
Abstract
Objective:
To provide updates on the epidemiology and recommendations for management of candidemia in patients with critical illness.
Data Sources:
A literature search using the PubMed database (inception to March 2023) was conducted using the search terms “invasive candidiasis,” “candidemia,” “critically ill,” “azoles,” “echinocandin,” “antifungal agents,” “rapid diagnostics,” “antifungal susceptibility testing,” “therapeutic drug monitoring,” “antifungal dosing,” “persistent candidemia,” and “Candida biofilm.”
Study Selection/Data Extraction:
Clinical data were limited to those published in the English language. Ongoing trials were identified through ClinicalTrials.gov.
Data Synthesis:
A total of 109 articles were reviewed including 25 pharmacokinetic/pharmacodynamic studies and 30 studies including patient data, 13 of which were randomized controlled clinical trials. The remaining 54 articles included fungal surveillance data, in vitro studies, review articles, and survey data. The current 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Management of Candidiasis provides recommendations for selecting empiric and definitive antifungal therapies for candidemia, but data are limited regarding optimized dosing strategies in critically ill patients with dynamic pharmacokinetic changes or persistent candidemia complicated.
Relevance to Patient Care and Clinical Practice:
Outcomes due to candidemia remain poor despite improved diagnostic platforms, antifungal susceptibility testing, and antifungal therapy selection for candidemia in critically ill patients. Earlier detection and identification of the species causing candidemia combined with recognition of patient-specific factors leading to dosing discrepancies are crucial to improving outcomes in critically ill patients with candidemia.
Conclusions:
Treatment of candidemia in critically ill patients must account for the incidence of non-albicans Candida species and trends in antifungal resistance as well as overcome the complex pathophysiologic changes to avoid suboptimal antifungal exposure.
Keywords
Introduction
Candidemia is recognized as a major cause of morbidity and mortality in the health care environment. 1 In fact, candidemia is associated with a 47% attributable mortality, with higher rates in critically ill patients. Previous data suggest that mortality is most closely linked with increased time to optimal therapy and/or inadequate source control. 2 According to the 2019 US Centers for Disease Control and Prevention (CDC) Antibiotic Resistance Threats report, Candida auris and drug-resistant Candida species were identified as urgent and serious threats in the United States, respectively. 3 Notably, the COVID-19 pandemic impacted resistance at an alarming rate with recent data demonstrating a 26% increase in azole-resistant Candida species and a 60% increase in C. auris from 2019 to 2020. 4 In addition, fungicide use and agrochemicals have sparked concern for cross-resistance to medicinal antifungal agents. 5
In patients with critical illness, candidemia remains an ongoing challenge to treat. To this end, understanding methods to optimize therapeutic modalities is crucial. The antifungal armamentarium is growing, and new agents may mitigate drug-drug interactions, toxicity, and constraints in administration routes. 6 In addition, optimization of dosing strategies in the critically ill, especially those who are obese, is vital. Therapeutic drug monitoring (TDM) may serve as a modality to optimize dosing strategies. Finally, interpretation and application of susceptibility breakpoints into clinical practice to guide therapeutic decision-making is critically needed to improve patient outcomes. 7 The purpose of this review is to address the emerging challenges surrounding antifungal selection, dosing, and susceptibility testing to optimize therapy in critically ill patients with candidemia.
Data Sources
A literature search using the PubMed database and conference abstracts was conducted using the search terms “invasive candidiasis,” “candidemia,” “critically ill,” “azoles,” “echinocandin,” “antifungal agents,” “rapid diagnostics,” “antifungal susceptibility testing,” “therapeutic drug monitoring,” “antifungal dosing,” “persistent candidemia,” and “Candida biofilm.” Reference lists of included articles and abstracts were reviewed to identify additional studies of relevance. Articles and abstracts were considered for inclusion in addition to ongoing trials identified through ClinicalTrials.gov. The final literature search was conducted on March 31, 2023.
Study Selection and Data Extraction
A total of 109 articles were reviewed including 25 pharmacokinetic/pharmacodynamic (PD) studies and 30 studies including patient data, 13 of which were randomized controlled clinical trials. The remaining 54 articles included fungal surveillance data, in vitro studies, review articles, and survey data.
Data were extracted to provide updates on the epidemiology and recommendations for management of candidemia in patients with critical illness.
Data Synthesis
The current 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Management of Invasive Candidiasis provides recommendations for selecting empiric and definitive antifungal therapies for patients with candidemia. 1 However, data are limited regarding optimized dosing strategies in patients who are critically ill with dynamic pharmacokinetic changes, which may be complicated by persistent candidemia or biofilm formation. Moreover, newly approved agents and rapid diagnostic platforms have become available since these guidelines were published.
Notably, the selection of empiric antifungal therapy in critically ill patients without microbiologic documentation of candidemia is complex and depends on patient-specific characteristics which are beyond the scope of this review.
Epidemiology of Candidemia in Patients With Critical Illness
The most common species causing candidemia in critically ill patients vary based on geographic, institutional, demographic, and clinical practice characteristics. 8 Candida albicans historically accounts for 40% to 70% of cases worldwide, but isolation of non-albicans Candida species has been increasing over the last decade. Candida glabrata (now known as Nakaseomyces glabrata) is the second most common in the United States, United Kingdom, northern Europe, and Australia, whereas Candida parapsilosis and Candida tropicalis are the second most common in other parts of the world.9-11 An increasing number of reports have been published implicating C. auris as an emerging cause of candidemia, including those with critical illness.9,12,13 Notably, C. auris can adhere to surfaces throughout hospital environment despite routine decontamination measures. 14 The incidence of C. auris may be underestimated as specialized methods are required to prevent misidentification. 15 Inaccurate or delayed identification of the specific Candida species may prolong the time to appropriate antifungal administration. As such, reliable and rapid identification of the causative Candida species is of great value, especially in patients who are critically ill.
Rapid Diagnostic Platforms in Candidemia
Isolation of Candida species from blood cultures remains the gold standard for diagnosis. 1 However, the sensitivity of blood cultures is poor (~50%) 16 and most blood culture systems require 1 to 3 days for growth with an additional 1 to 2 days needed to identify the organism.2,17 These delays present significant barriers in initiating culture-driven treatment.
