
Abstract
Background:
Immune thrombocytopenic purpura (ITP) in adults typically develops slowly and insidiously. The ITP medications might be linked to psychological disorders, but the connection is not well-understood.
Objective:
This study aimed to examine the association between ITP medication use and the risk of depression among participants in the National Health and Nutrition Examination Survey (NHANES) from 2005 to 2018.
Methods:
Using data from 70 190 NHANES participants, we conducted a cross-sectional study, excluding individuals under 18 years, with hypertension, HIV, hepatitis C, and various comorbidities. A total of 17 299 individuals were included in the analysis of this study. We identified 2 populations within this study: those using ITP medications, including prednisone, dexamethasone, and rituximab and those not using ITP drugs. Depression status was assessed using the Patient Health Questionnaire–9 (PHQ-9), and the relationship between ITP medication use and depression was analyzed through multivariate logistic regression.
Results:
There was no significant association between ITP medication use and an increased risk of depression after adjusting for demographic and health-related variables. Notably, among the study participants, 1.8% of the non-depressed population were on ITP medication compared with 0.3% in the depressed population. The analysis revealed varying depression risks associated with different sociodemographic factors. For instance, the correlation between ITP medication and depression risk was influenced by a combination of age, race, income, and smoking status.
Conclusion and Relevance:
The study suggests that ITP medication use does not independently increase the risk of depression. This finding is crucial for guiding clinical decisions and managing patient expectations regarding ITP treatment and its psychological impacts.
Introduction
Immune thrombocytopenic purpura (ITP) is a hematological disorder characterized by a reduction in platelet count within the blood. A decrease in platelets can lead to easy bruising, gum bleeding, and internal hemorrhages. In the United States, it is estimated that there are 9.5 cases of ITP per 100 000 individuals. Globally, it is estimated that over 200 000 individuals suffer from ITP at any given time. 1 The International Working Group defines primary ITP as a platelet count below 100 × 109/L in the absence of other causes or underlying conditions. Although ITP is a heterogeneous syndrome with a diverse pathogenesis, the mechanisms leading to platelet reduction during ITP predominantly involve peripheral destruction of platelets by the blood, spleen, and liver, as well as inappropriate bone marrow production due to autoimmunity against megakaryocytes and insufficient levels of thrombopoietin (TPO). 2 Given the disease’s insidious onset, even experienced clinicians can misdiagnose it, necessitating vigilant observation and attention. On the contrary, although the prevalence is not high and the harm to patients is not significant, the usual treatment medications that involve corticosteroids for ITP patients may lead to an increased risk of depression. 3
Corticosteroids are widely used to relieve the signs and symptoms of many diseases, including common inflammatory and autoimmune disorders affecting various organ systems. 4 However, corticosteroids also induce severe psychiatric adverse effects, including delirium, depression, mania, psychosis, and cognitive/memory impairment. These adverse effects occur in up to 60% of patients taking corticosteroids, with recent studies showing an increased rate of psychopathologies in this population. 5 The proposed mechanisms underlying corticosteroid-induced psychiatric changes involve complex interactions with neurotransmitter systems, alterations in brain structure and function, and disruptions in the hypothalamic-pituitary-adrenal (HPA) axis. Long-term use of corticosteroids can lead to persistent mood and behavioral changes, severely impacting the quality of life, employment, and health status of affected individuals. 5
Depression is a common affective disorder characterized by persistent sadness, hopelessness, feelings of worthlessness, and a lack of interest in previously pleasurable activities, severely disrupting patients’ psychosocial functions and reducing the quality of life. According to the American Society of Hematology (ASH) guidelines, first-line ITP medications such as prednisone or dexamethasone may induce depression. However, current studies provide conflicting evidence. For example, some studies have indicated that oral dexamethasone can significantly alleviate symptoms in patients with depression. 6 In contrast, other studies suggest that long-term corticosteroid use may induce both depressive and manic symptoms. 7 For instance, Brown et al 8 reported that long-term treatment with prednisone increased manic symptoms in asthma patients, with no significant impact on depression. In addition, treatment with antiglucocorticoid compounds benefits patients with severe depression. 9 These findings, taken together, make the interpretation of the cumulative evidence regarding the efficacy of corticosteroids as mood disorder therapeutics more complex. Nevertheless, the question of whether prednisone and dexamethasone, as first-line treatments for ITP, increase the risk of depression remains unclear; thus researching, the risk factors and valid predictors to alleviate the public health burden is necessary and crucial.
