
Abstract
Background
Currently, there is limited literature on the impact of the COVID-19 infection on medications and medical conditions in COVID-19 intensive care unit (ICU) survivors. Our study is, to our knowledge, the first multicenter study to describe the prevalence of new medical conditions and medication changes at hospital discharge in COVID-19 ICU survivors.
Objective
To determine the number of medical conditions and medications at hospital admission compared to at hospital discharge in COVID-19 ICU survivors.
Methods
Retrospective multicenter observational study (7 ICUs) evaluated new medical conditions and medication changes at hospital discharge in patients with COVID-19 infection admitted to an ICU between March 1, 2020, to March 1, 2021. Patient and hospital characteristics, baseline and hospital discharge medication and medical conditions, ICU and hospital length of stay, and Charlson comorbidity index were collected. Descriptive statistics were used to describe patient characteristics and number and type of medical conditions and medications. Paired t-test was used to compare number of medical conditions and medications from hospital discharge to admission.
Results
Of the 973 COVID-19 ICU survivors, 67.4% had at least one new medical condition and 88.2% had at least one medication change. Median number of medical conditions (increased from 3 to 4, P < .0001) and medications (increased from 5 to 8, P < .0001) increased from admission to discharge. Most common new medical conditions at discharge were pulmonary disorders, venous thromboembolism, psychiatric disorders, infection, and diabetes. Most common therapeutic categories associated with medication change were cardiology, gastroenterology, pain, hematology, and endocrinology.
Conclusion and Relevance
Our study found that the number of medical conditions and medications increased from hospital admission to discharge. Our results provide additional data to help guide providers on using targeted approaches to manage medications and diseases in COVID-19 ICU survivors after hospital discharge.
Background
More than 40 million people in the United States have been infected by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), and more than 2 million were hospitalized. 1 A recent meta-analysis reported that the rate of admissions to the intensive care unit (ICU) due to COVID-19 infection was 32% (95% confidence interval [CI]: 26-38; 37 studies and n = 741), with a pooled prevalence of mortality of 39% (95% CI: 34-43; 37 studies and n = 983). 2 In addition, ICU survivors are at increased risk of mortality and decreased quality of life compared to the overall population. 3 ICU survivors are also at risk of hospitalization for other complications. Forty-five percent of these patients had increased resource utilization (hospital readmissions and outpatient visits). 4 ICU survivors may experience several complications following their hospitalization. These complications can include new or worsening cognitive impairment (greater than 75%), mental health conditions (up to 62%), physical disabilities (ICU-acquired neuromuscular weakness reported in greater than 25%), financial issues (33 to 50%), and social impairment.5,6 This population may also be challenged with reintroduction to society, financial insecurities associated with daily living expenses and health care costs, loss of job or job obtainment, low health literacy, and management of current and new chronic conditions.
Furthermore, those unable to return home immediately following their ICU stay may undergo a complicated sequence of care transitions (e.g., skilled nursing facility) increasing the risk of medication-related problems at each transition. Inappropriate medication discontinuations, initiations, and titrations during and after a critical illness hospitalization have been identified as key modifiable factors mediating a patient’s risk for subsequent hospitalization and health setbacks.7 -9 These issues can be further worsened in the setting of COVID-19 due to extensive time in isolation, potential risk of delirium, less family involvement during hospitalization, high volume of patient admissions and discharges, and less personal contact with these patients, especially patients in the ICU.
Currently, there is limited literature on changes to medications and medical conditions associated with COVID-19 infection in COVID-19 ICU survivors. Our study is, to our knowledge, the first multicenter study to describe the prevalence of new medical conditions and changes to medication therapies at hospital discharge in COVID-19 ICU survivors. We hope to use the results of our study to identify potential medical- and medication-related needs for COVID-19 ICU survivors after hospital discharge.
