
Abstract
Background:
Drug-related problems (DRPs) are prevalent and avoidable disease that patients experience due to drug use or nonuse. However, secondary prevention policies have not yet been systematized.
Objective:
To assess the clinical impact of a secondary prevention bundle for DRPs in patients who visited the emergency department (ED) for medicine-related problems.
Methods:
A single-center randomized clinical trial was conducted from August 28, 2019, to January 28, 2021, with 1-month follow-up. We included 769 adult patients who visited ED with a DRP associated with cardiovascular, alimentary tract, and metabolic system medications. For the intervention group, a DRP prevention bundle, consisting of a combined strategy initiated in the ED was applied. Patients in the control group received standard pharmaceutical care. Intervention was evaluated in terms of 30-day hospital readmission due to any cause.
Results:
Final analysis included 769 patients, of which 68 (8.8%) were readmitted within 30 days (control group, 40 of 386 [cumulative incidence: 10.4%]; intervention group, 28 of 383 [cumulative incidence, 7.3%]). After adjustment of the model for chronic heart failure, there was a lower incidence of hospital readmission among patients in the intervention group compared with those in the control group, odds ratio: 0.59 [95% confidence interval: 0.37-0.97]; number needed to treat (NNT) = 32. No significant differences in other outcomes were observed.
Conclusion and Relevance:
In this clinical trial, DRP prevention bundle in adjusted analysis decreased the rate of 30-day hospital readmission for any cause in patients who visited ED for a DRP.
Trial registration:
ClinicalTrials.gov (Identifier: NCT03607097)
Keywords
Background
Demographic and epidemiological data reveal that population age and health needs are progressively increasing worldwide. Similarly, health care demands, especially in emergency departments (EDs), are growing among vulnerable people with chronic illnesses, multimorbidity, polypharmacy, dependence, and other long-term conditions, with an increasing risk of drug-related problems (DRPs) requiring medical attention.1-3
Developing multidisciplinary programs for the care of frail people, those who have advanced organ failure, dementia or cognitive impairment, dependence, visual or hearing impairment, psychiatric illness, active oncological disease, and its associated syndromes, including DRPs in the ED, has been shown to improve the patient outcomes at the Hospital de la Santa Creu i Sant Pau (HSCSP, Barcelona). 1
DRPs, health problems that patients experience owing to drug use or lack thereof, 4 pose a major public health issue in Western countries. Lazarou et al 5 ranked DRPs as the fourth or sixth cause of in-hospital deaths. Moreover, 21.0% to 37.6% of consultations in-hospital EDs are estimated to be for DRPs that are mostly avoidable.6-9
DRPs are directly responsible for approximately 5% to 10% of hospital admissions, 10 and 21% of readmissions due to medication events deemed preventable in a median of 69% cases. 11 DRPs, commonly caused by widely used drugs, such as cardiovascular, alimentary tract, and metabolism system medications, are associated with an increased risk of readmission within 30 days and early hospital revisits.12,13
A statistically significant reduction in disease prevalence associated with avoidable DRPs and the readmissions they cause has direct clinical relevance to patient health. In addition, health care systems will benefit from this reduction in the utilization of avoidable resources and can allocate this budget to the prevention or treatment of other health problems.
Although DRPs are a major public health problem that generate high and often avoidable costs for health care systems,14-17 primary and secondary prevention policies have not yet been systematized in Western countries.
Some studies have demonstrated that multidisciplinary pharmaceutical care programs focused on resolving situations that potentially lead to DRPs (primary prevention of DRPs) are effective in reducing the risk of ED visits and hospitalization for any cause, especially in frail polypharmacy patients.18-22
To our knowledge, no clinical trials have explored interventions focused on patients who experience a first episode of a DRP in an outpatient setting that requires ED assistance (secondary prevention of DRPs pharmaceutical care program), although they mostly affect frail patients at a high risk of revisiting these services.
Objective
This study aimed to assess the clinical impact of a secondary prevention bundle for DRPs in patients who visited the ED for an iatrogenic disease.
Methods
Design
This was a single-center randomized controlled clinical trial. Patients were randomized (1:1) to either the DRP prevention bundle (intervention group) or usual care (control group). Neither patients nor health care professionals were blinded to the treatment group in accordance with the nature of the intervention.
This study was approved by the HSCSP Research Ethics Committee (Reference no: IIBSP-COD-2018-25). The study protocol, follow-up of enrolled patients, and data analysis were approved by the HSCSP research institute monitoring team, following the institution protocols.
The study procedure complied with the ethical principles of the Declaration of Helsinki. All participants were informed of the study characteristics and agreed to participate by providing written informed consent prior to randomization. Due to the coronavirus disease 2019 (COVID-19) pandemic, the HSCSP Research Ethics Committee authorized the investigators to request consent from patients telephonically, adding a clinical note with the details of the request for the electronic medical records.
