
Abstract
Background
The furosemide stress test (FST) is a safe and easy assessment of renal tubular function. Other factors, such as mean arterial pressure (MAP), which may influence the success rates of the FST, have not been well defined.
Objective
To evaluate the relationship between MAP and success rates of the FST in critically ill patients.
Methods
Retrospective, single-center, institutional review board (IRB)-approved cohort study. Critically ill adult patients given at least one dose of intravenous (IV) furosemide (≥1-1.5 mg/kg) were included. Primary outcome was whether a MAP ≥ 75 mm Hg would equate to a higher FST success rate. Secondary outcome was the success rates of patient on one or more vasopressors.
Results
Of 225 patients, 88 (39.1%) had a successful FST. In patients with a MAP ≥ 75 mm Hg, 60 out of 104 (57.7%) had a successful FST compared to 28 out of 121 (23.1%) of patients who had a MAP < 75 mm Hg (odds ratio [OR], 4.53, 95% CI, 2.55-8.74, P < 0.001). Patients on vasopressors at the time of the furosemide dose had lower rates of success compared to those not on vasoactive agents (30.4% versus 68.2%, p = 0.026). Limitations of this study include its retrospective design and reliance on documented urine output.
Conclusion and Relevance
Patients with a MAP ≥ 75 mm Hg were significantly more likely to have a successful FST compared to those with a MAP < 75 mm Hg. This represents the first report of factors that may influence FST success rates.
Keywords
Introduction
Acute kidney injury (AKI) can occur in up to 20% to 50% of patients in the intensive care unit (ICU) and is associated with significant morbidity and mortality.1-5 Patients who develop an AKI may require the use of renal replacement therapy (RRT), an invasive procedure that carries a risk of complications. An acute increase in serum creatinine (≥0.3 mg/dL) is frequently used to identify an AKI, although it is well known that elevations in serum creatinine levels lag behind the actual time of injury.1,6 In addition, creatinine is a product of muscle breakdown that can be an unreliable marker in patients with high or low muscle mass such as the elderly or children.7,8 There have been studies investigating novel biomarkers, such as neutrophil gelatinase-associated lipocalin (NGAL) and interleukin (IL)-18, for earlier detection of AKI; however, the utility of these biomarkers may be limited by their availability and cost.7,9
Furosemide is a short-acting loop diuretic that is used to treat edematous conditions, such as heart failure, nephrotic syndrome, and cirrhosis. 10 Loop diuretics are commonly used in the ICU to treat fluid overload, a frequent occurrence in critically ill patients that can lead to increased morbidity and mortality.11,12 Furosemide can also be used diagnostically to assess the functional integrity of the renal tubules based on its pharmacokinetic properties.2-4 It is highly protein bound and enters the proximal convoluted tubule of the kidney via active secretion through the human organic acid transporter (hOAT) present in the tubule. 4 Once in the tubular lumen, furosemide blocks the sodium-potassium-chloride (Na+–K+–2Cl−) transporter on the luminal surface of the thick ascending loop of Henle, preventing sodium reabsorption resulting in increased urine flow and excretion.2,4,13 For furosemide to exert an effect of increased diuresis, the intrinsic function of the renal tubules must be intact and free of obstruction. 13 Adequate renal perfusion is also necessary for furosemide delivery and its diuretic action. 4
The furosemide stress test (FST) is the administration of intravenous (IV) high-dose furosemide, defined as ≥1 mg/kg in loop diuretic naive patients or ≥1.5 mg/kg in patients with loop diuretic exposure in the previous 7 days, and measuring the urine output (UOP) produced in the 2-hours postdose.2,3,13-15 A successful FST is defined as the production of ≥200 mL (100 mL/h) of urine during the 2-hour period following the furosemide dose. UOP of <200 mL has a correlation with AKI progression with a sensitivity of 87.1% and a specificity of 84.1%. 2 While there is literature to support the use of the FST to evaluate intrinsic kidney function, there is a lack of studies investigating other factors, such as mean arterial pressure (MAP), which may influence FST success rates. The primary purpose of this study is to determine the relationship between MAP and success rates of FSTs. We hypothesize that a MAP ≥ 75 mm Hg will equate to higher FST success rates. We also sought to describe other factors and/or patient characteristics that may influence the success rates of the FST, including the use of vasopressors and various comorbid conditions.
