
Abstract
Background
Different clinical trials for recurrent or metastatic nasopharyngeal carcinoma have studied different combinations of immuno-oncology in first-line treatment, but the optimal choice has not been determined.
Objective
To systematically examine and compare the efficacy and safety of different immune checkpoint inhibitors (ICIs) combined with chemotherapy as first-line treatment for recurrent or metastatic nasopharyngeal carcinoma.
Methods
Several electronic databases were systematically searched up to February 2023. Articles meeting the inclusion criteria were included.
Results
Three RCTs were eligible in the study. Compared with placebo plus gemcitabine-cisplatin (GP), toripalimab plus GP (HR = 0.59, 95% CI: 0.37-0.95) was significantly associated with a better OS. Tislelizumab plus GP generated best progression-free survival (PFS) benefit (HR = 0.50, 95% CI: 0.37-0.67), greatest improvement in 1-year PFS rate (RR = 3.00, 95% CI: 1.84-5.22), and objective response rate (ORR) (RR = 1.26, 95% CI: 1.04-1.53) over the placebo plus GP. Furthermore, tislelizumab plus GP appeared to be safer than toripalimab plus GP and camrelizumab plus GP in terms of adverse events (AEs)-grade ≥3, treatment-related AEs (TRAEs)-grade ≥3, serious AEs (SAEs), treatment-related SAEs (TRSAEs), and AEs leading to discontinuation of treatment.
Conclusion and Relevance
In recurrent or metastatic nasopharyngeal carcinoma, programmed death 1 (PD-1) inhibitors plus GP as first-line treatment have better survival outcomes than placebo plus GP with comparable toxicity. Toripalimab plus GP shows the best OS benefit over placebo plus GP, while tislelizumab plus GP generates the best PFS, 1-year PFS rate, ORR, and safety. Tislelizumab plus GP could be the best choice among the ICIs combined with chemotherapy regimens as first-line treatment in recurrent or metastatic nasopharyngeal carcinoma.
Keywords
Introduction
Nasopharyngeal carcinoma is a kind of head and neck cancer originating from nasopharyngeal epithelial cells. 1 Nasopharyngeal carcinoma has 3 pathological subtypes: keratinizing squamous, non-keratinizing, and basaloid squamous. 1 Non-keratinizing nasopharyngeal carcinoma could be categorized into differentiated and undifferentiated tumors. Non-keratinizing subtype accounts for the majority of cases (>95%) in endemic regions and is principally related to EBV infection; the keratinizing subtype is found in less than 20% of cases worldwide, and is comparatively rare in endemic regions. 1 Epidemiological trends over the past decade have suggested that nasopharyngeal carcinoma has a distinct geographic distribution, with a particular prevalence in East and Southeast Asia. 2 In recent years, the treatment of nasopharyngeal carcinoma has improved and its incidence has decreased worldwide due to medical advances and improvements in public health. However, 70% of patients are still diagnosed at an advanced stage with a poor prognosis. Patients with recurrent or metastatic nasopharyngeal carcinoma have limited treatment options. Platinum-based dual chemotherapy regimen, preferably gemcitabine combined with cisplatin (GP), is generally considered as the standard first-line treatment for patients with recurrent or metastatic nasopharyngeal carcinoma. However, current conventional treatments are often associated with limited efficacy. Therefore, novel therapeutic strategies are urgently needed to further improve the prognosis of patients with nasopharyngeal carcinoma.
In recent years, immune checkpoint inhibitors (ICIs), particularly programmed death 1 (PD-1) and programmed death-ligand 1 (PD-L1) inhibitors, have become a promising therapeutic strategy for various malignancies including nasopharyngeal carcinoma. 3 Several PD-1 inhibitors, such as camrelizumab and toripalimab, have been evaluated in recurrent or metastatic nasopharyngeal carcinoma. Camrelizumab and toripalimab monotherapies were approved by the National Medicinal Products Administration (NMPA) for refractory recurrent or metastatic nasopharyngeal carcinoma in 2021. Various combination approaches, including radiotherapy, chemotherapy, targeted therapy, or other immunotherapeutic agents have been investigated due to the promising therapeutic effect and manageable safety profile of PD-1/PD-L1 inhibitors. According to the results of CAPTAIN study, NMPA approved camrelizumab combined with GP regimen as the first-line treatment for recurrent or metastatic nasopharyngeal carcinoma in June 2021. 4 In November 2021, NMPA approved toripalimab combined with GP regimen as the first-line treatment for recurrent or metastatic nasopharyngeal carcinoma according to the outcomes of the JUPITER-02 study. 5
However, there is no head-to-head trial comparing the different ICIs-based regimens as the first-line therapy in recurrent or metastatic nasopharyngeal carcinoma. Thus, we performed the network meta-analysis to identify the optimal ICIs-based regimen in the treatment of recurrent or metastatic nasopharyngeal carcinoma.
Methods
We conducted this network meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist and its extension for network meta-analysis.6,7 A protocol of the study was registered with PROSPERO (CRD42023397881).
Search Strategy
We conducted a systematic search from their inception to February 2023 in PubMed, Web of Science, EMBASE, and Cochrane Library databases. Keywords for searching were “nasopharyngeal carcinoma or nasopharyngeal neoplasm or nasopharyngeal cancer,” “immune checkpoint inhibitor or PD-1 or PD-L1 or CTLA-4 or names of specific immune checkpoint inhibitors.” The detailed search strategy was shown in Supplementary Table 1. Conference abstracts were also reviewed. To find other eligible articles, we also manually reviewed the references of retrieved studies.
Study Selection
The inclusion criteria were: (1) randomized phase II or III clinical trial, (2) patients were diagnosed with recurrent or metastatic nasopharyngeal carcinoma, and (3) studies evaluated the efficacy and safety of ICIs-based regimen as the first treatment for recurrent or metastatic nasopharyngeal carcinoma. Exclusion criteria were: (1) non-RCTs, such as observational study, case report, review, meta-analysis, and study protocol, (2) mixed tumors, and (3) insufficient data.
