
Abstract
Objective:
To evaluate the safety and efficacy of the novel KRAS-targeting agents, sotorasib and adagrasib, in treating KRAS G12C-mutated non–small cell lung cancer (NSCLC).
Data Sources:
A comprehensive English-based literature search of PubMed and Clinicaltrials.gov between January 2000 and July 2023 was conducted using the terms sotorasib, Lumakras, AMG 510, adagrasib, Krazati, and MRTX849.
Study Selection and Data Extraction:
Relevant prescribing information, clinical trials, and treatment guidelines were evaluated.
Data Synthesis:
Sotorasib and adagrasib received accelerated US Food and Drug Administration (FDA) approval following pivotal phase I/II clinical trials. Sotorasib, a first-in-class KRAS inhibitor, demonstrated an overall response rate (ORR) of 41% and a progression-free survival (PFS) of 6.3 months. In a phase III confirmatory trial, sotorasib showed significantly longer PFS compared with docetaxel (5.6 vs. 4.5 months; P = 0.0017). Adagrasib produced an ORR of 42.9% and a PFS of 6.5 months. Both drugs present unique safety profiles, with common toxicities, including diarrhea, musculoskeletal pain, fatigue, and hepatotoxicity.
Relevance to Patient Care and Clinical Practice:
With KRAS mutations being among the most common oncogenic alterations in NSCLC, sotorasib and adagrasib offer new therapeutic avenues for this previously “undruggable” target. Current treatment guidelines list sotorasib and adagrasib as second-line options in patients with confirmed KRAS G12C-mutated NSCLC. Additional studies are required to further differentiate the safety and efficacy profiles of these 2 agents and identify their optimal place in therapy.
Conclusion:
Sotorasib and adagrasib demonstrated promising outcomes in targeting the constitutively active KRAS G12C oncogenic driver, underscoring the need for further research to optimize their therapeutic application in this high-risk population.
Keywords
Introduction
Lung cancer remains a predominant global health concern, projected to result in more than 2.2 million new diagnoses in 2023 alone.1,2 Despite advances in detection and therapeutic modalities, bronchogenic carcinoma continues to be the leading cause of cancer-related deaths, claiming a 5-year overall survival (OS) rate of less than 18% worldwide. 3 Within the United States, lung cancer is expected to be diagnosed in an estimated 238 340 individuals in 2023, leading to an anticipated 127 070 fatalities. 4 Non–small cell lung cancer (NSCLC), which comprises approximately 85% of all lung cancer diagnoses, is typically categorized into 3 main types: adenocarcinoma (40%), squamous cell carcinoma (25%-30%), and large cell carcinoma (5%-10%). 3
Surgical resection, when possible, is the standard of care for medically operable early-stage NSCLC, with resectability determined by factors, such as staging, tumor location, and patient-specific considerations (eg, age, comorbidities, lung function, and treatment preferences). In addition, approximately one-third of NSCLC patients present with locally advanced disease at diagnosis, with a mere 15% to 25% surviving 5 years postdiagnosis. 5
The treatment landscape for NSCLC has witnessed significant changes over the past 2 decades, largely due to the identification and molecular characterization of druggable oncogenic mutations. The first wave of this transformation came in 2004, when the US Food and Drug Administration (FDA) approved the tyrosine kinase inhibitor erlotinib (Tarceva) for treating locally advanced or metastatic NSCLC following the failure of at least one prior chemotherapy regimen. 6 A decade later, the approval of nivolumab (Opdivo), an immune checkpoint inhibitor (ICI) first indicated for the treatment of advanced melanoma, marked another milestone in the treatment of advanced NSCLC that had progressed during or after treatment with platinum-based chemotherapy. Targeted agents and immunotherapies have become cornerstone treatment options for managing advanced NSCLC. 7 Ongoing research into oncogenic driver mutations in NSCLC continues to yield promising advances in precision medicine and personalized treatment options.
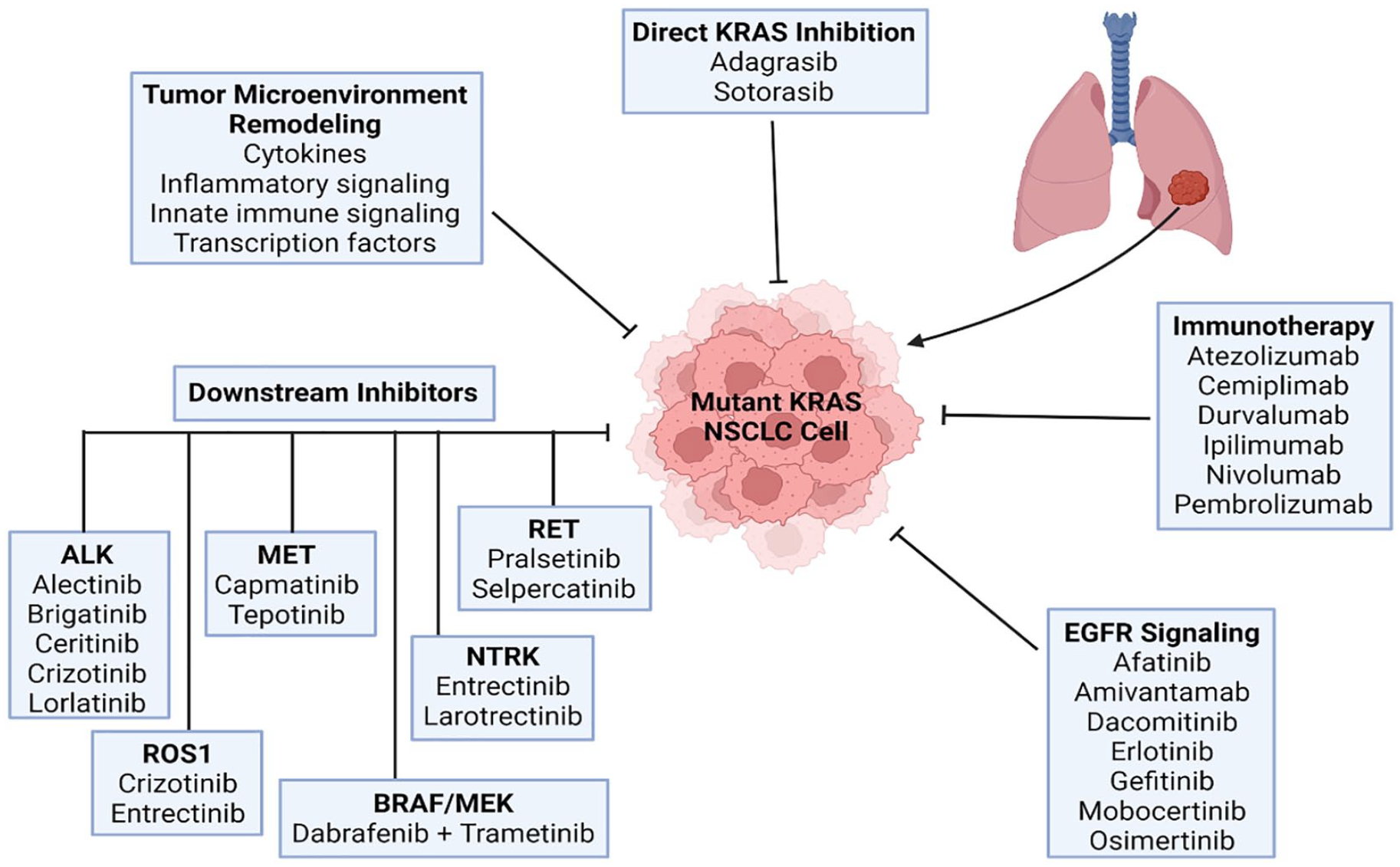
The discovery of sensitizing mutations in the epidermal growth factor receptor (EGFR) set the stage for biomarker-guided treatment strategies in NSCLC. Continued investigations into the molecular mechanisms underlying tumorigenesis have yielded significant insights, revealing numerous oncogenic alterations that now serve as effective therapeutic targets. Generally, these targeted therapies not only enhance treatment efficacy compared with conventional chemotherapy but also offer the advantage of improved tolerability. Examples of molecular alterations that are now targetable in NSCLC include ALK, BRAF, EGFR, HER2, MET, NTRK, RET, ROS1, and RAS (Figure 1). 7
The RAS family of proto-oncogenes is pivotal regulators of cell growth, differentiation, and survival through encoding a small intracellular guanosine triphosphatase (GTPase) protein. 10 This guanosine triphosphate (GTP)-bound RAS protein plays a critical role in transmitting mitogenic signals from upstream receptors. RAS mutations, which are implicated in nearly a third of all solid tumors, are the most identified oncogenic mutations in human cancer. Kirsten rat sarcoma viral oncogene homolog (KRAS), found in the short arm of chromosome 12, is the most frequently investigated human RAS isoform. 10 Furthermore, KRAS mutations are frequently found in colorectal cancer (45% of cases), pancreatic cancer (90% of cases), and NSCLC (30%-35% of cases). 11 Alterations in KRAS are also present in biliary, endometrial, intestinal, and peritoneal malignancies. 8 While TP53 mutations are the most frequently observed mutation found in NSCLC, approximately 30% of Caucasian patients with NSCLC exhibit gain-of-function KRAS alterations. Patients of Asian descent, however, demonstrate a lower likelihood of experiencing KRAS mutations, with a reported prevalence of approximately 10%.12,13 In addition to Caucasian ethnicity, other factors associated with higher rates of KRAS mutations include female sex, adenocarcinoma histology, and exposure to cigarette smoke. 14 The overall prognostic implications of KRAS mutations are controversial and require additional research.
