
Abstract
Objective:
To review dasiglucagon, a novel glucagon analogue approved by the Food and Drug Administration (FDA) for treatment of severe hypoglycemia in 2021.
Data Sources:
A literature search using the PubMed database (current to March 2022) and ClinicalTrials.gov was conducted using the search term dasiglucagon.
Study Selection and Data Extraction:
Relevant clinical data from English-language clinical trials were included.
Data Synthesis:
Dasiglucagon was studied in 3 clinical trials: 1 in patients aged 6 to 17 years and 2 in adults. In all 3 trials, dasiglucagon was found to provide clinically significant benefit in minutes to plasma glucose recovery compared with placebo (10 vs 40, P < 0.001; 10 vs 30, P < 0.001; 10 vs 35, P < 0.0001). Dasiglucagon was also comparable with reconstituted glucagon in plasma glucose recovery time measured from time of administration. The most common adverse events with dasiglucagon were nausea, vomiting, and headache; no serious safety events were observed.
Relevance to Patient Care and Clinical Practice:
Dasiglucagon is a novel glucagon analogue that is safe and effective for the treatment of severe hypoglycemia, and it is the first to be stable in aqueous solution. This makes dasiglucagon one of only 3 currently available glucagon treatment options that does not require reconstitution prior to administration.
Conclusions:
Dasiglucagon offers safe and effective treatment for severe hypoglycemia in patients aged 6 years and older. The stability of dasiglucagon in aqueous solution provides an additional option for emergency glucagon treatment that does not require reconstitution prior to administration.
Introduction
Despite advances in diabetes management over the past several years, hypoglycemia remains a concern, particularly for patients receiving treatment with insulin or sulfonylureas. Patients with type 1 diabetes require insulin for disease management and therefore are at risk of hypoglycemia as a side effect. 1 Cohort studies have found anywhere from 4% to 9% of deaths in patients with type 1 diabetes are linked to hypoglycemia. 2
The American Diabetes Association (ADA) recommends glucagon be prescribed for all patients at risk of level 2 hypoglycemia (blood glucose less than 54 mg/dL) as well as level 3 or severe hypoglycemia (impaired mental or physical function due to low blood glucose). 3 Because a patient experiencing severe hypoglycemia may be unable to self-administer glucagon, the ADA also calls for not only health care professionals, but also family members, caregivers, colleagues, and school personnel to be trained in proper recognition of hypoglycemia and administration glucagon of glucagon for treatment. 3
Historically, glucagon emergency kits have been used for treatment of severe hypoglycemia. These kits require reconstitution of lyophilized powder at the time of use, which requires the user to be familiar with use to administer them effectively and efficiently. This multistep process poses a challenge to timely treatment and may even prevent administration of glucagon entirely. 2
In recent years, intranasal glucagon (Baqsimi) and a subcutaneous injectable glucagon in methyl sulfoxide solution (Gvoke) have become available. 4 The newest ready-to-use form of glucagon approved by the Food and Drug Administration (FDA) is dasiglucagon. Dasiglucagon is a novel glucagon analogue that is made up of 29 amino acids, with 7 amino acids being substituted from native glucagon to increase stability in aqueous solution.5-8 This makes it one of only 3 currently available glucagon formulations that does not require reconstitution prior to administration.
This article summarizes the clinical data leading to FDA approval of dasiglucagon and examines its role in treatment of severe hypoglycemia based on currently available glucagon formulations.
Data Sources
A literature search was conducted using the search term dasiglucagon through the PubMed database (current to May 2022) and completed trials at Clinicaltrials.gov. Data included were limited to English-language phase 3 clinical trials; reference lists of included articles were also reviewed for additional relevant data.
