
Abstract
Patients with rheumatoid arthritis (RA) experience pain from inflammation, joint destruction, and neuropathy. Antidepressants may play a role among patients with RA and depression, fibromyalgia, or neuropathy to achieve desired outcomes. This commentary evaluated evidence for medications individually and identified important variables for future research. While we await the results of well-designed studies, a trial of duloxetine or milnacipran may be considered for patients with remnant pain and RA remission. Research is needed to evaluate the efficacy and safety of serotonin–norepinephrine reuptake inhibitors and tricyclic antidepressants in patients with RA and associated comorbid conditions.
Keywords
Introduction
Rheumatoid arthritis (RA) affected approximately 1.4 million adults in the United States, in 2014. 1 These patients experience pain due to complex interactions between joint inflammation, altered pain processing, and autoimmune pathologies. 2 Patients with RA may perceive pain through stimulation of peripheral nociceptors, inflammatory factors, joint destruction, increased peripheral and central pain sensitization, and neuropathy, exacerbated by psychological distress and depression. 3
An estimated 40% of patients with RA met criteria for the diagnosis of depression and approximately 25% of patients had moderate or worse depression severity.4,5 It is suggested that effective treatment of RA with disease modifying antirheumatic drugs (DMARDs) alone was unlikely to improve mental health outcomes. 6 History of depression, current depressive symptoms, and baseline pain have been identified as predictors of RA pain intensity and worse depression was associated with less improvement in pain.3,7-9 Additionally, worse depression was associated with worse pain at baseline and at 1-year follow-up. 9 Given the relationship between pain and depression, it is crucial to examine pain response to treatments for RA in the context of comorbid depression.
Approximately 70% of patients with RA despite statistically significant improvement in various measures of disease severity after recommended treatment, reported pain management to be a significant concern 1 year later. 10 This may occur as 1 in 4 patients with RA may have comorbid fibromyalgia, 11 while other studies have noted up to three-fourths of patients with RA may experience neuropathy.12,13 Despite the high prevalence of comorbid conditions (depression, fibromyalgia, neuropathy) that may influence pain outcomes and respond to specific antidepressant therapies, 1 review recommended against the use of antidepressants for pain in RA and another suggested there was low to moderate quality evidence for antidepressant medications to treat depression among patients with RA.14,15 One review indicated that the results from the available trials could not be used to make recommendations for antidepressants medications as a class; no recommendation was made for the use of individual antidepressants. However, given that antidepressants such as serotonin-norepinephrine reuptake inhibitors (SNRIs) are utilized to treat neuropathy, depression, and fibromyalgia, it is important to assess the published evidence for each medication individually to judiciously determine their place in therapy among patients with RA. In addition, new research has been published evaluating specific antidepressants among patients with RA since the publication of the previous reviews. The purpose of this commentary is to highlight the findings and limitations of research examining antidepressant therapies among patients with RA, provide recommendations for their use among patients with RA to treat pain and depression, and suggest important considerations for future research to assess the effectiveness of antidepressants among patients with RA.
Key Limitations of Findings From Existing Studies as a Group
Ten studies have been published assessing the effects of antidepressant medications on pain control and/or depression severity among patients with RA. Medications examined included amitriptyline,16-18 trimipramine, 19 imipramine, 20 milnacipran, 21 sertraline, 22 dotheipin,23,24 and duloxetine 25 (Tables 1 and 2). Among these studies only 4 specifically targeted patients with RA and depression in the inclusion criteria,17,19,22,23 seven assessed change in mental health outcome measures,17-20,22-24 none accounted for diagnosis of comorbid fibromyalgia or neuropathy, and 1 assessed change in fibromyalgia symptom severity. 21 Additionally, only 2 studies reported if patients were in disease remission or well controlled inflammation.21,25 One study titrated antidepressant therapy based on clinical efficacy. 20 These variables are of significant importance given the relationship between pain and comorbid depression, neuropathy, and fibromyalgia among patients with RA. Finally, only six studies utilized a medication and dose sufficient for the treatment of neuropathic pain or fibromyalgia16-18,20,21,25 and six utilized a dose sufficient to treat depression.17,19,21-23 Duration of illness was only reported in 5 studies.20-24 No study utilized any scale to determine the baseline or treatment effect for neuropathic pain or assessed medication adherence. Tables 1 and 2 contain key details for various studies and antidepressants assessed.