The study was registered at ClinicalTrials.gov (Identifier: NCT03607097) before the inclusion of the first patient. This study adheres to the Consolidated Standards of Reporting Trials guidelines.
Participants and Setting
The study was conducted in HSCSP in Barcelona, a university teaching hospital in Catalonia (Spain), which includes 407 000 inhabitants and records 150 000 ED visits annually. The territorial organization of Catalonia groups the citizens into health regions depending on their postal address. 23 HSCSP is the tertiary hospital reference center of the AIS Barcelona Dreta health region. EFAD (Equip de Farmàcia Assistencial de Barcelona Dreta- Barcelona Dreta Health Care Pharmacy Team) group is a network of clinical pharmacists working collaboratively with physicians and nurses at different health care levels in the AIS Barcelona Dreta Health Region.
The Catalan health system has a shared health record. This information system allows all providers of the Catalan public and universal health system to share the complete medical history of the citizens throughout the territory.
Eligibility Criteria
Patients were eligible if they were 18 years of age or older and visited the HSCSP ED for a primary or secondary diagnosis of drug-related DRPs in the Anatomical Therapeutic Chemical Classification System (ATC) 24 groups A (alimentary tract and metabolism), B (blood and blood-forming organs), and C (cardiovascular system), according to the clinical assessment written by the emergency physician in the admission note. Each episode was classified. Patients were grouped according to the main clinical event and drug involved in the episode. Patients were excluded if they were terminally ill (life expectancy of less than 30 days) or if the DRP was associated with a suicide attempt.
The total number of patients to be recruited in this project was estimated to be 808, equally distributed between the 2 groups (404/404). The minimum detectable difference (absolute difference) in the percentage of readmissions at 30 days (main variable) was used for the power calculation, which was obtained from a previous study (14), in which the percentage of readmissions at 30 days was 22.3% in the control group and 14.3% in the intervention group (minimum expected effect size: 8.0%). The percentage of subjects lost to follow-up was set at a value not exceeding 10%. Standard values for type 1 and type 2 errors were used (α = 0.05, β = 0.20, respectively), ensuring a minimum power of 80%. Sample size calculation was performed using the GranMo 7.12 software.
Sampling, intervention, monitoring, and data recording were performed on weekdays between 8 am and 5 pm.
Intervention
Intervention consisted of a secondary prevention bundle of DRPs (DRP prevention bundle).
The DRP prevention bundle was coordinated and led by 2 clinical pharmacists together with 2 ED physicians and the EFAD pharmacist network 25 in collaboration with the rest of the health care team of their work centers (physicians and nurses). These pharmacists were chosen because their professional curriculum was representative of that of most clinical pharmacists working at an ED: a hospital pharmacist specialist with clinical skills in chronic care management and emergency procedures, demonstrated by 5 years of experience. The decision to admit a patient after consulting with the ED is the responsibility of the medical team attending them in the ED. None of the decisions to admit patients were made by the research staff in this study.
The DRP prevention bundle was applied once in the intervention group and comprised the following steps (summarized in Supplement 2):
Actions aimed at improving the chronic drug prescription of the patients
1a. Obtaining the medication chart. As part of this process, the ED pharmacist interviewed the patient or caregiver, confirmed the medication taken at home, and listed them in the electronic health record.
In Catalonia, the patient’s medical history is shared by all health care providers (Catalan Shared Medical Record, Història Clínica Compartida de Catalunya), which facilitates the sharing of clinical information by different health providers.
The Catalan Shared Medical Record includes a medication plan. This document is visible to the full assistance team of the health care system, the community pharmacy, and the patients themselves.
Interview was conducted face-to-face in the ED, except during the first wave of the COVID-19 pandemic and when the person responsible for the medication, other than the patient, could not travel to the hospital. In the last 2 cases, the interview was conducted telephonically.
1b. Medication reconciliation at each care transition. 26 The procedure followed by the Institute for Healthcare Improvement, which defines reconciliation as “the process of obtaining a complete list of the patient’s medication prior to admission and comparing it with that prescribed at the health center at admission, during transfers, and at discharge..” Discrepancies were discussed with the prescriber and corrected, if necessary. The changes made were properly documented and communicated to the next health care provider and the patient through the electromedical record.
1c. Structured patient-centered medication review. This process was performed following the method of Espaulella-Panicot et al,27,28 which is a systematic 3-step process carried out by a multidisciplinary team comprising ED physicians and a clinical pharmacist:
Step 1—Patient-centered evaluation
The main objective of this step was to determine the global care goal for each patient: survival, improving or maintaining function, and symptomatic control. The first evaluation set the stage for the second and third steps.