KRAS-mutated NSCLC is a heterogeneous disease, encompassing a multiplicity of diverse subtypes and concurrent genomic alterations of other principal genes. The primary alteration in KRAS is attributable to a single point mutation at codon 12, entailing a substitution of glycine with cysteine. 14 This particular alteration, known as KRAS G12C, comprises 39% of all KRAS mutations in NSCLC. Other notable mutations include the substitution of glycine with valine (G12V) and glycine with aspartic acid (G12D), which account for 21% and 17% of KRAS mutations, respectively. 15 Researchers have identified other KRAS mutations occurring on codons 13, 59, 61, 117, and 14; however, not all KRAS-activating mutations exhibit oncogenicity. The clinical course and treatment outcomes associated with KRAS-mutated NSCLC demonstrate considerable variance. This disparity may be attributable to unique tumor biology, immune response patterns, and therapeutic vulnerabilities. 16
As RAS mutations are the most frequently mutated family of genes in cancer, researchers have sought opportunities to develop safe and effective RAS inhibitors. This pursuit over the last 4 decades was largely unsuccessful due to high affinity of RAS for GTP coupled with exceedingly high intracellular tumor concentrations of GTP. As a result, RAS proteins were considered “undruggable.” 17 However, the pivotal 2013 study by Ostrem and colleagues showed that small-molecule inhibitors could irreversibly bind to codon 12 of KRAS, which reinvigorated interest in precision therapies for KRAS-mutated cancers. 18
Sotorasib (Lumakras) gained accelerated FDA approval in May 2021 as the first targeted agent for locally advanced or metastatic, KRAS G12C-mutated NSCLC. 19 In December 2022, the FDA granted accelerated approval to a second KRAS inhibitor, adagrasib (Krazati), for the second-line treatment of locally advanced or metastatic NSCLC with KRAS G12C mutations. 20 This review aims to evaluate the safety and efficacy of these FDA-approved KRAS inhibitors for the treatment of advanced or metastatic NSCLC.
Data Sources
An English-based literature search for articles published between January 2000 and July 2023 was completed using PubMed with the following search terms: sotorasib, Lumakras, AMG 510, adagrasib, Krazati, MRTX849. An extended search was also conducted via ClinicalTrials.gov to discover ongoing or yet-to-be-published clinical trials pertinent to this review. Throughout the manuscript preparation, the researchers also evaluated relevant articles, abstracts, product package inserts, and guidelines.
Pharmacology
Mechanism of Action
Sotorasib is a small molecule that specifically and irreversibly inhibits KRAS G12C, a unique, tumor-restricted, mutant-oncogenic form of the RAS GTPase. 21 KRAS mutations occur in approximately 14% of lung adenocarcinomas. 22 Sotorasib forms an irreversible, covalent bond with the distinctive cysteine residue present in the G12C variant of KRAS. This locks the protein into an inactive guanosine diphosphate (GDP)-bound state, effectively preventing downstream signaling without affecting wild-type KRAS function. 23 Sotorasib binds to the switch II region, a feature that is present only in the inactive GDP-bound KRAS G12C. This binding irreversibly inhibits KRAS signaling, halts cell growth, and promotes apoptosis. 24 In contrast, healthy cells contain KRAS proteins that cycle between active GTP-bound states and inactive GDP-bound states. The active GTP-bound state initiates effector binding and intracellular signal transduction. 22 Therefore, the therapeutic potential of sotorasib hinges on the intricate molecular interplay of KRAS proteins. A detailed visualization of this mechanism can be found in Figure 2.
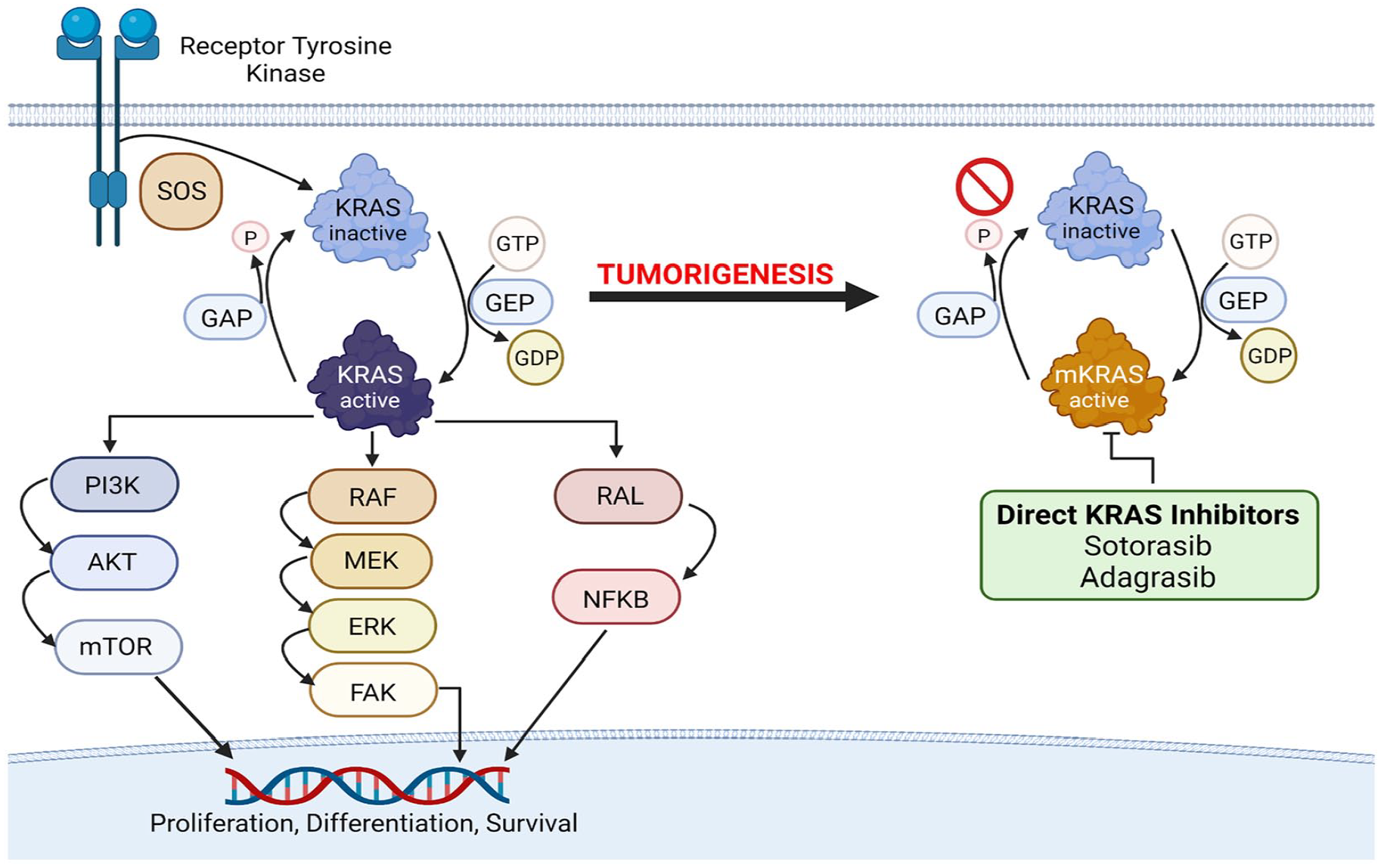
Guanine-nucleotide-exchange factors facilitate the transition between the active GTP-bound state and the inactive GDP-bound state. 14 Initially, these factors load GTP onto KRAS to activate it, and subsequently catalyze GTP hydrolysis with the aid of GTPase-activating proteins to return KRAS to its inactive state. However, the presence of mutations in KRAS, such as KRAS G12C, disrupts this cycle. As a prominent characteristic of many cancers, these mutations inhibit the interaction with GTPase-activating proteins, thereby preventing the shift to inactive GDP-bound state and consequently amplifying KRAS signaling. 25
Sotorasib does not appear to impact wild-type KRAS proteins, demonstrating selective inhibition of KRAS G12C both in vivo and in vitro with minimal detectable off-target activity. In mouse tumor xenograft models, sotorasib treatment resulted in tumor regression and prolonged survival, also showing an association with antitumor immunity specifically in KRAS G12C models. 21 Preclinical studies demonstrated that sotorasib can also inhibit nearly all detectable phosphorylation of extracellular signal–regulated kinase (ERK), a key downstream effector of KRAS. In mice, this led to durable, complete tumor regression in the presence of KRAS G12C-mutated tumors. 25
Another promising KRAS inhibitor, adagrasib, also employs a similar mechanism of action by specifically and irreversibly inhibiting KRAS G12C through covalent binding to the mutant cysteine 12 residue in the KRAS switch II pocket. This binding locks the mutant KRAS protein in its inactive GDP-bound conformation.26,27 In tumor xenograft models, adagrasib has demonstrated an ability to inhibit tumor cell growth and viability in cells harboring KRAS G12C mutations. This effect leads to tumor regression in KRAS G12C-mutated tumor models with minimal off-target activity. 28
The specificity of agents, such as sotorasib and adagrasib stems from the identification of mutations in codon 12 or 13 of RAS proteins that impair GTP hydrolysis, leaving RAS in the active GTP-bound state. Consequently, KRAS G12C inhibitors are specific to these mutations in codon 12, which minimizes their off-target activity and creates specificity only at the mutated KRAS protein.18,27,29