Data Extraction
The data extraction was independently performed by 2 authors. The extraction data mainly included the study name, inclusion period, country, names of ICIs, dosing regimen, number of patients and study outcomes. The main outcomes of overall survival (OS), progression-free survival (PFS), 1-year PFS rate, objective response rate (ORR), and adverse events (AEs) were extracted in each study. In addition, available data from subgroup analyses were extracted.
Risk of Bias Assessment
The Cochrane Risk of Bias Tool was used to evaluate the quality of included RCTs. 8 Evaluation criteria included random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and researchers (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other bias. Each risk of bias was categorized as either low, unclear, or high risk after assessment.
Statistical Analysis
This study was to compare the efficacy and safety of ICIs combined with chemotherapy as first-line treatment for recurrent or metastatic nasopharyngeal carcinoma. The survival outcomes of OS and PFS were expressed as HRs with 95% CIs. The 1-year PFS rate, ORR, and incidence of AEs evaluated using risk ratios (RRs) and 95% CIs. The statistical heterogeneity among studies was assessed by Cochrane’s Q test and I2 values. If no significant heterogeneity existed (P > 0.10), the fixed effect model was selected for analysis. Otherwise, the random effects model was used. A P value less than 0.05 was considered statistically significant. All statistical calculations were performed using gemtc, netmeta, and BUGSnet packages in R.4.3.0.
Results
Search Results and Characteristics of Included Clinical Trials
A total of 3606 articles were initially identified through the search strategies after the removal of duplicates. By title and abstract screening, 142 articles were chosen for full-text review. After rigorous screening, only 3 trials (6 articles) were finally included in this study (Figure 1).5,9-13 All the 3 studies (CAPTAIN-1st, JUPITER-02, and RATIONALE-309) were phase III trials and investigated the efficacy and safety of PD-1 inhibitors plus chemotherapy (GP) compared with placebo plus chemotherapy (GP) in recurrent or metastatic nasopharyngeal carcinoma. All the PD-1 inhibitors in the 3 trials were different. The main characteristics of the 3 trials are shown in Table 1.
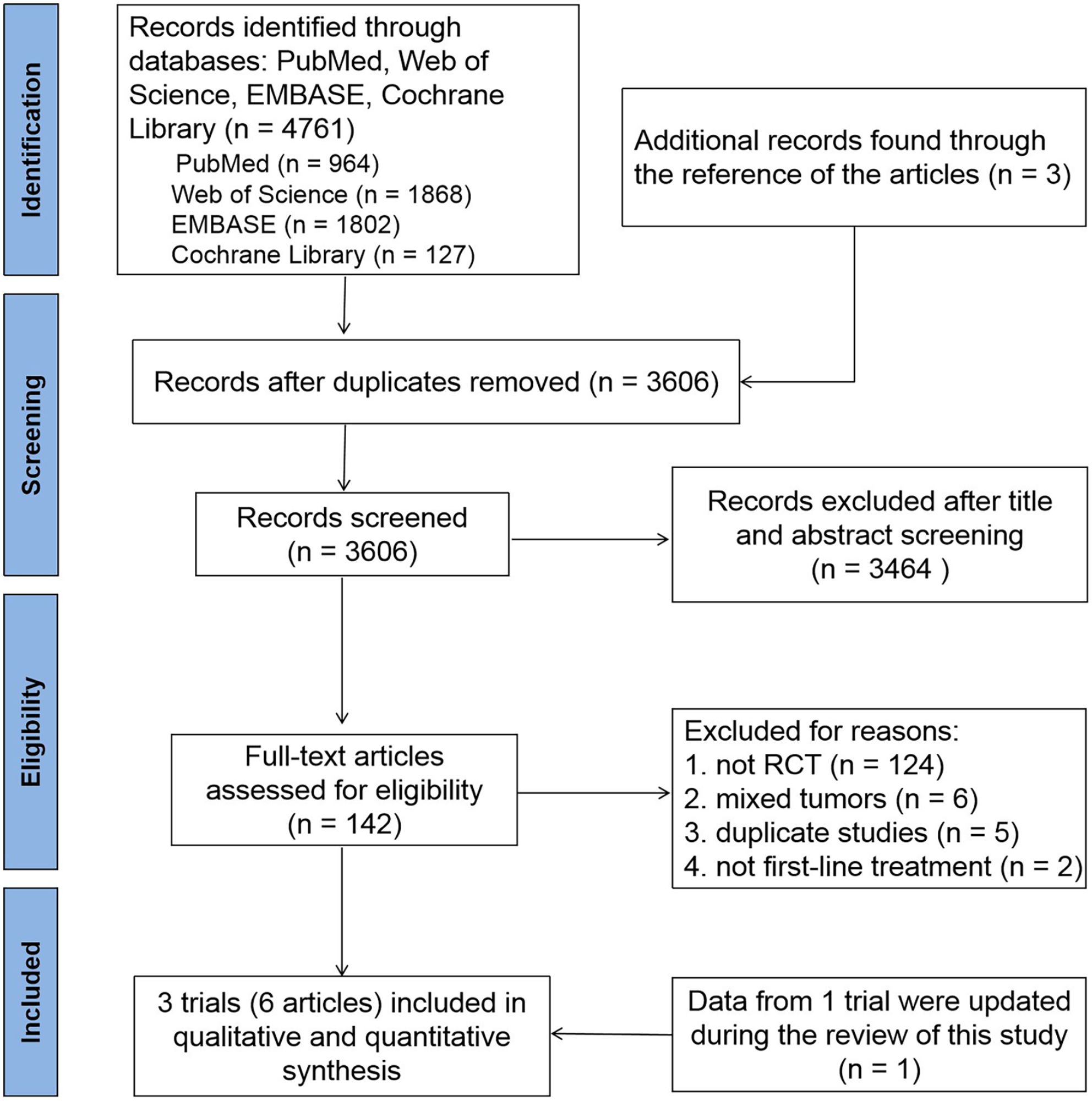
PRISMA flowchart of the identification and inclusion of studies.
