
Abstract
Background:
Approximately 30% of antimicrobials prescribed in the outpatient setting are unnecessary and up to 50% are inappropriate. Despite this, antimicrobial stewardship (AS) efforts mostly focus on the inpatient setting, and limited data describe AS interventions at hospital discharge. Acknowledging the potential value of discharge AS, we used our existing resources to review discharge oral antimicrobial prescriptions.
Objective:
The primary objective of this retrospective, single-center study was to evaluate the impact of an AS program on discharge oral antimicrobial prescriptions.
Methods
Discharge oral antimicrobial prescriptions sent to our hospital-operated outpatient pharmacy, reviewed by an infectious diseases (ID) pharmacist, and recorded into our data collection tool from September 1, 2020, to February 28, 2021, were evaluated retrospectively. The primary outcome was to identify the frequency a drug-related problem (DRP) was identified by an ID pharmacist. Secondary outcomes included DRP characterization, percentage of prescriptions with interventions, intervention acceptance rate, and reduction in antimicrobial days dispensed at discharge when interventions to limit treatment duration were accepted.
Results:
Of the 803 discharge oral antimicrobial prescriptions reviewed, at least 1 DRP was identified in 43.1% (346/803). The most frequently identified DRPs pertained to treatment duration, drug selection, and dose selection. At least 1 intervention was recommended in 42.8% (344/803) of prescriptions. In total, 438 interventions were made and the acceptance rate was 75.6% (331/438). The most common types of interventions included recommendations for a different duration, a different dose or frequency, and antimicrobial discontinuation. When interventions to reduce treatment duration were accepted, the median (interquartile range) number of antimicrobial days decreased from 8 (5-10) days to 4 (0-5.5) days (P < 0.001).
Conclusion and Relevance:
An ID pharmacist’s review of discharge oral antimicrobial prescriptions sent to our hospital-operated outpatient pharmacy resulted in identification of DRPs and subsequent interventions in a substantial number of prescriptions.
Keywords
Introduction
The Centers for Disease Control and Prevention (CDC) 2020-2025 National Action Plan to Combat Antibiotic-Resistant Bacteria promotes improvement in national outpatient antimicrobial use. 1 Specifically, the plan aims to lower the annual rate of outpatient antimicrobial dispensing per 1000 US population. In 2019, approximately 250 million outpatient antimicrobial prescriptions were prescribed in the United States. 2 The CDC estimates that at least 30% of outpatient antimicrobial prescriptions are unnecessary. When coupled with concerns for suboptimal antimicrobial selection, dosing, and treatment duration, 50% of outpatient antimicrobial prescriptions may be inappropriate.3-6 Currently, most antimicrobial stewardship (AS) efforts focus on the inpatient setting, and few address the extensive opportunities for antimicrobial treatment improvements in the outpatient setting. 7 Hospital AS programs (ASPs) are poised to leverage their access to the hospital electronic medical record (EMR), expertise, and rapport with prescribers to impact discharge prescribing.
In the course of reviewing inpatients through our daily AS activities, our AS team (AST) observed that patients were at times discharged with unnecessarily long courses, or suboptimal doses, of antimicrobials. In addition, patients were not being counseled on potential drug interactions or adverse effects, among other drug-related problems (DRPs). Acknowledging an untapped potential for AS, we used our existing resources to review oral antimicrobial prescriptions sent to our hospital-operated outpatient pharmacy to potentially optimize antimicrobial therapy. The primary objective of this study was to evaluate the impact of an ASP on discharge oral antimicrobial prescriptions.