Pharmacokinetics and Pharmacodynamics of KRAS Inhibitors
Pharmacokinetics
Sotorasib, an orally available KRAS G12C inhibitor, has demonstrated time-dependent, non-linear pharmacokinetics throughout the dosage range of 180 to 960 mg.21,24 The primary metabolic pathways of sotorasib involve non-enzymatic conjugation and oxidative metabolism through CYP3A enzymes. 21 At steady-state, once-daily dosing exhibited consistent systemic exposure and was comparable for both film-coated tablets and film-coated tablets predispersed in water when administered under fasting conditions. Steady-state plasma concentrations were reached within 22 days, with a median time to peak plasma concentration (Tmax) of 1 hour. 25 When administered with a high-fat, high-calorie meal, sotorasib area under the curve (AUC) increased by 25% compared with administration under fasting conditions. However, no clinically significant differences in systemic exposure were observed between fasted or fed conditions. Therefore, according to manufacturer recommendations, sotorasib may be taken without regard to food. The concomitant use of acid-reducing agents was found to decrease systemic exposure of sotorasib. After repeat doses of omeprazole, the maximum plasma concentration (Cmax) of a single sotorasib dose was reduced by 65%, and the AUC was reduced by 57%. 21 Furthermore, coadministration of famotidine 10 hours before and 2 hours after a single dose of sotorasib led to a 35% decrease in sotorasib Cmax and a 38% decrease in AUC. 21
Sotorasib has a mean volume of distribution (Vd) at steady state of 211 L (coefficient of variation [CV] 135%), with in vitro plasma protein binding of 89%. When administered at a dose of 960 mg once daily, the steady-state apparent clearance of sotorasib is 26.2 L/h (CV: 76%). 21 The drug has a mean terminal elimination half-life of 5 hours. Based on radiolabeled sotorasib, 74% of the dose was recovered in the feces (53% unchanged) and 6% in urine (1% unchanged). Sotorasib demonstrated consistent pharmacokinetics across a range of population variables, including age (28-86 years), sex, race (White, Black, and Asian), body weight (36.8-157.9 kg), line of therapy, Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1, and mild to moderate renal or hepatic impairment. 21 However, moderate hepatic impairment reduced sotorasib AUC by 25%, while severe hepatic impairment resulted in a 4% increase compared with patients with normal hepatic function. The effect of severe renal impairment on sotorasib pharmacokinetics has not been studied.
Adagrasib is an oral drug administered up to twice daily. Its AUC and maximum plasma concentration increase proportionally with doses between 400 and 600 mg. Steady state is achieved within 8 days, with a 6-fold accumulation at the recommended dosage. The median Tmax of adagrasib is approximately 6 hours. There were no clinically significant differences seen in the pharmacokinetics of adagrasib when administered with a high-fat, high-calorie meal. Adagrasib has a long half-life of approximately 23 hours after a single dose. 28 Adagrasib has an apparent volume of distribution of 942 L and binds to human plasma proteins at an estimated 98% in vitro. Notably, adagrasib can penetrate the central nervous system (CNS). 30 Following multiple doses and achieving stead-state concentrations, adagrasib is metabolized by several CYP enzymes, including CYP2C8, CYP1A2, CYP2B6, CYP2C9, and CYP2D6. Adagrasib is primarily metabolized by CYP3A4 following single-dose administration; however, following several doses, adagrasib inhibits its own CYP3A4 metabolism, enabling the other CYP enzymes to contribute more significantly to its metabolism. Approximately, 75% of an adagrasib dose was excreted in feces (14% unchanged), and 4.5% in urine (2% unchanged) following a single oral dose of radiolabeled adagrasib. 28 The pharmacokinetics of adagrasib demonstrated no clinically significant differences based on factors, such as age (19-89 years), sex, race, body weight (36-139 kg), ECOG PS of 0 or 1, or tumor burden. Furthermore, no clinically significant differences were expected in the pharmacokinetics of adagrasib in patients with mild to severe renal or hepatic impairment. 28
Pharmacodynamics
The exposure-response relationships and pharmacodynamic response timelines for sotorasib and adagrasib are currently undefined.21,28 Both agents function by irreversibly and covalently binding to mutant KRAS G12C in NSCLC cells, thereby inhibiting downstream signaling effects that promote cancer cell proliferation. In preclinical studies, adagrasib demonstrated an extended pharmacodynamic effect, consistent with its irreversible inhibition of KRAS G12C, which accounts for its prolonged half-life. 27 In contrast, sotorasib studies demonstrated peak plasma and tumor exposure occurring 30 minutes after a single dose, leading to a maximal inhibition of the p-ERK downstream signaling pathway within 2 to 4 hours posttreatment, which was sustained for 48 hours. Sotorasib also demonstrated dose-dependent p-ERK inhibition 2 hours posttreatment in KRAS G12C models, with maximum inhibition at doses of 30 mg to 100 mg/kg. 27
Regarding cardiovascular effects, sotorasib, at approved doses, did not significantly increase the QTc interval (> 20 ms). 21 Conversely, adagrasib showed a concentration-dependent QTc increase that may exacerbate the risk for ventricular tachyarrhythmias. 28
Clinical Efficacy
Sotorasib
Sotorasib, the first KRAS-targeting therapy, gained accelerated FDA approval in May 2021. This indication was for adults with locally advanced or metastatic NSCLC harboring a confirmed KRAS G12C mutation, who previously received at least 1 systemic therapy. Approval was based on the CodeBreaK100 23 (NCT03600883) clinical trial.