Chemistry and Pharmacology
Dasiglucagon is the only glucagon analogue stable in aqueous solution for injection currently, which is due to the 7 altered amino acids compared with endogenous glucagon. However, it has enough similarities to native glucagon to remain specific to the glucagon receptor in the body, maintaining consistent potency with native glucagon. Similar to native glucagon, dasiglucagon agonizes the glucagon receptor, stimulating breakdown of glycogen and release of glucose from the liver. 7 Dose-dependent, rapid increases in plasma glucose have been demonstrated with dasiglucagon comparable with reference glucagon formulations (GlucaGen—Novo Nordisk; Copenhagen, Denmark and Eli Lilly; Indianapolis, United States).8,9
Efficacy
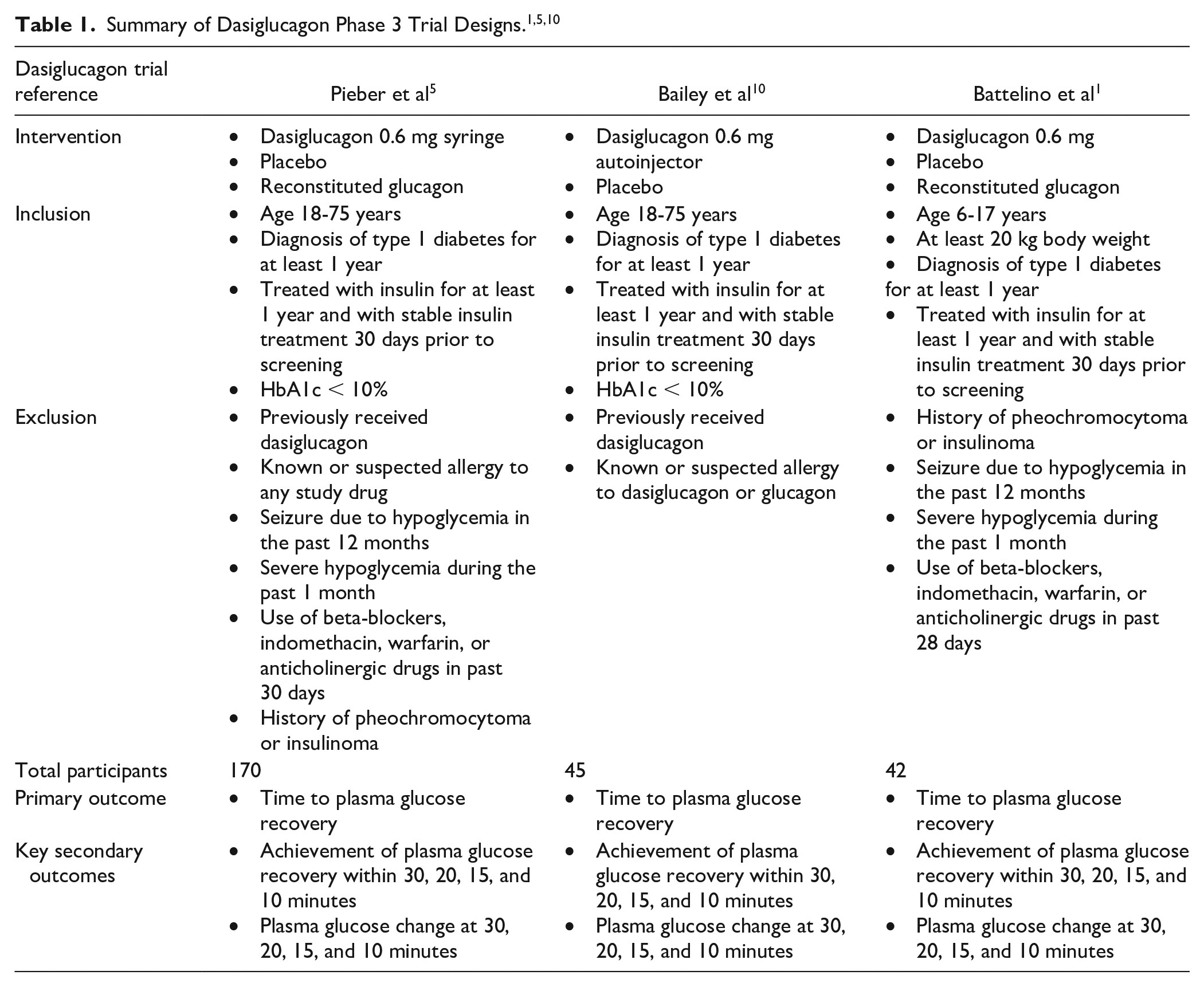
Dasiglucagon was studied in three phase 3 clinical trials in patients with type 1 diabetes: 2 in adults and 1 in children and adolescents. All 3 were randomized, double-blind trials that required patients to receive intravenous insulin to induce hypoglycemia prior to administration of dasiglucagon or placebo. The primary outcome for all trials was average time from administration to plasma glucose recovery, defined as an increase of at least 20 mg/dL in plasma glucose from baseline.