Therefore, the potential increase in depression risk associated with first-line ITP medications warrants attention and necessitates research into the potential consequences of such treatments. However, studies on the association between ITP medication use and the risk of depression are scarce. This study aims to investigate the impact of ITP medication on depression using data from the National Health and Nutrition Examination Survey (NHANES).
Methods
Search Population
We analyzed data from the NHANES, a cross-sectional, complex, multistage probability sampling design conducted by the Centers for Disease Control and Prevention (CDC) that oversamples minorities and the elderly to ensure the survey results are applicable to the broader US population. The NHANES survey combines interviews and physical examinations. Interviews include questions on demographics, socioeconomics, diet, and health. The examination component consists of medical, dental, and physiological measurements, as well as the collection of participants (self-reported) data using the Computer-Assisted Personal Interviewing (CAPI) system by trained interviewers and examination personnel. The NHANES data are released in 2-year cycles. To obtain a large sample size for analysis, we combined data from 7 consecutive NHANES cycles from 2005 to 2018. The Institutional Review Board (IRB) of the National Center for Health Statistics approved the ethical review. All individuals provided written informed consent before participating in the study (for more information about NHANES, please visit: http://www.cdc.gov/nhanes).
Diagnosis of Depression
Depression outcomes were assessed using the Patient Health Questionnaire–9 (PHQ-9), a brief screening instrument that is an effective tool for evaluating depression. It scores the symptoms and signs of depression from “0” (not at all) to “3” (nearly every day), based on the 9 diagnostic criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders. 10 Each subject’s PHQ score is the sum of all answers to the PHQ questions (ranging from 0 to 27). The PHQ-9 is a validated instrument based on the Diagnostic and Statistical Manual of Mental Disorders (5th edition; DSM-5) criteria. With a possible total score of 27, a cut-off point of ≥10 indicates a sensitivity of 88% and a specificity of 88% for diagnosing major depression. 10 Therefore, we categorized participants’ PHQ-9 scores into <10 (no depression) and ≥10 (depression). Exclusion criteria included individuals with a pre-existing diagnosis of mental health disorders or those currently undergoing treatment with antidepressants. This criterion ensured that the observed psychiatric effects could be more accurately attributed to corticosteroid use rather than pre-existing conditions or other medications.
Exposure
During the household interview portion of the survey, interviewers asked participants whether they had taken prescription medication in the past 30 days. Those who answered “yes” were asked to show the interviewer the medication containers for all medications used. If no container was available, participants were asked to name the prescription medications they used. The names and therapeutic classes of the medications were coded using Lexicon Plus, a comprehensive database of all prescription and some non-prescription drug products available in the US market, maintained by Cerner Multum, Inc., Kansas City, MI, USA. For NHANES, the Lexicon Plus files were modified, updated annually, and uploaded to a laptop computer with a search engine for interviewer use. 11 An extensive literature search was conducted, and the ASH guidelines were consulted to determine the medication status for ITP. First-line medications included prednisone and dexamethasone, and second-line medications included rituximab; we defined all first-line and second-line medications as ITP medications. In addition, we identified and excluded medications potentially affecting the outcome. Patients taking medications such as polystyrene sulfonate, 12 sulfamethoxazole, 13 fluoroquinolones, 14 benzathine penicillin, 15 sulfonamides, 16 nitrobenzene, 17 and heparin 18 were excluded from the study. These medications were excluded due to their known potential to interact with corticosteroids and independently influence psychiatric symptoms. 19 Such interactions could confound the study results, making it challenging to isolate the effects of corticosteroids on mental health outcomes.
Covariates
Sociodemographic data such as sex, race/ethnicity, and educational level were collected by NHANES personnel during household interviews. Standardized questionnaires were used to gather information on age, sex, race/ethnicity, education, annual household income, smoking status, and alcohol intake. Race/ethnicity was categorized into Mexican American, other Hispanic, non-Hispanic white, non-Hispanic black, or other. Education levels were divided into below 9th grade, 9th to 11th grade, high school graduate or equivalent, some college or Associate of Arts (AA) degree, and college graduate or above. Participants were classified as former smokers or current smokers based on their response to questions regarding “smoking at least 100 cigarettes in their lifetime” and “currently smoking.” Alcohol consumption status was derived from the question: “At least 12 drinks in a year?” Height, weight, and blood pressure were measured using a standardized protocol. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2). Hypertension was defined as currently taking antihypertensive medication, or if not taking medication, having a systolic blood pressure level of ≥130 mm Hg and/or a diastolic level of ≥80 mm Hg, according to the 2017 American College of Cardiology/American Heart Association guidelines for hypertension. 20 We excluded individuals with HIV and hepatitis C infections, as their immunity might be compromised, affecting the outcomes.