Methods
This study was a multicenter retrospective observational study (7 academic centers, 415 to 1,107 hospital beds per center) that included critically ill patients (18 years of age or older) admitted to the ICU with COVID-19 infection between March 1, 2020 to March 1, 2021. Patients who were in the ICU less than 48 h, discharged to hospice or a hospice patient, or died during hospitalization for COVID-19 infection were excluded from the study. The institutional review boards of each site involved approved the study. We also obtained ethical approval from each site prior to collecting data, and the requirement for written informed consent was waived due to the retrospective nature of the study. Data were collected in a de-identified manner from the electronic medical records and entered into a REDCap database (University of Michigan). Data collected included patient demographics and characteristics, hospital characteristics, baseline and at hospital discharge medication and medical conditions information, ICU and hospital length of stay, discharge destination, Charlson comorbidity index, and the number of changes to medications and medical conditions. The number and type of medications and medical conditions were collected from the hospital admission and discharge notes.
The primary endpoints were the number of medical conditions and medications at hospital admission compared to at hospital discharge in COVID-19 ICU survivors. We also determined the number of and characterized new medical conditions and changes to medication therapies at hospital discharge. Descriptive statistics were used to describe patient demographics and characteristics, hospital characteristics, number and type of medical conditions and medications, and number and type of new medical conditions and changes in medication therapies. A paired t-test was used to compare the primary endpoint, the change in the number of medical conditions and medications at the time of hospital discharge compared to hospital admission. A P value of .05 or less was considered to indicate a statistically significant difference. Statistical analyses were performed in SPSS, version 27 (IBM Corporation, Armonk, NY).
Results
A total of 973 critically ill COVID-19 ICU patients were included in the study. Baseline patient demographics and characteristics are summarized in Table 1. Median age was 58 (18-95) years, 61.1% were male, and 47.6% were African American and 36% were Caucasian. Most patients were discharged home (58.6%), followed by 25.1% discharged to an outpatient facility (i.e. skilled nursing facility). The most common types of medical conditions at hospital admission were hypertension (56.1%), diabetes (39.5%), obesity (35.7%), hyperlipidemia (24.9%), and pulmonary disorders (i.e. asthma, chronic obstructive pulmonary disease [COPD]) (26.7%). At hospital admission, the most common therapeutic categories of the medications were cardiology (60%), endocrinology (36.7%), pain (33.4%), and gastroenterology (29.9%). The most common drug categories of medications at hospital admission were statins (33.7%), angiotensin-converting enzyme inhibitors (ACEI)/ angiotensin II receptor blockers (ARBs) (32.4%), vitamins/minerals/electrolytes (31.9%), nonopiate pain medications (28.6%), diuretics (25.6%), and beta-blockers (25.3%). Refer to Supplementary tables for more details.
Patient Demographics and Characteristics (n = 973).
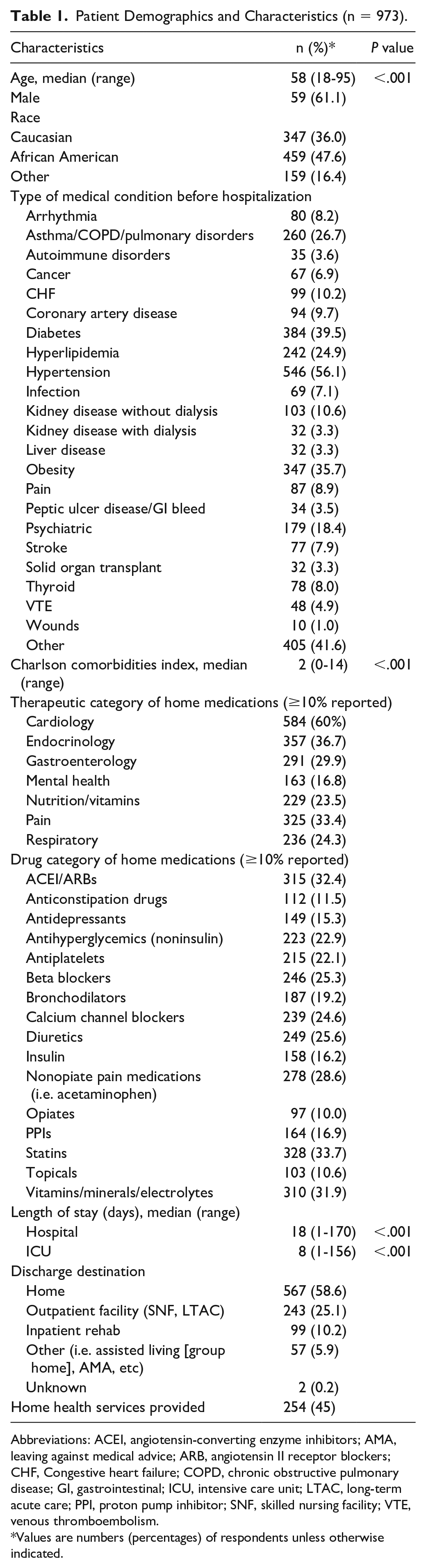
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; AMA, leaving against medical advice; ARB, angiotensin II receptor blockers; CHF, Congestive heart failure; COPD, chronic obstructive pulmonary disease; GI, gastrointestinal; ICU, intensive care unit; LTAC, long-term acute care; PPI, proton pump inhibitor; SNF, skilled nursing facility; VTE, venous thromboembolism.