The first trial included 170 participants with type 1 diabetes aged 18 to 75 years who were randomized to receive 0.6 mg dasiglucagon via a prefilled syringe, placebo, or 1 mg reconstituted glucagon in a 2:1:1 ratio. 5 Additional details are shown in Table 1. Participant baseline characteristics including sex, race, age, and hemoglobin A1c were similar between the 3 groups. 5 Time was measured starting with administration of the study drug, so reconstitution time was not included for the reference glucagon product. 5 The median time to plasma glucose recovery for the dasiglucagon group was 10 minutes, which was significantly faster than the placebo group which averaged 40 minutes (P < 0.001). 5 The time to plasma glucose recovery in the dasiglucagon group was similar to the reconstituted glucagon group (10 and 12 minutes, respectively). 5 Percent of participants achieving plasma glucose recovery at 10, 15, 20, and 30 minutes is shown in Table 2. Mean change in plasma glucose at 30 minutes was 90.9 mg/dL in participants receiving dasiglucagon, vs 19.1 mg/dL for those receiving placebo. 5
Plasma Glucose Recovery.
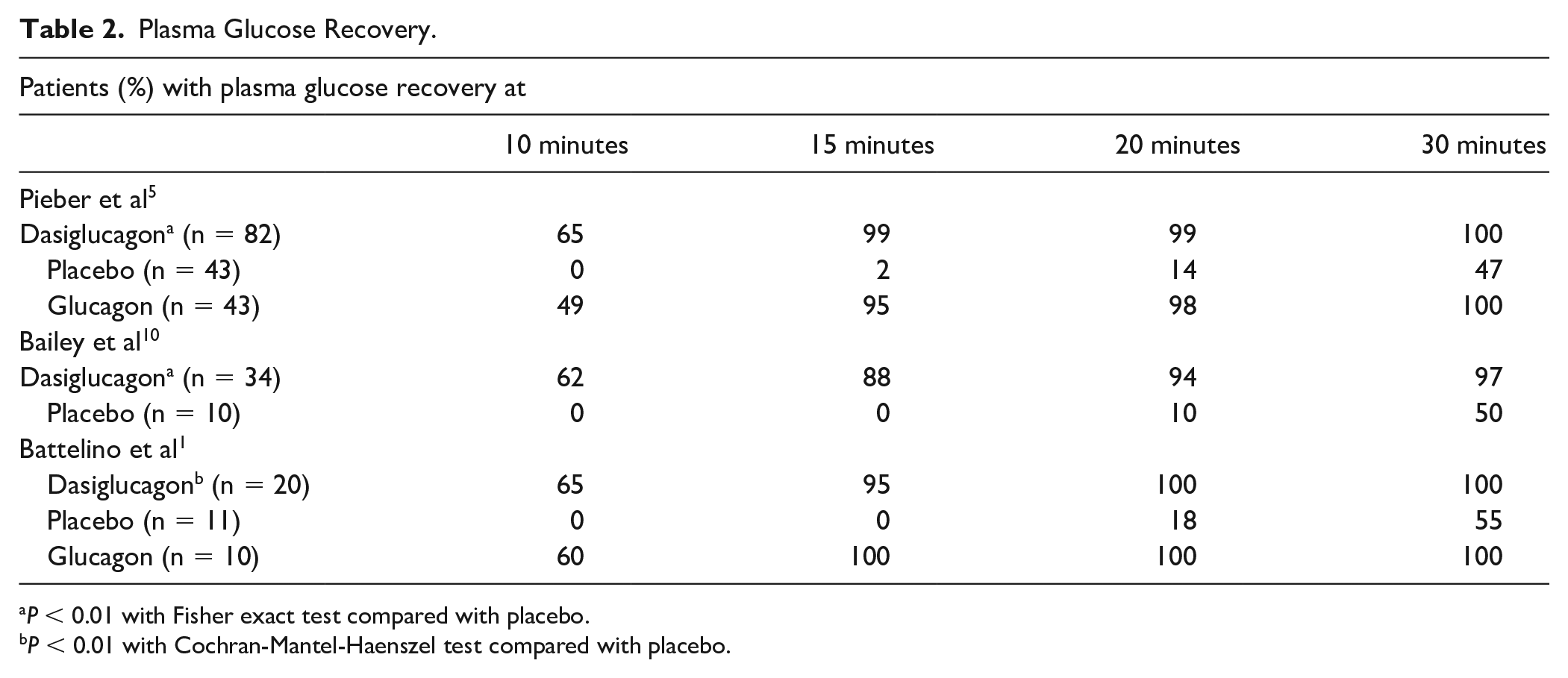
P < 0.01 with Fisher exact test compared with placebo.