Step 2—Diagnosis-centered evaluation
The health problems of the patient, along with the drugs prescribed for each diagnosis, are listed. Drug purpose should fit the main care goal previously agreed upon with the patient. Special attention was paid to the prevalent disease states.
Step 3—Medication-centered assessment
Based on the goals of care derived from step 1, the purpose of step 3 was to assess the adaptation to the medications prescribed as per the clinical situation of the patient through a review of the benefit/risk of the drugs.
Actions aimed at improving the therapeutic adherence
2a. At discharge from the hospital (ED or hospital ward), the patient received a written medication plan with clear indications for their drug therapy regimen. The medication plan was included in the discharge report shared with the rest of the health care providers via electronic medical records and prescriptions.
2b. Postdischarge telephone visit: A telephone call was scheduled by the pharmacist 48 hours after discharge from the ED or hospital ward. The aim of this visit was to check whether the process that led the patient to the ED was properly resolved and whether they understood the drug therapy regimen. The pharmacist conducted a telephone visit to the person responsible for the medication (patient, caregiver, or nursing home staff).
Actions aimed at improving the health care coordination
The hospital submitted a report to the patient’s primary care team via the electronic communication system set up by the Catalan health system with the primary care pharmacist, who shared the information with the rest of the team (physicians and nurses). This report included information related to the (1) identification of the DRP that caused the ED visit, (2) medication provided at discharge, and (3) recommendations for improving the medium-to-long term drug therapy.
Patients in the control group received standard pharmaceutical care that consisted of the validation of physicians’ prescriptions during their stay in the ED and/or inpatient ward. This process consisted of reviewing the following aspects of the patient’s medication: (1) indication for each medication in relation to the patient’s acute condition and (2) appropriateness of each medication, dose, schedule, and duration of treatment for the patient’s condition.
In both groups, patients received standard ED care, including the frailty care program, if they were labeled as such in the triage area. The Hospital Sant Pau ED program of care for frailty is summarized in Reference 1 and in the attached Supplementary Material.
Study Recruitment
Patients were enrolled from August 28, 2019, to January 28, 2021, and followed up for 30 days (the final follow-up was completed on February 27, 2021).
Outcome Event Definition
Primary outcomes
Readmission within 30 days in AIS Barcelona Dreta: Patients admitted for any reason to an AIS Barcelona Dreta hospital center after attending the HSCSP ED. In both groups, this information was collected by a retrospective review of the Clinical Health Shared Record of Catalonia (CHSRC) 30 days after the patient was included.
Secondary outcomes
Readmission within 30 days in the ED: patients who revisited the HSCSP ED within 30 days for any reason. This information was collected for both groups by a retrospective review of the CHSRC 30 days after patient enrollment.
Mortality at 30 days: This was confirmed by review of the CHSRC 30 days after patient enrollment.
Time in ED: time from patient admission to discharge from the ED.
At admission, we recorded selected variables that could modify the effects of DRPs in patients treated with drugs of Anatomical Therapeutic Chemical (ATC) therapeutic groups A, B, and C, according to the information obtained in previous studies 29 : age, sex, number of medications being taken, number of chronic conditions, hypertension, diabetes mellitus, dyslipidemia, atrial fibrillation, ischemic heart disease, chronic kidney disease stage 3 or worse (estimated glomerular filtration rate <60 mL∕min∕1.73 m2), active oncological disease, heart failure, cognitive impartment according to the Global Deterioration Scale de Reisberg, 30 functional dependence according to the Bathel index score prior to the admission to ED, 31 and social support.
At discharge, we recorded the mean hospital stay duration (in days) from ED admission to discharge from the ED or the hospital.
Randomization
Randomization was performed by the hospital pharmacy department using variable block sizes generated using STATA version 13.0 ralloc.ado v3.5.2 (Stata-Corp LLC, College Station, TX, USA) with a 1:1 distribution. The application used a seed obtained by rolling 2 dice to select the row and column from a random-number table; thus, the series was replicable but unpredictable and perfectly balanced between groups in 10 case blocks.
Randomized patient selection was performed between August 28, 2019, and January 28, 2021. Assessment of eligibility and distribution across the intervention and control groups was conducted chronologically by the pharmacist according to the randomization scheme.