Summary of Characteristics of Studies Assessing Antidepressants Among Patients With RA. (N:10).
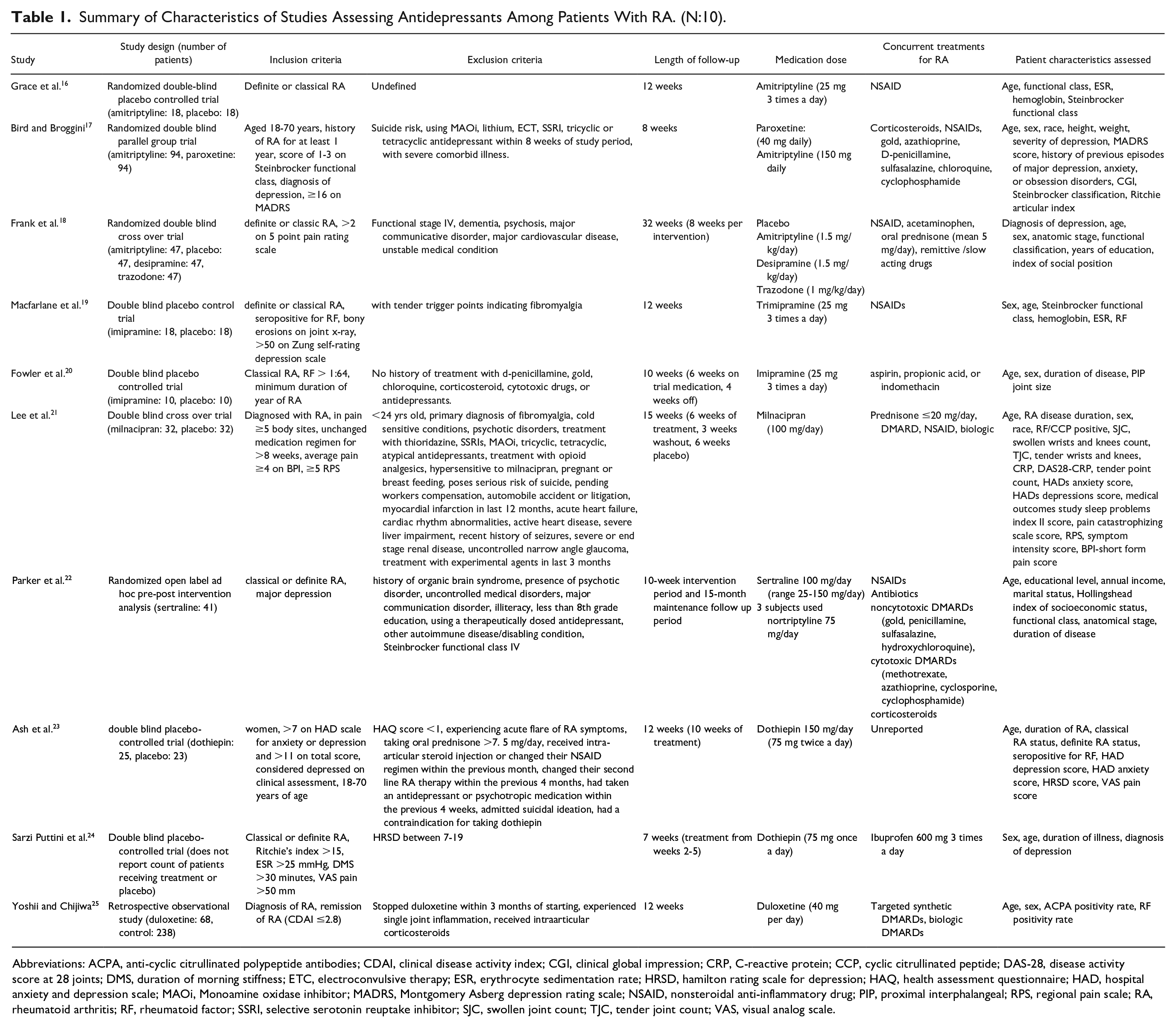
Abbreviations: ACPA, anti-cyclic citrullinated polypeptide antibodies; CDAI, clinical disease activity index; CGI, clinical global impression; CRP, C-reactive protein; CCP, cyclic citrullinated peptide; DAS-28, disease activity score at 28 joints; DMS, duration of morning stiffness; ETC, electroconvulsive therapy; ESR, erythrocyte sedimentation rate; HRSD, hamilton rating scale for depression; HAQ, health assessment questionnaire; HAD, hospital anxiety and depression scale; MAOi, Monoamine oxidase inhibitor; MADRS, Montgomery Asberg depression rating scale; NSAID, nonsteroidal anti-inflammatory drug; PIP, proximal interphalangeal; RPS, regional pain scale; RA, rheumatoid arthritis; RF, rheumatoid factor; SSRI, selective serotonin reuptake inhibitor; SJC, swollen joint count; TJC, tender joint count; VAS, visual analog scale.
Outcomes of Studies Assessed in This Commentary.
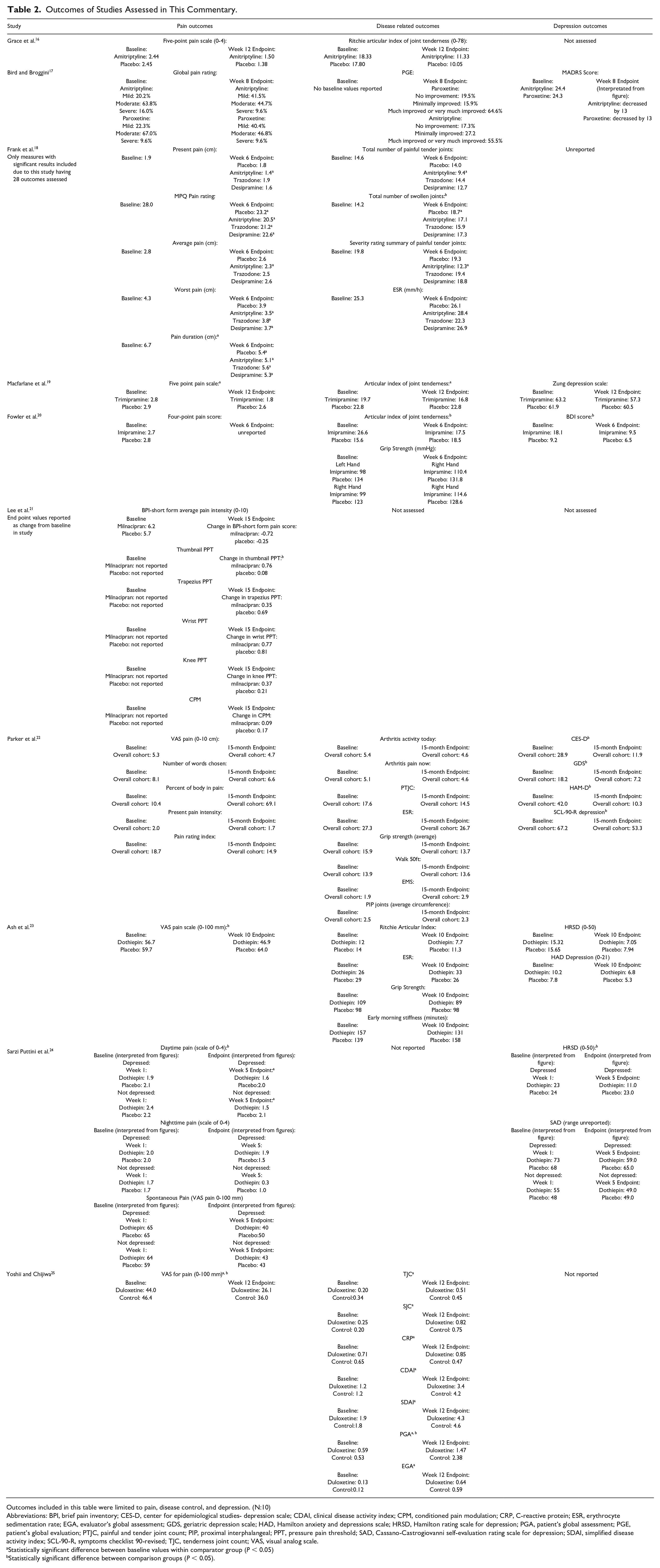
Outcomes included in this table were limited to pain, disease control, and depression. (N:10)
Abbreviations: BPI, brief pain inventory; CES-D, center for epidemiological studies- depression scale; CDAI, clinical disease activity index; CPM, conditioned pain modulation; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; EGA, evaluator’s global assessment; GDS, geriatric depression scale; HAD, Hamilton anxiety and depressions scale; HRSD, Hamilton rating scale for depression; PGA, patient’s global assessment; PGE, patient’s