Although a MAP of at least 65 mm Hg is generally thought to be adequate for renal perfusion, more evidence is emerging that suggests higher MAP goals may be associated with less kidney dysfunction.16-19 A large prospective study found that a MAP < 73 mm Hg is associated with progression of AKI in critically ill patients with severe sepsis. 17 Comorbid conditions such as hypertension (HTN), chronic kidney disease (CKD), and diabetes mellitus (DM) are associated with renal artery stenosis, potentially requiring higher MAPs for renal perfusion.16-19
Methods and Materials
This was a single-center, retrospective chart review of critically ill patients who received an FST from September 1, 2016, to July 31, 2020, at a large academic medical center. The University of Iowa Institutional Review Board (IRB ID # 202008074) approved this study. Patients were screened for eligibility if they were ≥18 years of age, either admitted to the medical ICU (MICU) or surgical and neurosciences ICU (SNICU) during the study period, had evidence of an AKI and/or reduced UOP, and received a dose of IV furosemide. The admission weight of each patient was assessed via review of the electronic medical record (Epic, Verona, WI) to ensure the dose of furosemide was at least 1 or 1.5 mg/kg (in patients previously exposed to loop diuretics). If patients received multiple doses of furosemide, the first dose that met inclusion criteria was included.
Patients were excluded if they had a past medical history of heart failure, kidney transplant, severe hypoalbuminemia (<2 g/dL), evidence of advanced CKD defined as an elevated baseline serum creatinine (≥2 mg/dL in males, ≥1.5 mg/dL in females), allergy to furosemide, pregnancy, extracorporeal membrane oxygenation (ECMO), continuous renal replacement therapy (CRRT), or use of other non-loop diuretics in the day prior to or during the FST. Patients who did not have blood pressure readings or UOP measurements during the FST period were also excluded.
Data collection was managed using the electronic data capture tool, REDCap® (Research Electronic Data Capture). Data collected include patient demographics, select comorbidities, diuretic use, vasopressor use, average MAP, and UOP during 2-hour period after furosemide administration. Average MAP was calculated by averaging documented 15-minute interval MAPs over the 2-hour period after furosemide administration. MAP measurements from arterial lines were used, if available, or cuff pressures if arterial line readings were not available. MAP readings were calculated from blood pressure measurements, if necessary. UOP was obtained from documentation within the electronic medical record. If UOP was not documented within the 2-hour period after the FST, average UOP was calculated by dividing the urine volume (mL) by the amount of time (hours) since the time UOP was last documented in relation to FST being administered. Baseline serum creatinine from hospital admission was used. If the patient appeared to have AKI on admission, records and medical documentation were reviewed for baseline serum creatinine, as applicable.
The primary outcome for this study was to determine if a MAP ≥ 75 mm Hg is associated with a higher rate of successful FST; defined as the production of ≥200 mL urine within 2 hours of administration of furosemide. The secondary outcome was the success rates of patients on one or more vasopressors. A subgroup analysis was performed to evaluate the success rates of patients who were on a single vasopressor, 2 vasopressors, and 3 or more vasopressors.
Data were described as n (%) for categorical data and mean with standard deviation for continuous data. Categorical data were analyzed with a chi-square test of independence or Fisher’s exact test, as appropriate. For continuous parametric variables, we used the Student’s t-test for comparison of groups; simple logistic regression model was used for non-parametric variables. Missing data were excluded from analyses.
Results
Patient Characteristics
Two-hundred twenty-five patients were included in the study (Figure 1). Baseline characteristics are described in Table 1. The mean age was 58.2 ± 13.9 years; 54.7% were male. Statistically significant differences between the success and failure group were noted for weight (80 kg vs 92.1 kg, P < 0.001), weight-based furosemide dose (1.66 mg/kg vs 1.84 mg/kg, P = 0.02), and serum creatinine level on the day of furosemide administration (2.36 mg/dL vs 3.72 mg/dL, P < 0.001). The only missing data were the baseline serum creatinine for 6 patients, which was excluded from the analyses.
Baseline Patient Characteristics.