Some laboratories may use commercial platforms to decrease the time needed to identify Candida species to expedite optimal treatment for candidemia, such as matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS),8,18,19 FilmArray Blood Culture Identification 2 (BCID2) (BioFire, Salt Lake City, Utah), 20 peptide nucleic acid fluorescence in situ hybridization (PNA-FISH),8,21 T2Candida Panel (T2 Biosystems, Lexington, Massachusetts),17,22 or ePlex BCID Panels (GenMark Diagnostics, Carlsbad, California)23,24 (Table 1). Unlike the other platforms which require positive blood cultures before use, T2Candida can detect C. albicans, C. tropicalis, C. krusei (now known as Pichia kudriavzevii), C. glabrata, and C. parapsilosis from whole blood within 3 to 5 hours, independent of positive blood cultures. While these platforms have great potential to improve management of candidemia, 25 decisions will depend on the Candida species and likelihood of fluconazole susceptibility as none detect resistance mechanisms or provide antifungal susceptibility data.
Commercial Platforms to Identify Candida Species in Patients With Candidemia.
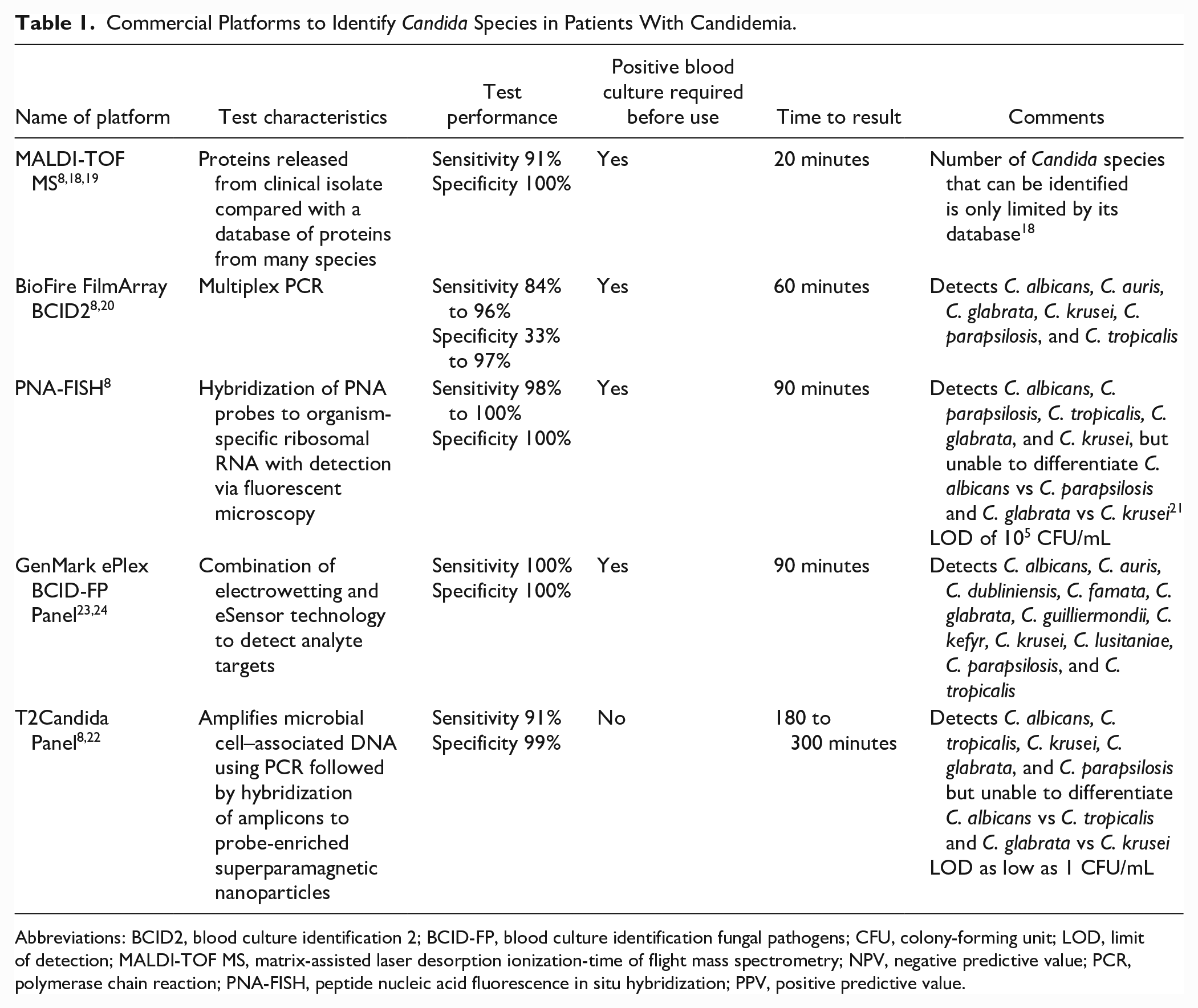
Abbreviations: BCID2, blood culture identification 2; BCID-FP, blood culture identification fungal pathogens; CFU, colony-forming unit; LOD, limit of detection; MALDI-TOF MS, matrix-assisted laser desorption ionization-time of flight mass spectrometry; NPV, negative predictive value; PCR, polymerase chain reaction; PNA-FISH, peptide nucleic acid fluorescence in situ hybridization; PPV, positive predictive value.
