
Abstract
Background:
The effect of drug-drug interaction (DDI) between tacrolimus and voriconazole on the pharmacokinetics of tacrolimus in different CYP3A5 genotypes has not been reported in previous studies.
Objective:
The objective of this study was to investigate whether CYP3A5 genotype could influence tacrolimus-voriconazole DDI in Chinese kidney transplant patients.
Methods:
All kidney transplant patients were divided into combination and non-combination groups based on whether tacrolimus was combined with or without voriconazole. Each group was subdivided into CYP3A5 expresser (CYP3A5*1/*1 or CYP3A5*1/*3) and CYP3A5 nonexpresser (CYP3A5*3/*3). A retrospective analysis compared tacrolimus dose (D)-corrected trough concentrations (C0) (C0/D) between combination and non-combination groups, respectively. Tacrolimus C0/D was also compared between CYP3A5 expresser and nonexpresser in both groups.
Results:
The C0/D values of tacrolimus were significantly different between CYP3A5 expresser and nonexpresser in combination group (378.20 [219.38, 633.48] ng/mL/[mg/kg/d] vs 720.00 [595.35, 1681.50] ng/mL/[mg/kg/d], P = 0.0010). Either in CYP3A5 expresser or nonexpresser, we found a statistically significant difference in tacrolimus C0/D between combination and non-combination group (P < 0.0001). The increase in CYP3A5 nonexpresser was 1.38 times higher than that in CYP3A5 expresser (320.93% vs 232.19%).
Conclusion and Relevance:
The median C0/D values were 90.38% higher in kidney transplant recipients with CYP3A5*3/*3 genotype than in those with CYP3A5*1/*1 or CYP3A5*1/*3 genotype when treated with both tacrolimus and voriconazole. A CYP3A5 genotype-dependent DDI was found between tacrolimus and voriconazole. Therefore, personalized therapy accounting for CYP3A5 genotype detection and therapeutic drug monitoring is necessary for kidney transplant patients when treating with tacrolimus and voriconazole.
Introduction
Kidney transplantation has become the standard treatment for patients with end-stage kidney failure due to its ability to significantly improve the life quality of patients. 1 Calcineurin inhibitors (CNI), such as cyclosporine and tacrolimus, are commonly administered to the recipients after organ transplantation as immunosuppressive agents. The biotransformation of tacrolimus is primarily mediated by the enzyme cytochrome P450 (CYP450) 3A, specifically, demethylated and hydroxylated by CYP3A in the liver and intestine, and then mainly cleared by bile. 2 Therefore, the concomitant administration of CYP3A4/3A5 inhibitors/inducers produces a drug-drug interaction (DDI) with tacrolimus by affecting blood concentrations and hence modifying its effectiveness.3,4 Genetic polymorphisms of CYP3A5 are known to affect the catalytic activity of these enzymes. 2 Some studies have investigated the role of CYP3A5 polymorphisms on the exposure as well as the clinical impact of tacrolimus. Patients with the CYP3A5*1/*1 genotype are extensive metabolizers (EMs) with normal functional expression of CYP3A5 enzyme, patients with the CYP3A5*1/*3 genotype are intermediate metabolizers (IMs) with partial enzyme function, and patients with the CYP3A5*3/*3 genotype are poor metabolizers (PMs) due to the lack of functional CYP3A5 protein.2,5,6 This interaction between the drug and genetic variation is referred to as drug-gene interaction (DGI).
Invasive fungal disease (IFD) is one of the important causes of high morbidity and mortality after kidney transplantation, among which invasive Aspergillus (IA) infection is a common type with an occurrence of 0.7% to 4%. 7 In a multinational case-control study, the overall mortality among early cases of IA was 61%. 7 In these cases, the kidney transplant recipients need to be co-administered with antifungal agents. Voriconazole, a second-generation triazole antifungal agent, is widely used in the treatment of IFD because of its activity against both Candida and Aspergillus species, especially for the prevention and treatment of fungal infection after solid organ transplantation (SOT).8,9 However, voriconazole is a substrate and strong inhibitor of CYP enzymes, including 3A4, 2C9, and 2C19, which has the potential to inhibit the metabolism of tacrolimus, leading to an increase in the blood drug concentration levels and the risk of adverse reactions. 10 As a result, a 50% to 60% reduction in the dose of tacrolimus may be necessary with the concurrent use of voriconazole. 10 In other words, voriconazole produces a strong DDI with tacrolimus.
The more complicated clinical situation is that tacrolimus treatment may be affected by both genetics (DGI) and drugs (DDI) that modulate the metabolic pathways simultaneously, which potentially affect the blood concentration unpredictably. The overlapping of DGI and DDI is referred to as drug-drug-gene interaction (DDGI). 11 It is speculated that voriconazole should have different inhibitory effects on enzymes with different metabolic functions, leading to the highly individual pharmacokinetic characteristics of tacrolimus. However, there are few studies in kidney transplant patients to verify this idea. The main objectives of this study were to evaluate the impact of voriconazole on C0/D of tacrolimus in kidney transplant recipients with different CYP3A5 genotypes and to provide evidence for the formulation of clinical individual protocol for tacrolimus. The results may further support the improvement of the individualized protocol of tacrolimus in kidney transplantation patients.