Statistical Analyses
Statistical analyses were conducted between January 31 and March 1, 2021. Data were analyzed according to modified intention-to-treat. Patients who died during hospitalization or those hospitalized for >30 days were excluded from the analysis because the main and secondary outcome variables could not be assessed. Baseline characteristics were tabulated according to the intervention and control groups. Multiple imputations were not made to handle the missing data. The χ2 tests were used to compare the categorical data, and parametric (t-tests) and nonparametric tests were used to compare the mean variables at baseline according to the sample distribution. To correct possible imbalances in baseline prognostic covariates despite randomization, multivariable logistic regression models were constructed to assess the associations between readmission (primary endpoint) and ED revisit (secondary endpoint) and baseline demographic and clinical characteristics. The multivariate model assumed independence of observations and minimal multicollinearity of the independent variables. Odds ratios (ORs) were calculated, corrected for variables associated with hospital readmission and revisit with a P value <0.100 in a previous bivariable analysis, providing an adjusted hospital readmission OR along with 95% confidence intervals (CIs). The following prespecified patient characteristics were used in a multivariate adjustment, based on their association with ED visits and hospital admissions29,32,33 : age over 80 years, chronic heart failure, atrial fibrillation, chronic renal failure, malignant diseases, hypertension, diabetes, ischemic cardiomyopathy, and major polypharmacy (>10 drugs in the electronic medical prescription). 34 In addition, the number needed to treat (NNT) was calculated. The analyses were conducted using Stata MP version 15.1 (Stata-Corp LLC, College Station, TX, USA). Statistical significance was considered statistically significant at P < 0.05.
Results
Patient Disposition
We invited 946 patients to participate in this study, and 808 accepted (85.4%) (Figure 1). A total of 404 patients were randomized to the usual care group and 404 to the intervention group. After randomization, 1 patient was excluded because of an administrative error that led to double inclusion, 22 patients died during hospitalization, and 16 patients were hospitalized for more than 30 days. No differences in mortality rates or prolonged hospitalizations were observed between patients selected before and after the COVID-19 pandemic. Finally, a total of 769 patients were included in the primary analysis.
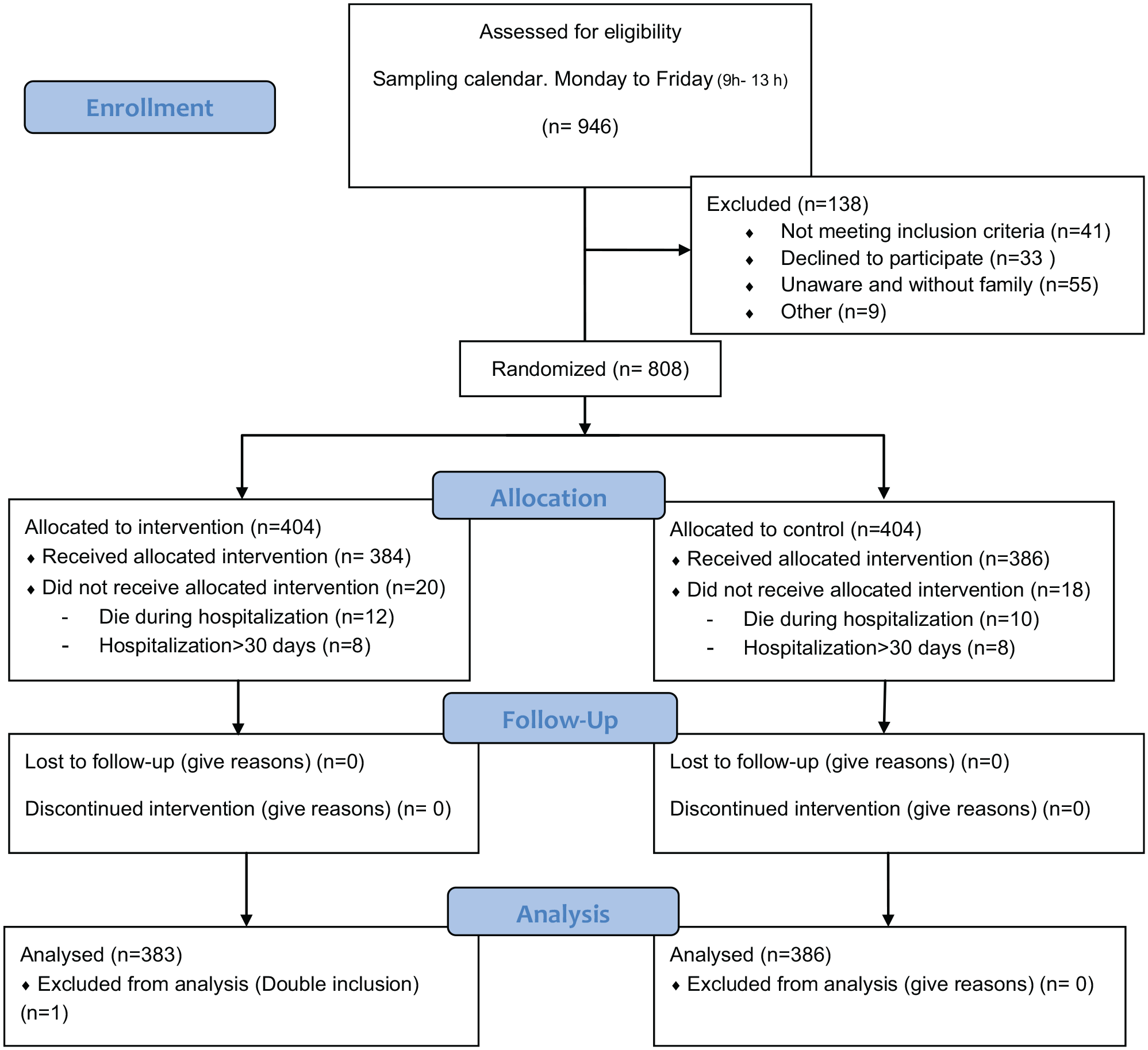
Participant flow.