CodeBreaK100, a multicenter, open-label, dose escalation and expansion phase I basket trial, involved 129 patients with advanced tumors and a verified KRAS G12C mutation. The primary outcome was safety, with key secondary outcomes evaluating pharmacokinetic parameters and overall response. Patients were heavily pretreated, with a median of 3 (range, 0-11) previous lines of treatment. For each treatment cycle of 21 days, sotorasib was administered once daily, starting at 180 mg and escalating in sequential cohorts to 360, 720, and 960 mg. After observing no dose-limiting toxicities, a recommended phase II dose (RP2D) of 960 mg once daily was established.
Of the 129 eligible patients, 59 had NSCLC, 42 had colorectal cancer, and 28 had other solid tumors. For the 59 patients with NSCLC, the median follow-up time was 11.7 months (range, 4.8-21.2). A total of 19 patients (32.2%; 95% CI, 20.62%-45.64%) with NSCLC had a confirmed partial response (PR). With an additional 33 patients demonstrating stable disease, the rate of disease control was 88.1% (95% CI, 77.07%-95.09%). Among the 34 patients in the 960 mg cohort, a confirmed objective response was noted in 35.3%. The median time to response and median duration of response (DoR) for those with NSCLC was 1.4 months (range, 1.1-9.5) and 10.9 months (range, 1.1+ to 13.6), respectively. The plus sign signifies the inclusion of patient data censored at the data cutoff, indicating that the duration could potentially extend beyond 1.1 months.
Investigators expanded CodeBreaK100 into a multicenter phase II trial to assess safety and efficacy of sotorasib 960 mg once-daily monotherapy in patients with KRAS G12C-mutated, locally advanced or metastatic NSCLC. 24 Patients were considered eligible if they had progressed following the administration of platinum-based chemotherapy, antiprogrammed death 1 (PD-1) or antiprogrammed death ligand 1 (PD-L1) immunotherapy, or a combined treatment protocol involving both immunotherapy and platinum-based chemotherapy. Key exclusion criteria were untreated brain metastases, systemic anticancer treatment within 28 days of sotorasib initiation, and the receipt of more than 3 previous lines of treatment. The primary endpoint was overall response rate (ORR), as determined by a blinded independent central radiologic review. Secondary outcomes included DoR, disease control, time to response, progression-free survival (PFS), OS, and safety.
From August 13, 2019 to February 5, 2020, the trial enrolled 124 eligible patients, with a median follow-up of 15.3 months (range, 1.1-18.4+), and median duration of treatment of 5.5 months (range, 0.2-17.8). Patient characteristics included the following: median age of 63.5 years (range, 37-80), female sex (50%), White race (81.7%), and former or current smoker (92.9%). Among the 124 evaluable patients, a complete response (CR) was found in 4 patients (3.2%), while a PR was observed in 42 patients (33.9%), yielding a combined ORR of 37.1% (95% CI, 28.6-46.2). Disease control was identified in 100 patients (80.6%; 95% CI, 72.6-87.2). The median time to response was 1.4 months (range, 1.2-10.1), with a median DoR of 11.1 months (95% CI, 6.9 to could not be evaluated). The median PFS and OS were 6.8 months (95% CI, 5.1-8.2) and 12.5 months (95% CI, 10.0 to could not be evaluated), respectively. The exploratory analysis indicated comparable response rates across all subgroups of PD-L1 expression. In addition, the effectiveness of sotorasib was showcased across a range of concurrent genetic mutations, such as STK11 and KEAP1. It’s noteworthy that these specific mutations have previously been linked to less favorable treatment results in patients with NSCLC. 31
Recently, long-term outcomes were reported for the CodeBreaK 100 trial involving 174 pooled patients with KRAS G12C-mutated, locally advanced or metastatic NSCLC. 32 With a median follow-up of 24.9 months (range, 0.7-35.9), sotorasib 960 mg once daily produced an ORR of 41% (95% CI, 33.3-48.4). The median DoR, PFS, and OS for this 2-year analysis were 12.3 months (95% CI, 7.1-15.0), 6.3 months (95% CI, 5.3-8.2), and 12.5 months (95% CI, 10.0-17.8), respectively. Investigators assessed for any potential molecular correlates with safety and efficacy of sotorasib. Durable responses were seen across PD-L1 expression levels. Furthermore, no identifiable trend was noted between PD-L1 tumor proportion scores (TPSs < 1% vs. TPS ≥ 1%) or STK11 and/or KEAP1 alterations. In a targeted exploratory evaluation of sotorasib in 16 patients with brain metastases, investigators identified 3 patients (19%) with a CR and 11 (69%) with stable disease. In the longest follow-up to-date of an FDA-approved KRAS inhibitor, sotorasib demonstrated durable efficacy with no new safety signals.
Based on the ORR and DoR found in the CodeBreaK 100 trial, the FDA granted accelerated approval contingent upon verification of clinical benefit in a future confirmatory trial. Two additional studies, CodeBreaK 200 and CodeBreaK 201, have since been initiated.33,34 The phase III confirmatory trial, CodeBreaK 200 (NCT04303780), is a randomized, open-label, multicenter clinical trial evaluating sotorasib versus docetaxel in previously treated patients with NSCLC harboring the KRAS G12C mutation. Adult patients were eligible if they had locally advanced or metastatic NSCLC, with KRAS G12C-confirmed mutation, and previous treatment with platinum-based chemotherapy and an ICI. Patients were excluded if they had new, untreated, or symptomatic brain lesions, identifiable oncogenic mutations that could be targeted with existing therapy, or if they had previously been treated with docetaxel or a KRAS G12C inhibitor.
Between June 4, 2020 and April 26, 2021, investigators randomized 345 patients (1:1) to receive either oral sotorasib (n = 171) 960 mg daily or intravenous docetaxel (n = 174) 75 mg/m2 every 3 weeks. The primary endpoint was PFS, assessed by a blinded independent review panel using an intention-to-treat methodology. With a median follow-up period of 17.7 months, PFS was significantly longer in the sotorasib group versus docetaxel (hazard ratio [HR] = 0.66; 95% CI, 0.51-0.86; P = 0.0017). The median PFS for sotorasib was 5.6 months (95% CI, 4.3-7.8) versus 4.5 months (95% CI, 3.0-5.7) for docetaxel. The rate of PFS at 12 months was 24.8% for sotorasib and 10.1% for docetaxel. The median duration of treatment exposure in the sotorasib group was 19.9 weeks (range, 0.4-101.3) versus 12.0 weeks (range, 3.0-101.0) in the docetaxel group. Crossover was allowed per protocol, with 46 (26%) patients receiving sotorasib following docetaxel. No difference was seen in OS, with a median OS of 10.6 months for sotorasib versus 11.3 months for docetaxel (HR = 1.01; 95% CI, 0.77-1.33). In the first phase III clinical trial comparing a KRAS G12C inhibitor to chemotherapy, sotorasib demonstrated superior rates of PFS and ORR. Additional data are required to fully assess the effects of sotorasib monotherapy on OS. Although OS is typically considered the ideal trial endpoint, PFS offers a surrogate assessment of the oncolytic activity of sotorasib compared with chemotherapy. Furthermore, the 5.6-month median PFS with sotorasib represents a clinically meaningful improvement over docetaxel for patients with advanced NSCLC who have exhausted other options.