Patients and Methods
Study Population and Study Design
This single-center retrospective cohort study was conducted in The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital. Inpatients receiving kidney transplants in the Department of Urology from January 2018 to December 2022 were included. The study protocol was approved by the local Ethics Committee and informed consent was waived. The study complied with the ethical standards of the Declaration of Helsinki. The study was registered at Chinese Clinical Trial Registry under the number ChiCTR2000029257.
The inclusion criteria were as follows: (1) at least 18 years old, (2) first kidney transplant, (3) taking tacrolimus-based triple immunosuppressive regimen (tacrolimus + mycophenolate sodium + glucocorticoids). Exclusion criteria were (1) patients with multiple organ transplants, (2) patients receiving drugs that affect the blood concentrations of tacrolimus or voriconazole (eg, rifampin, phenytoin sodium, carbamazepine, fluconazole, ketoconazole, or Wuzhi capsules [Wuzhi capsules, a patented Chinese medicine extracted from Schisandra sphenanthera, are commonly used as hepatoprotective drugs. Lignin is the major active component,12,13 binds more tightly to the CYP3A5 enzyme than tacrolimus, thus Wuzhi capsules can inhibit the metabolism of tacrolimus and increase its blood concentration]), 14 (3) patients with severe hepatic dysfunction (serum alanine aminotransferase [ALT] levels >3 times of the upper normal limit or total bilirubin > 2 mg/dL, or known hepatic cirrhosis) or severe gastrointestinal disease (eg, severe gastric ulcer, gastric perforation, ulcerative colitis, gastric bypass, banding, or gastric sleeve), (4) patients who were pregnant or breastfeeding, and (5) patients with significant rejection of transplanted organs or death from other causes within 1 to 2 months after operation.
The enrolled kidney transplant patients were divided into combination group or non-combination group based on whether voriconazole was used in combination with tacrolimus or not.
Sample Size Calculation
The sample size was calculated using Power Analysis and Sample Size (PASS, version 15.0) for cohort study with 2-sample t-tests. By reviewing the literature,15-19 sex assigned at birth, age, body mass index (BMI), CYP3A5*3, days post-transplant, hematocrit, hemoglobin, red blood cell count, and dose were strongly correlated with the C0/D values of tacrolimus, so these variables were used as covariates for propensity score matching. According to the results of the preliminary test, the adjusted trough concentration (C0/D) of tacrolimus in the combination and non-combination groups (704.96 ± 555.08 ng/mL/[mg/kg/d] and 167.99 ± 127.92 ng/mL/[mg/kg/d], respectively), with 90% power and 5% significance level, patients in the combination and non-combination groups were matched 1:3, with a minimum of 14 and 42 subjects required for each group, respectively. In order to compensate for the loss of data, the sample size was increased to 27 subjects for the combination group and 81 for the non-combination group.
Data Collection and Patients Treatment
The data were collected from the HIS (Hospital Information System). Demographic and biochemical characteristics of patients in both groups were collected. Estimated glomerular filtration rate (eGFR) was calculating by the CKD-EPI formula based on the serum creatinine at the start of voriconazole treatment. Hepatic dysfunction was defined as the serum ALT higher than 3 times the upper normal limit, total bilirubin higher than 2 mg/dL, or known hepatic cirrhosis at the time of being enrolled, including sex assigned at birth, age, height, weight, days post-transplant, alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyl transpeptidase (GGT), alkaline phosphatase (ALP), total bilirubin (TBIL), serum creatinine (Cr), estimated glomerular filtration rate (eGFR), hemoglobin (HGB), red blood cell count (RBC), hematocrit (HCT), proton pump inhibitor (PPI), CYP3A5 genotypes, trough concentration (C0) and dose (D) of tacrolimus before and after combined voriconazole, and drug use in combination at each trough measurement. The patients’ blood were collected in the morning before taking tacrolimus to ensure that the measured values were trough concentrations. Measurement of tacrolimus trough values was performed in our hospital laboratory using a uniform fluorescence immunoassay. The trough concentrations measured at least 3 days after the administration or dose adjustment of tacrolimus were chosen because tacrolimus concentrations generally reach to a steady state 2 to 3 days after the dosage. In the clinical practice, tacrolimus doses were adjusted according to The Kidney Disease: Improving Global Outcomes Clinical Practice Guideline (KDIGO) for the patients initiating voriconazole treatment. 20 Besides, the trough concentrations of tacrolimus were measured every 2 to 3 days before and after voriconazole is combined, and the dose of tacrolimus was adjusted accordingly. All patients’ tacrolimus trough concentrations were selected within 3 to 10 days after the combination therapy or dose adjustment.