Baseline characteristics of the study patients are presented in Table 1.
Baseline Characteristics of Patients.
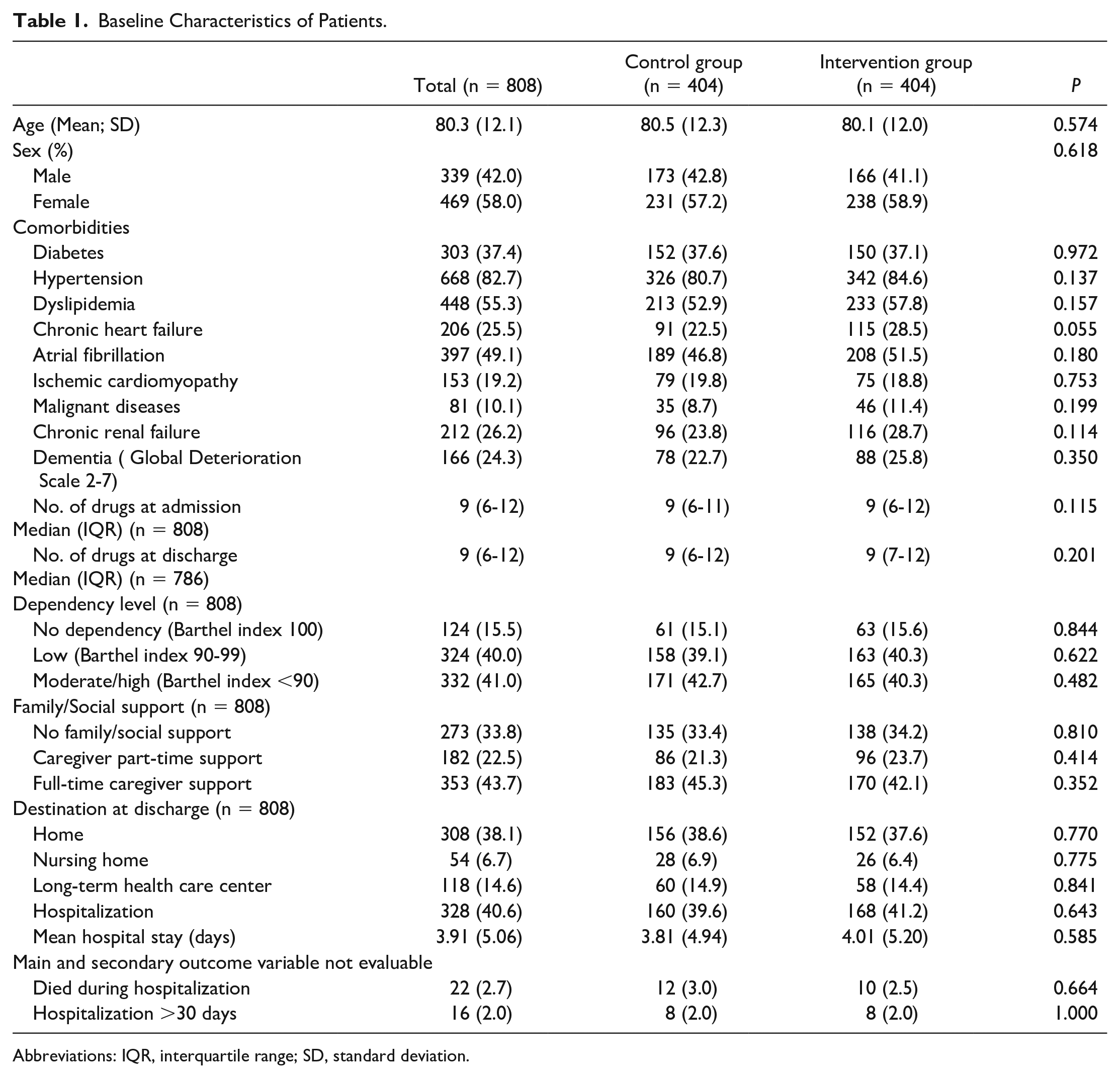
Abbreviations: IQR, interquartile range; SD, standard deviation.