Antifungal Susceptibility Testing
Antifungal susceptibility among Candida species is often predictable, though recent data have increasingly recognized the emergence of drug-resistant Candida species and C. auris. 3 Analysis of data from the CDC and SENTRY program demonstrated an increasing prevalence of C. glabrata and C. parapsilosis as well as a gradual increase in fluconazole and echinocandin resistance in the United States.26,27 In addition, greater utilization of antifungal therapies due to the widespread use of immunomodulatory therapies and the COVID-19 pandemic coupled with the agrochemical-induced resistance strengthens the need for antifungal susceptibility testing (AFST) in patients with candidemia.5,28,29
Indeed, the 2016 IDSA Clinical Practice Guideline for the Management of Invasive Candidiasis recommends AFST should be performed for Candida species isolated from blood cultures. 1 Despite these recommendations, AFST is not widely available. Surveillance data from 9 US sites found that AFST was performed in approximately 50% of patients with candidemia. 30 Echinocandin susceptibility was performed in fewer than 50% of cases caused by C. glabrata or C. parapsilosis. In many cases, patients with candidemia were transitioned from an echinocandin to fluconazole without AFST. Access to and utilization of AFST is critical when managing patients with candidemia to ensure appropriate definitive antifungal selection.
Modalities for AFST include a variety of methods such as broth microdilution, gradient diffusion strips (Etest; bioMérieux, Inc., Hazelwood, Missouri, or MIC test strip [MTS]; Liofilchem, Inc., Waltham, Massachusetts), Sensititre YeastOne assay (Thermo Scientific, TREK Diagnostic Systems, Cleveland, Ohio), and Vitek 2 fungal susceptibility cards (Vitek 2; bioMérieux, Inc., Hazelwood, Missouri). 31 The AFST remains in its infancy compared with bacterial susceptibility testing and is more limited in available breakpoints. In some situations, epidemiological cutoff values (ECVs) may be an asset in comparing isolate minimum inhibitory concentration (MIC) values with ECV, helping differentiate wild-type and acquired or mutational resistance population; however, ECVs are not available for all Candida species. 32 In addition, understanding of essential agreement or standard error and the limitations of different testing modalities is important when evaluating the reported MIC value. 31
Although each AFST has its own merits and limitations, there are some notable issues and barriers. Unfortunately, AFST requires fungal growth, which is slow, time-consuming, and unreliable in some cases.31,33 Even if protocols are standardized, fungal yield is subject to inoculum size, incubation temperature, incubation time, and in vitro phenomena, yielding substantial variability in interpretation.7,31,33 Trailing growth is a phenomenon with azoles where some Candida species are incompletely inhibited and appear to grow at higher dilutions, leading to possible misrepresentation of results. Furthermore, the Eagle effect is a phenomenon where distinct regrowth may restart at higher dilutional concentrations, possibly due to an upturn in cell wall chitin to compensate for the decrease in β-1,3- and β-1,6-glucan.7,31 Finally, AFST and clinical outcomes have been ambiguous without definitive results, likely due to the aforementioned spectrum of variability.
Emerging strides in advancement have started to shift away from “conventional” AFST and trended toward more culture-independent platforms, similar to that of bacterial multiplex polymerase chain reaction (PCR) platforms. Luminex MagPix assay (Luminex Corporation, Austin, Texas) detects various FKS mutations, which are known regions for mutations causing echinocandin resistance.7,31,33 Unfortunately, developing these types of molecular systems is challenging because molecular mechanisms of resistance must be known and well-studied. As such, in some cases, resistance may be secondary to multiple mechanisms, as seen in some azole-resistant Candida species.
Despite these limitations, there appears to be promising advancements on the horizon, such as flow cytometry, multiplex microsphere PCR, whole-genome sequencing, and MALDI Biotyper antibiotic (antifungal) susceptibility test rapid assay (MBT ASTRA), which may help obviate some of the concerns with conventional AFST once widely available.31,33-36
Echinocandins Versus Azole Antifungals for Candidemia in Patients With Critical Illness
Echinocandins are recommended by the 2016 IDSA Clinical Practice Guideline for the Management of Candidiasis as preferred empiric therapy for candidemia in critically ill patients who are hemodynamically unstable, previously exposed to an azole, and in those colonized with azole-resistant Candida species. 1 Alternatively, high-dose fluconazole (12 mg/kg) is acceptable for patients with candidemia who are hemodynamically stable, colonized with azole-susceptible Candida species, or have no prior azole exposure. However, a pooled analysis that included 1915 patients with candidemia and other forms of invasive candidiasis from 7 randomized trials found that initial treatment with an echinocandin was associated with significantly lower mortality and higher clinical success. 37 There have been 12 randomized trials that evaluated efficacy of treatment with polyene antifungals, azole antifungals, and echinocandins in patients with invasive candidiasis, some of whom had candidemia.38-49 Out of these, 11 demonstrated noninferiority between the regimens. One of the more recent trials did not demonstrate noninferiority of caspofungin versus isavuconazole. 47 In this study, patients with invasive candidiasis (84% with candidemia only) received either intravenous isavuconazole or caspofungin for 10 days followed by optional step-down therapy to oral isavuconazole or oral voriconazole, respectively. There was a lower clinical response at the end of treatment who had received isavuconazole compared with caspofungin (61% vs 72%), regardless of illness severity. Similar findings at the end of intravenous treatment were observed among patients with candidemia (65% vs 72%, respectively). A secondary analysis of critically ill patients included in a randomized trial comparing anidulafungin with fluconazole for invasive candidiasis and candidemia demonstrated improved response rates in the anidulafungin group at the end of intravenous treatment (71% vs 54%). 50 These findings support the use of echinocandins as preferred empiric therapy in patients with candidemia, especially those who are critically ill.
For definitive therapy, there was no difference in clinical and microbiological response at the end of treatment among patients with invasive candidiasis and candidemia treated with an echinocandin for at least 5 days who continued on an echinocandin compared with those transitioned to an oral azole. 51 Additional studies have demonstrated similar findings and support the recommendation to transition to an oral azole.39,41,42,52,53 As such, IDSA guidelines recommend transitioning from an echinocandin to oral azoles after 5 to 7 days of treatment in patients who are clinically stable with a functional gastrointestinal tract, azole-susceptible Candida species, and sterile repeat blood cultures. 1 The role for transitioning to an azole prior to 5 days of echinocandin therapy as a result of rapid pathogen identification is uncertain, though a recent multicenter post hoc analysis suggested early de-escalation to fluconazole within 5 days was appropriate for hemodynamically stable patients with candidemia caused by an azole-susceptible isolate who had undergone source control. These evidence-based recommendations must be considered alongside multiple other factors including AFST, antifungal penetration in cases of candidemia with metastatic foci, drug interactions, and clinical factors (eg, renal or hepatic dysfunction, cardiac conduction abnormalities), many of which are common in critically ill patients.