Patients were treated with a post-transplant immunosuppression protocol according to KDIGO. 20 More specifically, intravenous methylprednisolone sodium succinate was administered the day after transplantation with an initial dose of 500 mg/d, which was evenly tapered to 40 mg/d during the first week. During the second week, methylprednisolone tablets were given sequentially at 40 mg/d, which was gradually reduced to 16 mg/d as the maintenance dose. Immunosuppression was maintained with oral mycophenolate sodium 720 mg, twice daily. The dosing protocol and target concentration range of tacrolimus was in accordance with the manufacturer’s recommendations. 21 For kidney transplant patients, the initial oral dose should be 0.15 to 0.30 mg/kg/d, divided into 2 doses (morning and evening). Target tacrolimus trough levels in the first month following kidney transplantation were 6 to 15 ng/mL, 8 to 15 ng/mL in the first 2 to 3 months, 7 to 12 ng/mL in the 4 to 6 months after transplantation, and 5 to 10 ng/mL after the first 6 months. 22 For the patients in combination group, voriconazole was administered intravenously at a starting dose of 400 mg twice daily and was changed to 200 mg twice daily from the next day as the maintenance dose. The trough blood concentrations of voriconazole in all patients were within the treatment range (1.0-5.5 mg/L). The patient’s medication is strictly monitored by the nursing team to ensure good adherence. All patients had the Drug Interaction Probability Scale (DIPS) score of ≥5 and drug interactions were possible. 23
Statistical Analysis
The method of propensity score matching was used to match the baseline data of kidney transplantation patients in the combination and non-combination groups at 1:3, to obtain a new dataset with successful matching. Normality was tested using the Shapiro-Wilk test. Continuous data with normal distributions were represented as mean ± standard deviation (SD), and comparison between or within groups was performed by independent sample 2-sided t-test. Median and interquartile range (IQR) was used to represent continuous data with abnormal distributions, and nonparametric