CodeBreaK 201 is an open-label, randomized, phase II global trial (NCT04933695) evaluating sotorasib as first-line therapy in patients with metastatic KRAS G12C-mutated NSCLC with PD-L1 expression < 1% and/or presence of STK11 mutation. Enrollment in CodeBreaK 201 began in January 2022, with an estimated completion date of August 2024.
A real-world, retrospective, multicenter study to assess clinical and genomic features of response and toxicity of sotorasib was conducted in patients with KRAS G12C-mutant NSCLC who received sotorasib in routine practice. 35 With a median follow-up of 13.1 months, a total of 105 patients were identified for evaluation. Patients receiving standard-of-care sotorasib demonstrated a real-world response rate of 28%. Furthermore, treatment resulted in a median PFS of 5.3 months and a median OS of 12.6 months. Investigators found KEAP1 comutations were associated with a shorter PFS (HR = 3.19; P = 0.004) and OS (HR = 4.10; P = 0.003).
The key safety and efficacy findings from these clinical trials can be found in Table 1.
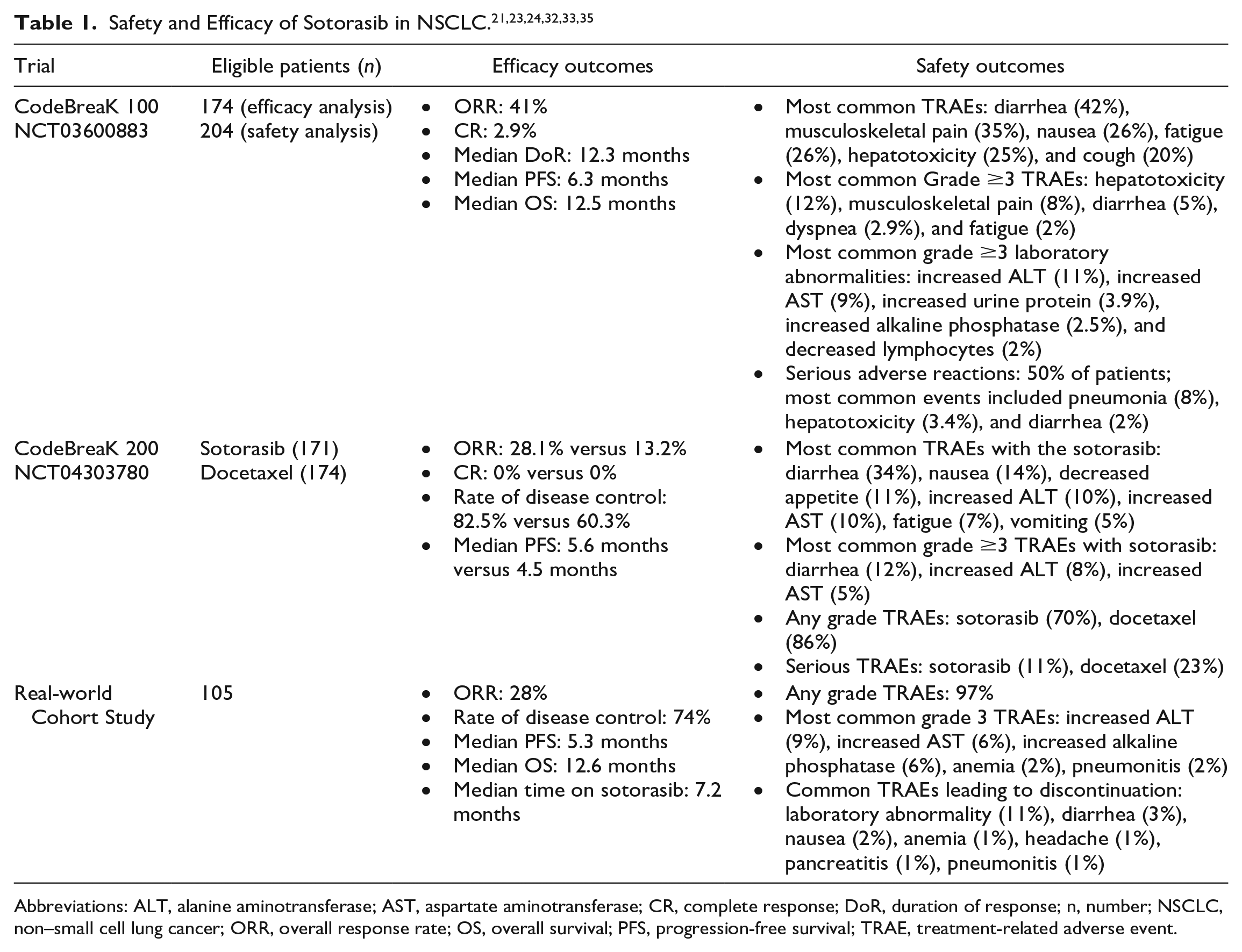
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; CR, complete response; DoR, duration of response; n, number; NSCLC, non–small cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; TRAE, treatment-related adverse event.
Adagrasib
In December 2022, the FDA granted accelerated approval to adagrasib for the treatment of adult patients with locally advanced or metastatic NSCLC harboring the KRAS G12C mutation. The approval was given for the use in patients whose tumors exhibit the KRAS G12C mutation, as confirmed by an FDA-approved test, and who have undergone at least one prior systemic therapy. This approval was based on the KRYSTAL-1 22 (NCT03785249) clinical trial.
KRYSTAL-1 was a first-in-human, open-label, dose escalation and expansion, phase I/Ib clinical trial evaluating the safety, tolerability, phase II dosing, and preliminary effectiveness of adagrasib (MRTX849) on 25 patients with KRAS G12C-mutant solid tumors. After a median follow-up of 19.6 months, initial findings included 18 enrolled patients with NSCLC who received at least 1 dose of adagrasib. Although no maximally tolerated dose was identified, 3 of the 18 evaluable patients experienced a dose-limiting toxicity from adagrasib 600 mg twice daily, which was subsequently determined to be the RP2D. A confirmed PR was observed in 8 of 15 patients (53.3%; 95% CI, 26.6-78.7) with RECIST-evaluable NSCLC who were administered adagrasib 600 mg twice daily.
After observing an acceptable toxicity profile and potential antitumor activity in the phase I/Ib segment of the KRYSTAL-1 trial, the investigators, in collaboration with industry sponsors, expanded the study to encompass a multicenter, single-arm, phase II cohort. 26 Between January 2020 and December 2020, a total of 116 patients with KRAS G12C-mutated NSCLC were enrolled to receive adagrasib 600 mg twice daily until disease progression, unacceptable toxicity, withdrawal of consent, or death. Patients were required to have measurable disease and at least one prior line of systemic therapy with platinum-containing chemotherapy and ICI to be eligible. In addition, key exclusion criteria included active CNS metastases and patients with previous treatment incorporating a KRAS inhibitor. As determined by a blinded independent central review, the primary outcome was ORR. Key secondary endpoints included disease control, DoR, PFS, OS, and safety. Nearly, all enrolled patients (98.3%) had previously received both platinum-based chemotherapy and an ICI. Among the 112 patients with RECIST-evaluable NSCLC, a confirmed ORR of 42.9% (95% CI, 33.5-52.6) was observed. This included 1 patient who showed a CR, and 47 patients who experienced a PR. Overall disease control was 79.5% (95% CI, 70.8-86.5). Seventeen patients could not be evaluated clinically for a best overall response. Among the 95 evaluable patients, the ORR was 50.5%.