Impact of Obesity on Antifungal Therapy
The prevalence of obesity in US adults has increased significantly from 30.5% in 2000 to 41.9% in 2020. 54 The increase in volume of distribution (V) of antifungals in obesity 55 and changes in volume and clearance (CL) of antimicrobials in critically ill patients 56 have been well described. Changes in antifungal pharmacokinetics (PK) and suggested dosing modifications for critically ill patients with obesity are discussed below.
Echinocandins
Although echinocandins are recommended for critically ill patients with candidemia, dosing recommendations for patients with obesity are not included in guideline recommendations. 1 Findings from 3 prospective PK studies of anidulafungin in persons who were obese or critically ill supported dose increases of 25% to 50% for those who are morbidly obese or weigh 140 to 150 kg (Table 2).57-59 These dosing recommendations were developed to provide similar exposures (area under the curve [AUC] of approximately 100) seen in patients with normal body weight (60-80 kg), but the optimal PK/PD target for anidulafungin is unknown.
Pharmacokinetic and Pharmacodynamic Studies of Echinocandins in Persons With Obesity.
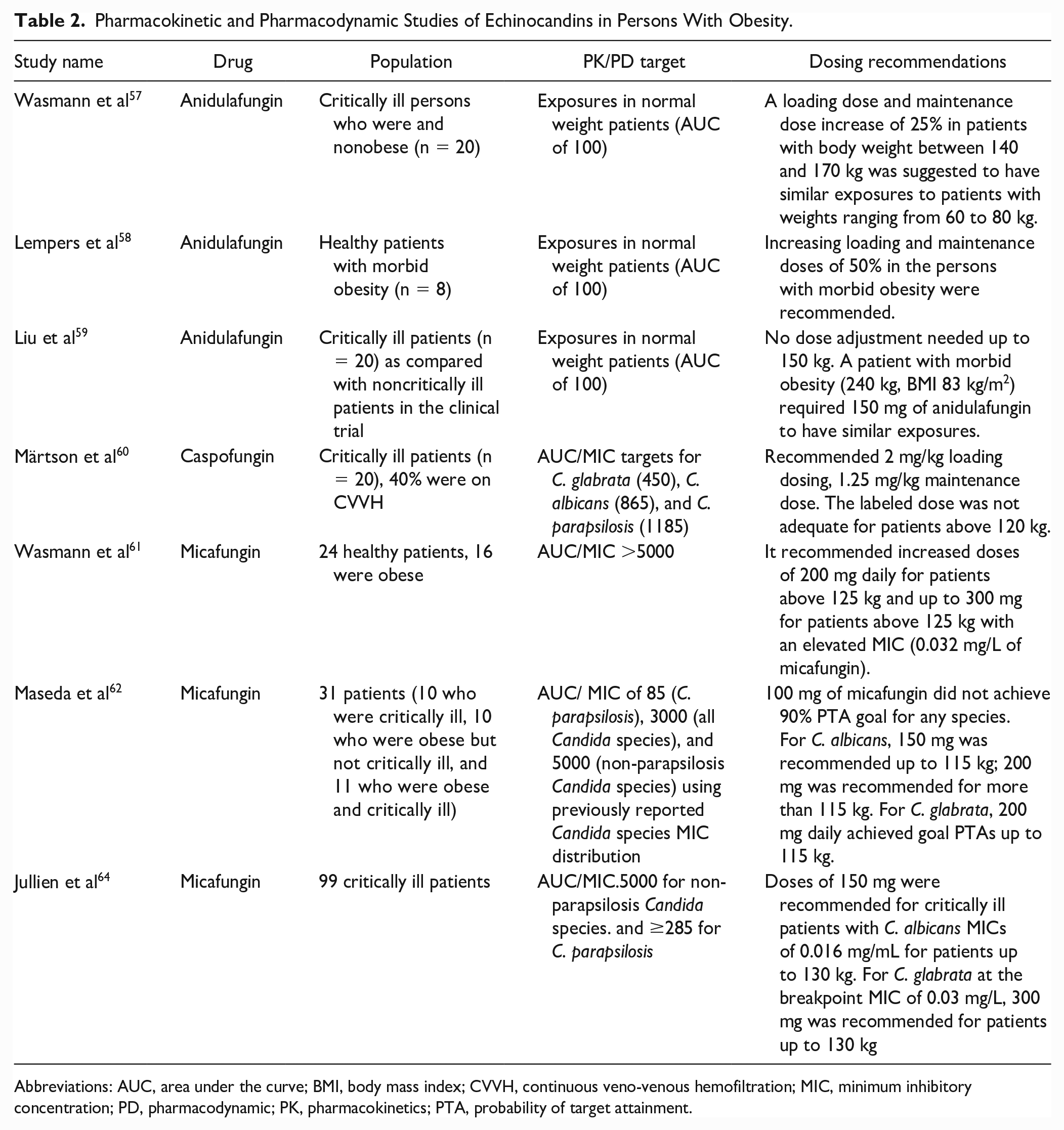
Abbreviations: AUC, area under the curve; BMI, body mass index; CVVH, continuous veno-venous hemofiltration; MIC, minimum inhibitory concentration; PD, pharmacodynamic; PK, pharmacokinetics; PTA, probability of target attainment.
The impact of body weight class (underweight, normal, overweight, obese, and morbid obesity) on anidulafungin was examined in a single-center retrospective study of patients with candidemia treated with anidulafungin 100 mg with a primary outcome of 30-day mortality. 65 Of the 173 patients included, 41% were obese, 69% had evidence of severe sepsis, and almost all (99%) had an infectious diseases consult. Weight class was not associated with differences in 30-day mortality (36% vs 26% vs 32% vs 34%, respectively).