Statistical Analysis
Continuous variables were presented as mean values ± standard deviation (SD), and categorical variables were presented as frequencies or percentages. For the analysis of baseline characteristics, univariate analysis of variance was used for continuous variables, and the Rao-Scott χ2 test was used for categorical variables. The relationship between ITP medication uses and depression status was studied using multivariate logistic regression, calculating the odds ratios (ORs) and 95% confidence intervals (CIs). We used both unadjusted and multivariable-adjusted models. In this study, model 1 did not correct for covariates, model 2 adjusted for age and sex, model 3 corrected for race, educational level, BMI, smoking status, and alcohol intake, and model 4 was model 2 plus model 3. All statistical tests were 2-sided, and SAS v. 9.4 (SAS Institute, Cary, North Carolina), along with GraphPad Prism (GraphPad Software, La Jolla, California), was used to create forest plots. A P-value of <0.05 was considered statistically significant.
Results
This cross-sectional study used the population data from continuous NHANES assessments between 2005 and 2018 (n = 70 190). We excluded individuals under 18 years of age (n = 33 931), those with hypertension (n = 17 129), those co-infected with HIV or hepatitis C (n = 161), and those with comorbid conditions like heart failure, coronary artery disease, angina, myocardial infarction, stroke, cancer, or malignant neoplasms (n = 1659). The study population thus comprised 17 319 individuals. Further exclusions were made for those receiving polypharmacy treatments such as polystyrene sulfonate, sulfamethoxazole, fluoroquinolones, benzathine penicillin, sulfonamides, nitrobenzene, and heparin (n = 20), leading to a final analysis population of 17 299 individuals. Participants prescribed ITP medications, including prednisone, dexamethasone, and rituximab, were identified (Figure 1).