Values are numbers (percentages) of respondents unless otherwise indicated.
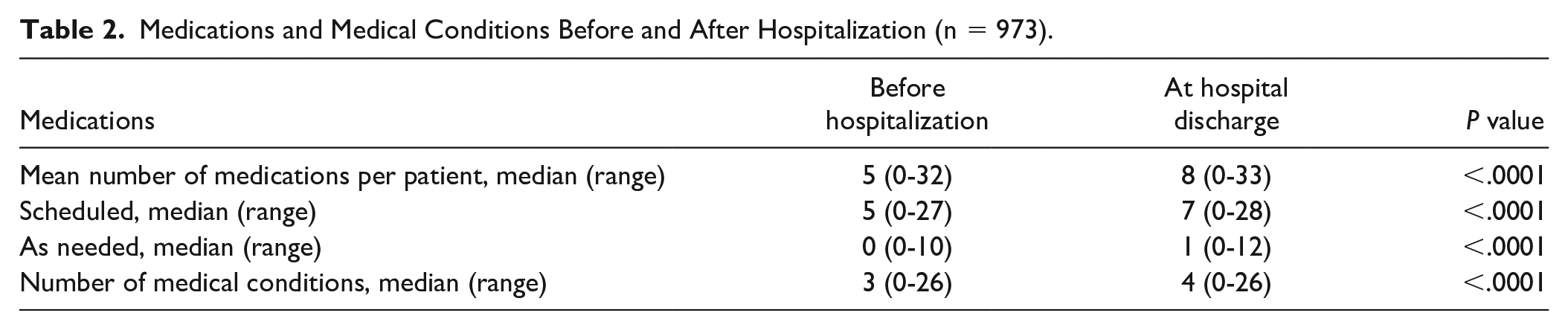
The primary outcome of the difference in the number of medical conditions and medications at hospital admission and at hospital discharge in COVID-19 ICU survivors is described in Table 2. There was a significant increase in the median number of medications (increased from 5 to 8, P < .0001) and medical conditions (increased from 3 to 4, P < .0001) from hospital admission to hospital discharge. A total of 6442 medication changes were identified at hospital discharge with a median number of 5 (0-33) medication changes per patient with 88.2% of patients having at least one medication change. Of all patients, 30.3% had a change in medication dose/interval, 83.0% had new medications added, and 54.4% had discontinuation of medications at hospital discharge. The most common therapeutic categories associated with any medication change were cardiology, gastroenterology, pain, hematology, and endocrinology. As for drug categories, the most common were anticoagulants, vitamins/minerals/electrolytes, nonopiate pain medications, anticonstipation drugs, insulin, ACEI/ARBs, beta-blockers, and diuretics. The most common new medications added at hospital discharge included anticoagulants, anticonstipation drugs, vitamins/minerals/electrolytes, nonopiate pain medications, and insulin. The most common medications discontinued at hospital discharge included ACEI/ARBs, diuretics, nonopiate pain medications, calcium channel blockers, and noninsulin antihyperglycemic drugs. The most common medications with a change in dose/interval at hospital discharge included insulin followed by beta-blockers. Table 3 describes the number and type of medication changes identified at hospital discharge.
Medications and Medical Conditions Before and After Hospitalization (n = 973).
Medication-Related Changes at Hospital Discharge (n = 973).