global evaluation; PTJC, painful and tender joint count; PIP, proximal interphalangeal; PPT, pressure pain threshold; SAD, Cassano-Castrogiovanni self-evaluation rating scale for depression; SDAI, simplified disease activity index; SCL-90-R, symptoms checklist 90-revised; TJC, tenderness joint count; VAS, visual analog scale.
Statistically significant difference between baseline values within comparator group (P < 0.05)
Statistically significant difference between comparison groups (P < 0.05).
Potential Role of Individual Antidepressants in RA Treatment
Amitriptyline
Three studies determined the effects of amitriptyline on pain and/or depression outcomes on patients with RA.16-18 Grace et al. 16 found no significant difference in pain outcomes among patients receiving only amitriptyline (25 mg 3 times daily) and nonsteroidal anti-inflammatory drugs (NSAIDs) as needed, compared to placebo. Patients in this study were not evaluated for comorbid depression, did not utilize other treatments including DMARDs for RA, and the dose utilized may have been insufficient to treat comorbid depression (recommended dose 100-300 mg/day). 26 While the dose may have been sufficient to treat fibromyalgia (25-50 mg/day) 27 or neuropathy (titrated up to 150 mg/day), 28 patients may have been experiencing uncontrolled inflammation given they did not receive any DMARD.
Bird and Broggini, 17 however, found amitriptyline, utilizing a dose generally used to treat depression, 26 produced similar improvements in depression, quality of life, and pain severity compared to paroxetine among patients with RA and comorbid depression. It is important to note, changes in measures of disease control were not reported nor was disease severity evaluated as a confounder.
Finally, Frank et al. 18 compared the effects of amitriptyline, desipramine, and trazodone using weight-based dosing to assess change in pain, mood, and disease control among patients with RA. Amitriptyline was associated with significant improvement in worst pain felt, pain intensity, and total number of painful joints compared to placebo and baseline. No significant differences between baseline and placebo were observed in any treatment cohort regarding measures of pain or disease control. In addition, measures of depression severity were not used in this study; thus, it is unclear how depression severity influenced outcomes.
Trimipramine
Macfarlane et al. 19 studied trimipramine (25 mg 3 times daily) among patients with RA and comorbid depression compared to placebo. Patients with trimipramine compared to placebo experienced significant improvements in pain and reduction in the number of tender joints, but depression did not improve significantly. Trimipramine, indicated for the treatment of major depressive disorder, however, is generally given at the dose of 75-300 mg daily. 26 Thus, certain patients in this study may have received subtherapeutic doses. Additionally, patients in this study were only using NSAIDs and no DMARD to treat RA. Patients suspected of having fibromyalgia were excluded given investigators considered the medication of proven benefit among patients with this disease.