P < 0.01 with Cochran-Mantel-Haenszel test compared with placebo.
A second adult trial was conducted in 45 patients aged 18 to 75 years with type 1 diabetes. Patients were randomized 3:1 to receive dasiglucagon via autoinjector device or placebo in the buttocks or deltoid. Inclusion and exclusion criteria as well as measured outcomes were similar to the previously described trial, as shown in Table 1. Similar to the previously described trial, the median time to plasma glucose recovery was 10 minutes. 10 Site of injection did not have an effect on time to plasma glucose recovery. 10
A separate pediatric trial was conducted in 42 patients aged 6 to 17 with type 1 diabetes. Participants were required to be receiving daily insulin and weigh at least 20 kg. 11 Inclusion and exclusion criteria as well as outcomes measured were similar to those used in the adult trials and are displayed in Table 1. The median time to plasma glucose recovery in the dasiglucagon group was the same as in the adult trials, 10 minutes, vs 30 minutes for the placebo group (P < 0.001). 11 The group receiving reconstituted glucagon also had a median plasma glucose recovery time of 10 minutes. 11 Percentage of participants with plasma glucose recovery is shown in Table 2. Mean change in plasma glucose at 30 minutes was 98.2 mg/dL in children and adolescents receiving dasiglucagon, vs only 17.3 mg/dL in the placebo group. 11
Safety
The most common adverse events observed in the clinical trials were nausea, vomiting, and headache in adults. These are known side effects of glucagon administration and were also observed in the reconstituted glucagon reference arm. In the trial that included children and adolescents, nausea and vomiting were the most common side effects and were observed at a slightly higher rate in the 12- to 17-year-old group than in 6- to 11-year-old group. No serious safety events occurred in any of the dasiglucagon groups. Nausea and vomiting were seen to occur within 3 hours of administration for all populations, with nausea typically occurring earlier than vomiting and none of these adverse events lasting longer than 3 hours.5,10,11
Injection-site reactions were rare in the dasiglucagon groups (1 adult and 0 children). The dasiglucagon injection reaction was also mild and self-resolved with time, similar to those seen with the glucagon groups (2 adults and 3 children). No significant difference was seen in these adverse effects when dasiglucagon was compared with reconstituted glucagon.5,10,11
The package insert for dasiglucagon lists adverse events including nausea, vomiting, headache, injection-site pain, diarrhea, and hypersensitivity reactions. Dasiglucagon is contraindicated in patients with pheochromocytoma or insulinomas. 7
Dosing and Administration
Dasiglucagon is available as a prefilled syringe and autoinjector. Dasiglucagon is dosed as 0.6 mg and administered subcutaneously for 1 dose; if there is no response, the dose may be repeated for a second administration after 15 minutes. Acceptable injection sites include the abdomen, buttocks, outer arm, or thigh. 7
The injection is a preservative-free, clear solution that is stable for 12 months at room temperature. In addition to the active ingredient dasiglucagon hydrochloride, each injection also contains small amounts of tromethamine, sodium chloride, and water. 7
Drug Interactions
Dasiglucagon may temporarily increase heart rate and blood pressure in patients taking beta-blockers. Dasiglucagon may be less effective in patients taking indomethacin due to inhibition of pancreatic release of glucagon that has been observed to also impact exogenous glucagon. The anticoagulant effects of warfarin may be increased by dasiglucagon. 7
Immunogenicity
In clinical trials, a total of 4 patients receiving dasiglucagon (n = 498, <1%) developed measurable anti-dasiglucagon antibodies. 7 One adult patient in the dasiglucagon group tested positive for anti-dasiglucagon antibodies at the 28 days follow-up visit. The antibodies were found to be non-neutralizing in vitro and had low titers. 11 One patient had temporary neutralizing activity that was found to be cross-reactive with endogenous glucagon. 5 No safety or efficacy concerns were identified based on clinical trials, but the potential significance of these antibodies on pharmacokinetics and pharmacodynamics of dasiglucagon remains unknown.5,7
A separate immunogenicity study has been conducted since the approval of dasiglucagon, in which 112 patients were randomized 1:1 to dasiglucagon or reconstituted glucagon (GlucaGen) to receive a series of 3 weekly doses of the study drug. 12 Participants were followed for 15 weeks. The overall incidence of antibody development in both groups was zero. 12 While not the primary endpoint, immunogenicity continues to be investigated in ongoing trials of dasiglucagon.