Baseline Characteristics of Included Trials.
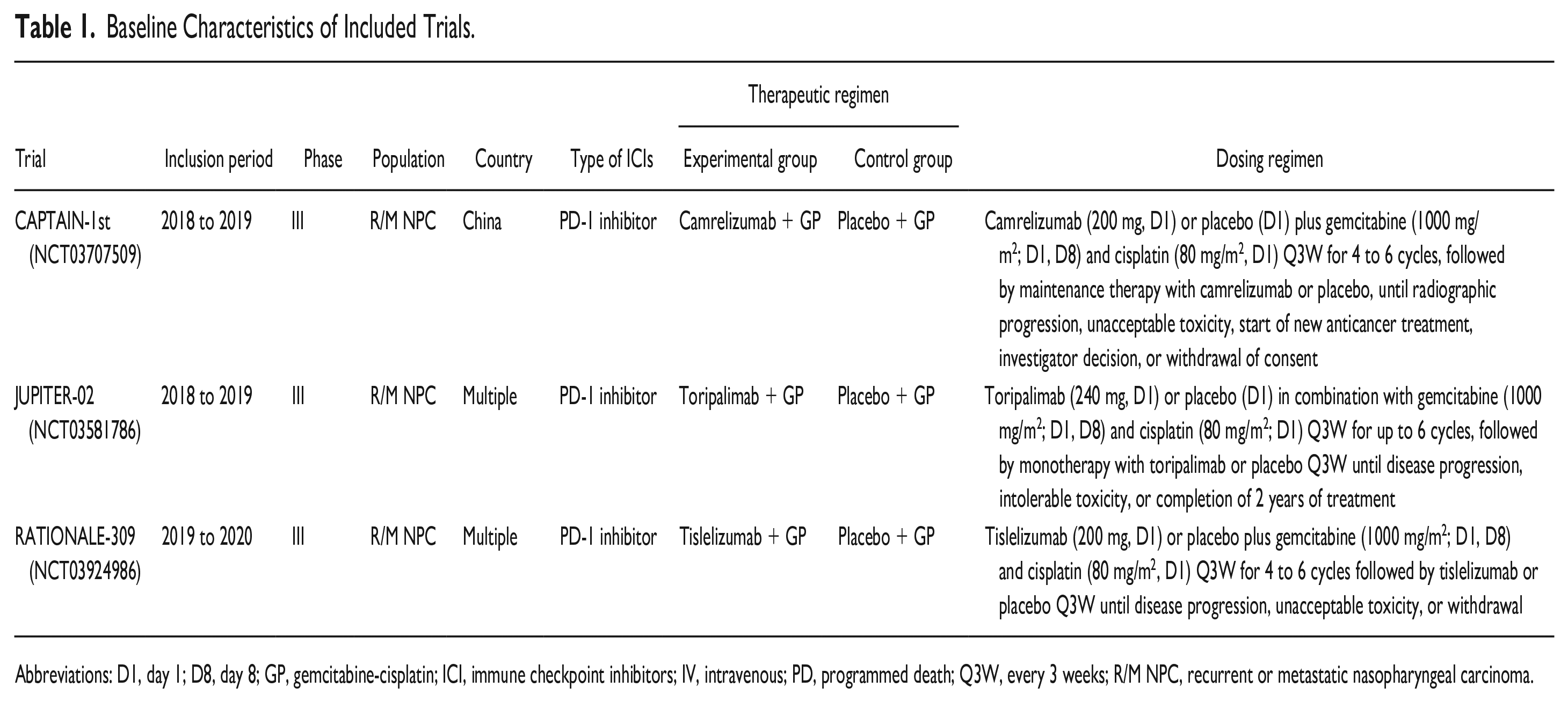
Abbreviations: D1, day 1; D8, day 8; GP, gemcitabine-cisplatin; ICI, immune checkpoint inhibitors; IV, intravenous; PD, programmed death; Q3W, every 3 weeks; R/M NPC, recurrent or metastatic nasopharyngeal carcinoma.
Methodological Quality Assessment
The quality of included RCTs was assessed by the Cochrane Risk of Bias Assessment Tool. The detailed bias risk for each trial is shown in Figure 2. The methodological assessment was influenced by the overall low risk of bias and provided very good quality.