Methods
Setting
This study was performed at the State University of New York (SUNY) Upstate University Hospital, a 472-bed, level 1 trauma, tertiary care, academic medical center with dedicated medical teams, and 72-bed pediatric hospital, with a well-established ASP and hospital-operated outpatient pharmacy in Syracuse, New York. SUNY Upstate University Hospital has centralized pharmacy distribution with decentralized pharmacy services that cover every patient care area. The pharmacy services component of our ASP structure includes 1.0 full-time equivalent (FTE) for an adult infectious diseases (ID) pharmacist, 1.0 FTE for a pediatric ID pharmacist, a pharmacy school–funded ID pharmacist faculty, and a postgraduate year 2 (PGY-2) ID pharmacy resident. Our adult and pediatric ID pharmacists perform prospective audit with intervention and feedback, and review certain targeted antimicrobials. Cases are discussed daily with the adult and pediatric ID teams. Inpatient AS largely focuses on optimization of empiric therapy selection and de-escalation based on culture results. Care plans are developed with discharge in mind, and some factors prompt following patients through discharge even if prescriptions are routed to external pharmacies. Others are not reviewed after the initial evaluation unless discharge antimicrobials are sent to our outpatient pharmacy. The pharmacy school–funded ID pharmacist faculty, ID PGY-2 pharmacy resident, and pediatric ID pharmacist consistently round with the ID consult services (adult and pediatric). Our ASP is also recognized as an AS Center of Excellence by the Infectious Diseases Society of America.
Discharge Antimicrobial Review Process
An overview of our discharge antimicrobial process is displayed in Figure 1. Specifically, the adult ID pharmacist and pediatric ID pharmacist are the primary reviewers of oral antimicrobial prescriptions sent to our hospital-operated pharmacy for their respective age groups and are assisted by the PGY-2 ID pharmacy resident and the ID pharmacist faculty as needed. The outpatient pharmacy uses the secure chat function within our EMR to contact an ID pharmacist to review discharge antimicrobial prescriptions for inpatients Monday-Friday from 8:00
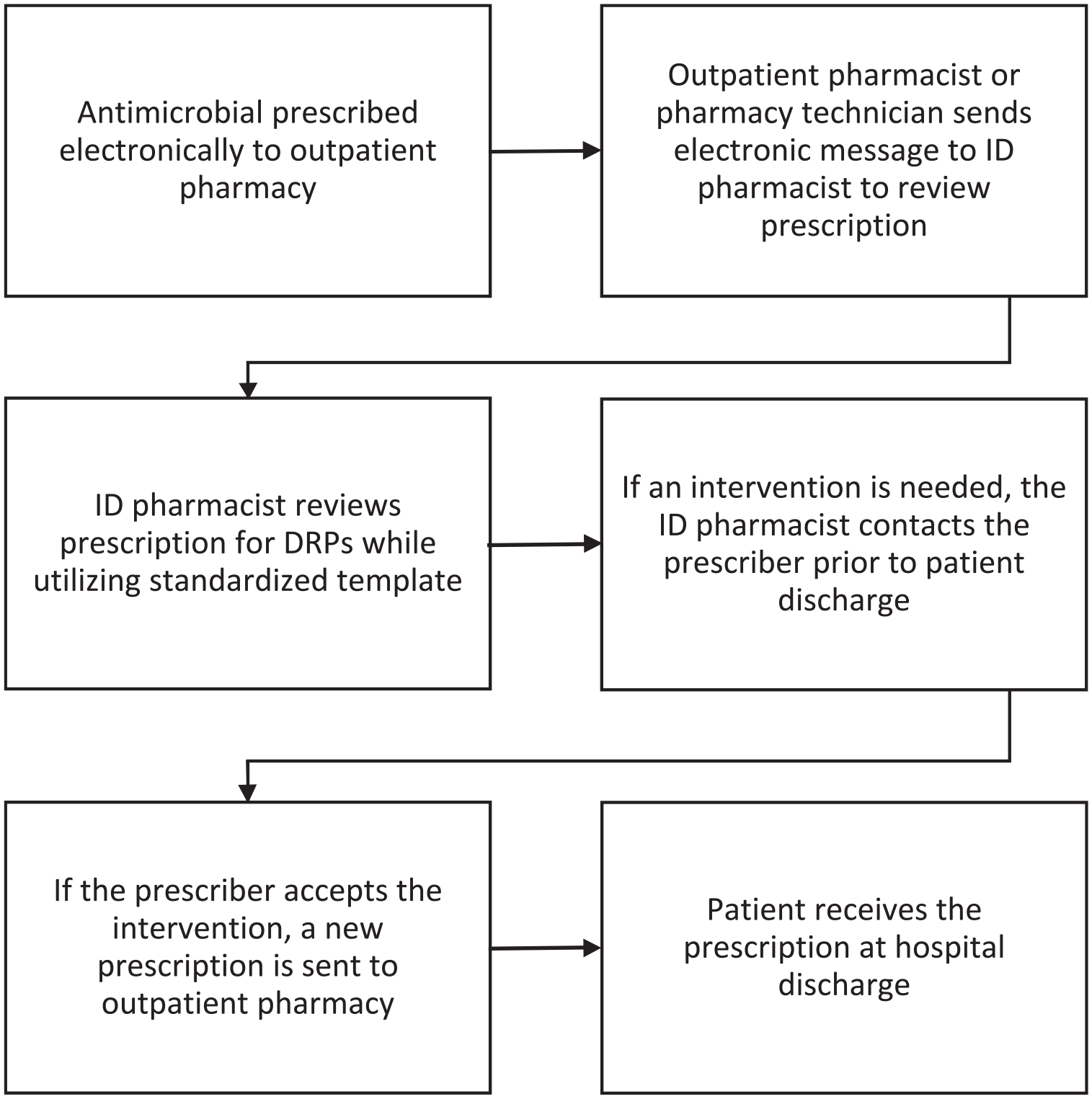
Discharge antimicrobial review process.