test was used to compare between or within groups. Categorical data were expressed as frequency and percentages, and chi-square test was used for comparison between groups. P < 0.05 represents significant difference. All analyses were performed using International Business Machine Statistical Product Service Solutions software package SPSS 22.0. Figures were generated using GraphPad Prism (version 8).
Results
Patients Recruitment and Baseline Information
A total of 1138 patients who underwent kidney transplantation were screened, of which 208 were excluded due to receiving the immunosuppressive regimen without tacrolimus, and 325 were excluded for not receiving voriconazole for fungal infection. In the remaining patients, those who lacked data of dosage or C0 of tacrolimus, combined with strong P450 enzyme inhibitors other than voriconazole, suffered with severe liver dysfunction, or died within 1 month after kidney transplantation were excluded. Finally, 280 kidney transplant recipients were enrolled in this study, among whom 32 for the combination group and 248 for the non-combination group. The enrolling process is shown in Figure 1.
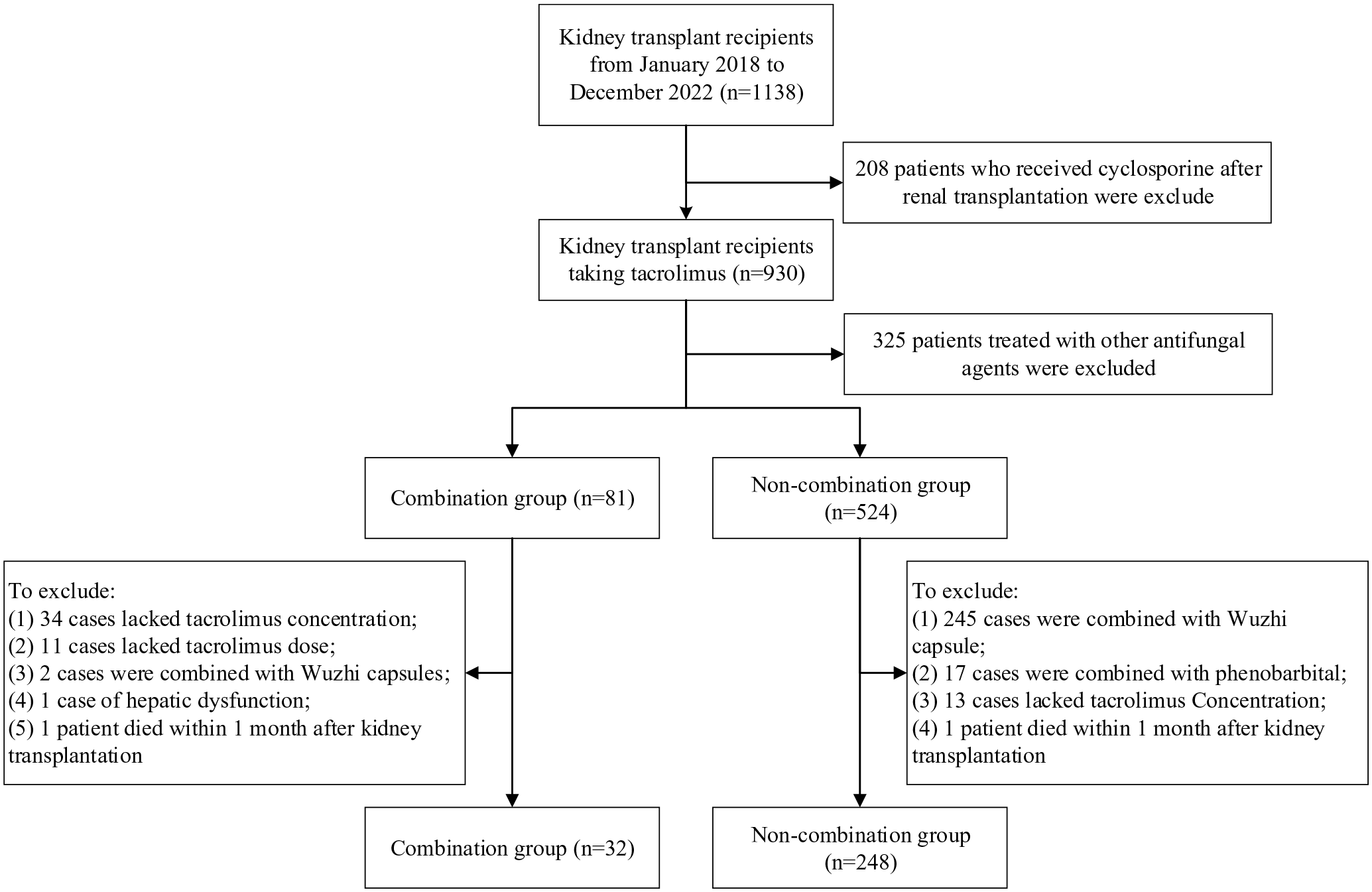
Flow chart of participants in the study.
The combination and the non-combination group were matched with propensity scores to reduce confounding by IBM SPSS. Finally, 27 and 81 cases were successfully matched in the combination and non-combination groups, respectively. In the combination group, there were 20 males and 7 females, aged 42.00 (33.00, 54.00) years old with a BMI of 22.49 ± 3.55 kg/m2. In the non-combination group, there were 61 males and 20 females, aged 39.00 (31.00, 53.00) years old with an average BMI of 22.10 ± 3.10 kg/m2. The groups were not significantly different when comparing the recipient age, sex assigned at birth, BMI, days post-transplant, and liver and kidney function at the baseline. The demographic and baseline characteristics of both groups are shown in Table 1.
Baseline Clinical Characteristics of Study Population.
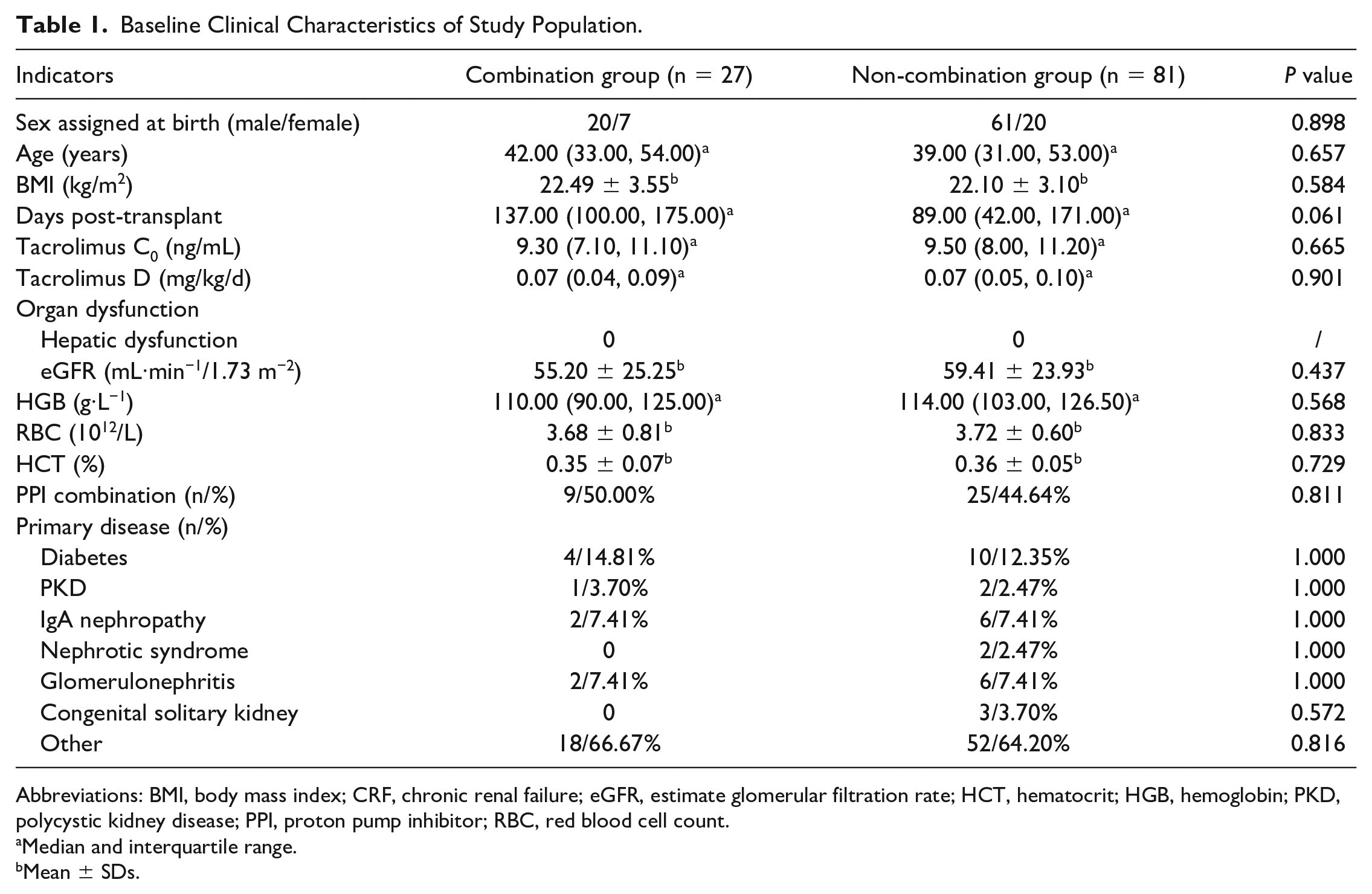