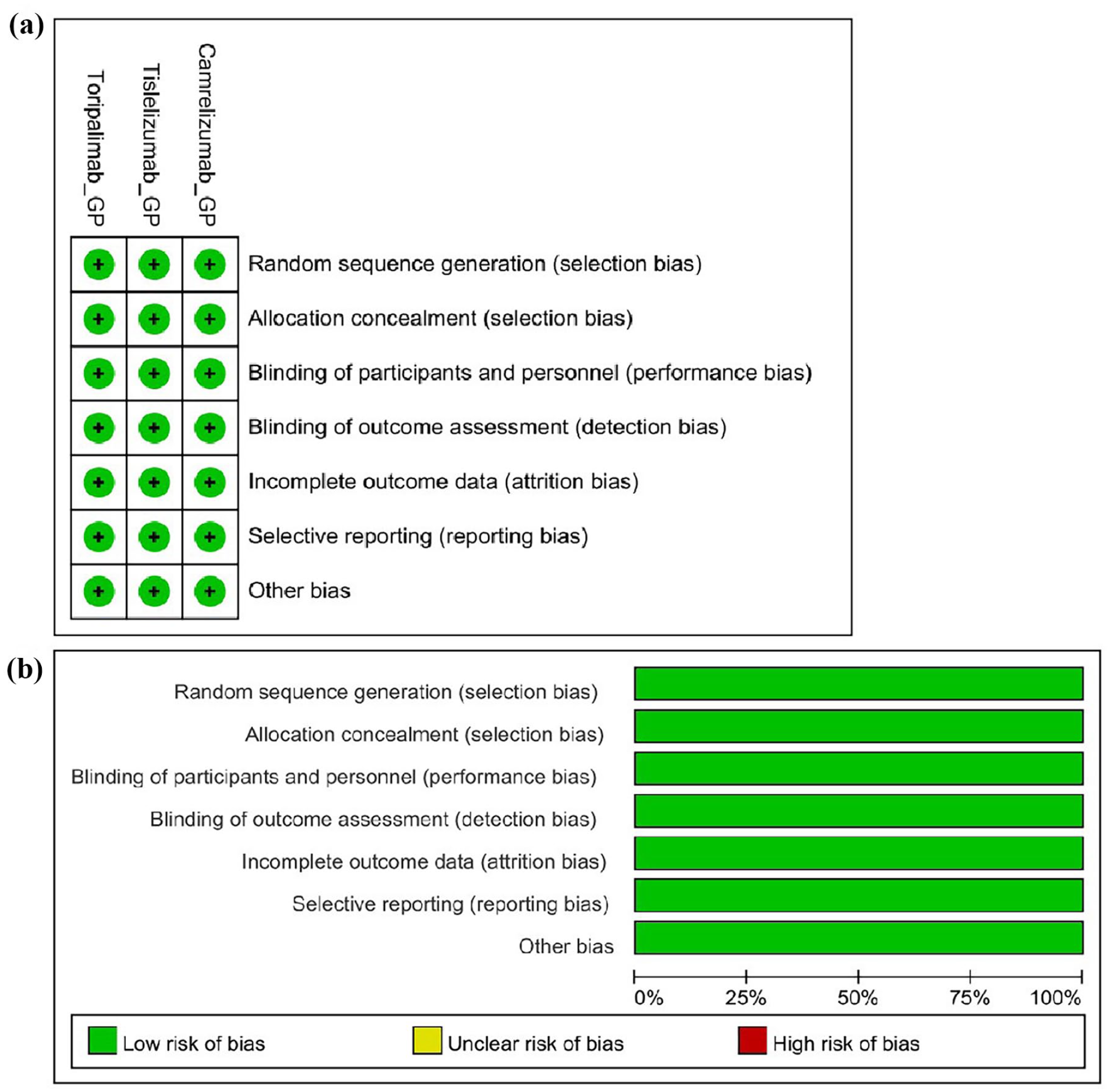
Quality assessment of included randomized controlled trials (RCTs): (a) risk of bias summary and (b) risk of bias graph.
Network Meta-Analysis of Efficacy
The network evidence plots of RCTs that assessed survival outcomes are shown in Figure 3. Since just 3 RCTs were included, we performed the network analysis only for survival outcomes reported in all the 3 RCTs. There was no obvious heterogeneity and inconsistency in this study (Supplementary Table 2).
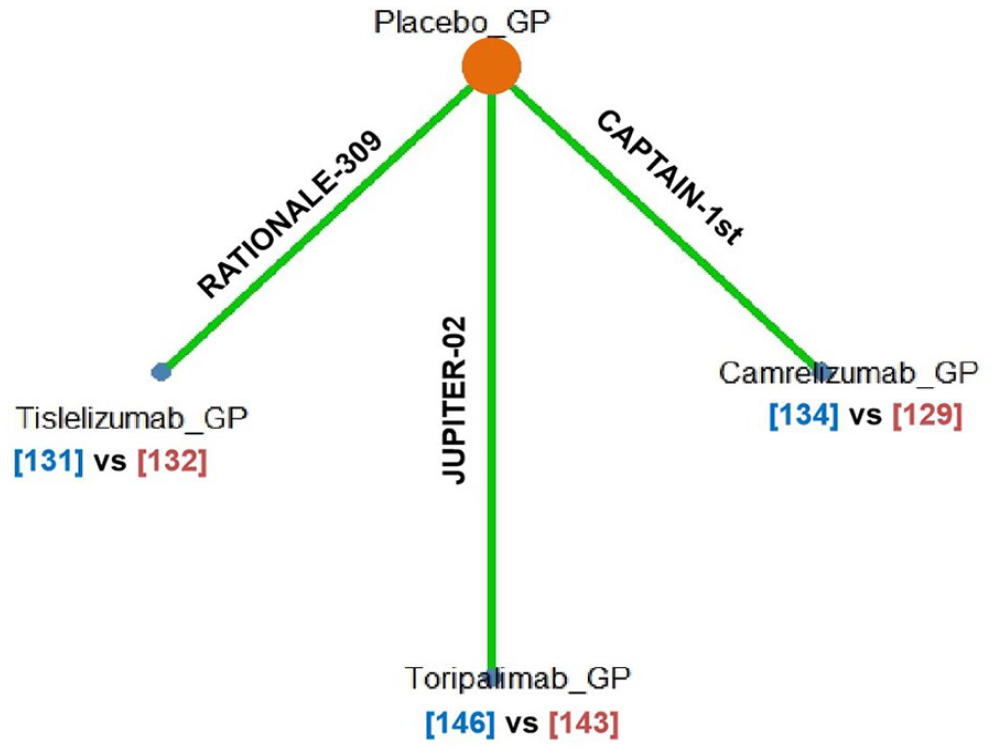
Network evidence plots of randomized controlled trials (RCTs) that assessed survival outcomes and adverse events.
Pooled results for direct comparison of efficacy analysis are shown in Figure 4. Compared with placebo plus GP, toripalimab plus GP (HR = 0.59, 95% CI: 0.37-0.95) was significantly associated with a better OS. Tislelizumab plus GP (HR = 0.60, 95% CI: 0.35-1.01) and camrelizumab plus GP (HR = 0.67, 95%: 0.41-1.11) were associated with a favorable trend in OS than placebo plus GP. On the basis of Bayesian analysis and treatment ranking analysis according to surface under the cumulative ranking curve (SUCRA), it was highly likely that toripalimab plus GP emerged as the best treatment regimen in terms of OS in recurrent or metastatic nasopharyngeal carcinoma (Figure 5, Supplementary Figure 1). Tislelizumab plus GP was superior to camrelizumab plus GP.