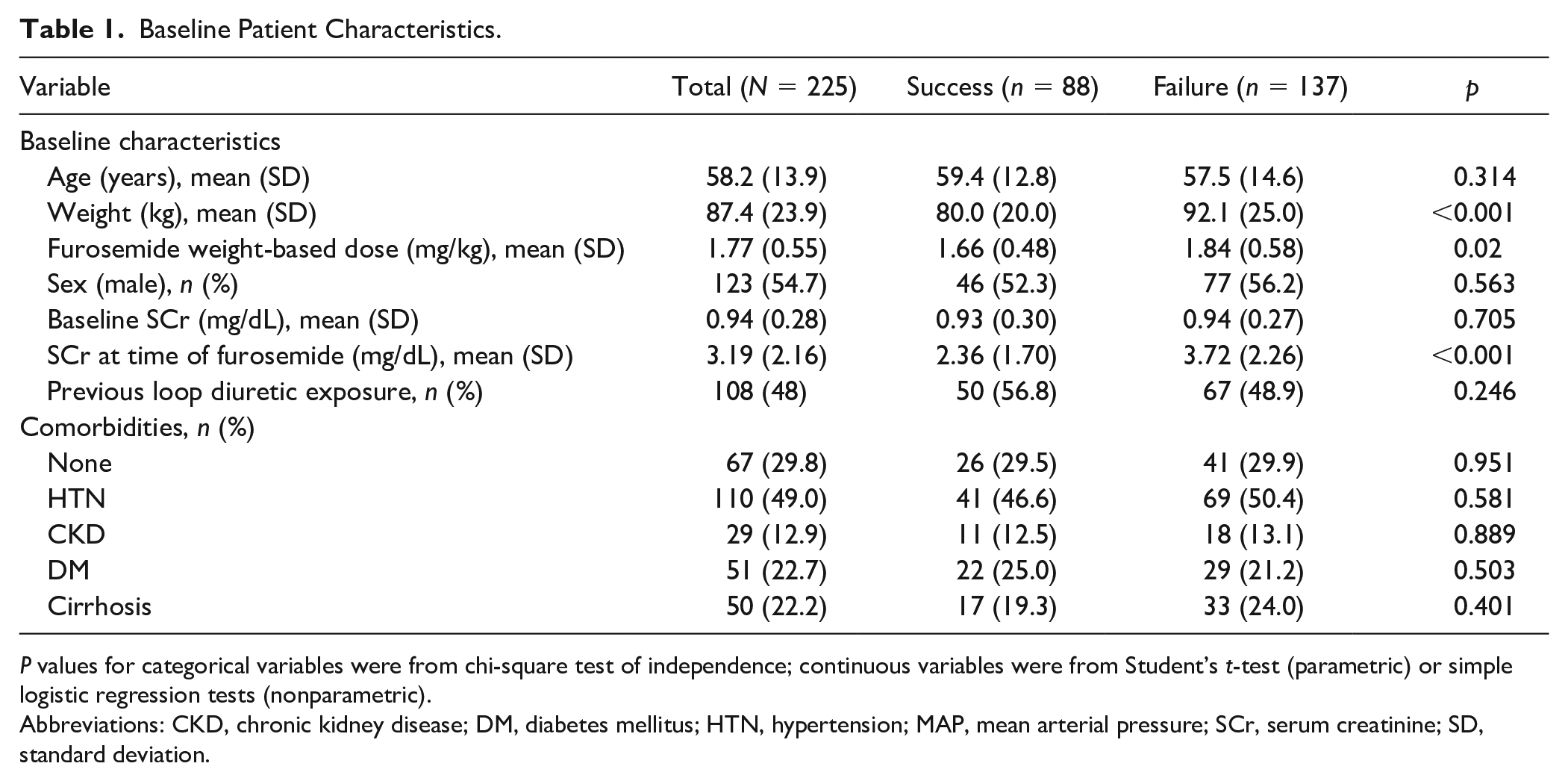
P values for categorical variables were from chi-square test of independence; continuous variables were from Student’s t-test (parametric) or simple logistic regression tests (nonparametric).
Abbreviations: CKD, chronic kidney disease; DM, diabetes mellitus; HTN, hypertension; MAP, mean arterial pressure; SCr, serum creatinine; SD, standard deviation.