Abbreviations: BMI, body mass index; CRF, chronic renal failure; eGFR, estimate glomerular filtration rate; HCT, hematocrit; HGB, hemoglobin; PKD, polycystic kidney disease; PPI, proton pump inhibitor; RBC, red blood cell count.
Median and interquartile range.
Mean ± SDs.
CYP3A5 Genotyping
The genotype frequencies of the CYP3A5*3 polymorphisms of the recruited patients are summarized in Table 2. Among the 108 kidney transplant recipients, 9 (8.33%) recipients exhibited the CYP3A5*1/*1 genotype, 46 (42.59%) carried CYP3A5*1/*3, and 53 (49.08%) carried CYP3A5*3/*3. Therefore, the allelic frequencies of CYP3A5*1 and CYP3A5*3 were 29.63% (64/216) and 70.37% (152/216), respectively. The allele distribution of CYP3A5 was consistent with the Hardy-Weinberg equilibrium (χ2 = 0.0494, P = 0.8242).
The CYP3A5 Genotype Distribution of Kidney Transplant Patients.

Effect of Voriconazole on C0/D of Tacrolimus
Tacrolimus trough concentrations were selected within 3 to 10 days after the combination therapy or dose adjustment, and the level of tacrolimus C0/D increased by 357.74% in the combination group compared to the non-combination group (628.30 [365.40, 769.50] ng/mL/[mg/kg/d] vs 137.26 [97.78, 206.77] ng/ml/[mg/kg/d], P = 0.0000). In non-combination group, there was a statistically significant difference in tacrolimus C0/D between patients with CYP3A5*1/*1 or CYP3A5*1/*3 genotype and patients with CYP3A5*3/*3 genotype (113.85 [85.88, 180.26] ng/mL/[mg/kg/d] vs 171.05 [128.57, 246.16] ng/mL/[mg/kg/d], P = 0.0004). In combination group, the C0/D levels were 90.38% higher in patients with the CYP3A5*3/*3 genotype than in patients with CYP3A5*1/*1 or CYP3A5*1/*3 genotype (720.00 [595.35, 1681.50] ng/mL/[mg/kg/d] vs 378.20 [219.38, 633.48] ng/mL/[mg/kg/d], P = 0.0010), as shown in Figure 2. Either CYP3A5 expresser (CYP3A5*1/*1 or CYP3A5*1/*3) or CYP3A5 nonexpresser (CYP3A5*3/*3), we found a statistically significant difference in tacrolimus C0/D between the combination group and the non-combination group (378.20 [219.38, 633.48] ng/mL/[mg/kg/d] vs 113.85 [85.88, 180.26] ng/mL/[mg/kg/d], P < 0.0001; 720.00 [595.35, 1681.50] ng/mL/[mg/kg/d] vs 171.05 [128.57, 246.16], P < 0.0001), as shown in Figure 2.