The mean age of the patients was 80.3 years (standard deviation [SD]: 12.2). Drugs involved in the DRP episode belonged to ATC group A (mostly antidiabetic drugs) in 216 patients (28.1%), group B in 306 patients (39.8%) (mostly anticoagulants), and group C in 247 patients (32.1%, especially drugs with negative chronotropic effects). Most common DRPs were gastrointestinal bleeding (136, 20.3%), constipation (97, 14.6%), INR (International Normlised Ratio) alterations (67, 9.9%), and hypertensive crisis (48, 7.1%). Major causes of DRP episodes were underprescription (139, 18.1%), overprescription (117, 15.2%), drug interactions (89, 11.2%), altered drug elimination (57, 7.41%), and poor adherence to treatment (66, 8.6%). In the intervention group (n = 384 patients), the following changes were proposed at discharge: deprescription (200, 52.1%), treatment initiation (76, 19.8%), dose modification (96, 25.0%), change to other treatments (112, 29.2%), and analytical monitoring (116, 30.2%).
Among the 769 patients included in the analyses, 68 (8.8%) patients were readmitted within 30 days (control group: 40 of 386, cumulative incidence: 10.4% [95% CI: 7.5%-13.8%]; intervention group: 28 of 383, cumulative incidence, 7.3% [95% CI: 4.9%-10.3%]; P < 0.068). In the adjusted model, there was a lower incidence of hospital readmission among patients in the intervention group than those in the control group (OR: 0.59 [95% CI: 0.36%-0.97%]; P < 0.044, NNT = 32).
Regarding the secondary outcome, 127 (16.5%) patients revisited the ED within 30 days after discharge (control group: 70 of 386, cumulative incidence: 18.1% [95% CI: 14.4%-22.3%]; intervention group: 57 of 383, cumulative incidence: 14.9% [95% CI: 11.5%-18.9%]; P < 0.244). In the adjusted model, no significant differences were found in the incidence of ED revisits among patients in the intervention and control groups (OR, 0.79 [95% CI = 0.54%-1.16%]).
No significant differences were found between the intervention and control groups during 30-day readmissions based on the ATC group involved in the DRP episode (Group A: 6.2% vs. 7.5%, P = 0.312; Group B: 10.2% vs. 17.4%, P = 0.092; and Group C: 4.6% vs. 7.7%, P = 0.312). There were also no significant differences between the groups in the frequency of ED revisits at 30 days based on the ATC subgroup (Figure 2). There were no significant differences in time spent in the ED between the 2 groups (mean [SD]: 25.1 [15.1] vs 26.9 [16.1] h; P < 0.206).
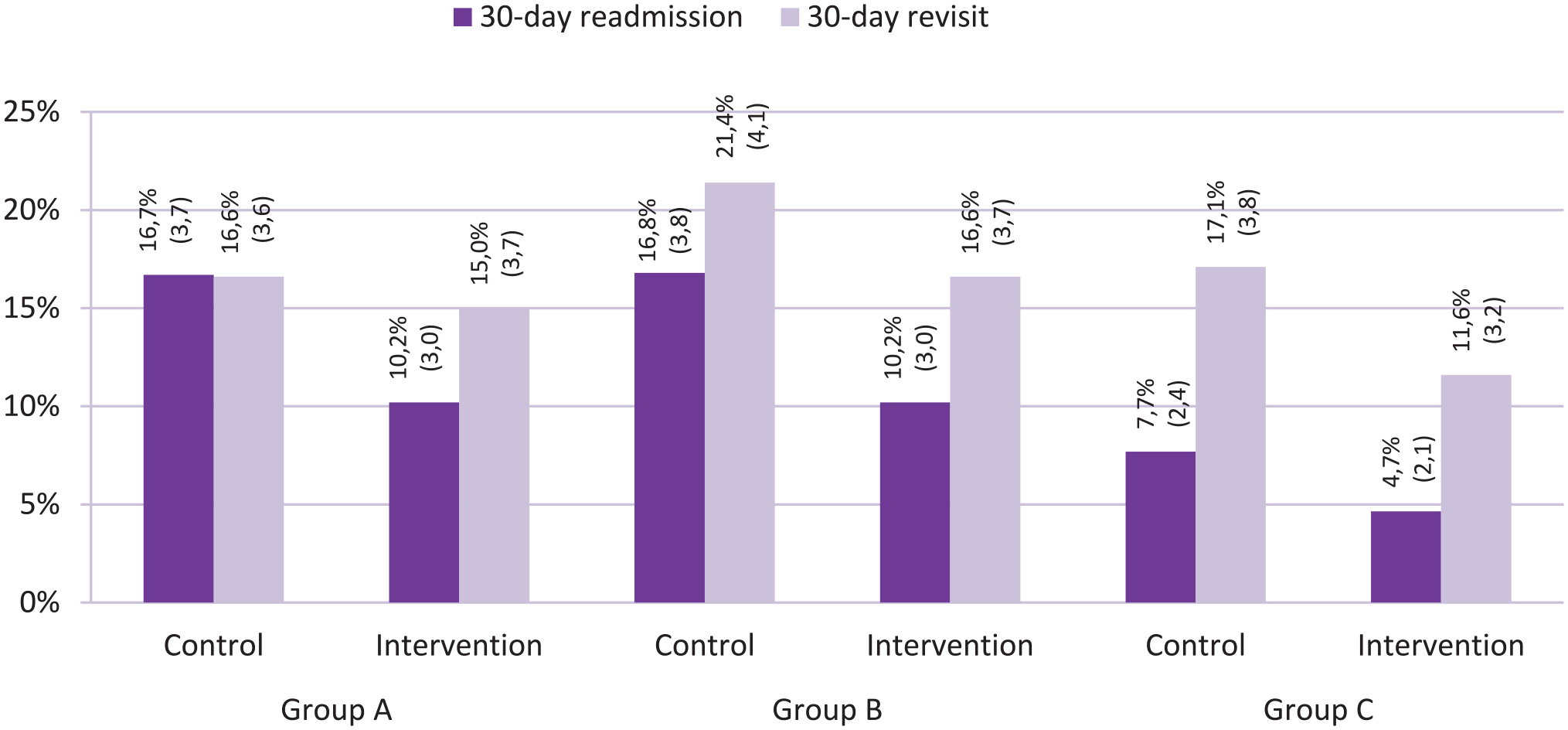
Results of percentage (SD) of 30-day readmission and 30-day ED revisit in the intervention and control groups by ATC group associated with the drug-related problem.
Finally, 36 participants died of any cause within 30 days of their index DRP (4.7%); the intervention was not significantly associated with a change in 30-day mortality (5.2% vs. 4.2%; P < 0.519).
Discussion
In this randomized clinical trial, a secondary prevention bundle for DRPs initiated in the ED by clinical pharmacists resulted in a significant decrease in early readmission for any reason (within 30 days) in patients with a first visit to the ED due to DRPs caused by cardiovascular, alimentary tract, and metabolic system medications.