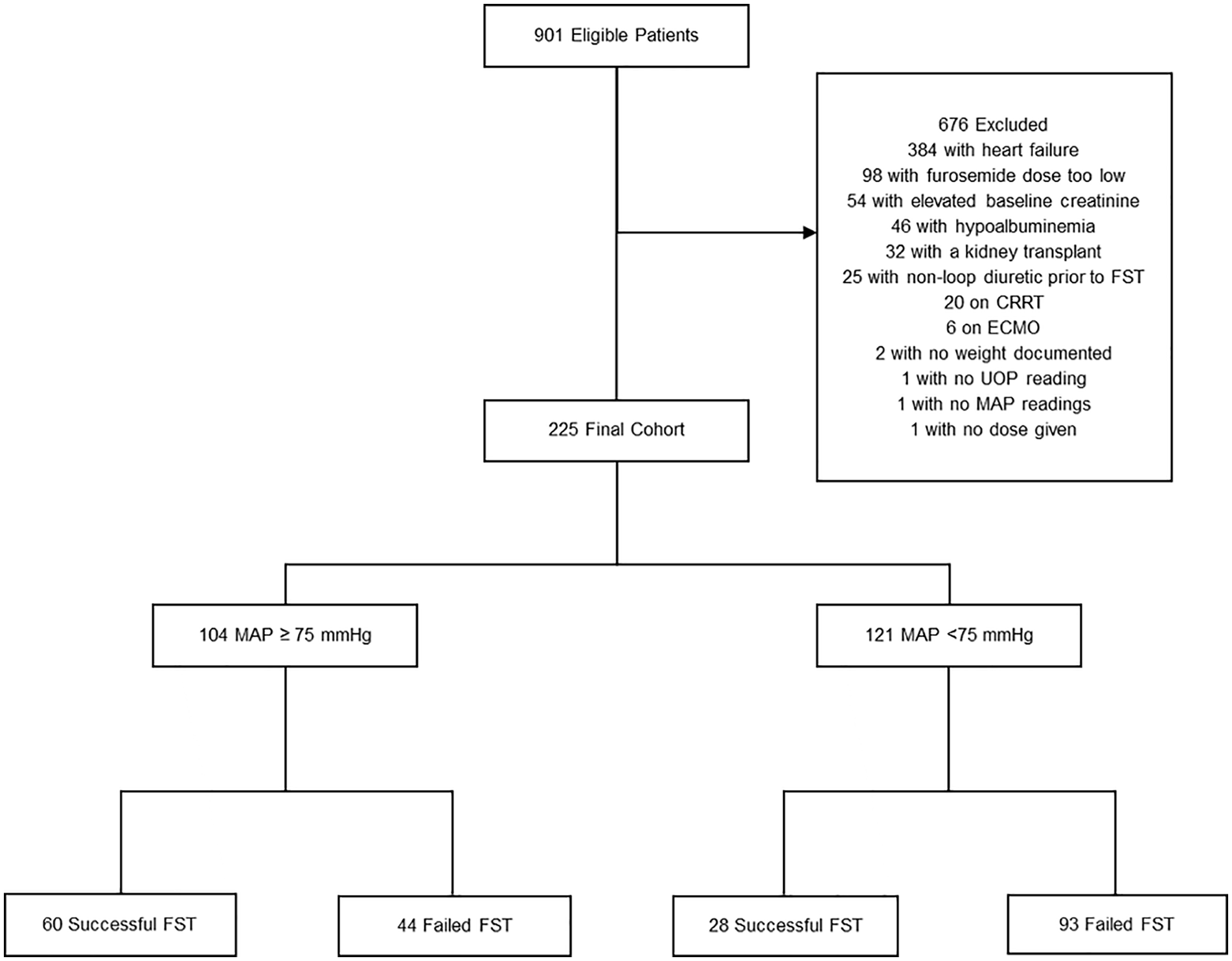
Flow diagram of screening and outcome.
Primary Endpoint
Of the 225 patients included in this study, 104 (46%) had an average MAP ≥ 75 mm Hg and 121 (54%) had an average MAP < 75 mm Hg. Patients who had a higher MAP were more likely to have a successful FST compared to those who did not, 60 (68%) vs 28 (32%) respectively (odds ratio [OR], 4.53, 95% CI, 2.55–8.74, P < 0.001; Table 2). Subgroup analyses of MAP ranges revealed that for each range < 75 mm Hg most patients failed the FST; for each MAP range ≥ 75 mm Hg most patients had a successful FST (Table 2).