Among the 48 responders, the median time to response was 1.4 months (range, 0.9-7.2), and the median DoR was 8.5 months (95% CI, 6.2-13.8). In addition, the median PFS was 6.5 months (95% CI, 4.7-8.4). The median OS and rate of OS at 1 year were 12.6 months (95% CI, 9.2-19.2) and 50.8% (95% CI, 40.9-60.0), respectively. A post hoc evaluation for intracranial response was conducted after preliminary indications suggested CNS-penetrating effects of adagrasib. Investigators highlighted an ORR of 33.3% among 33 patients with previously treated, stable CNS metastases. Given that the majority of these patients (81.8%) had recently received radiation therapy prior to adagrasib initiation, additional research is required to properly evaluate the CNS activity of adagrasib.
Analyses of exploratory biomarkers were conducted to assess the activity of adagrasib in patients with cooccurring mutations in CDKN2A, KEAP1, STK11, and TP53. Patients with these specific genomic variants exhibited ORRs of 58.3%, 28.6%, 40.5%, and 51.4%, respectively, demonstrating activity across commonly occurring comutations. Furthermore, ORRs were observed to be similar across different PD-L1 expression subgroups: < 1% (22 of 47; 46.8%), 1% to 49% (12 of 27; 44.4%), and ≥ 50% (5 of 12; 41.7%). Table 2 highlights the key safety and efficacy findings for adagrasib.
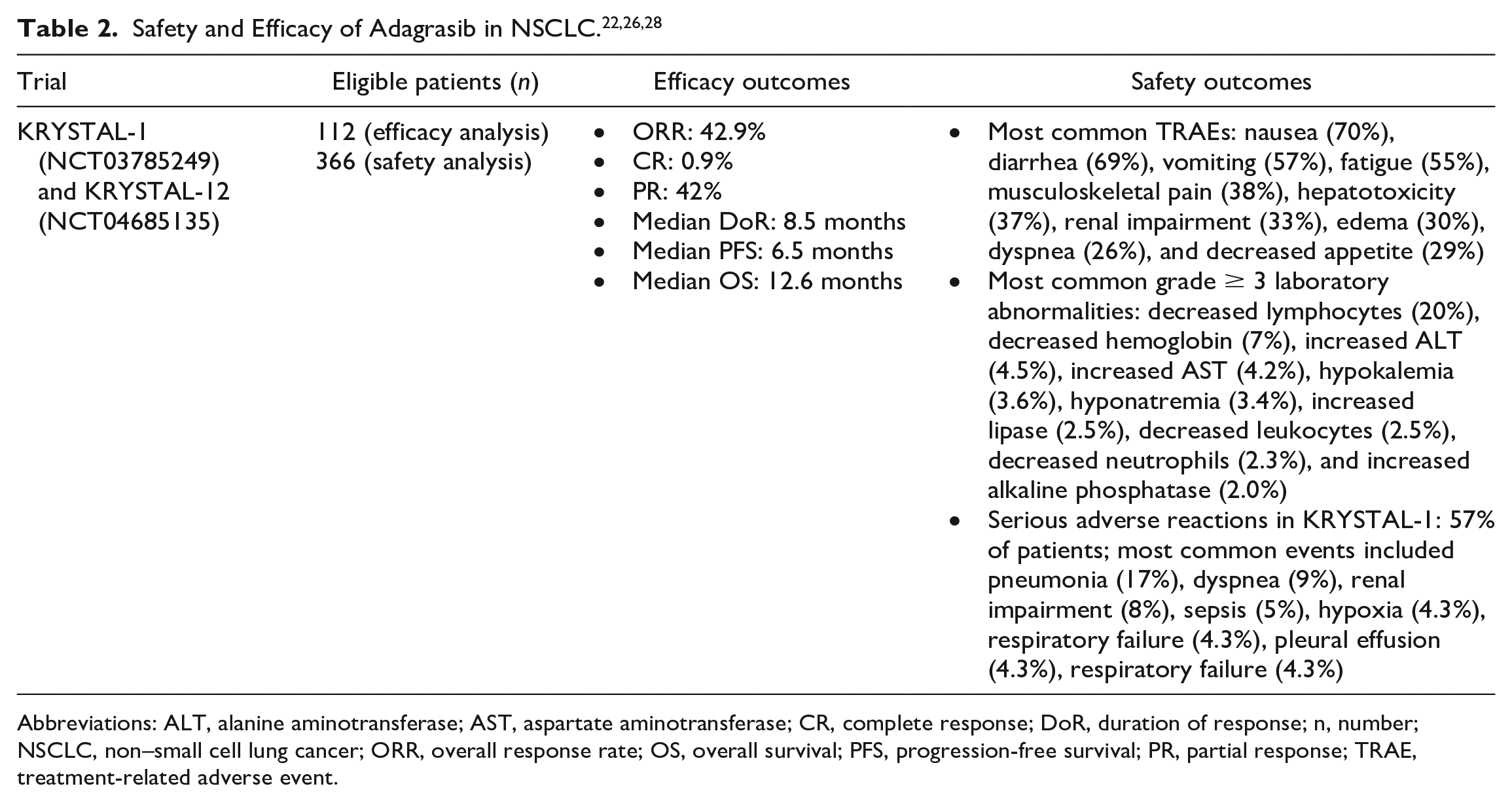
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; CR, complete response; DoR, duration of response; n, number; NSCLC, non–small cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; PR, partial response; TRAE, treatment-related adverse event.
Based on the ORR and tolerability observed in the KRYSTAL-1 trial, the FDA issued accelerated approval, pending validation of clinical benefit in a confirmatory phase III trial. Consequently, the randomized phase III KRYSTAL-12 trial (NCT04685135) was launched, with an expected completion date of May 2025, to evaluate adagrasib versus docetaxel in previously treated patients with KRAS G12C-mutated NSCLC.
Safety
Traditional chemotherapy used in NSCLC often induces a spectrum of toxicities, including alopecia, myelosuppression, nausea, organ dysfunction, and vomiting. Novel small-molecule inhibitors, such as sotorasib and adagrasib, often exhibit a unique toxicity profile in contrast to these conventional cytotoxic agents. These differences can significantly influence both the patient’s quality-of-life and the overall duration of treatment, underscoring the need for meticulous monitoring by a team of well-trained health care providers.