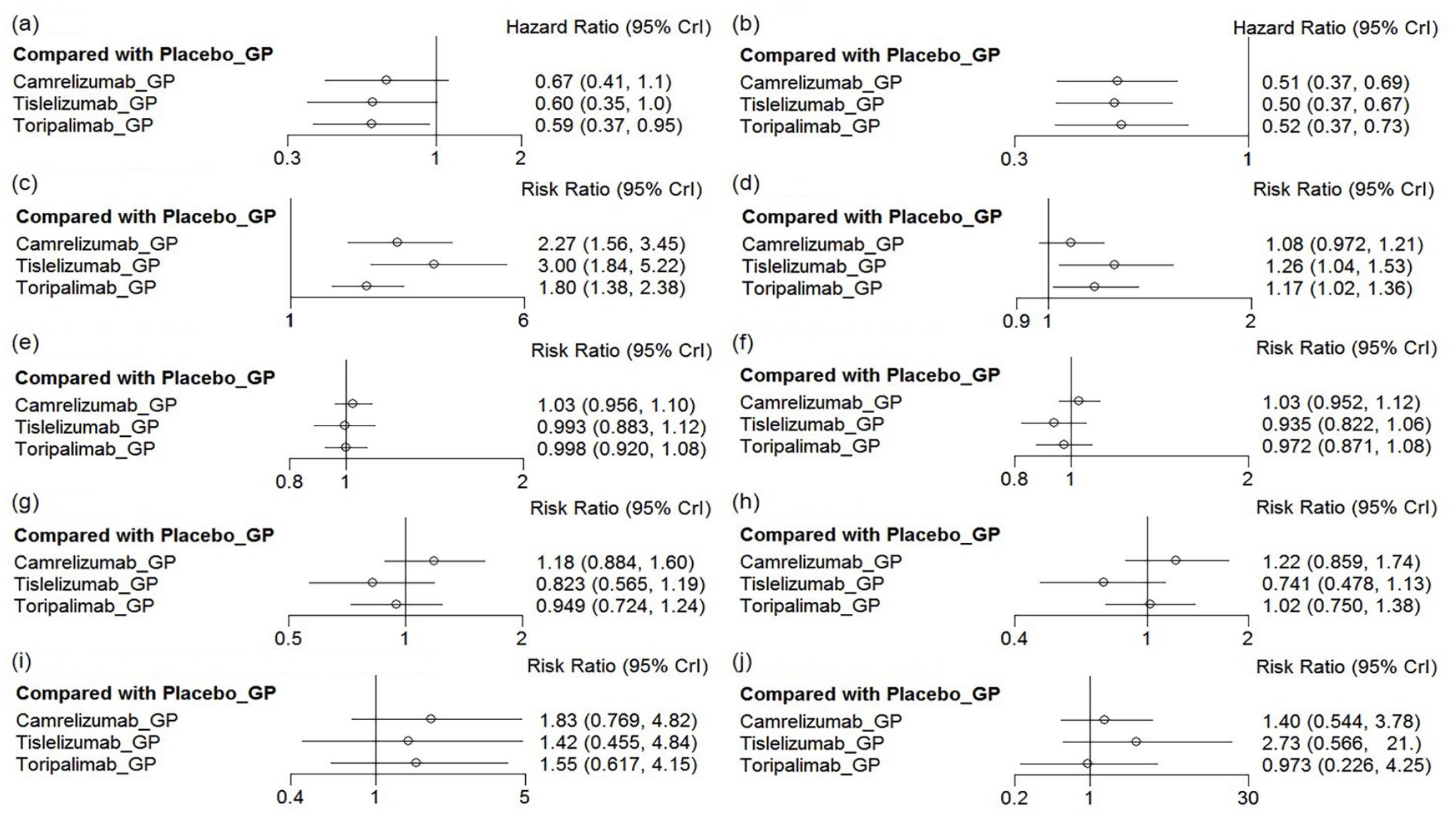
Forest plot for pooled direct comparison. “Placebo-GP” was the reference group, the hazards ratio/risk ratio of “intervention group” to “Placebo-GP” were provided. (a) OS; (b) PFS; (c) 1-year PFS rate; (d) ORR; (e) AEs-grade ≥ 3; (f) TRAEs-grade ≥ 3; (g) SAEs; (h) TRSAEs; (i) AEs led to discontinuation of treatment; and (j) AEs led to death.