Primary Outcome: Mean Arterial Pressure and Furosemide Stress Test Success Rate.
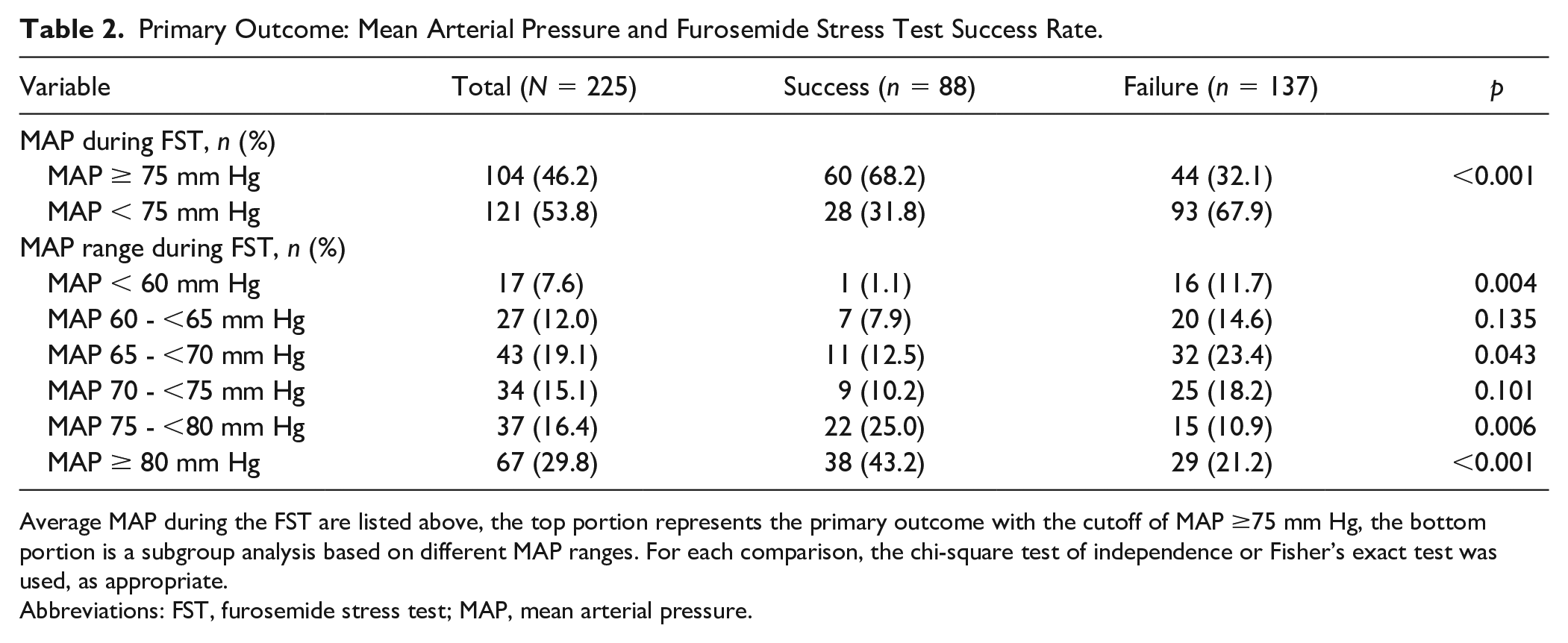
Average MAP during the FST are listed above, the top portion represents the primary outcome with the cutoff of MAP ≥75 mm Hg, the bottom portion is a subgroup analysis based on different MAP ranges. For each comparison, the chi-square test of independence or Fisher’s exact test was used, as appropriate.
Abbreviations: FST, furosemide stress test; MAP, mean arterial pressure.
Secondary Endpoints
Patients that were on vasopressors had a lower FST success rate compared to those without vasopressors, 28 (32%) vs 60 (68%), respectively (P = 0.02). There is an inverse relationship between number of vasoactive agents a patient received during the study period and FST success rate (Table 3). No significant differences in success rates were observed between patients who required no vasoactive agents compared to those who required 1 or 2 vasopressors; however, patients who required ≥ 3 vasopressors had a significantly lower success rate (0%) (P < 0.001) (Table 3). Of the patients on vasopressors (n = 92), those with an average MAP ≥ 75 mm Hg had a higher FST success rate 11/20 (55%) compared to those on vasopressors with a MAP < 75 mm Hg 17/72 (24%), (P = 0.007; Table 3).