Oral antimicrobial prescriptions reviewed by the ID pharmacist were logged into a confidential database using a standardized data collection tool in REDCap for the purpose of quality improvement.12,13 The Pharmaceutical Care Network Europe (PCNE) Classification Version 9.1 was referenced to characterize DRPs and associated interventions in the standardized template. 14 The PCNE Classification Version 9.1 is a validated tool to classify and document DRPs.
Study Design and Patient Population
This was a single-center, retrospective, descriptive study. Oral antimicrobial prescriptions sent to our hospital-operated outpatient pharmacy, reviewed by an ID pharmacist, and recorded into the REDCap data collection tool from September 1, 2020, to February 28, 2021, were evaluated. Both adult and pediatric patients were included. The primary outcome was the frequency a DRP was identified by an ID pharmacist while reviewing discharge oral antimicrobial prescriptions. Secondary outcomes included characterization of DRPs using the PCNE Classification tool, percentage of prescriptions reviewed with ID pharmacist interventions, the intervention acceptance rate by the provider, and reduction in antimicrobial days dispensed at discharge when interventions to limit treatment (including antimicrobial discontinuation) were accepted. The reduction in antimicrobial days dispensed was assessed by comparing the oral antimicrobial duration prescribed before and after the ID pharmacist’s intervention. This study was deemed exempt by the SUNY Upstate Medical University Institutional Review Board.
Data Collection
Collected data included prescribing service, consulting service if applicable, oral antimicrobial prescribed, antimicrobial indication, day(s) of therapy prescribed, day(s) of antimicrobial therapy received while hospitalized, DRP category based on PCNE Classification, intervention category, intervention acceptance, recommended modifications by the AST (including modifications to antimicrobial selection and duration of therapy), and the estimated time spent by the ID pharmacist on the review of the antimicrobial prescription. Data were intermittently reviewed by a second reviewer to ensure consistency and accuracy within the data collection process and to resolve any data-related inquiries.
Statistical Analyses
All data are presented using descriptive statistics including number and percentage, mean and standard deviation (SD), and median and interquartile range (IQR). The reduction in antimicrobial days dispensed was assessed by comparing the oral antimicrobial duration prescribed before and after the ID pharmacist’s intervention using the Wilcoxon signed-rank test. This was a 2-tailed test, and a P value <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, New York).
Results
In total, 803 discharge oral antimicrobial prescriptions were reviewed by an ID pharmacist from September 1, 2020, to February 28, 2021. Table 1 shows the characteristics of the antimicrobial prescriptions that were reviewed. Most prescriptions were prescribed by the adult medicine service (466/803, 58.0%), followed by general pediatrics (122/803, 15.2%) and surgery (92/803, 11.5%). In 25.4% (204/803) of prescriptions, the antimicrobial prescribed was recommended by a consult service, most commonly the ID service (130/803, 16.2%) followed by the Ear, Nose, and Throat (ENT) service (25/803, 3.1%). The most frequently prescribed discharge antimicrobials included amoxicillin-clavulanic acid (145/803, 18.1%), cephalexin (124/803, 15.4%), and sulfamethoxazole-trimethoprim (111/803, 13.8%). Prophylaxis was the most frequent indication (168/803, 20.9%). Other frequent indications included skin and soft tissue infection (159/803, 19.8%), urinary tract infection (120/803, 14.9%), intra-abdominal infection (120/803, 14.9%), and pneumonia (99/803, 12.3%).