A post hoc analysis of the caspofungin clinical trials for invasive candidiasis (n = 232) and empiric therapy (n = 546) showed similar rates of favorable response between patients who were obese (20% of the patients included) and nonobese (73% vs 77% and 33% vs 40%, respectively). 66 The proportion of critically ill patients in these trials was not described. A prospective PK study of 18 healthy patients who received a single dose of caspofungin demonstrated that caspofungin V and CL increases with body weight. 67 Based on these findings, higher caspofungin doses (2 mg/kg loading dose and 1.25 mg/kg maintenance dose) are recommended in critically ill patients (Table 2). 60
The CL of micafungin increases allometrically with weight through at least 43 to 155 kg. 68 Data from 3 PK studies of micafungin in patients who were obese or critically ill suggested doses of up to 300 mg should be used for patients with obesity, but are dependent on body weight and MIC.61,62,64 A retrospective single-center cohort study of 80 patients, of which 35% were obese, with candidemia examined the impact of obesity on outcomes. 69 Most (72.5%) received micafungin 100 mg as their treatment. Intensive care unit (ICU) admission was not stated, but 20% of patients were ventilated. Patients with obesity had a longer duration of candidemia (6 vs 5 days, P = 0.02) and infection-related length of stay (19 vs 13 days, P = 0.05). In-hospital mortality (21.4% vs 13.5%, P = 0.36) was numerically higher in the obese patients. A retrospective cohort of 23 adults examined the safety of higher doses of micafungin. 70 The median dose was 300 mg and most (60.9%) were in the ICU when treatment was initiated. Of those included, the median body mass index (BMI) was 37.1 kg/m2 and 70% were obese. Liver function tests remained stable despite treatment with high-dose micafungin.
Fluconazole
Up to a third of critically ill patients treated with fluconazole will not meet PK/PD targets, most often due to underdosing. 71 There is a paucity of data regarding fluconazole dosing in patients with obesity who are critically ill. Fluconazole concentrations were obtained from 21 critically ill patients (52% were obese) to perform population PK analysis and Monte Carlo dosing simulations. 72 Based on these results, the study recommended fluconazole 12 mg/kg as a loading dose followed by 6 mg/kg as a maintenance dose, both based on total body weight, for Candida species with MICs of 2 mg/L. Notably, these dosing recommendations follow current IDSA guidance. 1
Voriconazole
The other azole which has considerable data in obesity is voriconazole; however, the recommendations for dosing weight are nebulous. 73 Although controversial, previous data suggested use of total body weight in patients with BMI <35 kg/m2 and adjusted body weight in those with BMI ≥35 kg/m2 for initial doses would achieve similar exposures initially, which could then be optimized by TDM. 74
The extent of the dose increase of these agents depends on body weight and AFST. Limited data from retrospective studies in critically ill patients are unclear if increased doses improve outcomes. Therapeutic drug monitoring is also recommended for critically ill patients with obesity 75 but is not readily available for all antifungals used to treat candidemia. However, total body weight should influence echinocandin (at least 25% dose increase if more than 80 kg, but specific to each agent), fluconazole (12 mg/kg as a loading dose followed by 6 mg/kg as a maintenance dose, both based on total body weight), and voriconazole (adjusted body weight if BMI ≥35 kg/m2 for initial doses then adjusted based on TDM) dosing in critically ill patients with obesity being treated for candidemia.
Impact of RRT/ECMO on Antifungal Therapy for Candidemia
Critically ill patients may require temporary mechanical support as assistance for overcoming organ failure. 76 Common support mechanisms include renal replacement therapy (RRT) and extracorporeal membrane oxygenation (ECMO). While mechanical support can aid in the treatment of critically ill patients, it alters the PK of drugs and presents the challenge of providing adequate pharmacologic management.
Extracorporeal membrane oxygenation is a cardiopulmonary bypass device used to support patients with refractory respiratory and/or cardiac failures. 76 Optimal drug dosing in ECMO is unknown due to the PK alterations through 3 primary mechanisms: direct circuit extraction, increased V, and altered CL.
Vascular catheter removal, which is critical component for managing candidemia, 1 is often impossible for patients on ECMO, therefore relying on optimal therapeutic dosing of antifungal agents for therapy. Data for antifungal PK alterations are emerging, but still lacking, with the majority arising from children and ex vivo studies. Two drug properties that can be used to predict the impact of drug sequestration in ECMO are lipophilicity and protein binding. The lipophilicity of a compound is indicated by the octanol/water partition coefficient (logP) with higher positive values indicating increased lipophilicity and greater drug sequestration. 77 Drugs with higher protein binding are also subject to greater sequestration, despite similar lipophilicity.
Fluconazole (logP: 0.4-0.56; 12% protein binding) has demonstrated a significantly higher V but an unchanged CL during ECMO. 78 In an ex vivo study comparing closed-loop circuit configurations, fluconazole was not extracted, indicating minimal drug sequestration and therefore requiring no empiric dosing change. 79 In comparison, voriconazole (logP: 1, 58% protein binding) has demonstrated significant sequestration with up to 70% drug loss. 80 Two case reports of voriconazole use in ECMO used an increased dose initially, but due to inter-patient variability and time-dependent saturation, supra-therapeutic concentrations were later observed.81,82 Therefore, standard voriconazole dosing with routine TDM is recommended. Isavuconazole (logP: 3.4-4; >99% protein binding) has limited data. In one case report, the plasma trough was below than that of clinical trials when standard dosing (372 mg/d) was used but goal troughs were achieved when the dose was doubled (372 mg twice/d), indicating drug sequestration and warranting an increased dose. 83
Micafungin (logP: −1.5; >99% protein binding) has demonstrated increased V and CL during ECMO. 84 In an ex vivo study, micafungin recovery was low, ranging from 26% to 57% at 24 hours, indicating significant drug sequestration. These data suggest that the dosing should be increased for patients on ECMO. 79 In comparison, caspofungin (logP: <0.17; 97% protein binding) has also been studied in ex vivo ECMO models and critically ill adult patients. Conflicting data have demonstrated minimal to moderate drug sequestration and indicate a small adjustment in dosing may be required.80-82
The current data for antifungal dosing in patients with candidemia who are undergoing ECMO can be used as a guide; however, further studies are needed to better understand PK changes and identify optimal drug dosing.