Imipramine
Fowler et al. 20 conducted a double-blind placebo-controlled trial to determine the effects of imipramine (25 mg 3 times daily) on rheumatoid factor titers. While a significant improvement in depression severity and number of inflamed or tender joints in the treatment group were observed, depression severity nor disease severity were matched at the beginning of the study and patients were only utilizing aspirin, indomethacin, or propionic acid and no DMARD to treat RA. Significant differences in pain were not observed. It is important to note the recommended dose of imipramine for depression is 100-300 mg/day; 26 it is not recommended in fibromyalgia 27 and is typically used with gabapentin for neuropathic pain. 28
Dothiepin
Ash et al. 23 studied the use of dothiepin (150 mg once daily) in 48 women with RA and symptoms of anxiety and/or depression. This medication is only indicated to treat depression using a dose up to 200 mg per day. 29 Dothiepin was found to significantly reduce pain in comparison to placebo. However, no significant improvement in depression was observed compared to placebo. It should be noted, the dothiepin cohort had higher depression severity at the start of the study and use of medications to treat RA were not reported. 23
Sarzi Puttini et al. 24 studied the effects of dothiepin versus placebo among patients with and without depression. Individuals were only given ibuprofen (1800 mg daily) for treatment of RA. At the end of 5 weeks, a significant improvement in pain and depression was observed in favor of dothiepin among patients with depression. Patients in both studies were not matched for markers of inflammation in comparative cohorts.23,24 This medication is currently not approved by the United States Food and Drug Administration.
Duloxetine
Yoshi and Chijwa 25 compared patients treated with duloxetine (up to 40 mg/day) for the treatment of remnant pain after RA disease remission versus a cohort that used acetaminophen, tramadol, or NSAIDs. After 12 weeks, duloxetine led to significantly greater improvements in pain when compared to the control cohort. While the results demonstrated duloxetine significantly reduced pain among patients with controlled RA, important details such as concomitant medications to treat RA were not reported. Whether patients had depression, fibromyalgia or neuropathy was not mentioned. Additionally, patients in the duloxetine cohort experienced significant increases in markers for inflammation despite reporting lower levels of pain after 12 weeks. Duloxetine may be used in doses up to 60 mg/day for neuropathy 28 and fibromyalgia, 27 and between 60 and 120 mg/day to treat depression. 26
Milnacipran
Lee et al. 21 assessed the effects of milnacipran (50 mg twice daily) compared to placebo on patients with RA who presented with pain at greater than 5 body sites. Patients in this cohort generally, were without depression or anxiety. Significant improvement in pain was not observed. A subgroup analysis found pain significantly decreased among those with RA with less than one swollen joint, suggesting milnacipran was effective among patients with sufficient disease control. However, while milnacipran, indicated for treatment of fibromyalgia (50 mg twice daily), 30 was found to reduce pain severity in this cohort, it was not associated with a significant decrease in the symptom intensity scale, 31 a measure of fibromyalgia symptoms. Patients with a primary diagnosis of fibromyalgia were excluded from this study. It is also important to note, in the cohort of patients with controlled RA, pain severity was higher prior to treatment compared to placebo.
Sertraline
A post hoc analysis conducted by Parker et al 22 determined the effects of sertraline (titrated to effective dose, average 100 mg/day) in a cohort of patients with RA and major depression over a 15-month period. A secondary analysis compared the effects of sertraline in this cohort to a nonrandomized cohort that declined receipt of sertraline. Use of sertraline was associated with significant improvements in various measures of depression and was associated with lower levels of depression over time when compared to the no treatment cohort. It did not detect an improvement in pain or disease severity. Sertraline is indicated for depression (recommended dose 50-200 mg/day) 26 but not for the treatment of neuropathic pain or fibromyalgia, 32 components of RA pain. 23
Which Antidepressants Should Be Used for Pain and Depression in RA?
Despite the numerous factors relevant to the effective management of pain and depression among patients with RA, few clinical studies have effectively evaluated the use of antidepressants among patients with RA. Furthermore, while there are multiple medications indicated to treat chronic pain related to altered central pain processing or neuropathy, only duloxetine and milnacipran have been studied in recent years for the treatment of pain among patients with RA.