Discharge Antimicrobial Prescription Characteristics.
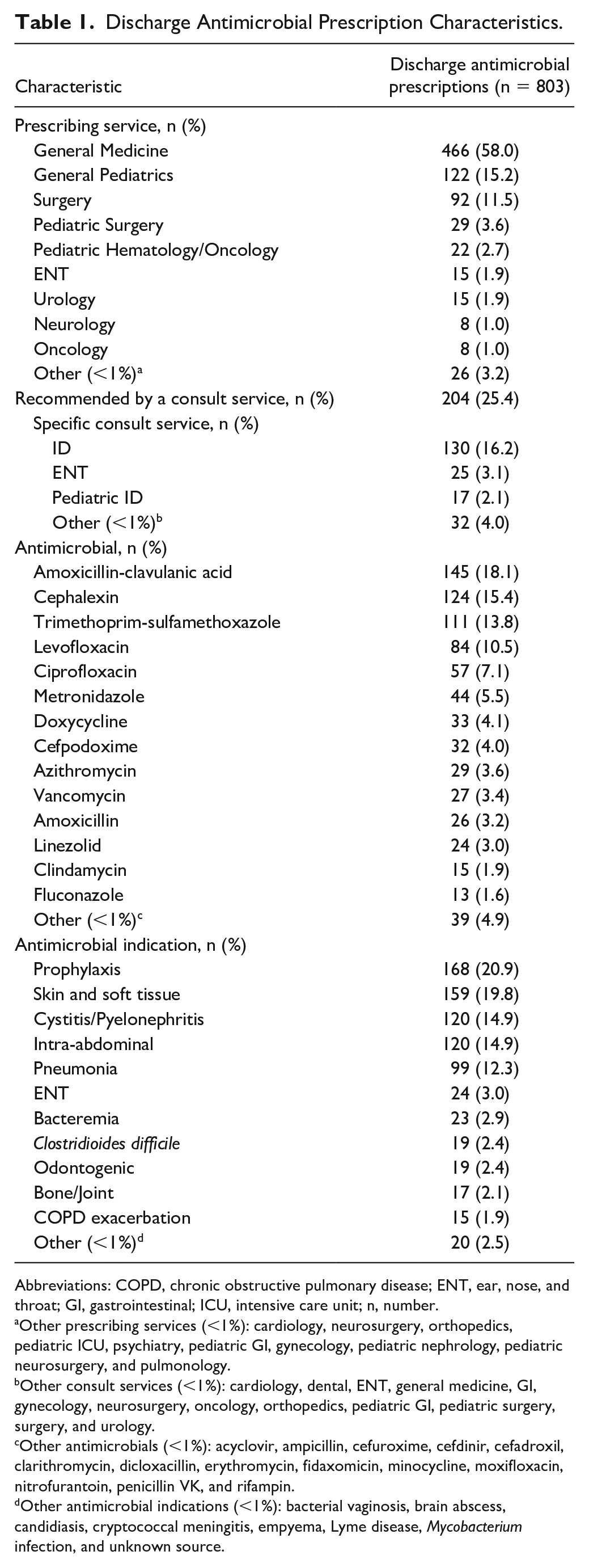
Abbreviations: COPD, chronic obstructive pulmonary disease; ENT, ear, nose, and throat; GI, gastrointestinal; ICU, intensive care unit; n, number.
Other prescribing services (<1%): cardiology, neurosurgery, orthopedics, pediatric ICU, psychiatry, pediatric GI, gynecology, pediatric nephrology, pediatric neurosurgery, and pulmonology.
Other consult services (<1%): cardiology, dental, ENT, general medicine, GI, gynecology, neurosurgery, oncology, orthopedics, pediatric GI, pediatric surgery, surgery, and urology.