Sotorasib
The safety of sotorasib was assessed in the CodeBreaK 100 trial, involving a subset of patients with KRAS G12C-mutated, locally advanced or metastatic NSCLC. Half of the patients receiving a once-daily dose of sotorasib 960 mg experienced a serious adverse reaction. 24 The most common adverse reactions, occurring in ≥20% of patients, were diarrhea (42%), musculoskeletal pain (35%), nausea (26%), fatigue (26%), hepatotoxicity (25%), and cough (20%). Lab abnormalities observed in ≥25% of patients were decreased lymphocytes (48%), decreased hemoglobin (43%), increased liver function tests (39%), hypocalcemia (35%), increased alkaline phosphatase (33%), increased urine protein (29%), and hyponatremia (28%). 21
The onset of grade ≥ 3 diarrhea and hepatotoxicity occurred at median times of 6.1 weeks (range, 1.7-11.1) and 9.1 weeks (range, 3.1-18.7), respectively. 32 Fatal adverse reactions occurred in 3.4% of patients due to various causes, such as respiratory failure (0.8%), pneumonitis (0.4%), cardiac arrest (0.4%), cardiac failure (0.4%), gastric ulcer (0.4%), and pneumonia (0.4%). Treatment-related adverse events (TRAEs) prompted the permanent discontinuation of sotorasib in 9% of patients, necessitated dose reductions in 5% of patients, and led to dose interruption in 34% of patients. 21
Following FDA approval, sotorasib was studied in a real-world cohort of patients, allowing further understanding of its short- and long-term toxicities. A retrospective, multicenter study of patients who initiated sotorasib outside of clinical trials between June 2021 and August 2022 reported their safety and efficacy findings. 35 This study found that the most common grade ≥ 3 TRAE was elevated liver function tests. In fact, 86% of discontinuations were due to elevated liver function tests, while 21% were due to diarrhea. Interestingly, among the 14 patients who discontinued sotorasib due to TRAEs, all had previously received anti-PD-1/PD-L1 immunotherapy. In contrast, those who had received only platinum-based therapy did not require discontinuation of sotorasib.
Adagrasib
The safety profile, as reflected in the package insert, is based on pooled data from the KRYSTAL-1 and KRYSTAL-12 (NCT04685135) trials. Serious adverse reactions occurred in 57% of patients who received adagrasib, leading to permanent discontinuation of adagrasib in 13% of patients. The most common adverse reactions, occurring in ≥25% of patients, included nausea (70%), diarrhea (69%), vomiting (57%), fatigue (55%), musculoskeletal pain (38%), hepatotoxicity (37%), renal impairment (33%), edema (30%), dyspnea (26%), and decreased appetite (29%). 28 Although not yet listed in the National Comprehensive Cancer Network (NCCN) Antiemesis Guidelines, adagrasib would be classified as having a moderate to high emetogenic potential (≥ 30% frequency of emesis). 36 In contrast, sotorasib is currently listed as having minimal to low emetogenicity.
The most common grade 3 or 4 (≥20%) laboratory abnormalities were decreased lymphocytes (20%), decreased hemoglobin (7%), increased alanine aminotransferase (4.5%), increased aspartate aminotransferase (4.2%), hypokalemia (3.6%), hyponatremia (3.4%), increased lipase (2.5%), decreased leukocytes (2.5%), decreased neutrophils (2.3%), and increased alkaline phosphatase (2.0%). 28
The KRYSTAL-1 trial, focusing on patients with NSCLC, revealed that 77% of patients experienced dose interruptions due to adverse reactions, and 28% required dose reductions. 28 Notably, adagrasib can cause concentration-dependent QTc prolongation. In the pooled safety population, increases from baseline QTc of > 60 ms were observed in 11% of patients, heightening the risk of ventricular arrhythmias. 28 This effect necessitates caution when using adagrasib in patients already on other QTc-prolonging agents, those with congenital long QT syndrome, or those with preexisting QTc prolongation.
Hepatotoxicity is another significant concern with adagrasib. Increased liver function tests were noted in 32% of patients, and hepatotoxicity of any grade was reported in 37%, with 7% experiencing grade 3 or 4 events. Hepatotoxicity led to dose interruption or reduction in 12% of patients. In addition, interstitial lung disease and pneumonitis occurred in 4.1% of patients, typically manifesting within a median of 12 weeks. 28
Warnings and Precautions
Sotorasib and adagrasib, while not carrying boxed warnings, have been associated with potentially severe reactions requiring close monitoring. Among these are significant gastrointestinal (GI) adverse reactions, including diarrhea, nausea, and vomiting.21,28 Gastrointestinal adverse reactions should be treated with supportive care, including correction of dehydration with intravenous fluids, antiemetic medications, and antimotility agents as indicated.
Sotorasib treatment may result in hepatotoxicity and, in rare cases, interstitial lung disease or pneumonitis. 21 Liver function tests should be monitored every 3 weeks for the first 3 months of treatment, then once monthly as clinically indicated. In addition, any new or worsening pulmonary symptoms should be promptly addressed. This risk is particularly significant in patients previously treated with immunotherapy or radiotherapy. 37
According to manufacturer recommendations, liver function tests should be monitored prior to initiating adagrasib, followed by monthly monitoring for the first 3 months, and then clinically as indicated thereafter to detect hepatotoxicity. Adagrasib has been linked to QTc prolongation, with increases > 60 ms observed in patients with preexisting long QT syndrome, prolonged QTc, or those concurrently on medications known to prolong the QTc. 22 Patients were typically impacted once steady-state concentrations of adagrasib were achieved, but QTc did not generally increase later in treatment. 38 Thus, it is important to monitor both electrolytes and electrocardiograms (ECGs) in patients at risk of QT prolongation while on adagrasib. 28
In addition, any new or worsening symptoms presenting as dyspnea, cough, or fever for patients on adagrasib should be closely monitored due to increased risk of interstitial lung disease or pneumonitis, as evidenced by a case of grade 3 pneumonitis reported in the KRYSTAL-1 trial.22,38 In the event of any grade 3 or 4 GI adverse reactions, dose modifications or reductions per the manufacturer’s recommendations should be considered. 28
Interactions
Sotorasib should be avoided with acid-reducing agents, such as proton pump inhibitors or H2-receptor antagonists, as they can decrease sotorasib concentrations. If an acid-reducing agent cannot be avoided, sotorasib should be administered 4 hours before or 10 hours after an antacid. 21
Coadministration with strong CYP3A4 inducers could lower sotorasib concentrations, potentially limiting its clinical efficacy. Furthermore, since sotorasib itself is a moderate CYP3A4 inducer, it can therefore reduce the plasma concentrations of CYP3A4 substrates. 21 If coadministration cannot be avoided, clinicians should consider increasing the dose of the CYP3A4 substrates in accordance with their prescribing information. In addition, sotorasib inhibits the metabolism of P-gp substrates, such as digoxin, potentially leading to increased concentrations of these substrates. 21
Adagrasib inhibits CYP3A4, CYP2C9, CYP2D6, and P-gp. As such, its concomitant use with sensitive substrates of these enzymes and transporters can increase their exposure, leading to an elevated risk of adverse reactions. 28 Furthermore, adagrasib also acts as a substrate of CYP3A4, and coadministration with strong CYP3A inducers or inhibitors should be avoided. In particular, strong CYP3A4 inhibitors should not be used until steady-state concentrations of adagrasib have been reached. 28 Due to QTc prolongation risk, patients should avoid using other QT-prolonging medications while on adagrasib. If such agents can’t be avoided, patients should undergo ECG and electrolyte monitoring prior to initiation, during concomitant use with other QT-prolonging agents, and as clinically indicated. Adagrasib should be held if the QTc interval is ≥500 ms or shows a change from baseline of >60 ms. 28 The concurrent use of QT-prolonging agents with adagrasib can heighten the risk of ventricular arrhythmias, such as Torsade de Pointes, and even sudden death. 28
Dosing and Administration
Sotorasib is only available as 120 and 320 mg tablets. The recommended dosing for sotorasib is 960 mg orally once daily until disease progression or unacceptable toxicity. Sotorasib can be taken with or without food. 21 Doses should be taken at the same time each day, and if a dose is inadvertently missed by more than 6 hours, the dose is skipped and the patient should proceed to take a dose the next day as prescribed. 21 Sotorasib tablets should be swallowed whole but can be fully dispersed in 120 mL of non-carbonated, room temperature water without crushing. The tablets will not completely dissolve, but the resulting solution should be consumed within 2 hours of dispersion. Any undissolved tablet particles should be consumed by rinsing the container with an additional 120 mL of water and drinking. 21
In the event of grade 3 or 4 adverse reactions, dosage modifications for sotorasib are allowed, but a maximum of 2 dose reductions are permitted. The first dose reduction is 480 mg once daily, and the second is 240 mg once daily. If intolerable adverse reactions, such as diarrhea or hepatotoxicity persist at the minimum dose of 240 mg once daily, sotorasib should be discontinued. 21
Adagrasib is available as a single-strength tablet of 200 mg. There are currently no capsule or intravenous formulations available. Food and Drug Administration labeling recommends dosing at 600 mg twice daily until disease progression or a grade 3 or 4 adverse reaction, necessitating dose modification.22,28 In the event of adverse reactions, a maximum of 2 dose reductions is permitted: the first dose reduction is 400 mg twice daily, and the second is 600 mg once daily. Tablets should not be crushed, split, or chewed. If a patient vomits, another dose should not be taken. Like sotorasib, adagrasib can be taken with or without food. If a dose is missed and more than 4 hours have elapsed from the expected dosing time, the missed dose should be skipped and the next scheduled dose taken as planned. 28
Relevance to Patient Care and Clinical Practice
Activating mutations in the KRAS proto-oncogene, discovered and characterized over 40 years ago, represent a distinct biological subtype. Among North Americans with adenocarcinoma, these somatic driver mutations in KRAS are the most common oncogenic alterations, posing a significant unmet medical need. In contrast to other actionable mutations, such as ALK rearrangements or EGFR mutations, KRAS mutations exhibit a strong correlation with cigarette smoke exposure and typically indicate a poor prognosis. 39 Historically, patients with advanced or metastatic KRAS-mutated NSCLC have derived limited benefits from multi-agent chemotherapy.