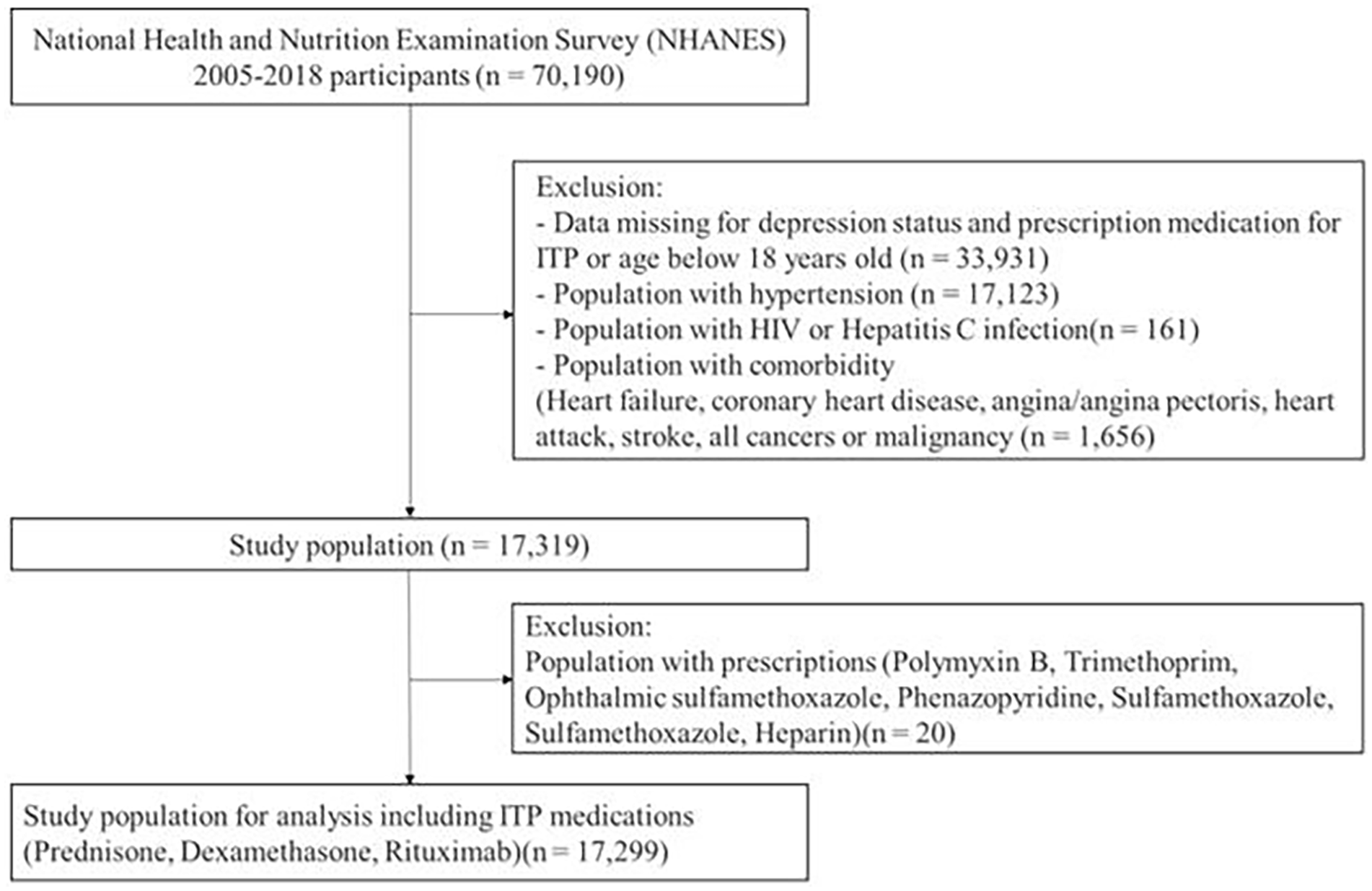
Flowchart of screening progress.
Table 1 presents the characteristics of NHANES participants from 2005 to 2018 categorized by depression status. Overall, the average age of non-depressed participants was 37.6 years, whereas the average age of depressed participants was 36.6 years. The 18 to 45 age group was the most represented, followed by 46 to 65, 65 to 75, and over 75 years age groups. Females slightly outnumbered males. Regarding family Poverty Income Ratio (PIR), after excluding population without values (referred to missing), 18.3% of the non-depressed population had family incomes below 130% of the federal poverty level, whereas 37.9% had family incomes exceeding 350% of the poverty level. Conversely, in the depressed population, these figures were 2.5%, 2.1%, and 1.4%, respectively. Non-Hispanic whites constituted the majority, followed by non-Hispanic blacks, Mexican Americans/other Hispanics, and non-Hispanic Asians. For education level, among the non-depressed population, 34.8% had not completed high school, 29.2% had some college education, and 29.5% were college graduates or higher, whereas among the depressed population, 3.4%, 2.2%, and 0.9%, respectively. In terms of BMI, the majority of the population is at normal levels of weight, followed by overweight levels, obesity, with the least number of people underweight. The number of people who drink alcohol or smoke cigarettes is generally lower than the number of people who do not have these habits. In addition, 1.8% of participants were using ITP medications among non-depressed population and 0.3% among depressed population.
Characteristics of Participants by Depression Categories in the National Health and Nutrition Examination Survey (NHANES), 2005 to 2018.