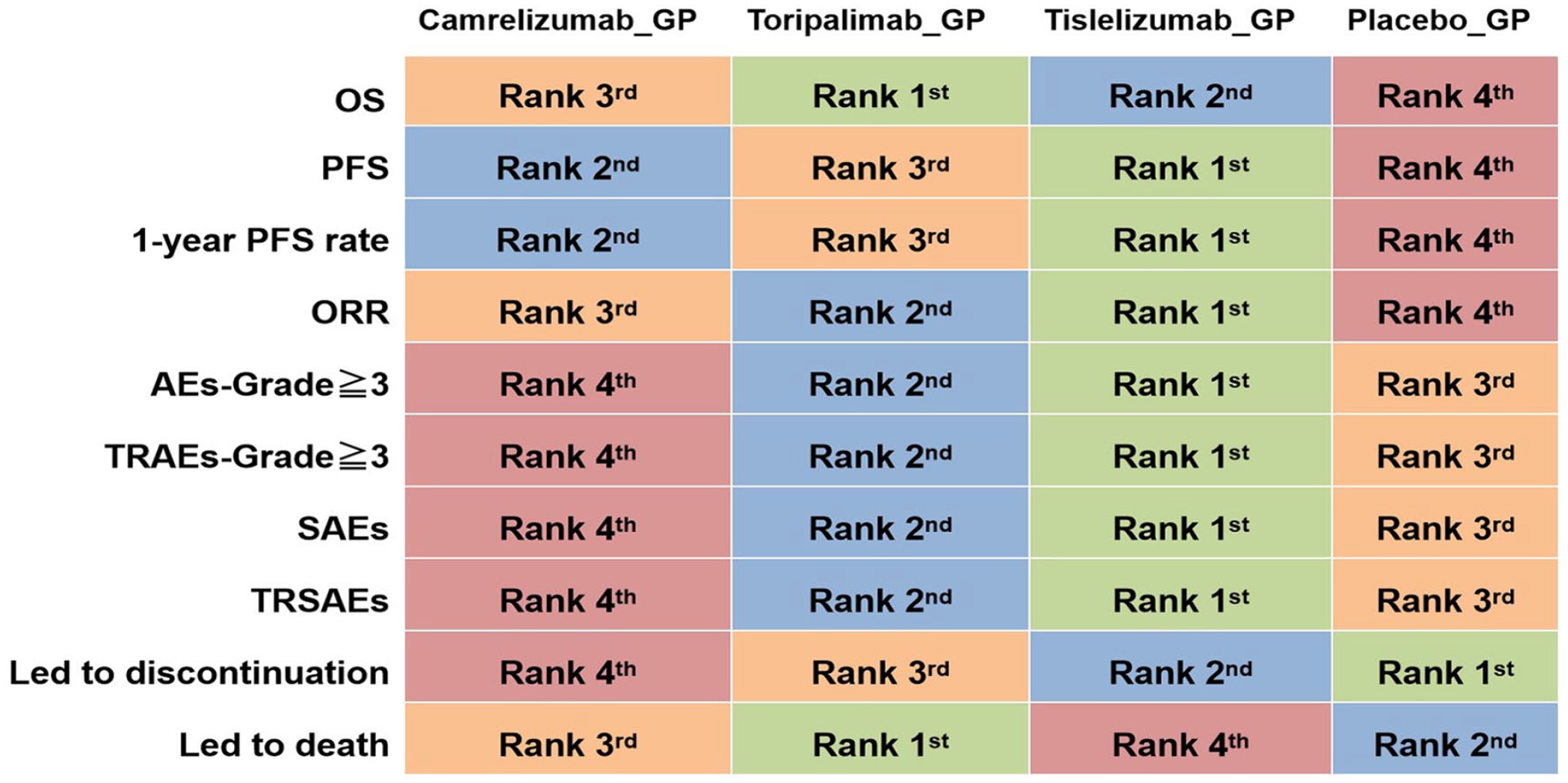
Ranking probability for efficacy and safety of different regimens.
Camrelizumab plus GP (HR = 0.51, 95%: 0.37-0.69), tislelizumab plus GP (HR = 0.50, 95% CI: 0.37-0.67), and toripalimab plus GP (HR = 0.52, 95%: 0.37-0.73) were significantly associated with better PFS (Figure 4). The results in PFS among the 3 regimens were similar. Tislelizumab plus GP seemed to be the best treatment regimen in terms of PFS in recurrent or metastatic nasopharyngeal carcinoma based on the Bayesian analysis and treatment ranking analysis according to SUCRA (Figure 5, Supplementary Figure 1).
A network meta-analysis of 3 different regimens (camrelizumab plus GP, tislelizumab plus GP, and toripalimab plus GP) was performed with regard to the 1-year PFS rate in patients with recurrent or metastatic nasopharyngeal carcinoma. Compared with placebo plus GP, all the 3 regimens were significantly related to a lower probability of 1-year disease progression (Figure 4). Tislelizumab plus GP appeared as the best treatment regimen in terms of 1-year PFS rate in recurrent or metastatic nasopharyngeal carcinoma (Figure 5, Supplementary Figure 1).
Patients receiving treatment with tislelizumab plus GP achieved the highest ORR improvement compared with those with placebo plus GP (RR = 1.26, 95% CI: 1.04-1.53), which was followed by toripalimab plus GP (RR = 1.17, 95% CI: 1.02-1.36), and camrelizumab plus GP (RR = 1.08, 95% CI: 0.97-1.21) (Figure 4,5 and Supplementary Figure 1).
Network Meta-Analysis of Safety
Pooled results for direct comparison of safety analysis are shown in Figures 4 and 6. Apart from immune-related AEs, there were no significant differences between PD-1 inhibitors plus GP and placebo plus GP in terms of AEs. We performed the network meta-analysis of AEs-grade ≥3, treatment-related AEs (TRAEs)-grade ≥3, serious AEs (SAEs), treatment-related SAEs (TRSAEs), AEs leading to discontinuation of treatment and AEs leading to death, as these outcomes were reported in all 3 trials. Compared with placebo plus GP, camrelizumab plus GP, tislelizumab plus GP, and toripalimab plus GP were not associated with a higher likelihood of AEs-grade ≥3, TRAEs-grade ≥3, SAEs, TRSAEs, and AEs leading to discontinuation of treatment and AEs leading to death (Figure 4). However, based on Bayesian analysis and treatment ranking analysis according to SUCRA, it was highly likely that tislelizumab plus GP seemed to be safer than toripalimab plus GP and camrelizumab plus GP in terms of AEs-grade ≥3, TRAEs-grade ≥3, SAEs, TRSAEs, and AEs leading to discontinuation of treatment (Figure 5, Supplementary Figure 1). Although toripalimab plus GP and camrelizumab plus GP seemed to be safer than tislelizumab plus GP in terms of AEs leading to death, tislelizumab plus GP was safer than camrelizumab plus GP in terms of TRAEs leading to death. Since TRAEs leading to death was not reported in JUPITER-02 trial, we did not perform analysis to compare that among the 3 trials.