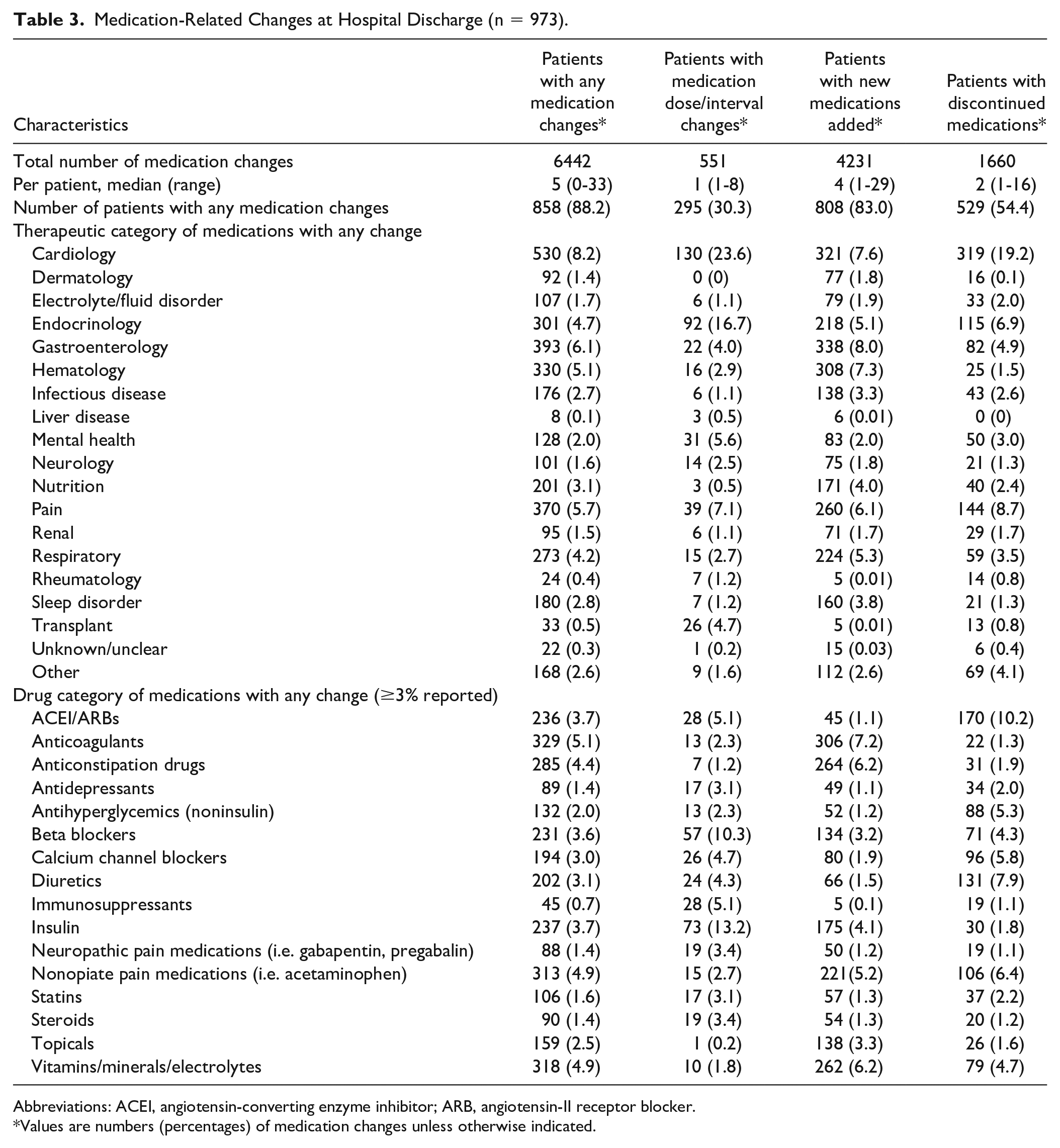
Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-II receptor blocker.
*Values are numbers (percentages) of medication changes unless otherwise indicated.
A total of 656 new medical conditions were identified at hospital discharge with 67.4% of patients having at least one new medical condition. The most common new medical conditions at hospital discharge included pulmonary disorders, venous thromboembolism (VTE), psychiatric disorders, infection, diabetes, hypertension, and arrhythmias. Table 4 describes the number and type of new medical conditions identified at hospital discharge.