Secondary Outcome: Success Rates in Patients on Vasopressors.
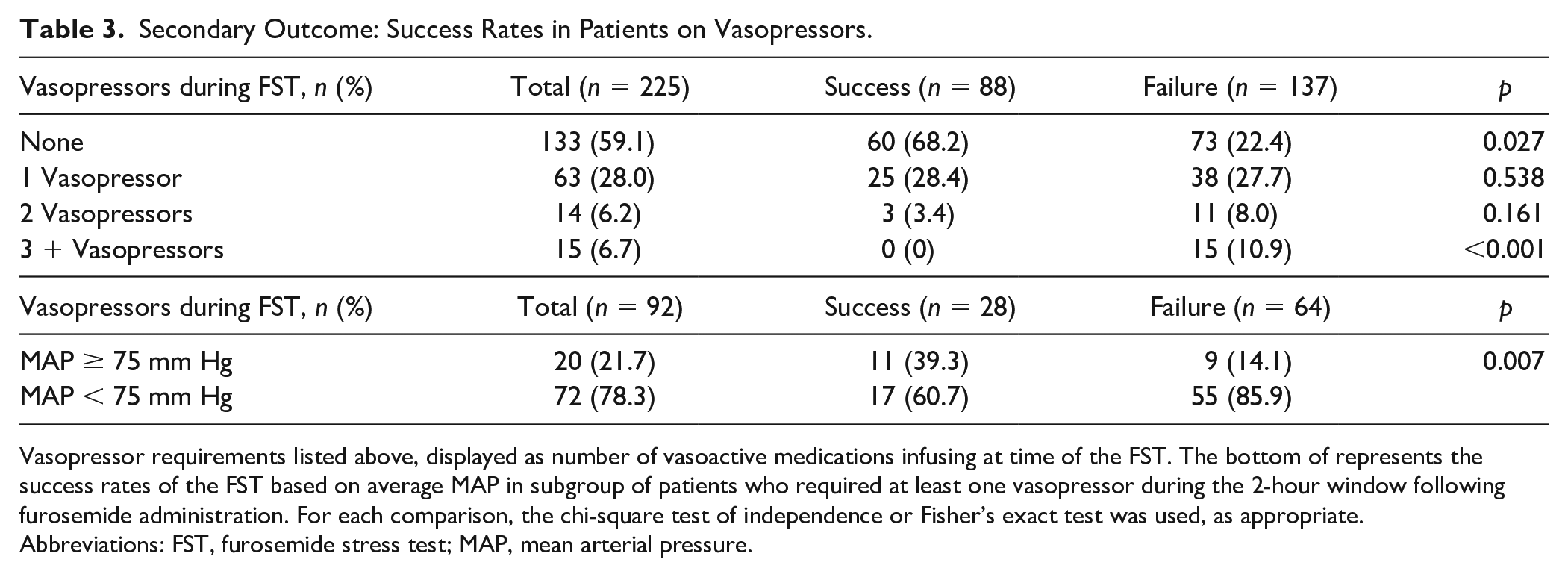
Vasopressor requirements listed above, displayed as number of vasoactive medications infusing at time of the FST. The bottom of represents the success rates of the FST based on average MAP in subgroup of patients who required at least one vasopressor during the 2-hour window following furosemide administration. For each comparison, the chi-square test of independence or Fisher’s exact test was used, as appropriate.
Abbreviations: FST, furosemide stress test; MAP, mean arterial pressure.
The most frequently used vasopressor was norepinephrine, 89/92 (97%). For patients requiring 2 vasopressors, the most common combination was norepinephrine with vasopressin, 12/14 (86%) (Table 4). There were 29 patients on at least 2 vasopressors at the time of the FST; none of these patients had additional vasoactive agents added within 24 hours of the furosemide dose.
Vasopressor Use Frequency by Specific Agent.
