TC. This change is explained by the publication of the favorable results of GEMINI-I and GEMINI-II clinical trials, which demonstrated the equivalence in efficacy of DTG plus 3TC in ART-naive adults compared to the 3-drug regimen composed of DTG plus tenofovir disoproxil fumarate and emtricitabine. 16 These results enhanced its use as a switching strategy in ART-experienced patients, along with other advantages over DTG plus RPV, such as the fewer drug-drug interactions, the lack of need to be taken with a meal, and its lower cost.
Another important finding is the difference in the prescribing profile between the different dual therapies. Whereas DTG plus 3TC was preferably used as a simplification therapy in VS patients with a low incidence of comorbidities, DTG plus RPV was used in heavily treatment-experienced patients with important comorbidities or predisposition to toxicity, who needed metabolic-friendly drugs. In contrast, DTG plus b-DRV was mainly used as salvage therapy in patients with previous VF.
Our study found an effectiveness greater than 95% for the 3 DTG-based dual combinations in VS patients by OT analysis, with no significant differences in the proportion of VF between the different therapies (0%-2.9%). However, by ITT analysis, we found a lower proportion of VS patients who maintained virological suppression with DTG plus RPV (87%), which contrasts with the 95% reported in SWORD-1 and SWORD-2 clinical trials. 5 This was probably a result of the different clinical characteristics of our patients, who were older, with a great number of comorbidities, and heavily pretreated, with a median time since first ART of 19 years compared to 4 years in SWORD-1 and SWORD-2. In addition, 8% of our patients discontinued the therapy before W48 for other reasons, compared to 4% in these clinical trials. Our results are more similar to those reported by Gantner et al 17 who found, in a cohort of 152 VS patients, a rate of virological suppression with DTG plus RPV of 90% at W24. Likewise, Capetti et al 15 reported a rate of virological suppression of 88% at W24 in a cohort of 132 patients, which included 12% of non-VS patients at baseline.
We did not find any VF in the 23 VS patients who switched to DTG plus 3TC and completed 48 weeks of follow-up. In the same line, the ASPIRE clinical trial 8 found a low rate of VF (0.9%) at W24: 0.3% in the randomized TANGO study 6 and 1.0% in the ANRS 167 trial (LAMIDOL). 7 Maggiolo et al 18 reported no VF in a cohort of 94 patients at W24, and Borghetti et al 19 found a rate of virological suppression of 98% at W48. However, we found a higher rate of discontinuations for toxicity reasons (9%) than in the LAMIDOL trial 7 (2%) but similar to the TANGO study 6 (6%).
With respect to DTG plus b-DRV, only 3% of patients experienced VF at W48. Navarro et al 10 reported 98% of virological suppression at W24 in a cohort of 50 VS and heavily treated patients, and Vizcarra et al 11 found no VF in their cohort of 51 patients at W48. We also found a low rate of discontinuations for nonvirological reasons (3%), which was lower than the rate of 8% to 10% reported by Navarro et al 10 and Vizcarra et al. 11
In the subgroup of 30 non-VS patients, the virological suppression rate was lower, being 52% for DTG plus b-DRV and 71% for DTG plus RPV. Resistance testing performed on samples from these patients did not show the emergence of new major drug resistance mutations. There are few experiences in the literature of switching to a DTG dual therapy in non-VS patients, with poor patient selection and heterogeneous populations. 20
Regarding the safety profile, discontinuation for toxicity reasons was observed only in 3% of patients. Although data from other real-life cohorts have suggested that DTG is associated with a higher incidence of neuropsychiatric adverse effects21,22 (insomnia, dizziness, headache, depression) compared with that reported in clinical trials, our rate of discontinuations resulting from these AEs was only 1.8%. Concerning laboratory data, there were no significant changes in the lipid profile. However, statistically significant reductions were found for TG and TC in the subgroup of patients previously treated with PIs (−20.0 and −2.5 mg/dL, respectively). In relation to renal function tests, GFR showed statistically significant decreases for the overall population at W48 (4.5 mL/min/1.73 m2 by MDRD). However, there was no significant difference in the proportion of patients having a GFR <60 mL/min/1.73 m2 from baseline to W48. DTG inhibits the organic cation transporter 2 (OCT2), which affects the active tubular secretion of creatinine, increasing its blood levels and producing a “false” decrease of the estimated GFR. RPV has also been shown to be an inhibitor of OCT2.
In terms of patient adherence to ART, we did not find significant differences between the different dual therapies. Our study shows an improvement after switching to the DTG dual therapy in the subgroups of patients whose previous regimen was based on ≥4 pills per day or on a twice-daily schedule. These results make these combinations an attractive alternative, both to reduce pill burden and to improve adherence in heavily treatment-experienced patients. In contrast, no significant improvements were observed in PLWH who were receiving 3 pills a day, nor a decrease in those with a previous STR.
Finally, cost analysis is particularly important in HIV given the recommendations for immediate initiation of lifelong treatment, the increasing number of patients taking ART, and the high cost of these regimens. This study showed that switching to DTG dual therapies increased the treatment cost in comparison to the previous ART. The annual cost per patient increase of €800 ($916) was obtained because of the higher cost of acquisition of DTG compared to other anchor therapies such as NNRTI and raltegravir. Switching to DTG plus 3TC has proved to be the unique cost-saving option, with a median annual reduction per patient of €85 ($97). However, it should be noted that the generic version of DRV and the STR DTG/RPV were not available at the time of this study, and their lower annual costs (€699 and €5840, respectively [$800 and $6687]) is expected to modify these economic results.
The main limitations of our study are its observational nature, which is prone to bias because of unmeasured confounders, and the short follow-up duration of up to 48 weeks. Second, adherence was calculated using dispensing data records, and it was assumed that each patient took all medications prescribed. Finally, regarding cost analysis, it should be considered that drug prices may differ between countries and their nationally established prices owing to discount negotiated with drug suppliers. Nonetheless, this study has its strengths in the description of the real use of DTG dual therapies (including prevalence and incidence data), in the comparison of the effectiveness of the different options, and in the accurate description of reasons for starting and discontinuing these new therapies and their impact on treatment adherence and costs.
Conclusion and Relevance
The use of DTG-based dual therapies has increased in real life, in particular DTG plus lamivudine, although the reasons for their use vary across the different dual therapies. The combinations of DTG with lamivudine, RPV, or DRV showed a favorable effectiveness and safety profile, with a low rate of VF and interruptions because of toxicity reasons. The costs of these simplified regimes increased with respect to previous therapies, except for DTG plus lamivudine.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.