Number of New Medical Conditions at Hospital Discharge (n = 973).
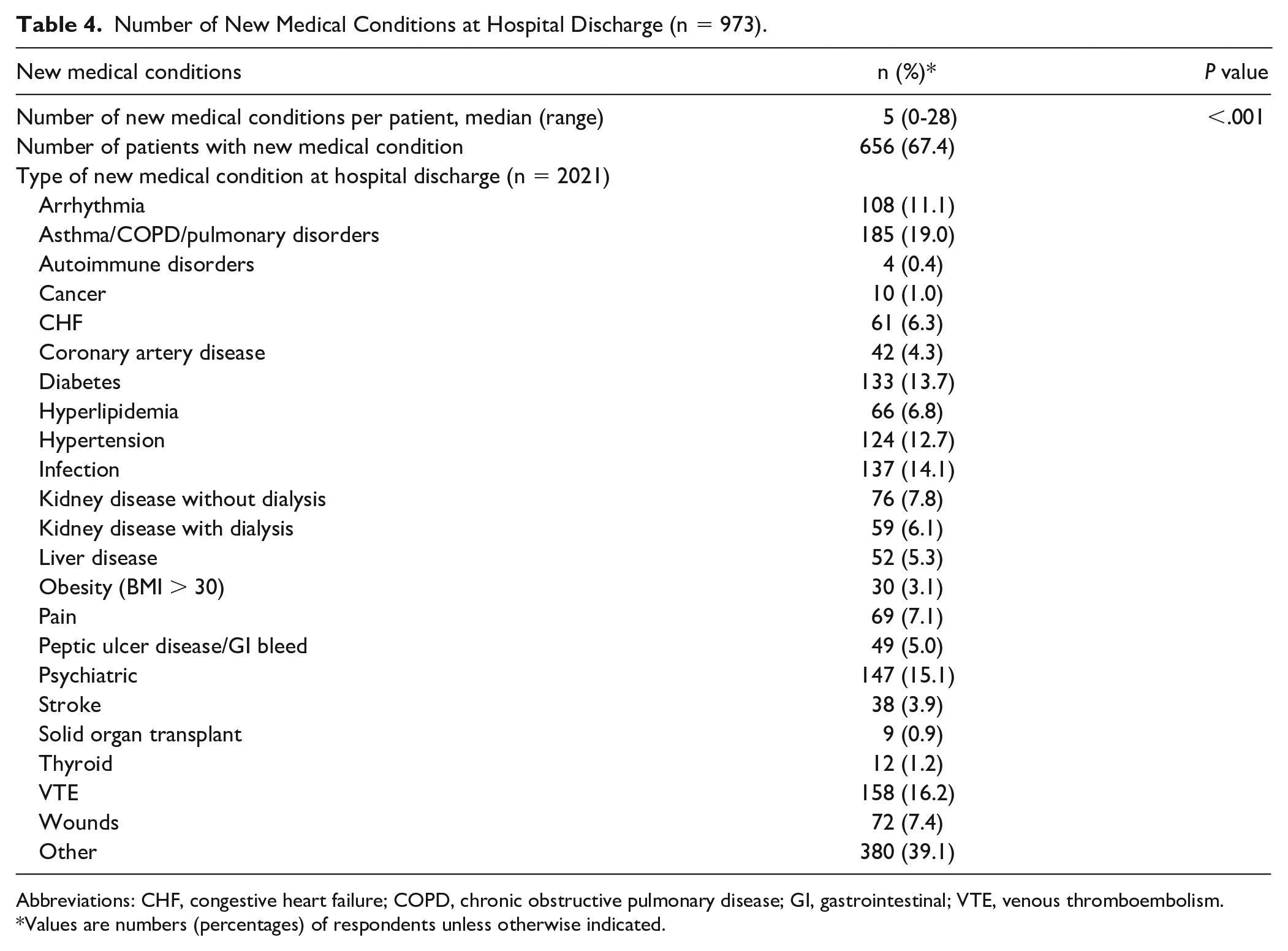
Abbreviations: CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; GI, gastrointestinal; VTE, venous thromboembolism.