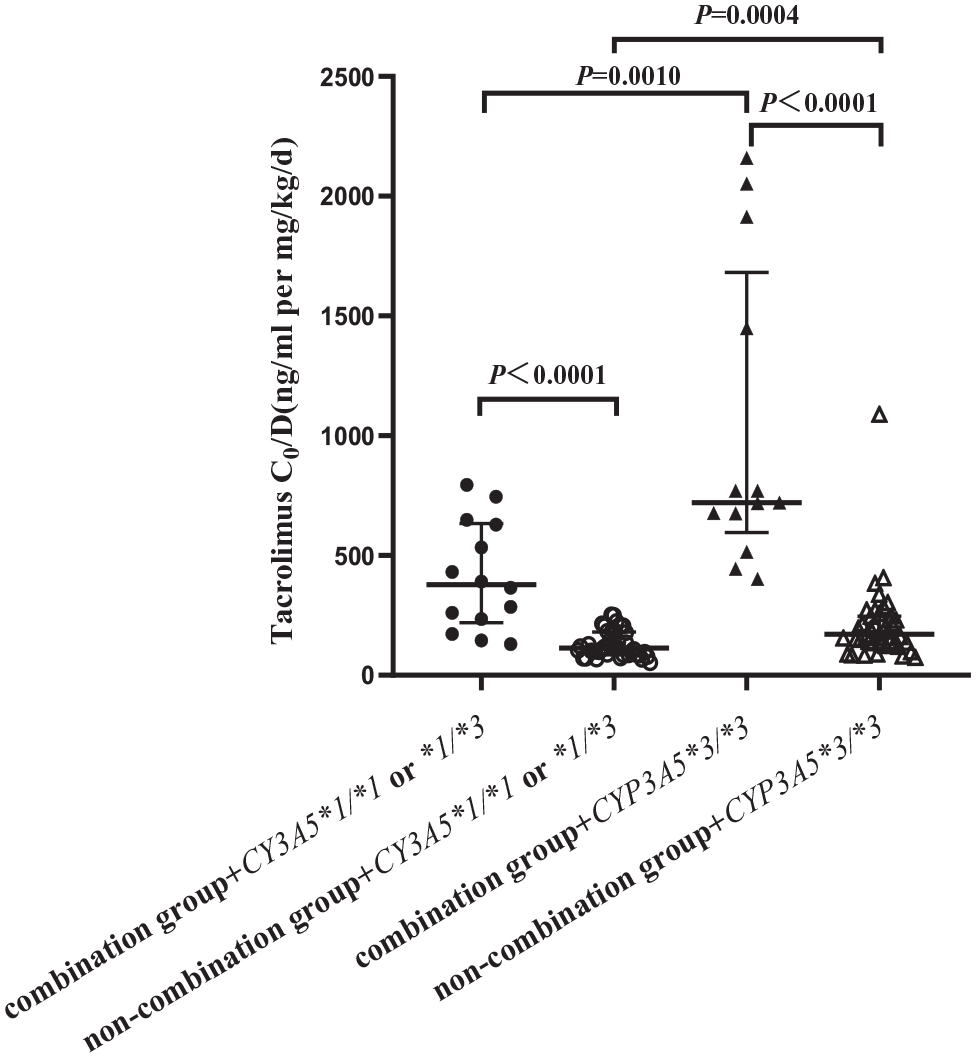
Tacrolimus dose-adjusted trough concentrations between combination and non-combination groups with different CYP3A5 genotypes. (P < 0.05 denotes a significant difference between corresponding data). Solid circle or triangle means tacrolimus combined with voriconazole, and hollow means no combination.
Changes in C0/D of Tacrolimus Before and After Voriconazole Co-administration
The C0/D values of tacrolimus in CYP3A5 expresser and CYP3A5 nonexpresser showed the same trend after receiving the same dose of voriconazole in kidney transplant recipients. The C0/D values of tacrolimus in CYP3A5 expresser were higher than those before combined treatment (134.19 ± 40.80 ng/mL/[mg/kg/d] vs 425.61 ± 227.95 ng/mL/[mg/kg/d], P = 0.0003). The values of tacrolimus before and after C0/D in CYP3A5*3/*3 genotype patients were as follows (158.40 [118.74, 215.20] ng/mL/[mg/kg/d] vs 720.00 [595.35, 1681.50] ng/mL/[mg/kg/d], P = 0.0002, Figure 3).
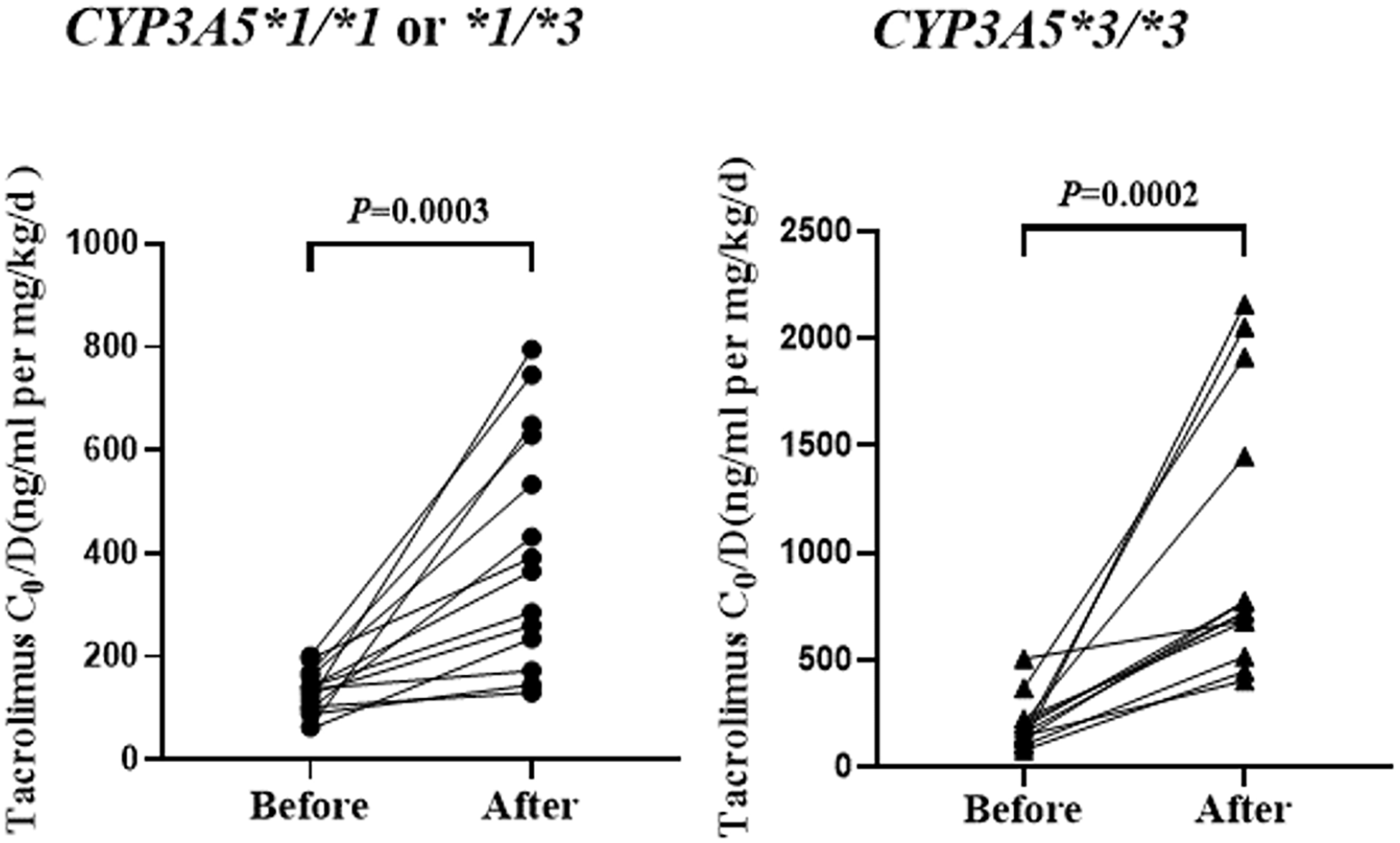
Tacrolimus dose-corrected trough concentrations between CYP3A5 expresser and CYP3A5 nonexpresser, respectively (P < 0.05 denotes a significant difference between corresponding data).
Discussion
In the present study, we found an important characteristic that voriconazole increased the blood concentrations of tacrolimus, that is, the degree of influence was associated with CYP3A5 genetic polymorphisms. When CYP3A5 expresser used tacrolimus combined with voriconazole, the increase in the C0/D of tacrolimus was significantly higher than that of CYP3A5 nonexpresser. Therefore, this DDGI involving tacrolimus and voriconazole suggests that the dual effects of both drugs and genes should be considered in clinical practice.
Studies have shown that in hematopoietic stem cell transplantation (HSCT) patients who are co-administered with azole antifungal agents, tacrolimus valley concentration in CYP3A5*3/*3 genotype patients is higher than that in CYP3A5*1/*1 or CYP3A5*1/*3 genotype patients (P = 0.034). Although the daily dose of tacrolimus was significantly lower in CYP3A5*3/*3 patients than in CYP3A5*1/*1 or CYP3A5*1/*3 genotype patients (P = 0.041). 