Pharmaceutical care programs (interventions that usually include treatment optimization by reviewing treatment adequacy and reconciling and improving adherence) can potentially lead to DRPs.35-39 However, to the best of our knowledge, there is no conclusive evidence from a randomized clinical trial that uses the ED visits of patients with DRPs on the impact of these programs in improving clinical outcomes, such as drug-related iatrogenic illness and utilization of health care resources. This can be attributed to several factors, such as failure to include populations at specific risk of severe DRP and/or inadequate communication and collaboration with the primary care teams.29,40-44 Moreover, only a few studies have explored the usefulness of pharmaceutical assessment in ED settings, although they have been identified along with surgical areas and intensive care units as the areas of the hospital with the highest risk of patients suffering from drug-related adverse events. 45
In line with other publications addressing the same issue, the patients with DRPs in our study were mainly older women with comorbidities, advanced chronic diseases, and polypharmacy. Women have a higher risk of reporting DRPs than men, even when differences in the numbers of drug used are taken into account. 46 This population comprised high-need, high-cost (HNHC) patients characterized by their limited ability to care for themselves independently, complex social needs, such as inadequate conditions at home, poor nutrition, and poor social support relationships, 47 and increased utilization of health care resources, including ED visits, hospital admissions and readmissions after discharge for any reason,27,28 and preventable DRPs associated with inappropriate prescription (overprescription and underprescription), and nonadherence to the medication chart.29,30 Effective and efficient care for HNHC patients requires multidisciplinary teams, health care level integration, awareness of the social sphere when defining the most appropriate trajectory for the patient in the health and social system in coordination with the center’s social worker, and the implementation of preventive and empowerment plans for outpatients. 48 Our DRP prevention bundle study, like others that reported reduced utilization of health care resources associated with iatrogenic disease, includes some of these key elements: It involves a multidisciplinary team, ensures continuity of care after the patient is discharged from the acute hospital, and has an adequate sample size.49,50
The fact that most of the patients included in the study were HNHC can explain the 30-day all-cause mortality observed in the 2 study groups, although patients in their last days of life were excluded from the study. Interestingly, although no significant difference was observed, a higher number of deaths were observed in the intervention group than that in the control group. Notably, despite randomization, certain variables, such as heart failure, dementia, or active oncological disease, presented greater number of cases in the intervention group than that in the control group, which may explain these results.