Other antimicrobials (<1%): acyclovir, ampicillin, cefuroxime, cefdinir, cefadroxil, clarithromycin, dicloxacillin, erythromycin, fidaxomicin, minocycline, moxifloxacin, nitrofurantoin, penicillin VK, and rifampin.
Other antimicrobial indications (<1%): bacterial vaginosis, brain abscess, candidiasis, cryptococcal meningitis, empyema, Lyme disease, Mycobacterium infection, and unknown source.
Table 2 displays the DRP characteristics. At least 1 DRP was identified in 43.1% (346/803) of prescriptions reviewed. In total, 457 DRPs were identified in 803 oral antimicrobial prescriptions. The most frequent DRP classifications identified were treatment duration (164/457, 35.9%), drug selection (161/457, 35.2%), and dose selection(92/457, 20.1%). Supplementary Table 1 displays pediatric-specific DRP characteristics. For pediatric patients, at least 1 DRP was identified in 55.5% (111/200) of prescriptions. In total, 168 DRPs were identified in 200 pediatric oral antimicrobial prescriptions. The most common DRP classification for pediatric patients was treatment duration (66/168, 39.3%), followed by dose selection (42/168, 25%), drug selection (34/168, 20.2%), drug form (14/168, 8.3%), and dispensing (12/168, 7.1%).
Drug-Related Problems and Intervention Characteristics.
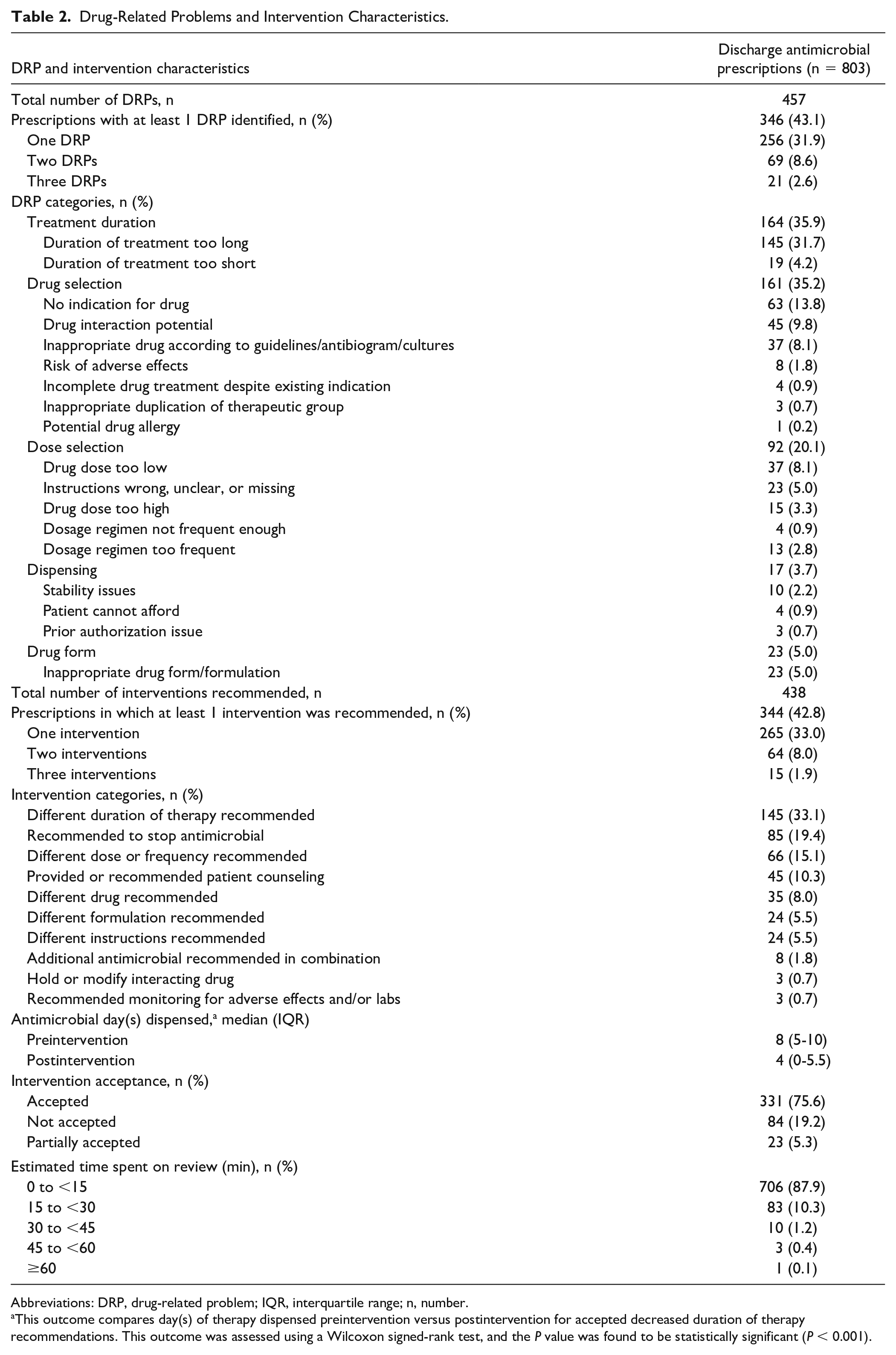
Abbreviations: DRP, drug-related problem; IQR, interquartile range; n, number.