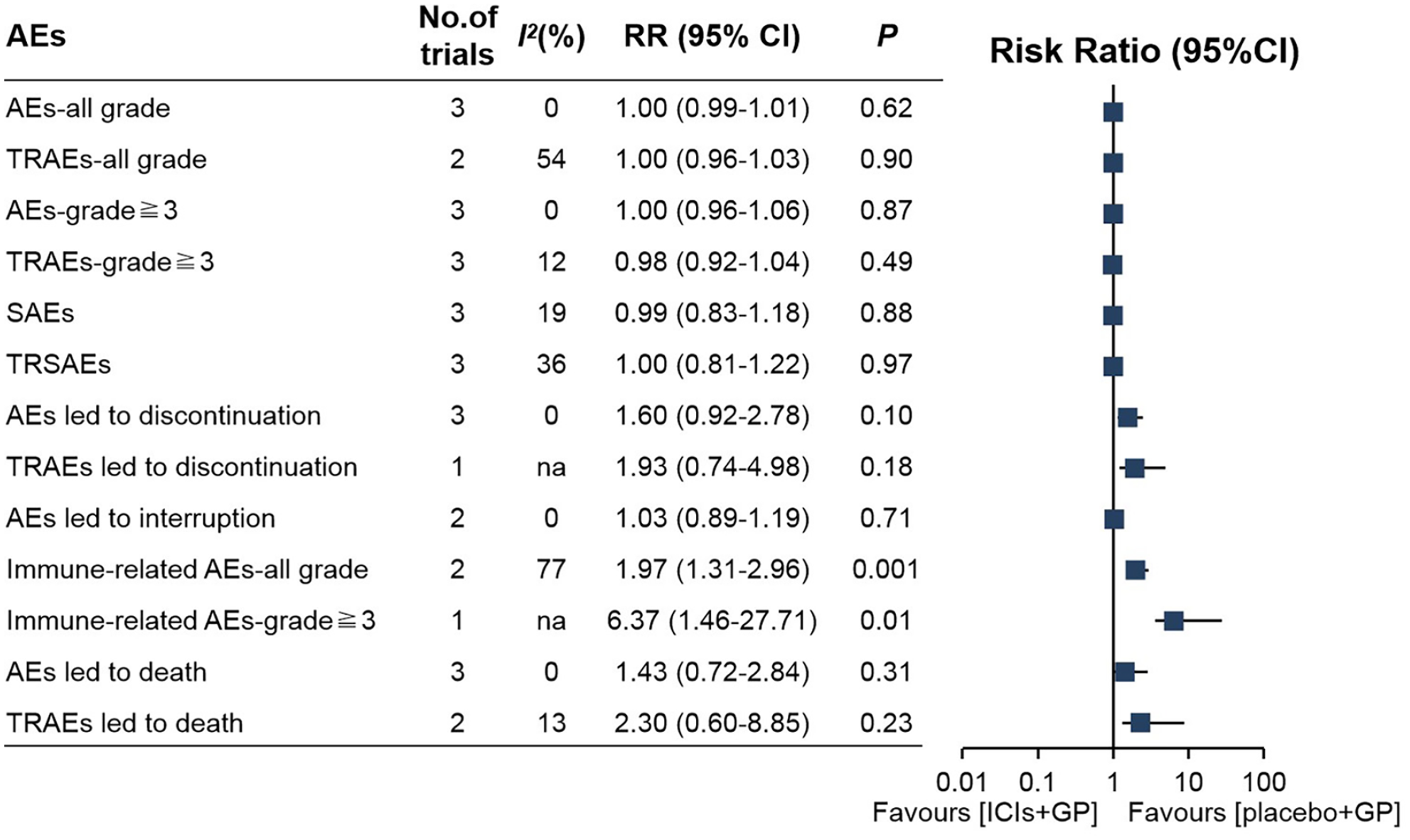
Forest plot of risk ratios for adverse events.
Discussion
Recently, ICIs, especially PD-1 inhibitors, have been investigated in various malignancies, including advanced non-small-cell lung cancer (NSCLC), advanced endometrial cancer, advanced esophageal squamous cell carcinoma, head and neck squamous cell carcinoma, advanced colorectal cancer, and so on.14-21 Whether used alone or in combination with other therapies, PD-1 inhibitors could improve the survival outcomes of cancer patients with an acceptable safety profile. What is more, several meta-analyses also confirmed the safety and efficacy of PD-1 inhibitors in certain types of malignancies.22-24 Although the fact that there have been meta-analyses investigating the safety and efficacy of PD-1 inhibitors in patients with nasopharyngeal carcinoma, the main studies included in these meta-analyses were non-RCTs.25,26 In addition, to date, no comparative studies have been conducted to assess the relative efficacy and safety of different PD-1 inhibitors in treating recurrent or metastatic nasopharyngeal carcinoma. Thus, we performed the network meta-analysis. To our best knowledge, this is the first network meta-analysis to compare the efficacy and safety of ICIs combined with chemotherapy as first-line treatment for recurrent or metastatic nasopharyngeal carcinoma. Our results indicated that patients receiving treatment with toripalimab plus GP got the best OS benefit comparing with those with placebo plus GP. In addition, OS was not reached in camrelizumab group from the CAPTAIN-1st trial. Tislelizumab plus GP generated the best PFS, 1-year PFS rate, ORR and safety among 3 different PD-1 inhibitors plus GP regimens. Our study may help us to determine the best choice of PD-1 inhibitor-based regimens in patients with recurrent or metastatic nasopharyngeal carcinoma.
Metastasis is the leading cause of death in patients with solid tumors in advanced stages. In some studies, the liver was considered the site of metastasis with the worst prognosis. The association between liver metastasis and treatment outcomes with PD-1 inhibitor was assessed in a previous study. 27 The study reported the efficacy of PD-1 inhibitor monotherapy was low in liver metastatic patients with NSCLC or melanoma. 27 Liver metastasis was also a poor prognostic factor for nasopharyngeal carcinoma. However, patients with nasopharyngeal carcinoma could benefit from PD-1 inhibitor combined with chemotherapy in terms of PFS regardless of the presence or absence of liver metastases in CAPTAIN-1st trial, which was consistent with a previous meta-analysis. 28 Despite the observed benefit, it was found that patients with liver metastases had a worse PFS compared with those without liver metastases.