Values are numbers (percentages) of respondents unless otherwise indicated.
Discussion
With the ongoing COVID-19 pandemic, it is critical to identify the medical- and medication-related needs of COVID-19 ICU survivors after hospitalization. This study showed that there was an increase in both medications and medical conditions at hospital discharge compared to on admission. In addition, approximately 67% of patients had at least one new medical condition at hospital discharge with the most common new medical conditions being pulmonary disorders, VTE, psychiatric disorders, infection, diabetes, hypertension, and arrhythmias. Our study also found that one-fourth of patients were discharged to an outpatient facility (i.e. SNF). These findings indicate the likelihood of both short-term and long-term morbidity that COVID-19 ICU survivors may face after hospital discharge. With these significant increases in medication therapies and medical conditions, these patients may be faced with managing more complex medication regimens and chronic conditions, new chronic conditions, and potential adverse effects and drug interactions due to medication changes. In addition, with a large portion of patients being discharged to an outpatient facility, these patients will be faced with more challenges compared to patients discharged home (i.e. multiple transitions), which stresses the importance of medication management during these transitions of care. Overall, there have been several studies that have shown that COVID-19 patients presented with several health outcomes and economic burdens;10,11 which stresses the importance of characterizing new medical conditions and medications post-COVID-19 infection which could potentially lead to these burdens.
There is limited data showing the changes in medication therapy in COVID-19 ICU survivor at hospital discharge. However, there have been several studies documenting that medication changes occur in non-COVID-19 ICU survivors during transitions of care. A retrospective cohort study showed that 15.1% of ICU survivors had statin therapy discontinued and 3.6% were newly prescribed an antipsychotic medication after hospital discharge. 12 Another study showed that nearly half of antipsychotic-naïve ICU survivors were prescribed antipsychotics at hospital discharge. 13 One study showed that 40% of patients had differences between medications prescribed at hospital discharge and medications documented in the outpatient setting. 14 Our study found that almost 90% of patients had at least one medication change at hospital discharge, which is higher than previously reported in the non-COVID-19 ICU survivors. Based on the results of our study and prior studies, it is crucial to review patients’ medication lists to ensure they are receiving appropriate medications upon and after hospital discharge and to be aware of the medication changes that occur due to hospitalization.
We also know that the COVID-19 infection can result in new or worsening pulmonary disorders, such as sleep apnea, COPD, and asthma, at hospital discharge.15,16 In addition, the COVID-19 infection can result in acute respiratory distress syndrome further leading to long-term effects on pulmonary function and disorders. 16 However, the COVID-19 infection has been associated with several extrapulmonary diseases, such as, but not limited to, VTE, diabetes, hypertension, and arrhythmias. A recent large retrospective cohort study (n = 47,780) described the rates of diagnoses of pulmonary, cardiovascular, metabolic, kidney, and liver diseases after hospital discharge in patients who were hospitalized for COVID-19 infection. 17 There were significantly higher rates of pulmonary disorders (12.7%), diabetes (4.9%), and cardiovascular disease (4.8%) in patients with COVID-19 infection after hospital discharge. Our study showed higher rates of new diagnosis of pulmonary disorders (19%), diabetes (13.7%), hypertension (12.7%), in addition to psychiatric disorders (15.1%), and VTE (16.2%). However, our study was limited to new diagnoses at hospital discharge and not after hospitalization, and was focused on COVID-19 ICU patients and not all COVID-19 hospitalized patients. Overall, with these new diagnoses, it is expected to see an increase in new, changes and discontinuation of medication therapies.
Recent studies have shown that the COVID-19 infection is associated with a prothrombotic and inflammatory state potentially leading to VTE.18,19 A recent meta-analysis reported the overall VTE prevalence to be 14.1% (95% CI, 11.6-16.9) in patients with COVID-19 infection 18 and one study showed that the VTE incidence was 37% in critically ill patients with sepsis. 20 Due to the hypercoagulable state of COVID-19 ICU patients, anticoagulation therapy is usually initiated in patients with high suspicion or radiologic confirmed diagnosis of VTE. 19 , 21 These patients are then continued and discharged on anticoagulation therapy to complete their treatment course. Therefore, it is not surprising to see that our study identified anticoagulation therapy as the most common new medication at hospital discharge.