This outcome compares day(s) of therapy dispensed preintervention versus postintervention for accepted decreased duration of therapy recommendations. This outcome was assessed using a Wilcoxon signed-rank test, and the P value was found to be statistically significant (P < 0.001).
Table 2 also displays the intervention characteristics. At least 1 intervention was recommended in 42.8% (344/803) of reviewed discharge antimicrobial prescriptions. In total, 438 interventions were recommended. The most common types of interventions included recommendations for a different duration (145/438, 33.1%), a different dose or frequency (66/438, 15.1%), and to discontinue the antimicrobial (85/438, 19.4%). The intervention acceptance rate was 75.6% (331/438). Most (706/803, 87.9%) of the discharge antimicrobial reviews took less than 15 minutes. When recommendations to reduce the treatment duration were accepted, the median (IQR) number of antimicrobial days decreased from 8 (5-10) days to 4 (0-5.5) days (P < 0.001).
Discussion
Discharge antimicrobial prescribing is infrequently addressed by inpatient ASPs despite the apparent need for AS interventions at hospital discharge.3-7 Discharge AS remains an important gap in the literature, and few studies are available to describe AS interventions in this area.15-18 Given that several studies have demonstrated the need for improved antimicrobial prescribing at transitions of care, we sought to create a streamlined process to identify antimicrobial DRPs encountered at hospital discharge. Using existing resources, our AST was successful in identifying DRPs in more than 40% of oral discharge antimicrobial prescriptions reviewed during a 6-month period. This finding aligns with the CDC’s estimates that at least 30% of antimicrobials prescribed in the outpatient setting are unnecessary and approximately 50% may be inappropriate.3-6 Our results highlight the importance of AS during transitions of care.
Few studies have described AS efforts at discharge and their impact on antimicrobial prescribing.15-19 Most studies focus on antimicrobial appropriateness before and after AS intervention, although intervention strategies vary between studies. Yogo et al performed a quasi-experimental, retrospective cohort study that used an institutional guideline with recommendations for oral step-down therapy and treatment duration in conjunction with prospective audit with real-time feedback to prescribers. 15 The preintervention cohort included 300 cases and the postintervention cohort included 200 cases. The median (IQR) duration prescribed at hospital discharge was reduced from 6 (4-10) days in the preintervention period to 5 (3-7) days (P = 0.003) in the post-intervention period. In a random sample of 100 cases, overall prescription appropriateness was 52% (26/50) and 66% (33/50) in the preintervention and postintervention cohort, respectively (P = 0.15).
Chavada et al performed a retrospective cohort study of hospitalized patients to assess the appropriateness of prescriptions after AS intervention. 16 The intervention consisted of discharge advice written in the EMR by the AST as part of their routine inpatient AS activities. The AST made interventions in 46 prescriptions, which were compared with 217 prescriptions with no AST intervention. When the AST performed interventions, antimicrobial selection, duration, and frequency were more likely to be appropriate.