EBV is the first identified tumor virus in humans.29,30 Nasopharyngeal carcinoma is predominantly associated with EBV infection. More than 90% of patients with diagnosed undifferentiated nasopharyngeal carcinoma are found to be infected with EBV. EBV DNA has been identified as a vigorous prognostic biomarker for nasopharyngeal carcinoma. Nasopharyngeal carcinoma induced by EBV often displays high expression of PD-L1 and considerable lymphocyte infiltration; hence, the application of PD-1 inhibitor might be potentially beneficial. The PFS benefit of PD-1 inhibitor plus chemotherapy was observed irrespective of EBV DNA levels in all 3 trials. In the JUPITER-02 trial, no significant difference was observed between patients with EBV baseline copy number < 2000 and those with a copy number ≥2000. However, compared with EBV DNA-positive patients at baseline, the median PFS was longer in EBV DNA-negative ones both in the PD-1 inhibitor plus chemotherapy and placebo plus chemotherapy groups according to the results of CAPTAIN-1st and RATIONALE-309 trials.
Previous studies have suggested that PD-L1 expression on tumor-infiltrating lymphocytes or tumor cells was associated with favorable responses to PD-1/PD-L1 inhibitors in various solid tumors, but its predictive performance in patients with nasopharyngeal carcinoma is not inconclusive.31-34 PFS was improved with PD-L1 inhibitor in combination with chemotherapy regardless of PD-L1 expression status in JUPITER-02 and RATIONALE-309 trials. The number of patients with negative PD-L1 expression is relatively small. Therefore, the research data should be construed with caution. Besides that possible reason, we speculate that the predictive value of PD-L1 could be interfered by EBV DNA levels. Since EBV could promote the high expression of PD-L1 via LMP1-mediated oncogenic pathways, positive EBV is an unfavorable prognostic biomarker for nasopharyngeal carcinoma. 35 The high expression of PD-L1 might be associated with high EBV DNA level. 36 Therefore, the prognostic value of PD-L1 might be disturbed by the level of EBV.
In terms of AEs, an elevated incidence of immune-related AEs was observed when PD-1 inhibitor was added to GP. In camrelizumab plus GP arm, the most common immune-related AEs were reactive capillary endothelial proliferation (58%), hypothyroidism (43%) and rash (25%). In patients who received toripalimab plus GP, the most common immune-related AEs included hypothyroidism (17.8%) and rash (8.9%). The most frequent immune-related AEs were hypothyroidism (13.7%) and rash (3.8%) in patients who received tislelizumab plus GP regimen. Hypothyroidism and rash were the common immune-related AEs in all 3 trials with the highest incidence of them in camrelizumab plus GP arm. These findings suggest that close monitoring and active management of immune-related AEs induced by PD-1 inhibitors in combination with GP should be carried out in clinical practice.
The main inclusion criteria of the 3 trials was consistent. All the 3 trials were conducted in patients aged 18 to 75 years with recurrent or metastatic nasopharyngeal carcinoma in Asia. The Eastern Cooperative Oncology Group (ECOG) performance status of all patients was less than or equal to 1 in the 3 trials. The majority of patients in all the 3 trials were recurrent nasopharyngeal carcinoma. There were also some differences among the 3 trials. The ECOG performance status of most patients in CAPTAIN-1 and RATIONALE-309 trials was equal to 1, while that of most patients in JUPITER-02 was equal to 0. In CAPTAIN-1 and JUPITER-02 trials, patients with non-keratinizing subtype of nasopharyngeal carcinoma were more than 98%, while those were 86% in RATIONALE-309 trial.
There are some limitations in this study. First, only 3 RCTs were included in the present study. The small sample size is a disadvantage of this study. Secondly, indirect comparisons via network meta-analysis might have lower validation power compared with head-to-head ones. Thirdly, baseline PD-L1 status was not reported in all 3 trials. Although all 3 trials reported baseline EBV status, however, they had inconsistent grouping of EBV status, which prevented subgroup analyses based on these factors. Furthermore, all the 3 trials were performed in Asia where the predominant histology is non-keratinizing nasopharyngeal carcinoma. Whether or not PD-1 inhibitors plus chemotherapy has comparable efficacy in regions where keratinizing carcinoma predominates remains to be clarified.
Conclusion and Relevance
In conclusion, PD-1 inhibitors plus GP as first-line treatment has better survival outcomes than placebo plus GP with comparable toxicity in recurrent or metastatic nasopharyngeal carcinoma. Toripalimab plus GP shows the best OS benefit over placebo plus GP, while tislelizumab plus GP generates the best PFS, 1-year PFS rate, and ORR. Tislelizumab plus GP appears to be a safer regimen. Longer follow-up and further research is needed to confirm our results.
Supplemental Material
sj-docx-1-aop-10.1177_10600280231188171 – Supplemental material for Efficacy and Safety of Immune Checkpoint Inhibitors Combined With Chemotherapy as First-line Treatment for Recurrent or Metastatic Nasopharyngeal Carcinoma: A Network Meta-analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-aop-10.1177_10600280231188171 for Efficacy and Safety of Immune Checkpoint Inhibitors Combined With Chemotherapy as First-line Treatment for Recurrent or Metastatic Nasopharyngeal Carcinoma: A Network Meta-analysis of Randomized Controlled Trials by Hong Sun, Fengjiao Bu, Ling Li, Xiuwen Zhang, Xiu Xin, Jingchao Yan and Taomin Huang in Annals of Pharmacotherapy
Footnotes
Acknowledgements
The authors would like to express their deep gratitude to all authors who performed all eligible trials that have been included in their analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The authors confirm that all data of this study are available in the article and its Supplementary Materials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.