When assessing antifungal dosing for patients with candidemia requiring RRT, there are data to determine the appropriate dose, including manufacturer recommendations. Modalities of RRT available in the ICU include both hemodialysis and continuous renal replacement therapy (CRRT). For the purpose of this review, the discussion will focus on CRRT. Factors to consider when determining drug clearance during CRRT include effluent flow rate, filter type, and method of renal replacement.
Fluconazole, isavuconazole, and voriconazole are not significantly dialyzable and do not require a dosage adjustment for CRRT. Of note, the intravenous formulations voriconazole contain the excipient sulfobutylether-β-cyclodextrin (SBECD), which may cause toxicity if accumulation occurs. Limited data suggest that SBECD removal by CRRT is adequate and usual indication-specific doses of these agents may be used.85,86
Caspofungin and micafungin are highly protein bound and unlikely to be removed by RRT, so standard dosing is appropriate. However, emerging data demonstrated lower plasma concentrations during the first days of treatment. A PK study including patients requiring CRRT treated with caspofungin showed that a 2-compartment linear model best described the drug concentrations. Compared with standard dosing (70 mg once followed by 50 mg daily), an increased loading dose of 100 mg better achieved the desired PK/PD targets. 87 A similar PK study was conducted with micafungin among patients receiving CRRT and the standard dose (100 mg daily) failed to achieve PK/PD targets in patients with Candida species demonstrating higher MIC values. 88 Given these data, higher micafungin doses in patients receiving CRRT are warranted, but more data are needed to determine optimal dosing strategies.
TDM for Antifungal Therapy for Candidemia
Numerous physiologic changes occur during critical illness that can affect the PK of antifungal agents. As such, it is important to ensure PD targets are achieved for antifungal agents in critically ill patients. Therapeutic drug monitoring can be used to optimize exposures while limiting the risk of potential toxicities but is not routinely performed for most antifungal agents used to treat candidemia.
Anidulafungin
Although the PD indices for anidulafungin are not fully defined, AUC0-24/MIC, Cmax/MIC, and Cmin of 1 mg/L are the most common targets associated with favorable outcomes. 89 Greater variability in AUC for anidulafungin has been observed critically ill patients when compared with those not requiring care in the ICU,90-92 as well as persons with obesity.57-59 Higher anidulafungin doses are often needed to optimize exposure, which suggests a potential role for TDM in patients with unpredictable PK parameters (eg, critically ill patients with obesity).
Caspofungin
Similar to anidulafungin, previous studies identified more variability in AUC for caspofungin in critically ill patients.93,94 Alternatively, a recent meta-analysis showed that the AUC for caspofungin was not significantly affected by critical illness. 95 While the clinical significance of these contradictory findings is unclear, TDM for caspofungin may be most appropriate for patients with unpredictable PK parameters (eg, critically ill patients with obesity).
Micafungin
Target AUC0-24/MIC for micafungin has been recommended to ensure optimal exposure against C. albicans (goal 3000), C. parapsilosis (goal 285), and non-parapsilosis Candida species (goal 5000). 96 Serum albumin ≤25 g/L, sepsis-related organ failure assessment (SOFA) score ≥10, and increased body weight were associated with lower micafungin exposure.62,64 Therapeutic drug monitoring is not routinely recommended for micafungin but may be beneficial to ensure AUC0-24/MIC goals in critically ill patients with obesity.
Fluconazole
AUC0-24/MIC and dose/MIC indices for fluconazole that are associated with improved clinical outcomes are >55.2 to 100 and >100, respectively. 97 Critical illness, body weight, augmented renal function, and continuous veno-venous hemofiltration may affect fluconazole exposure.71,98 Previous data suggest weight-based dosing is more likely than “standard dosing” to achieve PK/PD targets in critically ill adults with Candida species displaying higher MICs.71,72,98,99 While TDM-guided dosing may be useful in certain situations (eg, those undergoing RRT), it is not routinely recommended as weight-based dosing (12 mg/kg as a loading dose followed by 6 mg/kg as a maintenance dose, both based on total body weight) often achieves optimal exposure. 89
Voriconazole
Voriconazole displays Michaelis-Menten kinetics and is further subject to variable clearance due to CYP2C19 polymorphisms. 73 Support for TDM with azole therapy is perhaps best demonstrated with voriconazole in patients with invasive aspergillosis, though the 2016 IDSA Clinical Practice Guideline for the Management of Invasive Candidiasis recommends target trough concentrations of 1 to 5.5 mg/L. 1 However, the data supporting routine TDM in patients treated with voriconazole for candidemia are limited and likely extrapolated from experience in managing patients with invasive candidiasis without concomitant candidemia and invasive aspergillosis. 100
Isavuconazole
Limited data are available to establish PK/PD targets for isavuconazole as previous studies did not establish a need for TDM.89,101 However, a retrospective study of 41 critically ill adults being treated for invasive aspergillosis or other invasive fungal infections identified lower isavuconazole exposure in patients with BMI ≥25 mg/kg 2 or SOFA score ≥12. 101 Outcomes were not evaluated based on isavuconazole concentrations, so the clinical significance of these findings is unknown. Therapeutic drug monitoring is not routinely recommended for patients receiving isavuconazole, though more data are needed to determine whether standard dosing regimens achieve optimal exposure in critical illness.
Pharmacodynamic targets for most antifungal agents used to treat candidemia are not well defined and TDM assays are not widely available. However, multiple reports suggest greater variability in antifungal exposure in patients exhibiting unpredictable PK parameters, which suggests a potential role for TDM-guided dosing to optimize clinical outcomes.
Persistent Candidemia in Patients With Critical Illness
Persistent candidemia occurs in 8% to 93% of cases and is often associated with higher rates of treatment failure and worse outcomes, though the definitions used in various studies are heterogeneous. 102 Risk factors associated with persistent candidemia include host factors (eg, comorbidities, neutropenia), ineffective antifungal therapy due to inadequate concentrations or resistance, inadequate source control, endovascular infections, and infections associated with prosthetic material.