24 Other studies have shown that when combined with voriconazole, the median tacrolimus C0/D values of CYP3A5*1/*1 or CYP3A5*1/*3 genotype patients was significantly lower than that of CYP3A5*3/*3 genotype carriers (557 ng/mL/[mg/kg] vs 723 ng/mL/[mg/kg], P < 0.010). 5 Our results were consistent with those reported previously. Furthermore, our data demonstrated for the first time that the median C0/D value was 90.38% higher in kidney transplant recipients with CYP3A5*3/*3 genotype than in those with CYP3A5*1/*1 or CYP3A5*1/*3 genotype when treated with both tacrolimus and voriconazole. Another result was that the elevation was 1.38 times greater in patients with CYP3A5*3/*3 genotype than in those with CYP3A5*1/*1 or CYP3A5*1/*3 genotype after co-administration of voriconazole. Therefore, it could be concluded that patients with CYP3A5*1/*1 or CYP3A5*1/*3 genotype had a lower exposure to tacrolimus when combined with voriconazole than CYP3A5*3/*3 genotype patients. Results from previous studies support our finding. According to a study, the antifungal agent fluconazole, which had the activity of inhibiting the tacrolimus metabolism in vivo, had significantly lower effect on tacrolimus concentrations in patients with CYP3A5*1/*1 or CYP3A5*1/*3 genotype than in patients with CYP3A5*3/*3 genotype. In patients with CYP3A5*3/*3 genotype, the metabolism of tacrolimus was more likely to be inhibited by fluconazole, leading to an increased risk of supratherapeutic use of tacrolimus or even toxicity. 25 Another study reported that when tacrolimus was combined with nicardipine, tacrolimus C0 increased more slowly in patients with CYP3A5*1/*1 or CYP3A5*1/*3 genotype than in patients with CYP3A5*3/*3 genotype. 26 Therefore, regular monitoring of tacrolimus serum concentration is necessary, especially for patients initially added (or discontinued) voriconazole, and CYP3A5 genotyping helped to predict the extent to which voriconazole increased tacrolimus concentration.