Zampino et al performed a quasi-experimental study to determine the impact of pharmacist-driven AS on appropriateness of antimicrobial therapy prescribed at discharge. 17 The discharge AS pharmacist manually reviewed the EMR to identify patients with a discharge order for antimicrobials and provided recommendations to the medical team if the prescription was inappropriate. The preintervention and postintervention cohorts both included 61 patients. Appropriate prescribing based on guideline recommendations improved from 47.5% (29/61) to 85.2% (52/61) (P < 0.001).
Barnett et al performed a single-center, retrospective cohort study to evaluate the appropriateness of discharge antimicrobial prescriptions. 18 The AST reviewed 929 patients discharged on oral antimicrobials and made interventions on 9.7% (90/929) of prescriptions. Antimicrobial prescriptions were reviewed twice weekly, and as a result, 58% (52/90) of interventions were not implemented in a timely manner. For these cases, the intervention was aimed at educating the discharge provider. For the remaining interventions, 58% (22/38) were accepted by providers.
Finally, Daniels and Weber performed a systematic review assessing interventions to improve antimicrobial prescribing at hospital discharge. 19 However, only a few studies were identified for inclusion (n = 6). The authors concluded that AS interventions focused on improving discharge antimicrobial prescribing need further study.
Unlike other studies, ours did not focus on antimicrobial appropriateness, but rather the potential for DRPs. We chose this outcome because antimicrobial appropriateness may be subjective depending on a number of factors including the patient’s initial clinical response, local susceptibility rates, the organism’s minimum inhibitory concentration, and potential for adverse effects to antimicrobial therapy. We also sought to characterize the type of DRPs and the prescribing services that required frequent interventions to target potential quality improvement endeavors. We were surprised to observe that the largest percentage of antimicrobial prescriptions were for prophylaxis. Often, these prescriptions were for prophylaxis of infections such as Pneumocystis jirovecii or Toxoplasma gondii in susceptible patient populations or for prophylaxis of bacterial infections in high-risk neutropenic patients. However, we identified numerous adult and pediatric patients, particularly those with traumatic injuries or surgical procedures, who were prescribed antimicrobial prophylaxis for durations longer than recommended in clinical guidelines or when not indicated.20,21 Minimizing these prescribing practices with formal, evidence-based education is a future target and goal of our ASP. Thus far, we have met with our institution’s ENT services to discuss antimicrobial prophylaxis following traumatic facial fractures, we discussed stopping routine discharge antimicrobial prophylaxis following implantable cardiac device placement with our institution’s Cardiology services, and we continue to address prolonged discharge antimicrobial prophylaxis following endoscopic retrograde cholangiopancreatography at our monthly AS meetings and with our institution’s gastroenterology services. We have also addressed EMR-specific problems such as pre-established directions or durations that were not appropriate for all patients that contributed to DRPs. Examples of these included default azithromycin “Z-pak” instructions and default sulfamethoxazole-trimethoprim 10-day duration.
Like other investigators, we found excessive antimicrobial duration as a common DRP (145/457, 31.7%) for both adult and pediatric patients. In many cases, additional treatment at discharge was not required, as the patient had completed an appropriate antimicrobial course while hospitalized. When providers accepted the recommendation to either shorten the duration or stop the antimicrobial, we found a statistically significant reduction in antimicrobial days from the original prescription. In addition, of the 84 interventions that were not accepted by providers, 73 of these interventions fell into the “different duration of therapy recommended” or “recommended to stop antimicrobial” categories. If these interventions were accepted, there may have been potential to further reduce the median antimicrobial days dispensed at discharge.
Using the PCNE Classification for DRPs, we were able to identify the potential for drug interactions and the need for counseling in a significant number of adult and pediatric patients. Previous studies have not assessed the potential for drug interactions or need for counseling to avoid the drug interaction such as chelation of fluoroquinolones and tetracyclines with polyvalent cations. In our study, nearly 10% of DRPs identified were related to the potential for drug interactions.