Baseline characteristics of the patients in the 2 study groups were similar for all variables that could modify the effects of the registered DRPs, except for the prevalence of heart failure, which was predominant in the intervention group. In our study, chronic heart failure was associated with an increased risk of readmission of patients. Heart failure is a well-known factor associated with hospitalization. 51 Therefore, our analysis included this variable in the final model to improve the comparison between the 2 groups. Although nonsignificant differences between ATC groups were observed, patients with cardiovascular drugs involved in DRPs (ATC-C) tended to have more positive results after the implementation of the prevention bundle. Future studies should properly assess the benefits of this intervention in patients at a high risk of new consultations with the health system.
ED consultations due to DRPs are disruptive, have a significant health impact on patients, and generate high costs for the health care systems. Detection of DRPs and appropriate management in the ED are necessary to implement multidisciplinary team interventions, avoid new episodes, and reduce the DRP gap.
The Catalan health system has developed different strategies for the primary prevention of DRPs in polypharmacy patients. Establishing and evaluating policies for the secondary prevention of avoidable DRPs in patients who fail primary prevention strategies, in addition to reducing the utilization of health care resources in patients who benefit directly from them, will help in improving the primary prevention strategies already implemented in the health care system. The results of this study showed that the implementation of these set of measures at different levels of care would provide significant economic benefits, despite the need to incorporate full-time pharmacists in the ED. 52 Notably, the potential benefits of the implementation of this type of program include a reduction in the number of ED revisits and improvement in the quality of life of the patients.
Strengths and Limitations
One of the principal strengths of this medication code study is that, to the best of our knowledge, it is the first to demonstrate the usefulness of a secondary prevention program for avoidable DRPs. This study also provides evidence of a successful multidisciplinary approach for the management of HNHC patients. Moreover, the study was conducted in an ED environment, demonstrating the benefits of involving pharmacists in this setting.
This study has some limitations. First, geographical differences in health care services, including professional roles, management of chronic patients in primary care, access to certain medicines, operational functioning of the ED itself, and the unicentric character of the study, may lead to alternative outcomes in other health care settings. However, we believe that due to the type of patients (elderly and polypharmacy patients) and low complexity of related interventions (patient interview, telephone call, and contact with the next health provider via email) in this study, it can be easily extendable to other health care settings.
As this was an open randomized trial, in the control group, health professionals, other than the study investigators, may have performed practices of the intervention group beyond the standard pharmaceutical care program that includes only prescription validation, influenced by the work performed by the research team on patients in the intervention group. Likewise, the study was carried out in a center with a systematic pharmaceutical care program in the ED. Based on these 2 facts, the differences in favorable outcomes could have been of greater magnitude in favor of the program.
Due to the high variability in the types of DRPs evaluated in this study, it is difficult to determine the type of patients in which the intervention can be more effective. The analyses of the results 30 days after the inclusion of the patients in the study and not after completion of the intervention may have left little time to evaluate the effect on a reduced number of patients with long hospitalization periods after the ED visit or in those interventions coordinated with other levels of care that require a gradual application period. Based on the results of the study, future research should be carried out to evaluate the external validity of the DRP prevention bundle in other health care settings, including DRPs caused by medications other than cardiovascular, alimentary tract, and metabolic system drugs. Moreover, the effectiveness of this type of intervention on a medium-to-long term should be evaluated, with a particular focus on assessing the impact of care coordination.
Conclusions and Relevance
In the adjusted analysis, the DRP prevention bundle program decreased the 30-day hospital readmission for any cause in patients who visited the ED for a DRP associated with cardiovascular, alimentary tract, and metabolic system medications.
This study reinforces the findings of other multidisciplinary and continuity care interventions by clinical pharmacists in other care settings.
Supplemental Material
sj-pptx-1-aop-10.1177_10600280221143237 – Supplemental material for The Effect of the Drug-Related Problems Prevention Bundle on Early Readmissions in Patients From the Emergency Department: A Randomized Clinical Trial
Supplemental material, sj-pptx-1-aop-10.1177_10600280221143237 for The Effect of the Drug-Related Problems Prevention Bundle on Early Readmissions in Patients From the Emergency Department: A Randomized Clinical Trial by Ana Juanes, Jesús Ruíz, Mireia Puig, Marta Blázquez, Antoni Gilabert, Laia López, M. Isabel Baena, Josep M. Guiu and Maria Antònia Mangues in Annals of Pharmacotherapy
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received the following financial support for the research, authorship, and/or publication of this article: funds from the Spanish Ministry of Health (Carlos III Health Institute, ISCIII) FONDOS FEDER through the Fondo de Investigación para la Salud (FIS; PI18/00889). The funder had no roles in the study design, data collection and analysis, decision to publish, and manuscript preparation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.