
Abstract

We describe a patient case in which rivaroxaban failed to maintain therapeutic anticoagulation in a patient while also taking oxcarbazepine. A 28-year-old male presented to the emergency department (ED) after developing chest tightness, shortness of breath, and falling unconscious at home. He regained consciousness before arriving to the ED. While in the ED, he was hypoxemic and tachycardic requiring supplemental oxygen. Significant medical history includes chronic anticoagulation for heterozygous prothrombin gene mutation with rivaroxaban, history of pulmonary embolism (PE), schizophrenia, psychosis, bipolar disorder, depression, diabetes, hypertension, gastric esophageal reflux disease, obesity (146 kg; BMI = 50.7 kg/m2), and hypertriglyceridemia without hypercholesterolemia. Home medications included rivaroxaban 20 mg daily for 2 years, oxcarbazepine 600 mg twice daily for more than 2 years, alogliptin, atorvastatin, benztropine, divalproex, gabapentin, glipizide, ibuprofen, insulin aspart, insulin glargine, lisinopril, mirabegron, metformin, metoprolol, ondansetron, paliperidone, pantoprazole, sertraline, tolterodine, and topiramate.
A computed tomography scan revealed bilateral PE with suspected saddle embolus and no evidence of right ventricular heart strain. Venous ultrasound was negative for deep-vein thrombosis. The patient and family assured adherence to the anticoagulation regimen, stating that the last dose was taken the evening prior to admission. An anti-Xa level calibrated for rivaroxaban was obtained roughly 21 hours from the last known dose. The level was reported to be undetectable (<10 ng/mL; lab reported expected trough values: 19-60 ng/mL). 1 Heparin was initiated for the treatment of PE, and his symptoms improved overnight. On day 2, the patient’s oxygen saturation and heart rate returned to baseline. Warfarin was selected as the long-term anticoagulant. The patient was continued on heparin until 2 therapeutic international normalized ratios were achieved 24 hours apart and was discharged from the hospital in good condition (Table 1).
Pertinent Labs and Days of Admission.
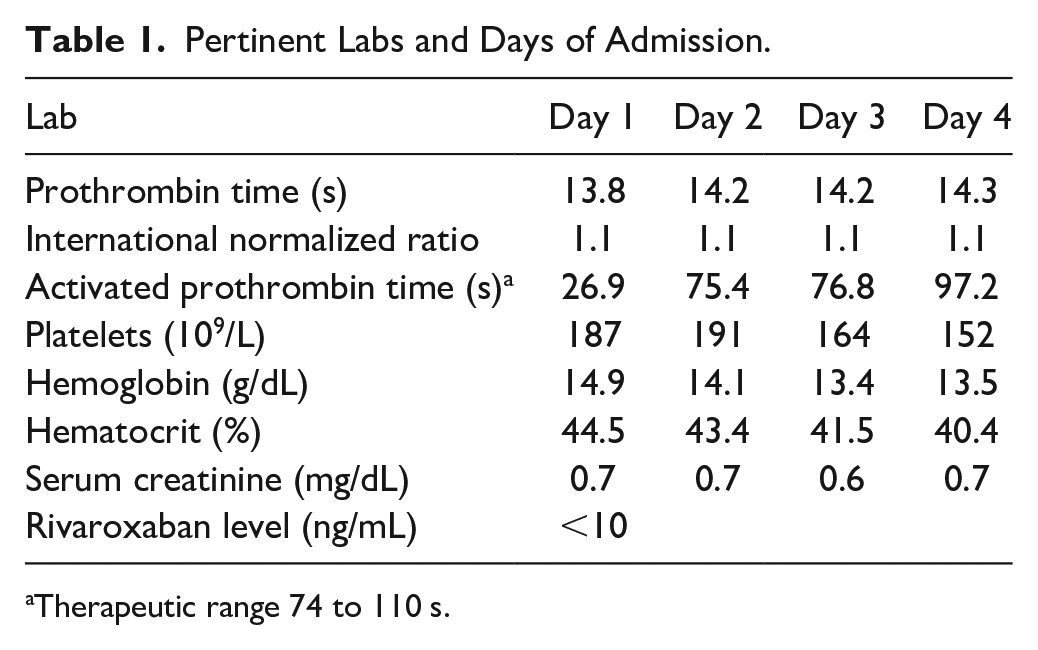
Therapeutic range 74 to 110 s.
There is a growing amount of literature for the use of rivaroxaban in obesity. Martin et al 2 demonstrated that trough levels of rivaroxaban in obese patients (120-230 kg) did not differ significantly from expected trough levels. Therefore, we would not attribute undetectable levels of rivaroxaban solely to the patient’s obesity.
According to LexiComp and the rivaroxaban package insert, concomitant use of strong CYP3A4 inducers, such as carbamazepine, reduces serum concentrations of rivaroxaban, and it is recommended that this should be avoided.3,4 Oxcarbazepine is described as a weak CYP3A4 inducer and has a moderate interaction with rivaroxaban. 3 Serra et al 5 reported a case of concomitant use of rivaroxaban and oxcarbazepine. The patient with atrial fibrillation was taking rivaroxaban for stroke prevention. However, the patient developed a left atrial thrombus after 6 weeks of therapy. This case was referenced in a review of pharmacokinetic interactions of direct oral anticoagulants and antiepileptic medications. 6 They concluded that concomitant use of oxcarbazepine and rivaroxaban could not be excluded as a cause for anticoagulation failure. Our case is the second report of rivaroxaban failure while taking oxcarbazepine and the first substantiated with a rivaroxaban level. This case demonstrates the need for a heightened awareness of this medication interaction.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.