Single-nucleotide KRAS G12C mutations, identified in up to 14% of patients with NSCLC, have emerged as a new therapeutic target.22,40 The accelerated approvals of sotorasib and adagrasib represent a significant milestone in cancer treatment, offering a newfound hope for this vulnerable patient population. Despite demonstrating response rates of approximately 40% in pivotal phase II clinical trials, anti-KRAS therapies have proven less efficacious than treatments targeting other actionable mutations in NSCLC. 14 This disparity may be attributable to a myriad of factors present in KRAS-mutated NSCLC, including multiple intrinsic drug resistance mechanisms, concurrent molecular alterations, intratumor RAS-mutant heterogeneity, and suboptimal immunogenic profiles.14,39,40
To address these challenges, several innovative treatment approaches are being pursued. For example, KRAS mutations are linked with a pro-inflammatory microenvironment, and ongoing research is assessing the efficacy of ICIs, either alone or in combination with anti-KRAS therapy.14,41,42 Other research is exploring combination therapies to circumvent drug resistance and cotarget cell signaling pathways. 39 Several non-FDA-approved KRAS inhibitors are currently under investigation, including GDC-6036 (NCT04449874), JDQ443 (NCT05445843), GFH925 (NCT05756153), and JAB-21822 (NCT0527626). In this rapidly evolving landscape of targeted medicine, these initiatives aim to further the treatment paradigm for patients with KRAS-mutated NSCLC.
The NCCN continues to recommend conventional chemoimmunotherapy as the preferred first-line treatment option for eligible patients with KRAS-mutated NSCLC. 7 However, the advent of KRAS G12C inhibitors has paved the way for new possibilities for second-line treatment. According to NCCN guidelines, sotorasib or adagrasib should be considered for patients with locally advanced or metastatic KRAS G12C-mutated NSCLC following disease progression after at least one line of therapy. With no head-to-head clinical trials evaluating sotorasib against adagrasib, and no preference stated in the NCCN guidelines, intertrial comparisons of the 2 medications should be done with caution. Nonetheless, sotorasib and adagrasib demonstrated similar ORRs (41% vs. 42.9%), PFS (6.3 vs. 6.5 months), and OS (12.5 vs. 12.6 months) in phase II clinical trials.26,33
Despite similar efficacy profiles of sotorasib and adagrasib in NSCLC, they possess notable differences warranting consideration. For instance, sotorasib has a shorter half-life (5.5 hours) and requires only once-daily dosing. In contrast, adagrasib has a significantly longer half-life of 24 hours. However, due to a high pill burden and propensity for postdose emesis, adagrasib necessitates a twice-daily regimen. Furthermore, adagrasib demonstrates clinically significant CNS penetration, which may prove useful for patients with CNS metastases—a common occurrence at diagnosis in patients with KRAS G12C-mutated NSCLC (27%-42%). 43 There is a recognized need for CNS-penetrating therapies with clinically significant anticancer activity, and to address this, ongoing studies are currently evaluating the compartment-specific activity of both sotorasib and adagrasib.43-46
From a safety perspective, both KRAS inhibitors shared several notable toxicities. Adverse reactions occurring in ≥ 20% of patients include cough, diarrhea, fatigue, hepatotoxicity, musculoskeletal pain, and nausea.21,28 Both drugs can induce certain laboratory abnormalities, such as decreased lymphocytes, increased aspartate aminotransferase, hyponatremia, decreased hemoglobin, and increased alanine aminotransferase. These shared toxicities necessitate careful clinical assessment and therapeutic management. Of note, adagrasib, unlike sotorasib, may cause QTc interval prolongation. Overall, the rate of drug discontinuation due to adverse reactions is similar for both drugs (7.1% for sotorasib and 6.9% for adagrasib). At this time, clinician choice of agent should focus on adverse effect profile, patient characteristics, and individual preferences based on insurance coverage and drug affordability. With observed QT-prolonging effects, avoiding adagrasib in at-risk patients may be warranted.
Sotorasib and adagrasib both require diagnostic testing to confirm the KRAS G12C mutation in NSCLC tumor tissue samples. The FDA has approved several companion diagnostic tests for determining KRAS G12C mutation status in NSCLC, including the Guardant360 CDx for sotorasib, the Therascreen KRAS Kit for sotorasib, and the Agilent Resolution ctDx assay for adagrasib. Like many other targeted anticancer therapies, the widespread adoption of sotorasib and adagrasib will be influenced by their cost-effectiveness. Currently, The IBM Micromedex Redbook database lists the average wholesale price for sotorasib as $24 133 per bottle containing 90 capsules of 320 mg each, with a 1-month supply of adagrasib comparably priced at $23 700 per bottle, which includes 180 capsules of 200 mg each. 47
The goals of treating metastatic NSCLC focus heavily on prolonging survival while optimizing quality of life. The toxicity profiles of targeted therapies, such as sotorasib and adagrasib, often differ from those of conventional cytotoxic chemotherapy. By delaying disease progression and potentially reducing symptom burden from TRAEs, these agents align with the palliative goals of advanced NSCLC care. It is important to note that cost and access to care remain barriers that may limit the therapeutic and quality-of-life benefits in real-world settings.
Conclusion
The development of KRAS-targeting therapies has significantly altered the treatment landscape for NSCLC, bridging a longstanding gap in the treatment paradigm for patients with KRAS G12C mutations. Decades of focused research efforts have now shifted the perception of drugging the “undruggable.” In NSCLC, the constitutively active and tumorigenic KRAS G12C protein can now be effectively targeted with 2 novel FDA-approved drugs. Sotorasib is a once-daily oral formulation that demonstrated improved response rates and PFS when compared with a standard second-line chemotherapy regimen of docetaxel in patients with locally advanced or metastatic disease. Adagrasib, a twice-daily oral option, is currently undergoing evaluation in a confirmatory phase III clinical trial against second-line docetaxel. Additional clinical questions remain as KRAS G12C is now an established therapeutic target, including treatment strategies to overcome resistance mechanisms, optimal treatment sequencing, the role of comutations on treatment safety and efficacy, and the potential therapeutic synergies with other anticancer agents. Future research is required to address these emerging questions, promising to further refine and advance the utilization of KRAS-targeted therapies in NSCLC and other malignancies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.