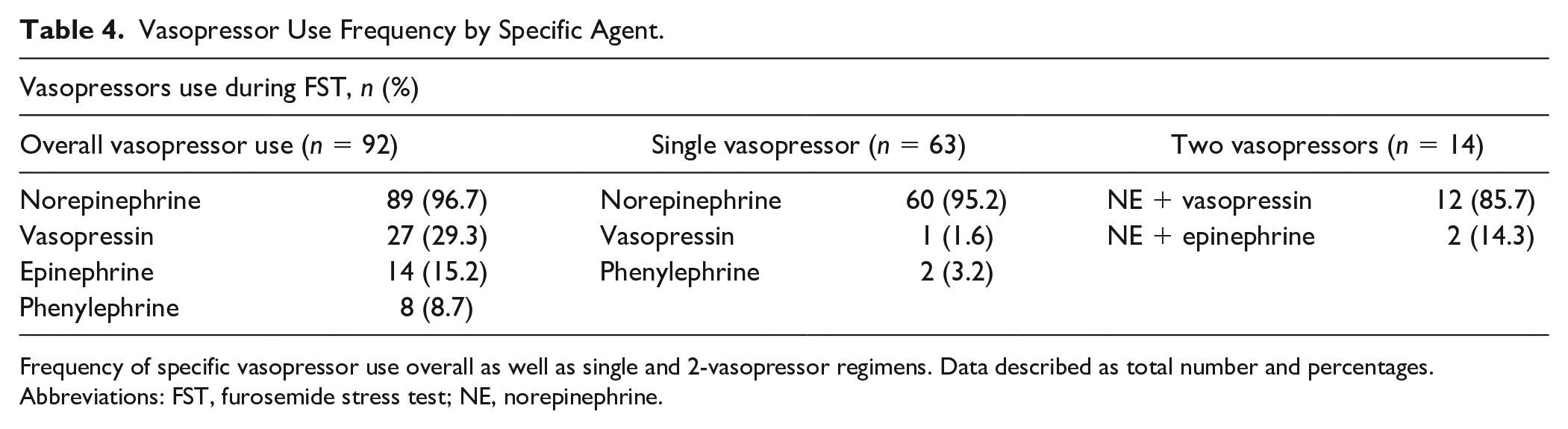
Frequency of specific vasopressor use overall as well as single and 2-vasopressor regimens. Data described as total number and percentages.
Abbreviations: FST, furosemide stress test; NE, norepinephrine.
Discussion
To our knowledge, this is the first study to assess other factors that may contribute to the success rates of the FST. The results of this retrospective review of critically ill patients who received an FST support the hypothesis that higher MAPs equate to higher success FST rates. Regardless of whether vasopressors were used, patients with a MAP ≥ 75 mm Hg had a significantly higher rate of success compared to those with a MAP < 75 mm Hg. This finding may be due to enhanced renal perfusion and better drug delivery associated with higher MAPs in critically ill patients. The Surviving Sepsis Campaign Guidelines recommend targeting an initial MAP of at least 65 mm Hg. 20 However, there is literature to support a higher MAP is associated with a decreased incidence of AKI progression in critically ill patients.16,17,21 The pathophysiological derangements in critically ill patients is not well characterized; although, it has been hypothesized that inflammatory responses, apoptosis, and changes in microcirculation lead to an increased MAP threshold for autoregulation.16,22
Diuretic resistance can develop in critically ill patients, especially in the setting of repeat doses. Several mechanisms for diuretic resistance have been proposed, including: rebound sodium retention in the distal nephron, postdiuretic effect resulting in compensatory sodium retention and “diuretic braking.” 23 Diuretic braking is a decrease in response to a diuretic after receiving the first dose which has been thought to be the result of the other proposed mechanisms of sodium retention. 23 Approximately half of the patients in this study had at least one dose of loop diuretics within 7 days of the FST, these patients required a higher weight-based dose of at least 1.5 mg/kg to account for potential resistance.
Patients in the success group had lower body weights as well as lower serum creatinine level on the day of furosemide administration. Weight excess not only leads to increased risk of several renal risk factors such as HTN and diabetes but has also been associated with unfavorable renal hemodynamics independent of other risk factors.24,25 The success group had a lower weight-based furosemide dose compared to the failure group despite having a lower average weight suggesting the difference in FST success is not due to a higher weight-based dose. The serum creatinine level noted in the failure group on the day of furosemide administration was higher than the success group; this may be indicative of more severe AKI. 26 We did not find a significant difference in FST success rates for any other factors or baseline characteristics, including baseline serum creatinine.