Studies have demonstrated that antidepressants at appropriate doses may lead to significant improvements in depression severity in patients with RA and depression. However, defining a clear role of antidepressant medications to treat pain requires greater scrutiny. The data assessing the effects of trimipramine, 19 imipramine, 20 or dothiepin23,24 cannot be effectively applied to today’s population of patients with RA as these patients were not utilizing DMARDs. It is likely these patients were not in RA disease remission or with controlled inflammation. Given the lack of effect on pain, sertraline should not be considered for pain control among patients with RA. 22 Finally, while amitriptyline is widely utilized to treat fibromyalgia and neuropathy, the findings and limitations of current studies restrict its consideration as a therapy for remnant pain in RA.
Due to the serious limitations of the published literature and as we await for results from well-designed studies, a trial of duloxetine or milnacipran may be considered off-label for patients diagnosed with RA, in disease remission and with remnant pain. Despite this recommendation, it is important to emphasize that these medications are not approved for pain among patients with RA and in disease remission. Furthermore, while these medications may benefit patients with RA with comorbid depression, patients in the milnacipran trial did not have depression and depression severity was unknown in the cohort treated with duloxetine.
The findings from studies evaluating TCAs and sertraline were affected by potential critical flaws. Important limitations included the lack of use of DMARDs, no assessment for confounding conditions such as depression, fibromyalgia, neuropathy, or duration of RA, a lack of measures of disease or depression severity, and use of doses that may have been too low to treat pain and/or confounding conditions. Despite positive findings regarding the use of duloxetine or milnacipran to treat pain among patients with RA, those studies also had important limitations. For example, patients in the duloxetine study were not assessed for confounding diseases or depression severity; the baseline pain in the comparator groups in the milnacipran trial was not balanced given it was a post-hoc exploratory analysis of a small subgroup. Thus, future research, should consider the important confounders and covariates noted in this commentary to examine the effects of SNRIs and TCAs among patients with RA on pain control. These medication classes are commonly used to treat fibromyalgia and neuropathy, important components of RA pain.27,28
Patients should be monitored to prevent or minimize adverse events associated with medications. If used, slow uptitration of an antidepressant’s dose to effective response can reduce rates of initial adverse effects and medication nonadherence or early discontinuation of therapy. 33 Frequently seen adverse effects of SNRIs include nausea, insomnia, dry mouth, headache, increased blood pressure, sexual dysfunction, and weight gain. 33 Common adverse effects observed with TCAs include constipation, dizziness, xerostomia, urinary retention, and blurred vision. 34 Additionally, patients should be screened for cardiac conditions such as heart disease or arrhythmias as TCAs may cause QT prolongation, QRS widening, and tachycardia. 34
Summary and Research Needs
Patients with RA may frequently have comorbid conditions including depression, neuropathy, and fibromyalgia, and thus may benefit from the use of antidepressants. Those with RA, in disease remission, and with remnant pain should be screened for depression, fibromyalgia, and neuropathic pain. While we await the results of well-designed trials, these patients may benefit from a trial of duloxetine or milnacipran to reduce pain severity. Future research should assess the effects of SNRIs and TCAs on pain among patients with RA. Studies should utilize current measures of disease control, assess pain severity, evaluate comorbid depression, fibromyalgia, and neuropathy, individualize doses of antidepressants, document use of DMARD(s) to treat RA and duration of RA illness, and assess medication adherence. These efforts may significantly improve disease control and outcomes among patients with RA.
Footnotes
Acknowledgements
We appreciate the editorial contributions of Ann M. Taylor, MPH, MCHES and David Rhys Axon, PhD, MPharm, MS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Milap Nahata is supported in part by the Avatar Foundation. Dr. Armando Silva-Almodovar’s position is supported by Tabula Rasa Healthcare (TRHC). The opinions expressed herein are solely those of the authors and do not reflect the opinions or views of TRHC, its companies, or its employees.