Relevance to Patient Care and Clinical Practice
Severe hypoglycemia remains a major risk for patients with diabetes. While oral glucose is first-line treatment for mild hypoglycemia, a patient with severe hypoglycemia may be unable to take glucose by mouth or self-administer therapy. In these situations, a ready-to-use glucagon formulation is valuable for prompt and effective treatment. It is also beneficial to have formulations of glucagon that are easy to administer, for both trained caregivers and untrained bystanders. Currently, there are 3 ready-to-use glucagon formulations available: dasiglucagon (Zegalogue), intranasal glucagon (Baqsimi), and glucagon in methyl sulfoxide (Gvoke). Compared with the other agents, dasiglucagon is not approved for children below the age of 6 years. However, dasiglucagon does avoid some side effects typically seen with intranasal glucagon by nature of administration, such as upper airway discomfort, congestion, and lacrimation. 1 It also had a slightly faster time to plasma glucose recovery in clinical trials, although this is based on data extrapolated from separate trials. While these novel formulations have not been directly compared with each other in head-to-head trials, they have been compared with traditional glucagon kits that require reconstitution of lyophilized powder with similar findings regarding time to plasma glucose recovery.
Dasiglucagon has also been studied regarding user perceptions of use and administration success rate compared with conventional glucagon emergency kits that require reconstitution in an open-label, randomized, cross-over trial that included both trained caregivers and untrained bystanders. 2 Both trained caregivers and untrained bystanders were significantly more likely to be successful administering the dasiglucagon autoinjector within 2 minutes. 2 In addition, most study participants preferred the dasiglucagon autoinjector and rated it as easier to use and less stressful than the glucagon emergency kit. 2 The finding consistently highlighted the increased speed and efficiency of dasiglucagon preparation and administration over traditional glucagon emergency kits across several outcomes, including overall administration success rate, administration completion time, study task success rate, and user preference and device questionnaires. 2 The overall results of the study were similar to those found when comparing intranasal glucagon to glucagon emergency kits that require reconstitution, strengthening the case for adopting novel ready-to-use glucagon rescue therapies. 2
Among ready-to-use formulations, dasiglucagon is currently the only available option in aqueous solution, a unique characteristic that could lead to further development in artificial pancreas research. Particularly for patients with type 1 diabetes, the ability to use a glucagon analogue that is stable in aqueous solution in combination with an insulin pump to regulate blood glucose could change the standard of care. To date, 1 human pilot study has been conducted to observe safety and operational outcomes in an iLEt bionic pancreas. 13 The study included 10 patients and found no infusion-site reactions or occlusions over a 7-day period, supporting future studies of dasiglucagon with this device. 13
Despite the unique features that may make dasiglucagon clinically desirable, the Centers for Medicare & Medicaid Services (CMS) and most major commercial insurers do not prefer it as a first-line option. Instead, a traditional reconstituted form of glucagon must be trialed first. If failure with the reconstituted form occurs, then dasiglucagon may be considered. This stepwise approach is likely due to the cost of dasiglucagon being higher than any other glucagon formulations, with a wholesale acquisition cost (WAC) of $309 per dose. In comparison, the generically available reconstituted glucagon formulation has a WAC of less than $200 per dose. Specific cost and other comparison data for available glucagon formulations are shown in Table 3. However, a recent budget impact model found that dasiglucagon actually demonstrated reduced costs in treating severe hypoglycemia when compared with reconstituted glucagon, ready-to-use injectable glucagon, and intranasal glucagon. 14 This lower cost was due to higher treatment success rates and faster plasma glucose recovery time, which prevents emergency calls, emergency transportation, emergency department visits, and hospitalizations. 14 When compared with reconstituted glucagon, dasiglucagon had a number needed to treat of 9 to avoid 1 hospitalization. 14 It remains to be seen how this budget impact model will affect payer preferences for dasiglucagon over other glucagon formulations.