While patients on vasopressors had a lower success rate compared to those without vasopressor requirements, this seems to be driven by patients requiring ≥ 3 vasopressors, as there was no statistically significant difference between FST success rates for patients on ≤2 vasopressors. This finding may be explained to the alterations of autoregulation of renal blood flow in critically ill patients. The most frequently used vasoactive agent in this study was norepinephrine followed by vasopressin. Norepinephrine leads to vasoconstriction in many vascular beds through potent adrenergic agonism, it is thought that this may result in decreased renal blood flow and impair function. 27 However, catecholamines can help achieve or maintain adequate renal blood flow when perfusion pressure decreases outside of the kidney’s autoregulatory zone.19,28 Vasopressin can increase vascular tone and augment end-organ perfusion, which may have renoprotective effects in the setting of hypotension and shock. 18 This may result in constriction of the efferent arteriole, increased pressure within the glomerulus, and increased UOP. When used with norepinephrine, vasopressin can also reduce tubular apoptosis and inflammation as well as exhibit a catecholamine-sparing effect.19,29,30 This may explain why the addition of norepinephrine with or without vasopressin did not appear to significantly alter FST success rates.
This study has several methodologic limitations that warrant consideration. The retrospective and open design of our study introduces bias and limits our capacity to examine specific outcomes. Patients were screened if they received a dose of furosemide 100 mg or more, this could potentially omit patients <100 kg that received at least 1 mg/kg. It may also disproportionately represent lighter patients that are diuretic tolerant or larger patients who are diuretic naïve. The UOP readings were obtained from the electronic medical record. If the UOP was not documented within 2 hours of the furosemide dose, UOP was calculated using the next documented measurement and may not accurately represent the true urine volume produced within the initial 2-hour period. Exposure to other potentially nephrotoxic agents prior to, or during, the FST interval was not evaluated which may have contributed to reduced UOP. Given the potential bias and limitations of this study, assessment of clinically important outcomes such as progression to CRRT or mortality rates were not assessed. In addition, we did not assess for potential adverse effects related to the vasopressors used to maintain higher MAPs or adverse effects related to furosemide administration including hypotension and electrolyte abnormalities.
Conclusion and Relevance
In this retrospective cohort study of critically ill patients receiving at least 1 to 1.5 mg/kg of furosemide, we found that a MAP ≥ 75 mm Hg was associated with a significantly higher rate of successful FSTs compared to those with a MAP < 75 mm Hg. Our data represent the first study to our knowledge that evaluates the effect of MAP, and other factors, on success rates of the FST in critically ill patients. The results of this study suggest that furosemide is more effective in patients with a MAP ≥ 75 mm Hg, regardless whether the patient required vasopressors or not; perhaps due to improved renal perfusion and/or drug delivery. In patients that are undergoing a FST, maintaining a MAP ≥ 75 mm Hg may maximize the chance of a successful test. If already on vasopressors, it may be reasonable to target a MAP ≥ 75 mm Hg in conjunction with the FST; in patients who are not on vasopressors, holding blood pressure lowering drugs to target a MAP ≥ 75 mm Hg prior to an FST may be considered.
These results can only be exploratory and hypothesis generating. It adds to the existing literature that a higher MAP may be necessary to maintain renal perfusion in critically ill patients and may help optimize conditions before performing an FST, further challenging the MAP recommendations as provided by Surviving Sepsis Campaign. 19 A prospective trial would need to be performed to confirm our findings that higher MAPs equate to a greater rate of FST success and to assess clinically significant outcomes such as progression to RRT.
Footnotes
Acknowledgements
The authors thank Andrew Jatis, PharmD (University of Iowa) for assisting in data collection and auditing, and they also thank Tori Adams, PharmD (University of Iowa) for assistance in statistical analysis.
Authors’ Note
This research was previously presented at the Society of Critical Care Medicine 2022 Annual Congress Meeting and presented as an abstract in the supplement of the January 2022 issue of Critical Care Medicine (doi: 10.1097/01.ccm.0000811660.90081.b8). This work was performed at the University of Iowa Hospitals and Clinics.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.