In addition to VTEs, there has been published data suggesting an association with new or worsening diabetes in patients hospitalized with severe COVID-19 infection. The development or worsening of diabetes may be due to the stress response associated with the infection or the use of glucocorticoids for the treatment of complications associated with the infection. 22 A recent meta-analysis showed that 14.4% of hospitalized COVID-19 patients were newly diagnosed with diabetes. 23 Another systematic review showed that the risk of developing diabetes in COVID-19 ICU patients was 2.21 times greater than non-ICU patients. 24 In addition, severe COVID-19 infection has been associated with increased hemoglobin A1c and blood glucose levels during and after hospitalization.25,26 Therefore, appropriate and early therapy is recommended in patients who are newly diagnosed with or have worsening of diabetes. Initiation of insulin therapy and discontinuation of noninsulin therapy would be expected, and these findings are confirmed by our study.
The strengths of our study include the size and inclusion of patients from multiple centers and demographics. In addition, this is the first multicenter study to describe the prevalence of new medical conditions and changes to medication therapies at hospital discharge in COVID-19 ICU survivors. We found that there was an increase in the number of new medical conditions and medication therapies in these patients at hospital discharge. The results of our study stress the importance of immediate, close and thorough follow-up of these patients’ posthospital discharge, especially focusing on providing a detailed comprehensive medication review, medication reconciliation, and disease management. Our study identifies common medications and medical conditions that COVID-19 ICU survivors may present with at hospital discharge, which can help guide providers on identifying potential problems or provide appropriate disease and medication management as these patients transition to the outpatient setting. In addition, these results can be used as transitions of care or follow-up clinics and services are developed to care for these patients. Our study did have several limitations. This was an observational study and residual confounding, such as age, race, and sex, is possible. In addition, due to the retrospective nature of our study, we depend on the accuracy of documentation in the electronic medical record. Each institution had different approaches with medication reconciliation (i.e. pharmacist involvement), and the pandemic has impacted the process of medication reconciliation at these institutions due to, but not limited to, decreased resources, and changes in staff models and roles. We realize this is a limitation that would need to be considered, and unfortunately, it would be difficult to retrospectively evaluate the process and accuracy of medication reconciliation in each institution. We also did not have post-hospital discharge data on the COVID-19 ICU survivors; therefore, we were not able to assess the long-term impact of the COVID-19 infection or observed long-term changes in the patient’s other medical conditions or medications. In addition, we did not collect 30-day readmissions; therefore, we were not able to assess the clinical outcomes of COVID-19 ICU survivors post-hospital discharge. We also were not able to include the number of COVID-19 patients (ICU and non-ICU) in our study; therefore, we could not describe the large patient population. Despite these limitations, the cohort size and demographics allowed us to present detailed information on medication and medical conditions in COVID-19 ICU survivors at hospital discharge.
Conclusions and Relevance
Our study showed that there was an increase in the number of new medical conditions and medications at hospital discharge compared to on admission. In addition, the most common medications associated with changes and new medical conditions identified at hospital discharged focused on cardiovascular disease, diabetes, VTE, pulmonary disorders, and psychiatric conditions. The results of our study can help guide providers deliver targeted and appropriate disease and medication management in COVID-19 ICU survivors after their hospitalization.
Supplemental Material
sj-docx-1-aop-10.1177_10600280211063319 – Supplemental material for Medication Changes and Diagnosis of New Chronic Illnesses in COVID-19 Intensive Care Unit Survivors
Supplemental material, sj-docx-1-aop-10.1177_10600280211063319 for Medication Changes and Diagnosis of New Chronic Illnesses in COVID-19 Intensive Care Unit Survivors by Rima A. Mohammad, Cynthia T. Nguyen, Patrick G. Costello, Janelle O. Poyant, Siu Yan Amy Yeung, Kaitlin Landolf, Andy Kim, Katherine L. Artman, Dakota C. Taylor, Michael T. Kenes, Tuqa Alkhateeb and Joanna L. Stollings in Annals of Pharmacotherapy
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Previous Presentations of the Work
This study has not been presented or published previously.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.