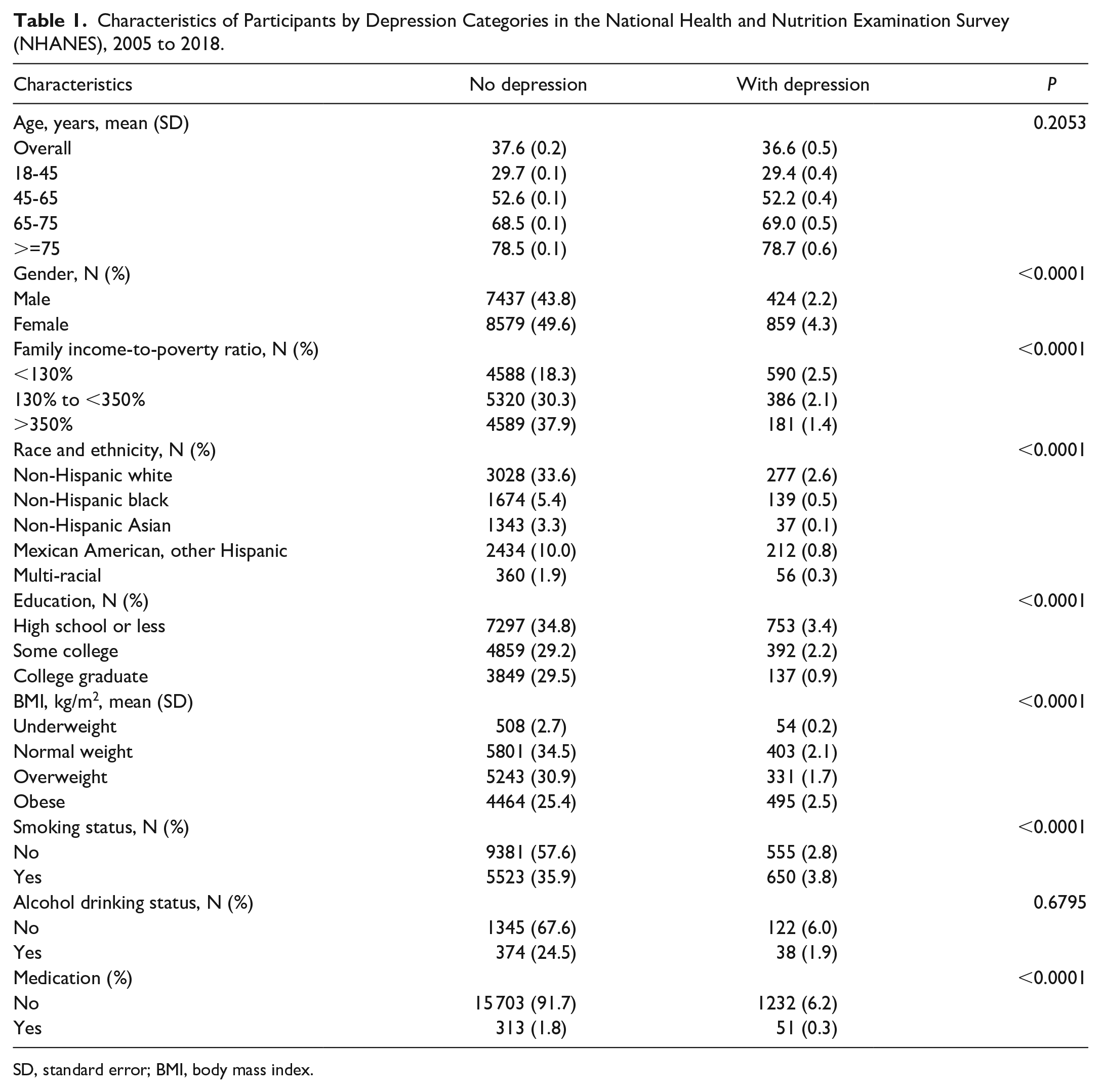
SD, standard error; BMI, body mass index.
Through multivariate logistic regression analysis, we identified significant associations with depression (Table 2 and Figure 2). In model 1 (unadjusted), medication use was negatively correlated with depression (OR = 0.417, P < 0.0001). This negative correlation persisted in model 2 after adjusting for age and sex (OR = 0.414, P < 0.0001). However, in model 3 (adjusted for household income, race, education, BMI, smoking, and drinking status), the association was not statistically significant (OR = 0.626, P = 0.3948). In addition, gender, age, race, and household income were significant factors. For example, compared with multiple races, non-Hispanic whites (OR = 0.521, 95% CI = 0.272-0.997), non-Hispanic Asians (OR = 0.234, 95% CI = 0.100-0.546), and Mexican Americans/other Hispanics (OR = 2.933, 95% CI = 1.739-4.948) had varying odds of depression. The 18 to 45 age group had a higher risk of depression compared with those over 75 years (OR = 14.117, 95% CI = 1.636-121.787). In model 4 (adjusted for household income, race, education, BMI, smoking, and drinking status), these associations remained significant. For instance, non-Hispanic Asians had a significantly lower risk of depression compared with those of multiple races (OR = 0.270, 95% CI = 0.112-0.655). Overweight individuals (OR = 0.836, 95% CI = 0.512-1.365) did not have a significant risk of depression compared with those of normal weight, whereas smokers (OR = 0.477, 95% CI = 0.306-0.744) had a lower risk of depression. These results suggest no direct causal relationship between ITP medications and depression after controlling for other factors, highlighting the need to consider a combination of relevant factors when evaluating depression risk.