Indwelling vascular catheters or intravascular prostheses (eg, cardiac devices, vascular grafts) in the setting of candidemia may be complicated by biofilm formation and likely contribute to persistent candidemia due to the extracellular matrix, reduced antifungal susceptibility from decreased antifungal penetration, adherence to antifungal therapies, development of persister cells, mixed Candida-bacterial biofilm formation, or quorum sensing.63,103,104 While Candida species differ in their ability to form biofilms, biofilm formation diminishes antifungal activity often requiring removal or replacement of indwelling devices. In addition, the impact of biofilm formation on mortality remains unclear.105,106
Strategies to combat persistent candidemia include selection of antifungal therapy with potent activity against biofilms or deployment of combination therapy. Candida albicans biofilms exerted high levels of resistance to fluconazole at physiologic concentrations, whereas high concentrations of amphotericin B, including lipid formulations, demonstrated potent anti-biofilm activity and decreased biofilm dispersion. 107 Despite higher MICs, echinocandins retain activity against most Candida species biofilms, particularly when concentrations remain at least 2 µg/mL.108,109 While most combinations of antifungal therapies produced indifferent results against biofilms, amphotericin B and posaconazole demonstrated synergistic activity against C. albicans biofilms. 110 Although outcome data are limited, patients with candidemia who were treated with anti-biofilm antifungal therapies had decreased length of hospitalization, but applicability to critically ill patients is unknown. 105
Use of combination therapy for candidemia is limited to a single randomized control trial which was conducted prior to the introduction of the echinocandin class as well as newer azoles such as posaconazole and voriconazole. Rex and colleagues described use of amphotericin B deoxycholate (0.6-0.7 mg/kg/d) plus fluconazole 800 mg daily for non-neutropenic candidemia other than C. krusei. 49 The findings indicated the concurrent use of fluconazole and amphotericin B is not antagonistic and led to faster clearance of blood cultures. Overall success rates were 56% (60 of 107 patients) with use of fluconazole monotherapy compared with 69% (77 of 112 patients; P = 0.043) with combination therapy. Notably, the time to failure analysis did not indicate benefit with use of combination therapy. The results of this study, while intriguing, are limited by the availability of safer more effective antifungal agents for patients with candidemia. Animal model data are suggestive of benefit with azole plus echinocandin therapy; however, persistent disease is often attributed to lack of source control and/or deep-seated infection versus antifungal failure. 111
Novel Options for Candidemia in Critically Ill Patients
Treatment of candidemia in critically ill patients remains challenging due to the increasing rates of fluconazole and echinocandin resistance demonstrated in Candida species along with the dosing discrepancies for many of the available antifungal agents. New antifungal therapies, some with novel mechanisms of action, may offer opportunities to circumvent the disadvantages associated with current therapies.
Ibrexafungerp
Ibrexafungerp is a triterpenoid antifungal derived from enfumafungin and in a new class of “fungerps” antifungals. Although ibrexafungerp has a similar mechanism of action as echinocandins which inhibit fungal 1,3-β-glucan synthase, ibrexafungerp is also a triterpenoid glucan synthase inhibitor. As a result, ibrexafungerp is not affected by the resistance mechanism that limits activity of echinocandins and demonstrated potent in vitro activity against C. auris, C. albicans, C. parapsilosis, C. tropicalis, C. glabrata, and C. krusei. In an ongoing phase 3 open-label and single-arm study evaluating use of ibrexafungerp (administered once daily) for severe fungal infections (FURI), 73% of patients with candidemia experienced clinical improvement at the end of treatment (Table 3). 112 Notably, ibrexafungerp does not require dose adjustments for renal or hepatic dysfunction, but decreased doses are recommended when used concomitantly with strong CYP3A4 inhibitors and use is contraindicated in pregnancy. Given its novel mechanism of action and activity against drug-resistant Candida species, ibrexafungerp may be useful in patients with candidemia who are critically ill, though more data comparing outcomes with echinocandins are needed before widespread use.
Novel Options for Candidemia in Critically Ill Patients.
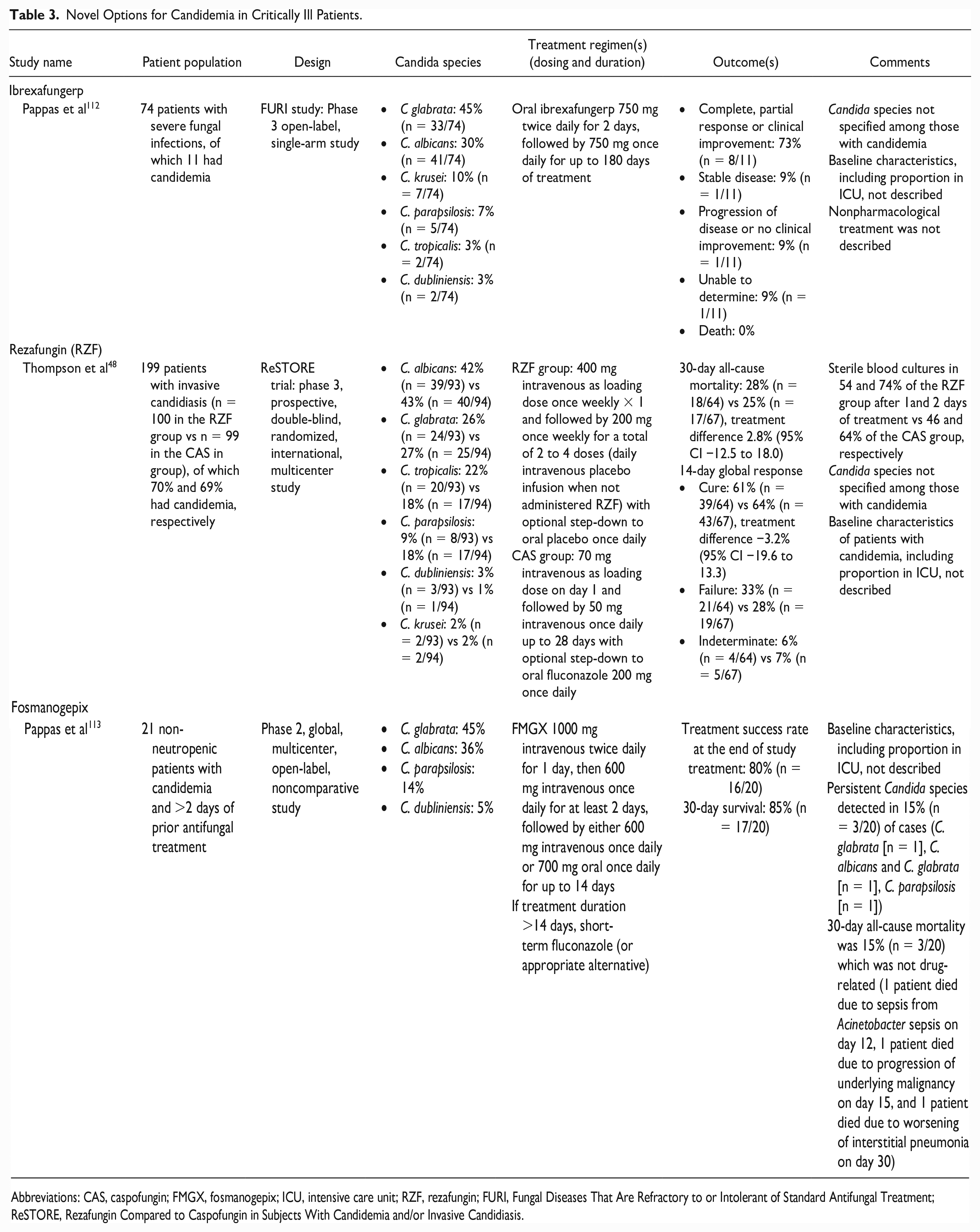