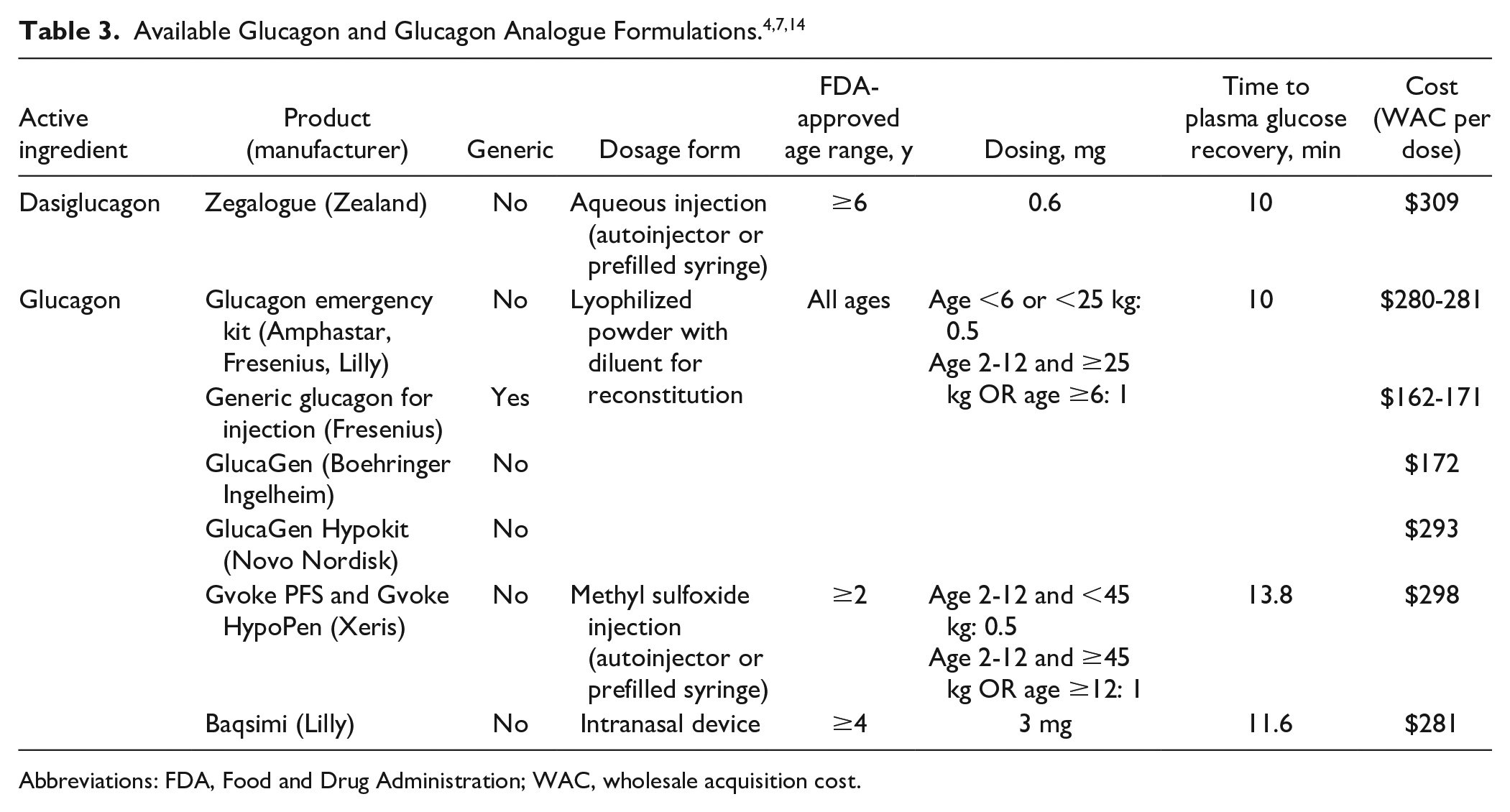
Abbreviations: FDA, Food and Drug Administration; WAC, wholesale acquisition cost.
Summary
Dasiglucagon is a novel glucagon analogue that is FDA-approved for severe hypoglycemia in patients 6 years and older. It has been shown to be as safe and effective in reference to placebo and performs similarly to reconstituted glucagon. The stability of dasiglucagon in aqueous solution provides an additional option for emergency glucagon treatment that does not require reconstitution prior to administration and avoids potential side effects of intranasal administration. As the only formulation stable in aqueous solution, it also allows for future research to determine its role in insulin pumps and artificial pancreases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.