Adjusted Associations of Medication Use with Depression, NHANES 2005 to 2018.
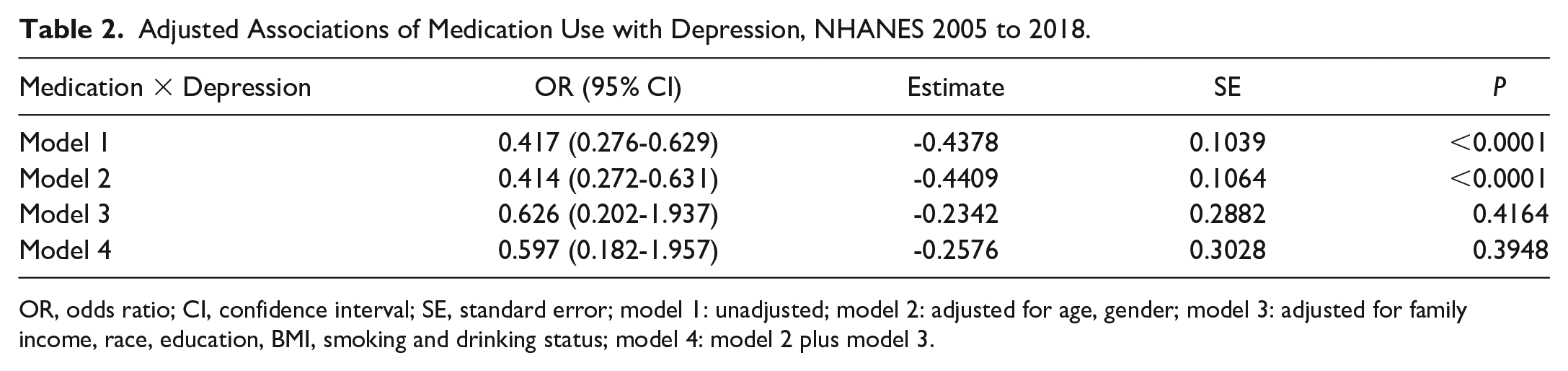
OR, odds ratio; CI, confidence interval; SE, standard error; model 1: unadjusted; model 2: adjusted for age, gender; model 3: adjusted for family income, race, education, BMI, smoking and drinking status; model 4: model 2 plus model 3.
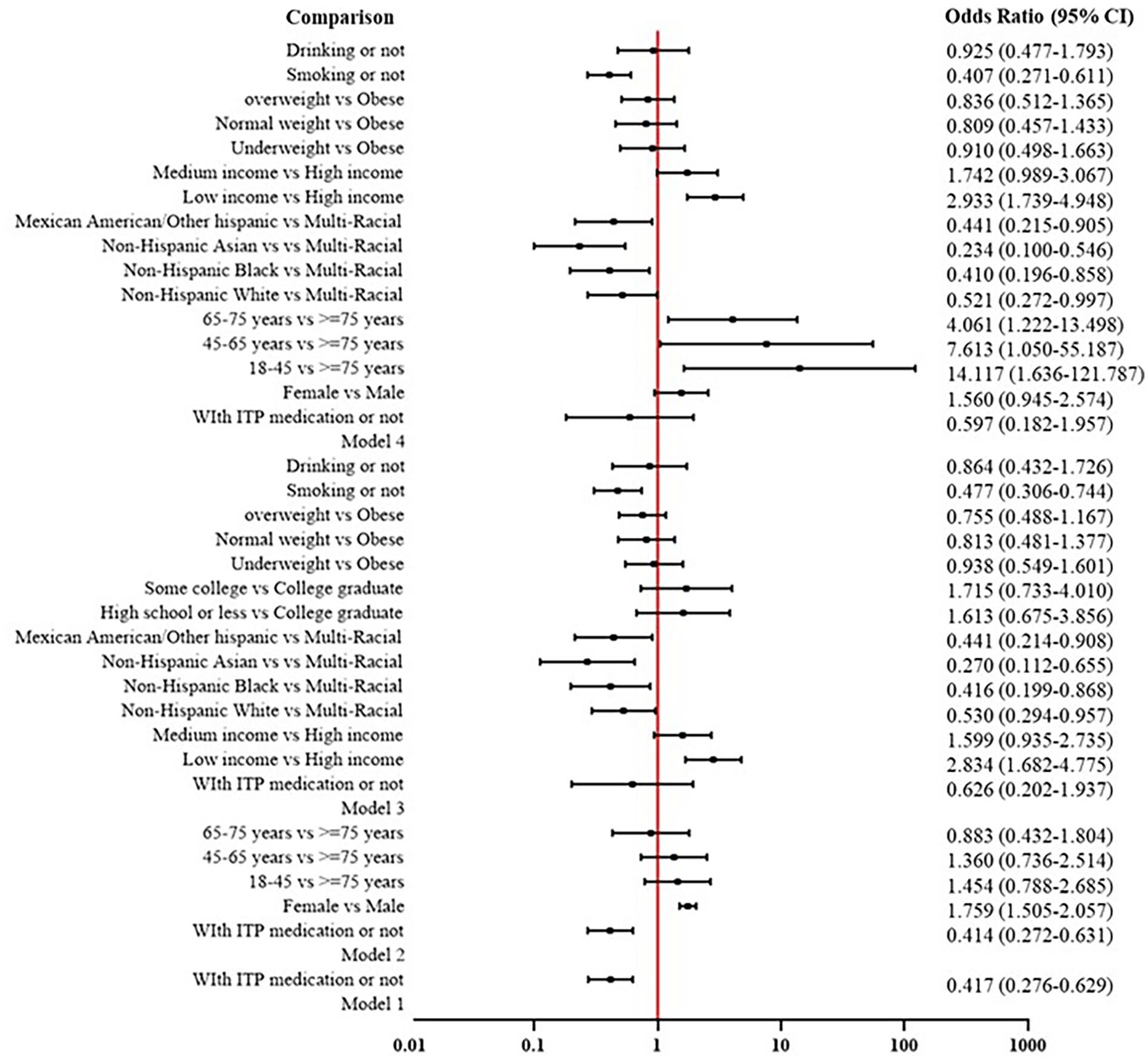
Multivariate logistic regression of medication use and depression (OR, odds ratio; CI, confidence interval; model 1: unadjusted; model 2: adjusted for age, gender; model 3: adjusted for family income, race, education, BMI, smoking and drinking status; model 4: model 2 plus model 3).
Discussion
Our study aligns with the guidelines by the ASH, 21 which emphasize the management of ITP without strong recommendations for various treatments due to a lack of evidence, often favoring strategies to avoid medication adverse effects. Despite the low prevalence of ITP, its psychological aspects still need attention, as ITP medication may affect mental health. 22 The prevalence and consequences of depression present an ever-increasing challenge globally, necessitating a deeper understanding of its risk factors. 23 The noted incidence of depression among ITP patients 22 further supports the importance of routine depression screening during follow-up care. This study aimed to examine the association between ITP medication use and depression among participants in the NHANES data set from 2005 to 2018. Our analysis included 17 299 individuals from NHANES data, and the findings indicated that there was no significant association between ITP medication use and an increased risk of depression after adjusting for demographic and health-related variables. Among the study participants, 1.8% of the non-depressed population were on ITP medication compared with 0.3% of the depressed population. This lack of significant association suggests that other factors may play more critical roles in influencing depression risk among patients. Our study’s findings align with previous research that has shown mixed results regarding the impact of corticosteroids on mental health. 24 Some studies have highlighted the potential for these medications to induce mood disturbances, whereas others have suggested that they can have mood-stabilizing effects in certain contexts. 25 For instance, a study on the use of dexamethasone in patients with asthma indicated that although corticosteroids could alleviate depressive symptoms, they also had the potential to induce manic symptoms. 26 This complexity underscores the importance of considering individual patient characteristics and the specific context of corticosteroid use when evaluating their psychotropic effects.