The feature of this study was to match the baseline data of the combined medication group and the non-combined medication group using a propensity score matching method to reduce the interference of confounding factors. In addition, this study is the first observational study of DDGI in kidney transplant patients. The main limitations of this observational study include the following: (1) this study was a single-center design and the results lack generalizability. (2) This study only investigated the effect of CYP3A5 gene polymorphisms. Because the mutation rate of CYP3A4 in Chinese is almost 0,27-29 the effect of CYP3A4 gene polymorphism on tacrolimus metabolism was not considered. (3) Data regarding azole trough concentrations were not included. Azole TDM did not become routine in our institutions until several years into the study period and was performed in only 30% of all (mostly voriconazole-treated) patients. (4) The study only evaluated tacrolimus immediate-release formulations, and the results may differ from those of extended-release formulations. 30 (5) Only assessed a Chinese kidney transplant population, so it is unknown if finding would be applicable to other populations who may have additional CYP3A4 or CYP3A5 variants. Previous studies showed that the C0/D of tacrolimus depended on the combination of CYP3A5 and CYP2C19 genotypes in HSCT and heart transplant recipients treated with voriconazole.5,31 Unfortunately, we could not obtain the CYP2C19 genotypes of the patients enrolled, which was one of the limitations of this study. We expect larger sample multi-center clinical trials to verify the effect of CYP3A5 and CYP2C19 genotype combination on the interaction between voriconazole and tacrolimus.
Conclusion and Relevance
Our study demonstrated for the first time that the median C0/D value was 90.38% higher in kidney transplant recipients with CYP3A5*3/*3 genotype than in those with CYP3A5*1/*1 or CYP3A5*1/*3 genotype when treated with both tacrolimus and voriconazole, and the elevation of tacrolimus C0/D values was 1.38 times greater in patients with CYP3A5*3/*3 genotype than in those with CYP3A5*1/*1 or CYP3A5*1/*3 genotype, suggesting that drug-drug interactions were lower in CYP3A5 expresser than in CYP3A5 nonexpresser. Therefore, genetic pre-evaluation of kidney transplant patients is considered during clinical administration, so that clinicians can develop targeted therapy to improve therapeutic efficacy while minimizing overexposure and toxicity.
Supplemental Material
sj-xlsx-1-aop-10.1177_10600280231197399 – Supplemental material for CYP3A5 Genotype-Dependent Drug-Drug Interaction Between Tacrolimus and Voriconazole in Chinese Kidney Transplant Patients
Supplemental material, sj-xlsx-1-aop-10.1177_10600280231197399 for CYP3A5 Genotype-Dependent Drug-Drug Interaction Between Tacrolimus and Voriconazole in Chinese Kidney Transplant Patients by Yundi Zhang, Yue Du, Shuyu Ren, Yue Li, Xiaoming Zhang, Xiaohong Cao, Fengxi Liu, Huiying Zong and Yan Li in Annals of Pharmacotherapy
Supplemental Material
sj-xlsx-2-aop-10.1177_10600280231197399 – Supplemental material for CYP3A5 Genotype-Dependent Drug-Drug Interaction Between Tacrolimus and Voriconazole in Chinese Kidney Transplant Patients
Supplemental material, sj-xlsx-2-aop-10.1177_10600280231197399 for CYP3A5 Genotype-Dependent Drug-Drug Interaction Between Tacrolimus and Voriconazole in Chinese Kidney Transplant Patients by Yundi Zhang, Yue Du, Shuyu Ren, Yue Li, Xiaoming Zhang, Xiaohong Cao, Fengxi Liu, Huiying Zong and Yan Li in Annals of Pharmacotherapy
Footnotes
Acknowledgements
We would like to thank the staff at the Center for Big Data Research in Health and Medicine, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, for their valuable contribution.
Author’s Note
Yue Du is now affiliated to Department of Pharmacy, Zibo Central Hospital, Zibo, China.
Author Contributions
YL, YZ, and YD contributed to conception and design of the work. YZ, YD, and RSY collected the datasets and carried out the experiments. ZXM, CXH, and LFX collated the data and performed the analysis. YZ, ZHY, and YL interpreted the results, performed the analysis, and wrote the manuscript. Yundi Zhang and Yue Du are co-first authors and contributed equally to this work. All authors read and agreed the final manuscript.
Data Availability Statement
The authors declare that the data supporting the findings of this study are available within the paper and the accompanying supplementary information files.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Drug Risk Management Project: Diabetes Drug Risk Management Research (DRM2021001).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.