Abbreviations: CAS, caspofungin; FMGX, fosmanogepix; ICU, intensive care unit; RZF, rezafungin; FURI, Fungal Diseases That Are Refractory to or Intolerant of Standard Antifungal Treatment; ReSTORE, Rezafungin Compared to Caspofungin in Subjects With Candidemia and/or Invasive Candidiasis.
Rezafungin
Rezafungin (RZF) is a long-acting echinocandin and structural analogue of anidulafungin with a half-life of 130 hours permitting once-weekly dosing while retaining all the advantages of the current echinocandins. 114 Similar 14-day global response and 30-day mortality were observed among patients with candidemia treated with RZF and caspofungin in the phase 3 ReSTORE trial. 48 Interestingly, RZF sterilized blood cultures faster than caspofungin, though this did not translate in improved clinical outcomes. Dose adjustments are not needed for renal or hepatic dysfunction or when administered concomitantly with cyclosporine, ibrutinib, mycophenolate mofetil, or venetoclax. 115 While RZF decreased time to blood culture sterilization, it is likely best reserved for definitive therapy in patients with candidemia given its PK properties.
Fosmanogepix
Fosmanogepix (FMGX), the first and only Gwt1 inhibitor, inhibits fungal enzyme Gw1 (mannoproteins), which is the enzyme required for the synthesis of glycosylphosphatidylinositol-anchored mannoproteins to the fungal cell wall. 116 The FMGX demonstrated potent in vitro activity against most Candida species, except C. krusei, but similar activity against fluconazole-susceptible and nonsusceptible Candida species. In a phase 2 open-label study non-neutropenic patients with candidemia, 80% experienced success at the end of treatment and 85% survived at 30-day follow-up. 113 Among those with Candida species nonsusceptible to amphotericin B, anidulafungin, or fluconazole, treatment success was demonstrated in 71% (n = 10/14) of patients and 30-day survival was 93% (n = 13/14). The FMGX was safe and effective in patients with mild to severe renal impairment (estimated glomerular filtration rate 22-86 mL/min), whereby 86% (n = 12/14) experienced treatment success and 79% (n = 11/14) survived at 30-day follow-up. While FMGX appears useful in treating patients with candidemia, no data are available on use in patients with critical illness.
Relevance to Patient Care and Clinical Practice
Improved recognition and management of candidemia in critically ill patients are essential to combat the high morbidity and mortality. While an increasing number of rapid diagnostic platforms are available, institutional availability is limited and all except the T2Candida require positive blood cultures before use. Many of the platforms can detect the most common Candida species, but some group species based on antifungal resistance patterns. Although this improves the process of selecting antifungal therapy, clinicians are forced to rely on historic susceptibility patterns as resistance mechanisms and susceptibility information are not detected by rapid diagnostic platforms. These issues coupled with the changing epidemiology of candidemia in critically ill patients solidify the need for AFST for all Candida species isolated from blood cultures.
The trends for fluconazole resistance and non-albicans Candida species in critically ill patients with candidemia previously described warrant the use of echinocandins as empiric therapy for. Depending on the likelihood of fluconazole resistance or AFST, fluconazole can be used as step-down therapy. While previous studies support this approach, there is no consensus for dosing recommendations to account for the dynamic pharmacokinetic changes observed in those with critical illness. Therefore, our review provides recommendations to optimize antifungal dosing based on body weight, RRT, or ECMO, and potential roles for TDM. In addition, the development of novel antifungals may help address the increasing rates of resistance and complex pathophysiologic changes impacting exposures to the antifungals currently used in treating candidemia.
Conclusion
Despite the introduction of rapid diagnostic platforms and novel antifungal agents, management of candidemia in the ICU remains complex. Many centers are unlikely to have access to rapid diagnostic testing (RDT) or AFST in general, in addition to the novel therapeutic agents. Pathogen identification is a pivotal decision point significantly influencing morbidity and mortality outcomes. Clinicians should recognize the impact of patient-specific variables commonly seen in critically ill patients including the need for RRT and dosing adjustments which may be necessary in those who are obese. The plausible benefit of novel agents is predicated on identification; however, real-world clinical experience with these agents in critically ill patients is needed to better define their place in therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.