While other studies have excluded patients followed by the ID consult service, we chose to include these patients and found that our inpatient ID consult services (adult and pediatric) recommended 18.3% (147/803) of antimicrobial prescriptions we reviewed. The ID consult service does not write any inpatient or discharge orders, and it is the primary team’s responsibility to prescribe any discharge oral antimicrobial prescriptions recommended by the ID consult service. Interestingly, we identified DRPs in 32.7% (48/147) of these antimicrobial prescriptions, many of which were due to prescriptions being written for durations or doses that were not consistent with ID consult service recommendations. This highlights the importance of reviewing discharge antimicrobial prescriptions even for those patients seen by the ID consult service.
Finally, we were able to use the existing framework of our ASP to integrate the review of antimicrobial prescriptions sent to our hospital-operated outpatient pharmacy. Communication was facilitated between key personnel by using a secure chat function within our EMR that allowed for the majority of reviews to take place in less than 15 minutes. Other studies have not assessed the time required to perform discharge AS. Our system has several pre-established efficiencies including using our hospital-operated outpatient pharmacy to trigger review from the AST, which obviates the need to manually review patients’ records to identify those being discharged on antimicrobials. We also coordinate with our discharge pharmacists to provide counseling to select patients, especially when there is a concern for drug interactions due to chelation. We also found that many of the patients reviewed at discharge had already had empiric therapy reviewed and assessed as part our inpatient AS activities, thereby expediting the review of antimicrobials prescribed at discharge.
Our study did have some important limitations aside from the single-center, retrospective study design. Our AS discharge process may limit the generalizability of our results to other institutions, particularly for those without a hospital-operated outpatient pharmacy. Our discharge antimicrobial review process includes reviewing oral antimicrobial prescriptions sent to our hospital-operated outpatient pharmacy and does not include reviewing those sent to other pharmacies. During the study period, an average of 45.2% of discharged patients per month used our hospital-operated outpatient pharmacy. This is a limitation of our study as we did not assess all oral discharge antimicrobial prescriptions at our institution. In addition, the ID pharmacists were allowed sufficient time to review antimicrobial prescriptions before they had to be filled, which may not be the case with other outpatient pharmacy models. Also, our outpatient pharmacy was the trigger for the AST antimicrobial review; identifying discharge antimicrobials to review may be more difficult if institutions do not have a similar process. The secure chat function within our EMR was instrumental in communicating with the outpatient pharmacy and providers, which led to a high degree of efficiency. Institutions without this ability may be less efficient. Also, many of the interventions pertaining to unnecessary antimicrobial prophylaxis were in trauma patients, which may not apply to institutions that are not level I trauma centers. Finally, we did not assess any clinical outcomes as this was outside the scope of this study.
Conclusion and Relevance
An ID pharmacist’s review of oral antimicrobial prescriptions sent to our hospital-operated outpatient pharmacy resulted in identification of DRPs and subsequent interventions in a substantial number of prescriptions. Interventions were accepted by prescribers at a high frequency. Finally, antimicrobial days dispensed were significantly decreased versus antimicrobial days initially prescribed when prescribers accepted interventions to limit antimicrobial treatment duration. The development of a discharge oral AS review process may help identify institution-specific DRPs which could be addressed by ASPs and quality improvement endeavors. Our study highlights the importance of AS efforts at hospital discharge to identify DRPs and the need for future research in this area.
Supplemental Material
sj-docx-1-aop-10.1177_10600280211052677 – Supplemental material for Hospital Discharge: An Opportune Time for Antimicrobial Stewardship
Supplemental material, sj-docx-1-aop-10.1177_10600280211052677 for Hospital Discharge: An Opportune Time for Antimicrobial Stewardship by Katie A. Parsels, Wesley D. Kufel, Jeni Burgess, Robert W. Seabury, Rahul Mahapatra, Christopher D. Miller and Jeffrey M. Steele in Annals of Pharmacotherapy
Footnotes
Acknowledgements
We would like to acknowledge the SUNY Upstate Outpatient Pharmacy for their significant contribution to the discharge antimicrobial review process.
Authors’ Note
Conference Presentations: This project is being presented as a poster at the virtual IDWeek 2021 Conference in September 2021.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Wesley D. Kufel has served on the advisory board for Theratechnologies, Inc. and has received research grant funding from Merck and Melinta Therapeutics. Jeffrey M. Steele has served on the advisory board for Paratek Pharmaceuticals. All other authors have nothing to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.