Prednisone use has been specially associated with higher anxiety symptom scores. 27 The theoretical psychotropic effects of steroids, such as prednisone and dexamethasone, are complex and multifaceted. Previous studies have shown conflicting evidence regarding the impact of corticosteroids on mood and mental health. For instance, some research suggests that corticosteroids can alleviate depressive symptoms in certain patients, whereas other studies indicate that long-term use of these medications can induce depressive and manic symptoms.25,26 This dichotomy may be due to the different underlying mechanisms through which corticosteroids exert their effects on the brain. For example, prednisone has been associated with higher anxiety symptom scores, potentially due to its impact on neurotransmitter systems involved in mood regulation. 28 Our analysis revealed an OR of 0.407 for smokers compared with non-smokers regarding medication use and depression. This finding suggests that smokers may have a different baseline risk or protective factors affecting depression. Nicotine, the primary psychoactive component in tobacco, interacts with neurotransmitter systems that are involved in mood regulation, such as dopamine and serotonin pathways. 29 Nicotine’s complex interaction with these systems can result in both antidepressant and anxiogenic effects, depending on the context and individual susceptibility. 28 Therefore, smokers may exhibit a different pattern of depression risk compared with non-smokers, potentially explaining the lower observed OR in this population.
Individuals specifically taking polystyrene sulfonate, sulfamethoxazole, fluoroquinolones, benzathine penicillin, sulfonamides, nitrobenzene, and heparin were excluded from our study to avoid confounding effects that these medications might have on depression risk or platelet counts. These medications were excluded to avoid interference with the primary analysis of ITP medications’ impact on depression. 25 For example, certain antibiotics and anticoagulants have been associated with neuropsychiatric adverse effects, which could confound the results of our study if not properly controlled for. 30 Although our study primarily focused on the relationship between ITP medication use and depression, it also highlighted significant associations between depression and various sociodemographic and health-related factors. For example, our data indicated a higher prevalence of depression among individuals with lower income, less education, and higher BMI. These findings are consistent with the broader literature on the social determinants of mental health, which suggests that economic and social inequalities are critical factors influencing depression risk. 29 In addition, our study found that females exhibited higher levels of depression and anxiety than males, aligning with previous research. 28 However, given that this was not the primary focus of our study, we did not delve deeply into the gender-specific mechanisms underlying these differences. Nonetheless, it is important to note that gender disparities in depression prevalence may reflect differential exposure to risk factors, such as social stressors and hormonal influences, as well as distinct coping styles between males and females. 31
One of the main limitations of our study is its cross-sectional nature, which precludes establishing causality between ITP medication use and depression. However, it is important to consider potential treatment bias that may influence the results. Certain populations might be more likely to receive ITP medication, and these populations could also have a different risk profile for developing depressive symptoms. Addressing this bias in future studies could provide a clearer understanding of the true relationship between ITP medication use and depression risk. In addition, the reliance on self-reported data may introduce bias, and the exclusion of certain populations with comorbid conditions could limit the generalizability of our findings. Furthermore, our study did not include formal diagnoses of depression, relying instead on survey data that may not capture the clinical complexity of depressive disorders. Despite these limitations, our study has several strengths, including the large sample size and the comprehensive adjustment for various potential confounders, which enhances the robustness of our findings. Overall, our study has important clinical implications. Given that ITP medication use does not appear to independently increase the risk of depression, clinicians can be reassured when prescribing these medications. However, it remains crucial to monitor patients for any potential psychological adverse effects, particularly given the complex psychotropic effects of corticosteroids. In addition, our findings underscore the importance of considering a comprehensive array of factors, including sociodemographic and health-related determinants, when evaluating depression risk in patients. Future research should focus on longitudinal studies to better understand the temporal relationship between ITP medication use and depression. Moreover, investigations into the biological mechanisms underlying the psychotropic effects of corticosteroids could provide further insights into how these medications influence mental health. In addition, further research on depression in individuals under 18 years is needed, as this age group may have unique vulnerabilities and risk factors that warrant specific investigation. Finally, research exploring the impact of various sociodemographic factors on depression risk in the context of ITP treatment could help to identify vulnerable populations and inform targeted interventions.
Conclusion and Relevance
This study revealed no significant association between the use of ITP medications and depression after adjusting for confounders, challenging assumptions about direct causal links between specific treatment regimens and mental health outcomes. The implications suggest a reevaluation of the psychosocial aspects of ITP management and highlight the necessity for personalized care strategies that consider the complex interplay of medical and sociobehavioral factors in patient wellness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of Zhejiang Province (no. LYY22H310009) and Hospital Pharmacy Scientific Research Funding Project of Zhejiang Pharmaceutical Association (no. 2020ZYY10).